Introduction
Primary mediastinal germ cell tumors (GCTs) are
relatively rare, and are often complicated by various pathological
types and characteristics. Seminoma is one kind of such tumors.
Primary mediastinal seminoma usually occurs in young males, and the
tumor often locates to the anterior mediastinum. Primary
mediastinal germ cell tumors (GCTs) are relatively rare, accounting
for only approximately 1%-3% of all GCTs (1) and seminoma is the second most common
mediastinal GCTs. Approximately 90% of primary malignant
mediastinal GCTs occur in male subjects in the 2nd, 3rd, 4th
decades of life (2). The histogenesis
of primary seminoma of the anterior mediastinum is unknown; it has
suggested that it develops from extragonadal, potentially biphasic
germ cells left within the embryonic thymus. In terms of survival,
the prognosis of seminoma is usually well, 5-year survival rate
~75%. Nonseminoma has a worse prognosis compared with seminoma.
Cases with pleural dissemination or metastasis also have a worse
prognosis. It would be possible to improve the prognosis with the
establishment of a standard treatment regimen, development of new
agents for the treatment of tumors resistant to current
chemotherapy regimens, and detection of more tumors in the early
stage (3).
Here we present an extremely rare case of primary
seminoma arising in the middle mediastinum of a 52-year-old
man.
Case presentation
A 52-year-old male was admitted to Qingdao Central
Hospital (Qingdao, China) in June 2014, due to a cough and chest
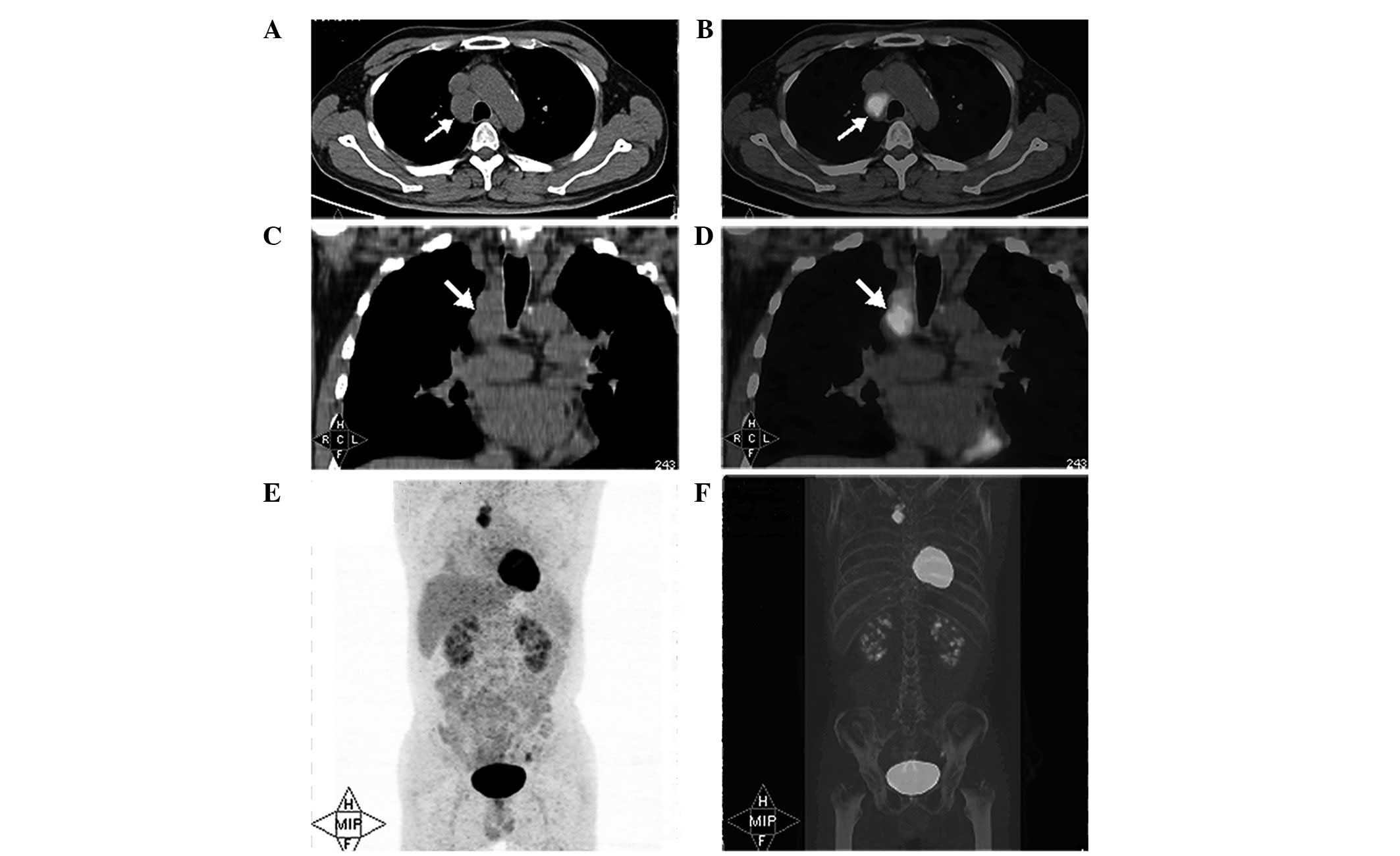
tightness. Thoracic computed tomography (CT) scans showed a
3.0×2.3-cm mass located in the space between the trachea and the
superior vena cava (Fig. 1A).
Fluorine-18 fluorodeoxyglucose-positron emission tomography
(18F-FDG-PET) scans revealed unique abnormal FDG uptake
in the mediastinal tumor, with a clear margin and uniform inner
density without calcification (Fig.
1B–F). Serum α-fetoprotein and β-human chorionic gonadotropin
levels were tested and found to be within the normal ranges. The
patient's leukocyte level was a little bit higher than the normal
range (9.8×109; normal range 3.5–9.5×109).
All other blood tests were in normal ranges. The patient had
suffered from type II diabetes mellitus (DM) for 10 years and also
had a family history of DM.
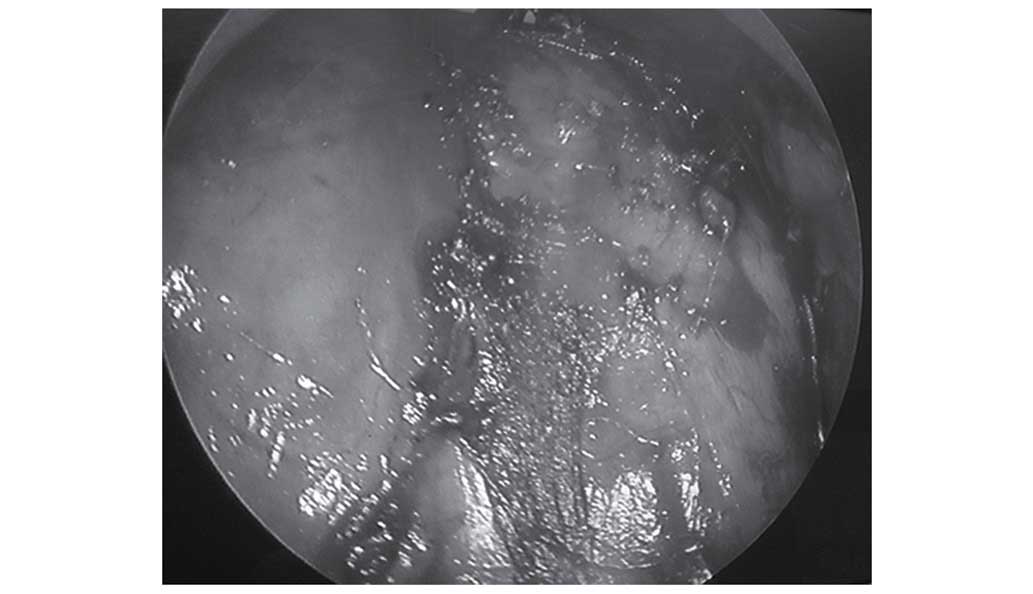
A mediastinoscopy was performed and the tumor was
found located on the right side of trachea, behind the vena cava
and beneath the azygos vein (Fig. 2).
