Introduction
Endometrial cancer (EC) is the most common malignant
tumor of the female genital tract in the developed countries of
North America and Europe. At diagnosis, endometrioid endometrial
cancer (EEC) does not extend beyond the uterus in >75% of cases
and is characterized by a good prognosis, with an overall 5-year
survival rate of 75–80% (1,2). Histological diagnosis reports in most
cases a type 1 EC, termed EEC, which is usually associated with low
aggressiveness and long term disease free survival; whereas type 2
EC refers to high-risk neoplasias, such as serous or clear cell EC
(1).
The current management of EC includes total
hysterectomy with bilateral salpingo-oophorectomy (BSO),
lymphadenectomy, if necessary, and peritoneal cytology (3). Laparoscopy offers unique benefits
including shorter recovery time, improved performance status
following surgery and a decreased risk of adhesions when compared
with open laparotomy procedures, and is increasingly used as an
alternative to abdominal surgery in the management of EC (4).
The laparoscopic management of malignancies has also
brought about novel, late complications of surgical therapy in the
form of tumor recurrences and trocar insertion sites metastases
(5). Laparoscopic port-site
metastases (PSMs) are early recurrent tumorous lesions developing
locally in the abdominal wall within the scar tissue of one or more
trocar sites, and can be compared to wound metastases after open
surgery. By definition, port site recurrences are not associated
with diffuse peritoneal carcinomatosis (5–7).
The overall incidence of PSM in gynecologic
malignancies has been estimated to be 1–2%, reaching 19.6% in
patients with advanced ovarian cancer undergoing diagnostic
laparoscopy; PSMs have also been reported in patients with previous
EC (8). The purpose of the present
case study is to describe a rare case of isolated port-site
metastasis following laparoscopic surgical staging for early
low-grade EEC and to review all the published cases of PSMs after
laparoscopic surgery for EC.
Case report
A 57-year-old woman who had been complaining of
postmenopausal uterine bleeding for 8 months underwent hysteroscopy
without anaesthesia with endometrial biopsy in January 2013 at the
University Hospital of Parma (Parma, Italy). The pathology report
revealed a grade 1 EEC. The patient's medical history revealed
arterial hypertension, diabetes, severe obesity, gastric banding
and had 3 previous successful pregnancies and 2 miscarriages.
Preoperatory CA125, CA19.9, CA 15.3 and CEA immunopositivity were
negative. Preoperative imaging, including transvaginal ultrasound
and total body computed tomography (CT) suggested a stage I tumor.
In February 2013, a total laparoscopic hysterectomy (TLH) with BSO
and pelvic washing were performed.
The surgical procedure started with uterine
manipulator placement. A 12 mmHg pneumoperitoneum was induced
through a 10-mm optic view umbilical port; three 5-mm additional
ports in the right and the left iliac fossa and in the sovrapubic
region were placed. The fallopian tubes were coagulated in their
uterine proximal portion and peritoneal washing for cytology was
performed. A surgical specimen was vaginally extracted without a
protection bag. Frozen sections, 10-µm thick and stained with
hematoxylin and eosin to reveal morphology, revealed an
endometrioid grade 1 tumor with myometrial invasion <50%, thus
it was decided that pelvic and paraortic lymph-nodes dissection
would not be performed. The ancillary trocars were removed after
desufflating through the umbilical port, then the abdominal wall
was closed. All port-wounds were irrigated with povidone. No
complications occurred during and after the procedure.
