Introduction
Lung cancer is the leading cause of cancer-induced
mortality worldwide, and non-small cell lung cancer (NSCLC)
accounts for ~85% of all lung cancer cases (1,2). The
majority of NSCLC patients already have advanced or metastatic
disease at the time of diagnosis (3).
Recently, mutations to the EGFR gene were identified in patients
with NSCLC and the most commonly found EGFR mutations were
deletions in exon 19 and mutations in exon 21 (4). Approximately 10% of these EGFR mutations
were detected in Caucasian patients with NSCLC, and 40–60% in Asian
NSCLC patients. The disease has been previously associated with
sensitivity to the small molecule TKIs (4,5). Epidermal
growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) have
been used for the treatment of advanced NSCLC harboring EGFR
sensitizing mutations, and have been shown to improve
progression-free and overall survival in these patients (median
overall survival OS, >2 years) (6). In addition, 70% of patients with EGFR
sensitizing mutations treated with TKIs achieved a complete or
partial response, while only 33% of patients receiving chemotherapy
had the same results (7); however,
every patient who had initially responded to EGFR-TKI treatment
eventually acquired EGFR-TKI resistance, resulting in relapse while
still under TKI therapy (8).
Bevacizumab is a recombinant, humanized monoclonal
antibody that blocks vascular endothelial growth factor (VEGF)
(9). The Eastern Cooperative Oncology
Group 4599 study compared the efficacy of treatment with
carboplatin/paclitaxel with or without bevacizumab in patients with
advanced non-squamous NSCLC (10).
The results showed that the use of paclitaxel and carboplatin,
combined with bevacizumab resulted in a significant improvement in
the median overall and progression-free survival, which marked the
start of a new paradigm for the treatment of advanced nonsquamous
NSCLC. The JO25567 study, a phase II randomized controlled trail,
provided evidence that first-line treatment with a combination of
erlotinib and bevacizumab significantly improved the median
regression-free survival in patients with nonsquamous NSCLC with
activating EGFR mutations (11);
however, the effect of bevacizumab on TKI resistance in patients
with NSCLC with activating EGFR mutations remains largely unknown.