Tumor tissues were in close proximity and adhered to the superior
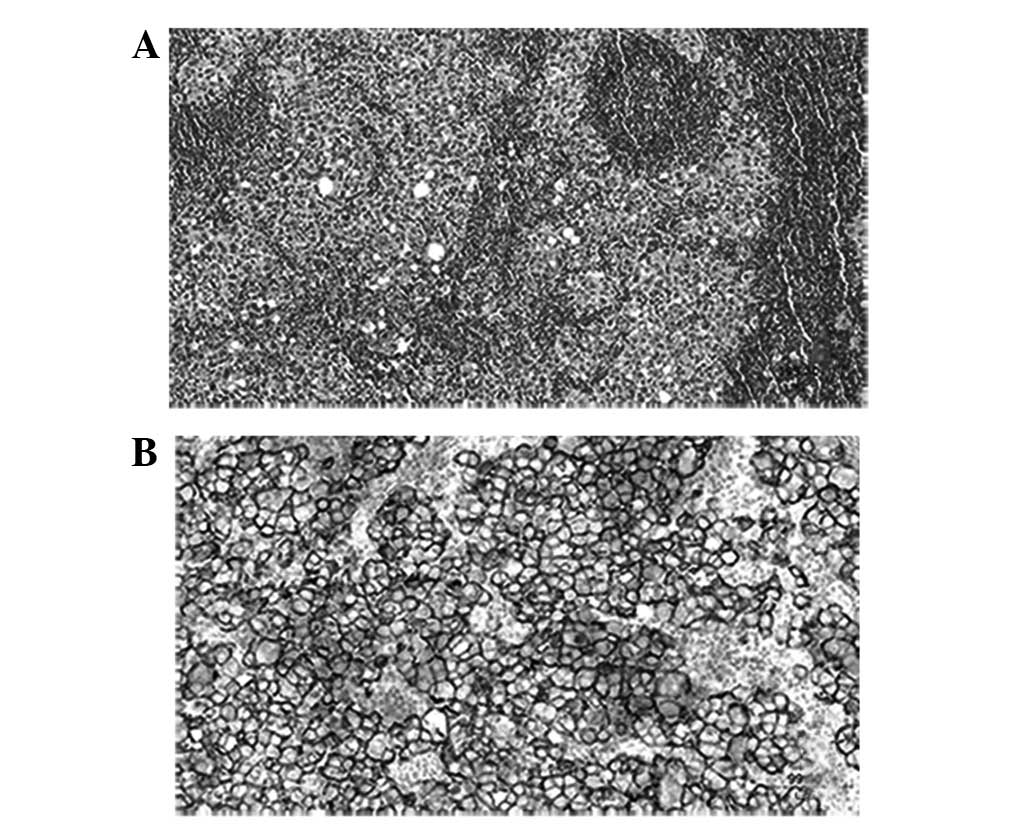
vena cava, and integral excision was difficult. A biopsy was
implemented and histological examination revealed a primary
seminoma, with some sheets of round and polygonal tumor cells
surrounded by lymphocytes on the paraffin-embedded sections
(Fig. 3A). The tumor cells had a
clear or granular cytoplasm, coarse-clumped chromatin and prominent
nucleoli with frequent mitoses. The diagnosis of seminoma was
established by the immunohistochemical studies of the neoplastic
tissue. The tumor was positive for placental alkaline phosphatase
(PLAP) (Fig. 3B), which is used as a
representative surface marker of seminoma. As there were no tumors
found at the thymus or testicles, or at any other site upon
18F-FDG-PET, a primary middle mediastinal seminoma was
diagnosed.