The pathology report revealed a FIGO 2009 Stage IA
grade 1 EEC with negative pelvic washing and did not indicate a
requirement for adjuvant therapy. A total of 7 months after the
primary surgery the patient complained of pain in the right iliac
fossa near to the port site scar. While examining the patient, a
little tender nodule was identified. An abdominal ultrasound and an
abdominal CT revealed a 28×24×19 mm irregular solid nodule close to
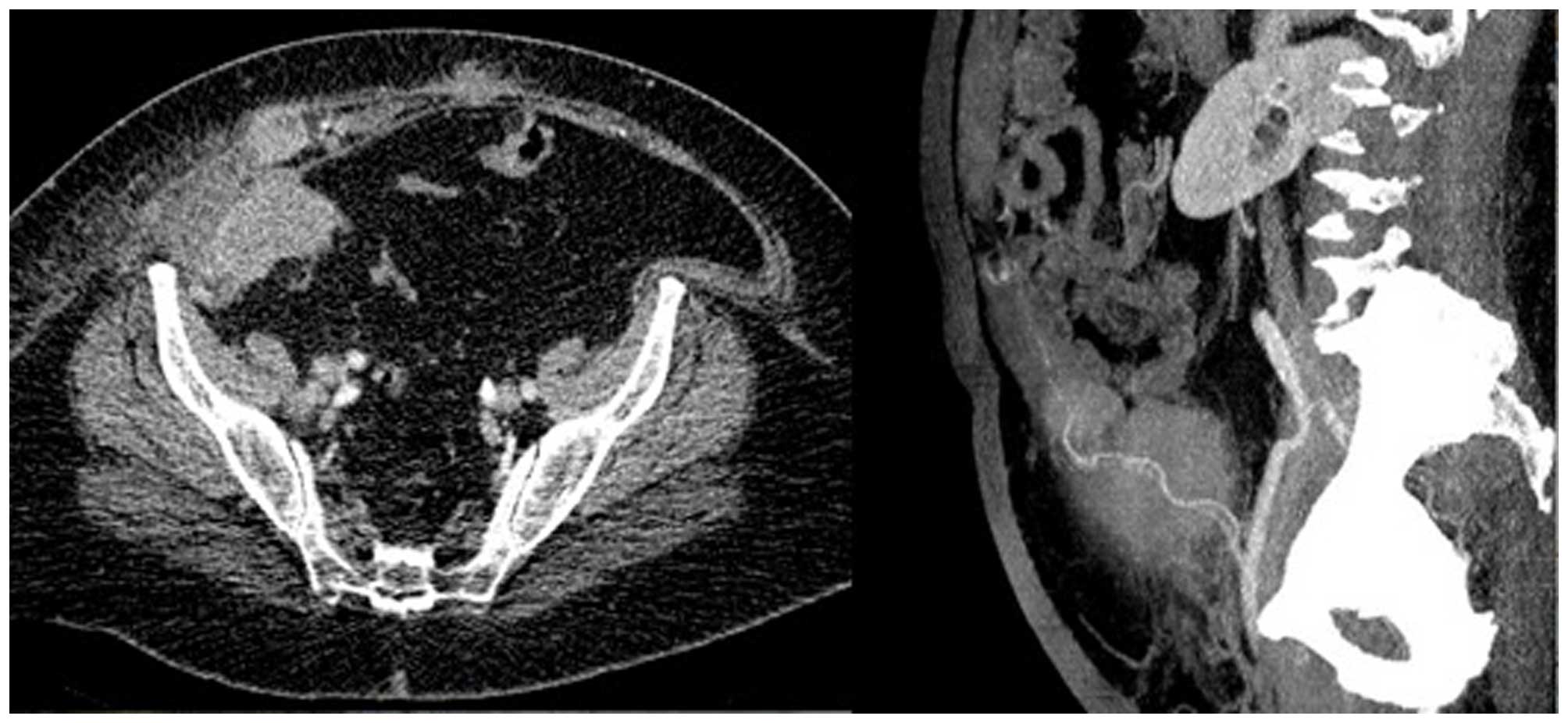
the right rectus abdominis muscle. After 2 months, immunopositivity
for CA125 was significantly increased and a CT scan revealed
multiple highly vascularized nodules, the largest one being 7 cm
and the second largest was 4 cm, into the right rectus abdominis
muscle near to the homologous fascia and a bulky right common iliac
lymph node, consistent with metastatic lesions (Fig. 1).