In the present case of metastatic lung adenocarcinoma with acquired
EGFR-TKI resistance, the use of bevacizumab with TKI treatment lead
to the stabilization of the disease and minimal tumor
regression.
Case report
A 53-year-old female patient presented with a cough
and hemoptysis in May 2013, without a headache, nausea, vomiting or
shortness of breath. A mass was detected in the right inferior
lung, with malignant ipsilateral pleural effusion and multiple
brain metastases (BM) in bilateral lobes, as well as mediastinal
and supraclavicular lymph nodes upon thoracic computed tomography
(CT) and whole-body positron emission tomography/CT, performed in
Shenzhen People's Hospital (Shenzhen, China). The patient was
referred to Xinqiao Hospital (Chongqing, China) and a core biopsy
of the mass in the right lung was performed, confirming a moderate
differentiated adenocarcinoma. Scorpion/Amplification Refractory
Mutation System EGFR mutation test detected an EGFR exon 19
deletion in tumor cells. The patient was started on first-line
treatment with EGFR-TKI on June 2013 and developed a partial
response, according to chest CT evaluation; however, after 8 months
of EGFR-TKI treatment, a thoracic CT scan confirmed disease
progression in the lung lesion. Second line chemotherapy
(pemetrexed, 500 mg/m2 plus cisplatin, 75
mg/m2) was initiated on 28 February 2014, and cell
biological treatment was administered in Daping Hospital
(Chongqing, China). Following four cycles of chemotherapy, the
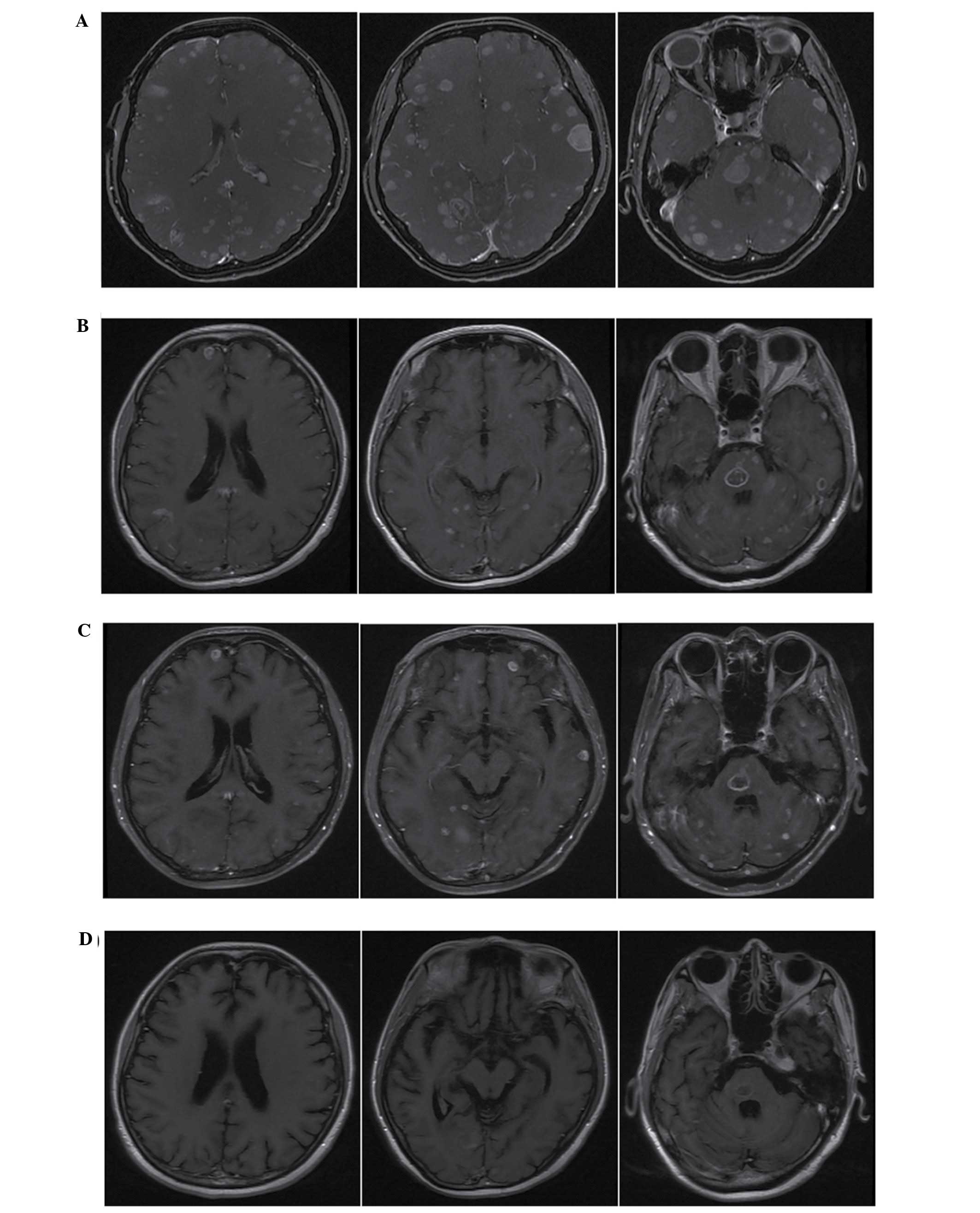
patient's symptoms worsened and she experienced headaches,
dizziness and worsening neurological symptoms of speech and
left-sided limb impairment. Radiographic evaluation showed disease
progression in the lung lesion and pleural effusion (Fig. 1A), and new multiple brain metastases
(Fig. 2A); therefore, treatment with
the second-generation TKI afatinib (40 mg/day) and concurrent
whole-brain radiotherapy (WBRT; 30 Gy/10F/2W) was initiated on July
2014. A partial radiographic and clinical response of the mass in
the primary right lobe and metastases in the lung, pleura (Fig. 1B) and brain (Fig. 2B) was achieved. After 3 months of
treatment with afatinib, disease progression was detected in the
right lung lesion and pleural effusion (Fig. 1C), while the BM remained stable
(Fig. 2C).