At 2 weeks post-biopsy, chemotherapy was started
with the bleomycin, etoposide and cisplatin regimen [25 mg
intravenous (i.v.) bleomycin once a week for 3 weeks, 100 mg i.v.
etoposide on days 1–4 and 60 mg i.v. Naida platinum on days 1–2],
for 4 cycles, followed by conformal intensity-modulated radiation
therapy (2 Gy/day; total, 40 Gy). A partial response was achieved,
as the tumor decreased in size and no FDG uptake was apparent on
18F-FDG-PET after finishing the chemoradiotherapy. The
patient has not received any further treatment after finishing 4
cycles of chemotherapy and 40 Gy radiotherapy, regular follow-up
was initiated thereafter. The last follow-up date was April 2016
and the patient has remained disease-free for 20 months.
Discussion
Extragonadal germ cell tumors (GCTs) are typically
located along the midline of the trunk, and seminoma is the second
most common type of all mediastinal GCTs. Mediastinal seminoma is
frequently located in the anterior mediastinum involving the
thymus. Upon reviewing the English literature in PubMed (http://www.ncbi.nlm.nih.gov/pubmed), only 3 cases
of seminoma that primarily originated from the middle mediastinum
were found (4–6). As certain anterior mediastinal seminomas
may enlarge and extend into the middle mediastinal compartment, it
is a challenge to distinguish the initial site for large tumors. In
the present study, 18F-FDG-PET scans assisted in
locating the unique mass in the middle mediastinum, and also played
an important role in clinical staging and the evaluation of therapy
effects.
These extragonadal tumors are believed to develop
from germ cell precursors that become arrested during embryological
migration and survive in ectopic locations. Approximately 90% of
primary malignant mediastinal GCTs occur in male subjects in the
third decade of life. In the three studies of seminoma that
occurred in middle mediastinum (4–6), all cases
were in men and the age ranged from 25 to 69 years old, with a mean
age of 53 years old when including the present patient.
Primary mediastinal seminoma typically occurs with
non-specific symptoms, including chest pain or pressure, dyspnea,
hoarseness, dysphagia and fever. Rarely, the tumor may cause
superior vena cava syndrome (7) and
severe back pain (8). With regard to
the three aforementioned studies, all cases were either
asymptomatic or presented with dull retrosternal chest pain
(4–6).
The present patient complained of a cough and chest tightness,
which was due to the closeness of the tumor and/or its compression
of the trachea. The symptoms were closely associated with the
location and size of the tumor.
The differential diagnosis of mediastinal seminoma
includes a range of metastatic and primary malignant mediastinal
neoplasms. The possibility of metastasis from a testicular primary
tumor should always be considered. In the present case,
18F-FDG-PET played an important role in distinguishing
the primary tumor from a metastasis. Considering the unusual
location of the tumor and the age of the patient,
poorly-differentiated carcinoma, embryonal carcinoma, thymic
carcinoma, lymphoma and mesothelioma were also differential
diagnostic considerations (9). The
morphological overlap between embryonal carcinoma or seminoma and a
poorly-differentiated carcinoma (e.g., pulmonary, thymic or
metastatic) is significant. Cytokeratin and cluster of
differentiation (CD)30 are characteristically coexpressed in
embryonal carcinoma, but are not specific to only this tumor. Other
primary carcinoma markers, including thyroid transcription factor-1
(TTF-1; lung) and CD5 (thymic), may also be useful in this setting
(9). The present case was negative
for CD30, TTF-1 and CD5, but positive for PLAP, so the possibility
of embryonal carcinoma, metastatic lung cancer or thymic carcinoma
was excluded. Primary mediastinal (thymic) large B cell lymphoma
(PMBL), lymphoblastic lymphoma (LBL), anaplastic large cell
lymphoma (ALCL) and classic Hodgkin's lymphoma (CHL) may
potentially mimic embryonal carcinoma or seminoma (9). The markers of lymphoma are complicated,
with the main distinguishing markers including CD20 and CD23
(PMBL), CD34 and terminal deoxynucleotidyl transferase (LBL),
epithelial membrane antigen and anaplastic lymphoma kinase (ALCL);
and CD15 and paired box protein Pax-5 (CHL). As all the
aforementioned markers were negative, the possibility of a number
of lymphomas was also excluded. Although PLAP has traditionally
been the preferential marker for the objective verification of germ
cell origin (mostly seminoma) in the setting of an undifferentiated
neoplasm, it has been found that for extragonadal seminoma,
octamer-binding transcription factor 3/4, activator protein 2γ,
D2-40 and c-kit are equivalently superior to PLAP (10).