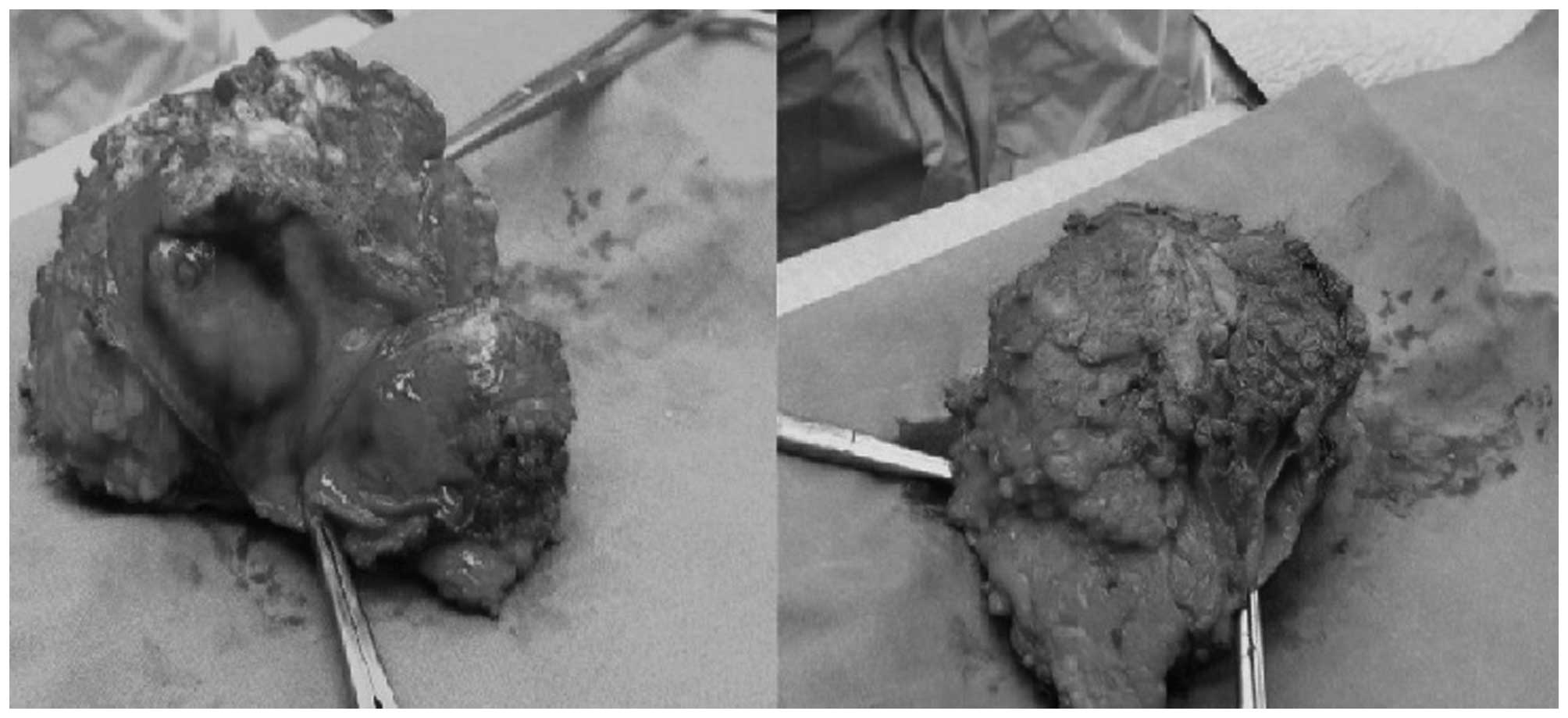
The patient underwent surgery. Peritoneal
carcinomatosis was not observed during the laparotomic procedure;
the abdominal metastatic lesion with the corresponding fascia and
skin was removed (Fig. 2) and the
right external lymphnodes were positive on positron emission
tomography (PET) scan. The fascia defect was repaired with a
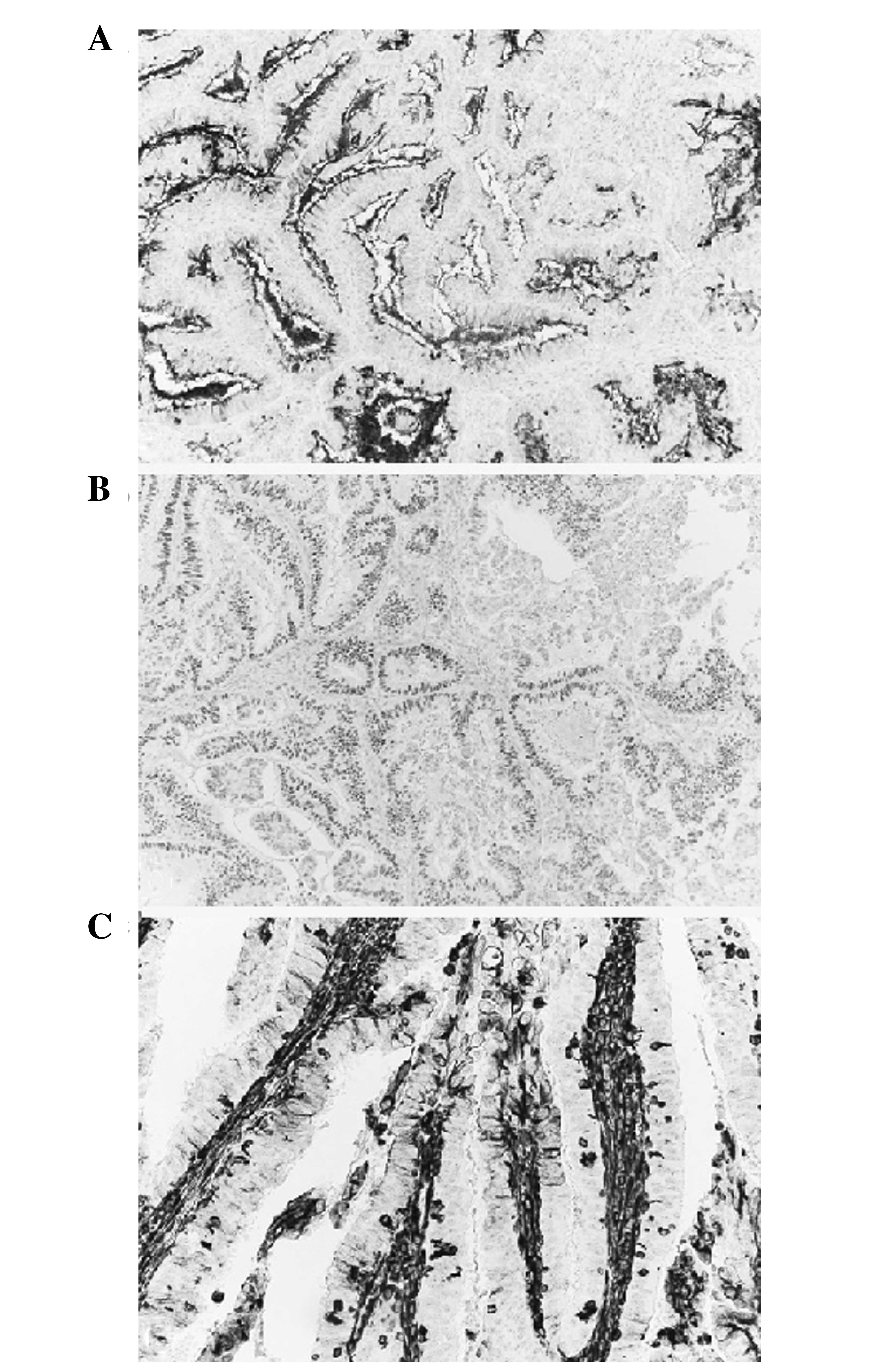
synthetic, nonabsorbable polypropylene mesh. The pathology report
revealed a metastatic endometrioid Grade 1 tumor; resected edges
and the lymph nodes were both negative for neoplastic spread
(Fig. 3). The adjuvant treatment
comprised chemotherapy with 175 mg/m2 carboplatin AUC 5
and taxolo, which had been stopped after the first cycle because of
intolerance (the patient completed 6 cycles monochemotherapy with
carboplatin, AUC 5, every 21 days), followed by abdominal external
radiotherapy, which remains ongoing. After 9 months, the patient
remains disease free and is negative for CA125.