The patient refused to receive re-biopsy and
additional chemotherapy. Combination treatment with bevacizumab and
afatinib was recommended and approved by the patient; treatment
with bevacizumab (7.5 mg/kg once every 2 weeks) by intravenous
infusion was commenced in Xinqiao Hospital on October 9, 2014,
combined with continued therapy of afatinib (40 mg/day). No
hypertension, hemorrhage or proteinuria was recorded during the
treatment. After 1 month of treatment, thoracic CT and brain
magnetic resonance imaging (MRI) scans showed shrinkage of the mass
in the right lung and BM, as well as a right pleural effusion
reduction. At the time of writing, the patient remained under
combination therapy with afatinib with bevacizumab, and the right
lung mass, BM and pleural effusion were shown to be stable on
follow-up CT (Fig. 1D) and MRI scans
(Fig. 2D). No serious adverse events
occurred throughout the treatment period, and the patient had a
good quality of life.
Discussion
To date, no previous reports have been published on
the use of bevacizumab against EGFR-TKI resistance in patients with
activating EGFR mutations. To the best of our knowledge, the
present study is the first to report combination treatment with
bevacizumab and afatinib overcoming acquired EGFR-TKI
resistance.
EGFR-TKIs have been shown previously to have a
positive effect on patients with advanced NSCLC with EGFR
activating mutations, and are therefore used as first-line treatment
for this condition (12–14); however, treatment with EGFR-TKI is not
curative; tumor cells inevitably develop EGFR-TKI resistance, which
leads to disease progression. Additionally, it has been shown that
the major resistance mechanisms are due to T790M point mutation on
EGFR exon 20 (15). The
third-generation EGFR-TKIs that are able to overcome T790M-mediated
resistance to EGFR inhibitors in lung cancer are still being
studied in clinical trails (16). The
JO25567 phase 2 trial showed that combination treatment with
erlotinib and bevacizumab significantly improved the
progression-free survival of patients with NSCLC with activating
EGFR mutations, as compared with erlotinib alone (11); however, no evidence has demonstrated
that the addition of bevacizumab to TKI treatment can reverse
acquired TKI resistance in NSCLC; the findings of the JO25567 trial
implied that bevacizumab can postpone the resistance of tumor cells
to TKI. In the present case, the lung and pleural lesions developed
a resistance to afatinib, but shrank following the administration
of combination treatment with bevacizumab and afatinib. In
addition, follow-up CT and MRI scans showed that the lesions
remained stable on, which suggests that the addition of bevacizumab
helped overcome TKI resistance in patients with NSCLC harboring
EGFR activating mutations.
WBRT remains the cornerstone of treatment for
multiple central nervous system metastases caused by NSCLC. Lately,
a therapeutic effect of EGFR-TKI in BM harboring EGFR-activating
mutations has been demonstrated (14,17). The
concomitant use of EGFR-TKI and radiotherapy plays an important
role in patients with multiple, symptomatic BM due to NSCLC
harboring EGFR mutations (18). The
effect of combined treatment with TKIs and WBRT against BM was
observed in the present patient. An MRI scan following treatment
with afatinib and concurrent WBRT confirmed that a marked partial
response of the BM had been achieved.
Bevacizumab in combination with chemotherapy has
shown a significant survival benefit in NSCLC, and has been
approved for the treatment of patients with locally advanced or
metastatic non-squamous NSCLC (10).
Due to concerns regarding the risk of central nervous system
hemorrhage, patients with BM had previously been largely excluded
from clinical trials involving bevacizumab; however, it has since
been demonstrated that anti-angiogenic therapy with bevacizumab is
safe for patients with BM (19,20).
Bevacizumab is a humanized anti-vascular endothelial growth factor
monoclonal antibody. Questions on whether bevacizumab is capable of
penetrating the brain-blood barrier and having a certain effect on
NSCLC-induced BM have arisen. In the present study, MRI scans
showed that the BM remained stable under treatment with afatinib;
however, the addition of bevacizumab to afatinib treatment achieved
further shrinkage of the BM, which suggests that the combination of
EGFR-TKI and bevacizumab could achieve a favorable outcome for
patients with BM caused by nonsquamous NSCLC habouring EGFR
activating mutation.
In conclusion, the addition of bevacizumab to
afatinib treatment can tackle TKI resistance and promote a better
outcome for patients with NSCLC-induced BM with EGFR activating
mutations; however, further studies are required to confirm these
findings.