Patients with early-stage mediastinal seminoma are
curable by complete surgical resection followed by radiation
therapy (4,000–4,500 cGy). All other advanced-stage patients should
receive initial cisplatin-based chemotherapy. In those individuals
who are considered not to be good candidates for combination
chemotherapy and who have tumors in the mediastinum, radiation
therapy is an acceptable initial treatment (11).
In conclusion, primary seminoma in the middle
mediastinum is extremely rare, but may be cured by combined
modalities. Oncologists should be aware of this disease and
continue to shed further light on its early diagnosis. Primary
seminoma in the middle mediastinum is extremely rare, but may be
cured by combined modalities. Completely surgical resection with
adjuvant chemo-irradiation was the cornerstone for the successful
treatment of this case.
References
|
1
|
Nichols CR: Mediastinal germ cell tumors:
clinical feature and biologic correlates. Chest. 99:472–479. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Knapp RH, Hurt RD, Payne WS, et al:
Malignant germ cell tumors of the mediastinum. J Thorac Cardiovasc
Surg. 89:82–89. 1985.PubMed/NCBI
|
|
3
|
Yano M and Fujii Y: Results of surgical
treatment for pimary germcell tumors of the mediastinum. Nihon Geka
Gakkai Zasshi. 107:278–83. 2006.[In Japanese]. PubMed/NCBI
|
|
4
|
Nakamura H, Hashimoto T, Kusama H, Sudoh
A, Adachi H, Yagyu H, Kishi K, Oh-ishi S and Matsuoka T: Primary
seminoma in the middle mediastinum. Intern Med. 43:1191–1193. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kiffer JD and Sandeman TF: Primary
malignant mediastinal germ cell tumor: A study of 11 cases and a
review of the literature. Int J Radiat Oncol Biol Phys. 17:835–841.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kitami A, Suzuki K, Suzuki S and Hori G:
Primary seminoma in the middle mediastinum: Case report in a
69-year-old male. Jpn J Clin Oncol. 28:142–144. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xu X, Sun C, et al: A case of mediastinal
seminoma presenting as superior vena cava syndrome. Intern Med.
51:1269–1272. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kaako A, et al: Mediastinal extragonadal
seminoma presenting as severe back pain in a young male. Tenn Med.
104:41–45. 2011.PubMed/NCBI
|
|
9
|
McKenney JK, Heerema-McKenney A and Rouse
RV: Extragonadal germ cell tumors: A review with emphasis on
pathologic features, clinical prognostic variables, and
differential diagnostic considerations. Adv Anat Pathol. 14:69–92.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Iczkowski KA, Butler SL, Shanks JH,
Hossain D, Schall A, Meiers I, Zhou M, Torkko KC, Kim SJ and
MacLennan GT: Trials of new germ cell immunohistochemical stains in
93 extragonadal and metastatic germ cell tumors. Hum Pathol.
39:275–281. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hainsworth JD and Greco FA: Germ cell
neoplasms and other malignancies of the mediastinum. Cancer Treat
Res. 105:303–325. 2001. View Article : Google Scholar : PubMed/NCBI
|