Discussion
PSMs have been described as a rare phenomena,
occurring in <80 cases of gynecologic malignancies. Historically
the first case of PSM after laparoscopic surgery for EC was
reported in 1997 by Kadar et al (9).
A recent review by Palomba et al (8) of published and unpublished work up to
2011 reported only 9 cases of PSMs following laparoscopic surgery
for EEC: Amongst those, there was 1 Stage IA Grade 2 case and 3
Stage IB Grade 2 cases according to the FIGO 2009
Classification.
After 2011, Grabosh and Xynos (10) described 2 cases of isolated PSM after
robotic surgery for EEC. The first case was a Stage IA Grade 1 EEC
treated with TLH, BSO and pelvic lymphadenectomy. The second case
was a Stage IA Grade 1–2 EEC treated with TLH, BSO and pelvic and
paraortic lymphadenectomy due to uterine perforation during the
surgical procedure. Both cases were treated with surgical excision
of the PSM followed by chemo- and radiotherapy. Lonnerfors et
al (11) reported 4 cases of
PSMs, the first one was following a EEC Stage IIIC, the second and
the third case were after clear-cell adenocarcinoma Stage III and
the fourth case occurred following a carcinosarcoma Stage IB. EEC
was treated with laparoscopic radical hysterectomy, BSO, pelvic
nodal sampling and adjuvant chemo-, radio- and progesterone
therapy. The PSM was diagnosed 19 months after the primary surgery
and was associated with nodal and vaginal-cuff metastases. The
patient did not undergo additional treatment. Nguyen et al
(12) reported a case of PSM after
surgical treatment for Stage IB Grade 3 EEC treated with TLH, BSO,
pelvic and paraortic lymphadenectomy and brachitherapy. Two PSMs of
1.5 cm were diagnosed 12 months after surgery in two different port
sites and were associated with vaginal cuff metastases. The
treatment comprised surgical excision followed by chemotherapy.
Rindos et al (13) reported
two cases of PSMs after primary surgery for EC. The first case was
an isolated PSM 25 months after TLH and BSO for Stage IA Grade 2
EEC treated with surgical excision followed by chemo and
radiotherapy; the second case was a Stage 2 Grade 3 EC with
sarcomatous component treated with radical hysterectomy and BSO.
Finally, Rauff et al (14)
reported a case of serous Stage IIIB Grade 3 EC treated with
robotic surgery comprising TLH, BSO, pelvic lymphadenectomy and
omentectomy, followed by pelvic and vaginal cuff radiotherapy (the
patient refused chemotherapy). PSM was diagnosed 5 months after
primary surgery and treated with surgical excision and chemotherapy
with the addition of radiotherapy due to peritoneal progression of
disease during chemotherapy.
The etiology of PSM remains unknown. Factors
involved in PSMs may include exfoliation and spread of tumor cells
by laparoscopic instruments, direct implantation at the trocar site
by frequent changes of instruments, direct implantation from the
passage of the specimen, and the pneumoperitoneum itself can create
a ‘chimney effect’ that causes the passage of tumor cells at
port-sites. Moreover, laparoscopic port sites and peritoneal
incisions have demonstrated rapid cellular turnover and might
provide fertile ground for tumor cells. Other risk factors for the
development of port site metastases include ascites and advanced
stage (9).
According to the recommendations by Ramirez et
al (15), PSMs prevention could
be achieved through a reduction in tissue trauma and in the number
of the transferred instrument, a 5% povidone-iodine trocar rinsing
before insertion and trocar fixation. In addition, it may be useful
to rinse the tip of the instruments with 5% povidone-iodine when
interchanging them, to resect the tumor with adequate margins, to
use protective retrieval bags, to remove all the intraabdominal
fluid before trocar removal, to deflate the abdomen without trocars
removal, to irrigate the trocar sites with 5% povidone-iodine and
to close the peritoneal trocar sites (10–12 mm trocars).