References
|
1
|
Siegel R, Ma J, Zou Z and Jemal A: Cancer
statistics, 2014. CA Cancer J Clin. 64:9–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dempke WC, Suto T and Reck M: Targeted
therapies for non-small cell lung cancer. Lung Cancer. 67:257–274.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ettinger DS, Akerley W, Borghaei H, Chang
AC, Cheney RT, Chirieac LR, D'Amico TA, Demmy TL, Ganti AK,
Govindan R, et al: Non-small cell lung cancer. J Nal Compr Canc
Netw. 10:1236–1271. 2012.
|
|
4
|
Sequist LV, Joshi VA, Jänne PA, Muzikansky
A, Fidias P, Meyerson M, Haber DA, Kucherlapati R, Johnson BE and
Lynch TJ: Response to treatment and survival of patients with
non-small cell lung cancer undergoing somatic EGFR mutation
testing. Oncologist. 12:90–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ji H, Li D, Chen L, Shimamura T, Kobayashi
S, McNamara K, Mahmood U, Mitchell A, Sun Y, Al-Hashem R, et al:
The impact of human EGFR kinase domain mutations on lung
tumorigenesis and in vivo sensitivity to EGFR-targeted therapies.
Cancer Cell. 9:485–495. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Petrelli F, Borgonovo K, Cabiddu M and
Barni S: Efficacy of EGFR tyrosine kinase inhibitors in patients
with EGFR-mutated non-small-cell lung cancer: A meta-analysis of 13
randomized trials. Clin Lung Cancer. 13:107–114. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nguyen KS, Kobayashi S and Costa DB:
Acquired resistance to epidermal growth factor receptor tyrosine
kinase inhibitors in non-small-cell lung cancers dependent on the
epidermal growth factor receptor pathway. Clin Lung Cancer.
10:281–289. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hurwitz H, Fehrenbacher L, Novotny W,
Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S,
Holmgren E, et al: Bevacizumab plus irinotecan, fluorouracil, and
leucovorin for metastatic colorectal cancer. N Engl J Med.
350:2335–2342. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sandler A, Gray R, Perry MC, Brahmer J,
Schiller JH, Dowlati A, Lilenbaum R and Johnson DH:
Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med. 355:2542–2550. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Seto T, Kato T, Nishio M, Goto K, Atagi S,
Hosomi Y, Yamamoto N, Hida T, Maemondo M, Nakagawa K, et al:
Erlotinib alone or with bevacizumab as first-line therapy in
patients with advanced non-squamous non-small-cell lung cancer
harbouring EGFR mutations (JO25567): An open-label, randomised,
multicentre, phase 2 study. Lancet Oncol. 15:1236–1244. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Reck M, Popat S, Reinmuth N, De Ruysscher
D, Kerr KM and Peters S: ESMO guidelines working group: Metastatic
non-small-cell lung cancer (NSCLC): ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol.
25(Suppl 3): iii27–iii39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pao W, Miller VA, Politi KA, Riely GJ,
Somwar R, Zakowski MF, Kris MG and Varmus H: Acquired resistance of
lung adenocarcinomas to gefitinib or erlotinib is associated with a
second mutation in the EGFR kinase domain. PLoS Med. 2:e732005.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liao BC, Lin CC and Yang JC: Second and
third-generation epidermal growth factor receptor tyrosine kinase
inhibitors in advanced nonsmall cell lung cancer. Curr Opin Oncol.
27:94–101. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Park SJ, Kim HT, Lee DH, Kim KP, Kim SW,
Suh C and Lee JS: Efficacy of epidermal growth factor receptor
tyrosine kinase inhibitors for brain metastasis in non-small cell
lung cancer patients harboring either exon 19 or 21 mutation. Lung
Cancer. 77:556–560. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang J, Yu J, Sun X and Meng X: Epidermal
growth factor receptor tyrosine kinase inhibitors in the treatment
of central nerve system metastases from non-small cell lung cancer.
Cancer Lett. 351:6–12. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Soffietti R, Trevisan E and Rudà R:
Targeted therapy in brain metastasis. Curr Opin Oncol. 24:679–686.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Besse B, Le Moulec S, Mazières J,
Senellart H, Barlesi F, Chouaid C, Dansin E, Bérard H, Falchero L,
Gervais R, et al: Bevacizumab in patients with nonsquamous
non-small cell lung cancer and asymptomatic, untreated brain
metastases (BRAIN): A nonrandomized, Phase II Study. Clin Cancer
Res. 21:1896–1903. 2015. View Article : Google Scholar : PubMed/NCBI
|