PSMs are rare complications following laparoscopic
surgery. Stage IA Grade 1 EEC usually has a high survival rate and
a low 5-year recurrence risk. Amongst the 23 cases of EC PSMs
reported so far, 14 followed EEC and only 4 followed EEC Stage IA
Grade 1–2. In the present study, a rare case of PSM after Stage IA
Grade 1 EEC was reported. Surgeons must be conscious that PSMs may
occur even after low-risk disease and should take steps to prevent
them. The clinical and prognostic relevance of PSMs has not been
clarified at present as PSMs etiology is unknown; and it is not
known whether PSMs represent a local or systemic recurrence. The
gold-standard treatment has not been established and in the
majority of cases results in a combined approach with surgery,
chemo- and radiotherapy.
Glossary
Abbreviations
Abbreviations:
|
EC
|
endometrial cancer
|
|
EEC
|
endometrioid endometrial cancer
|
|
PSM
|
port site metastasis
|
|
CT
|
computed tomography
|
|
TLH
|
total laparoscopic hysterectomy
|
|
PET
|
positron emission tomography
|
|
BSO
|
bilateral salpingo-oophorectomy
|
References
|
1
|
Prat J: Prognostic parameters of
endometrial carcinoma. Hum Pathol. 35:649–662. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Giordano G, D'Adda T, Bottarelli L,
Lombardi M, Brigati F, Berretta R and Merisio C: Two cases of
low-grade endometriod carcinoma associated with undifferentiated
carcinoma of the uterus (dedifferentiated carcinoma): A molecular
study. Pathol Oncol Res. 18:523–528. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sanjuán A, Hernández S, Pahisa J, Ayuso
JR, Torné A, Martínez Román S, Lejárcegui JA, Ordi J and Vanrell
JA: Port-site metastasis after laparoscopic surgery for endometrial
carcinoma: Two case reports. Gynecol Oncol. 96:539–542. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dargent DF and Plante M: Laparoscopic
surgery in gynecologic cancer. Principles and practice of
gynecologic oncology. Hoskins WJ, Perez CA and Young RC: (3rd).
Lippincott Williams & Wilkins. (Philadelphia, PA). 265–295.
2000.
|
|
5
|
Schneider C, Jung A, Reymond MA, Tannapfel
A, Balli J, Franklin ME, Hohenberger W and Köckerling F: Efficacy
of surgical measures in preventing port site recurrences in a
porcine model. Surg Endosc. 15:121–125. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Castillo OA and Vitagliano G: Port site
metastasis and tumor seeding in oncologic laparoscopic urology.
Urology. 71:372–378. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee BR, Tan BJ and Smith AD: Laparoscopic
port site metastases: Incidence, risk factors, and potential
preventive measures. Urology. 65:639–644. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Palomba S, Falbo A and Zullo F: Isolated
port-site metastasis after laparoscopic surgery for endometrial
cancer: A case report. Gynecol Oncol Case Rep. 2:16–17. 2012.
View Article : Google Scholar
|
|
9
|
Kadar N: Port-site recurrences following
laparoscopic operations for gynaecological malignancies. Br J
Obstet Gynaecol. 104:1308–1313. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Grabosch S and Xynos F: Isolated port-site
metastasis after robotic hysterectomy for stage IA endometrial
adenocarcinoma. Obstet Gynecol. 122:437–439. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lönnerfors C, Bossmar T and Persson J:
Port-site metastases following robot-assisted laparoscopic surgery
for gynecological malignancies. Acta Obstet Gynecol Scand.
92:1361–1368. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nguyen T, Friedman J, Pradhan TS, Pua TL
and Tedjarati SS: Abdominal wall port site metastasis after
robotically staged endometrial carcinoma: A case report. Int J Surg
Case Rep. 4:613–615. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rindos N, Curry CL, Tabbarah R and Wright
V: Port-site metastases after robotic surgery for gynecologic
malignancy. JSLS. 18:66–70. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rauff S and Ng JS: Port-site recurrence in
a patient undergoing robot-assisted gynecologic cancer surgery for
endometrial cancer-A case report. Gynecol Oncol Case Rep.
2:127–129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ramirez PT, Frumovitz M, Wolf JK and
Levenback C: Laparoscopic port-site metastases in patients with
gynecological malignancies. Int J Gynecol Cancer. 14:1070–1077.
2004. View Article : Google Scholar : PubMed/NCBI
|