Introduction
Spindle cell carcinoma (SpCC), also known as
sarcomatoid carcinoma, pseudosarcoma and carcinosarcoma, is a rare
variant of squamous cell carcinoma (SCC), accounting for ~3% of all
head and neck SCCs (1). It is known
to be a biphasic tumor, with the epithelial component composed of
poorly differentiated SCC and the mesenchymal component composed of
spindle cells (2). In the head and
neck region, it commonly involves the larynx, while sinonasal
involvement is more rare (3). The
clinical presentations of sinonasal SpCC resemble those of
rhinosinusitis and there is currently no treatment protocol for
sinonasal SpCC (3,4). The present study reports a case of
synchronous inverted papilloma of the sphenoid sinus and SpCC
presenting with bilateral visual loss.
Case report
A 54-year-old male patient visited the Ophthalmology
Department of Shuang Ho Hospital (Taipei, Taiwan) in Febuary, 2014,
complaining of left-sided vision loss for 2 weeks, and was found to
have a visual acuity of 0.6 in oculus dexter (OD), and hand
motion/20 cm in the oculus sinister (OS). Fluorescence angiography
revealed no obvious anomalies, and the patient was released. One
week later, the patient also presented with right visual loss and
returned to the Department of Ophthalmology. Visual acuity was
found to have deteriorated (OD, 0.04; OS, no sensation of light).
The patient reported that he had been suffering from nasal
obstruction and discharge, and right frontal to parietal headache
for 3 months; thus, he was referred to the Department of
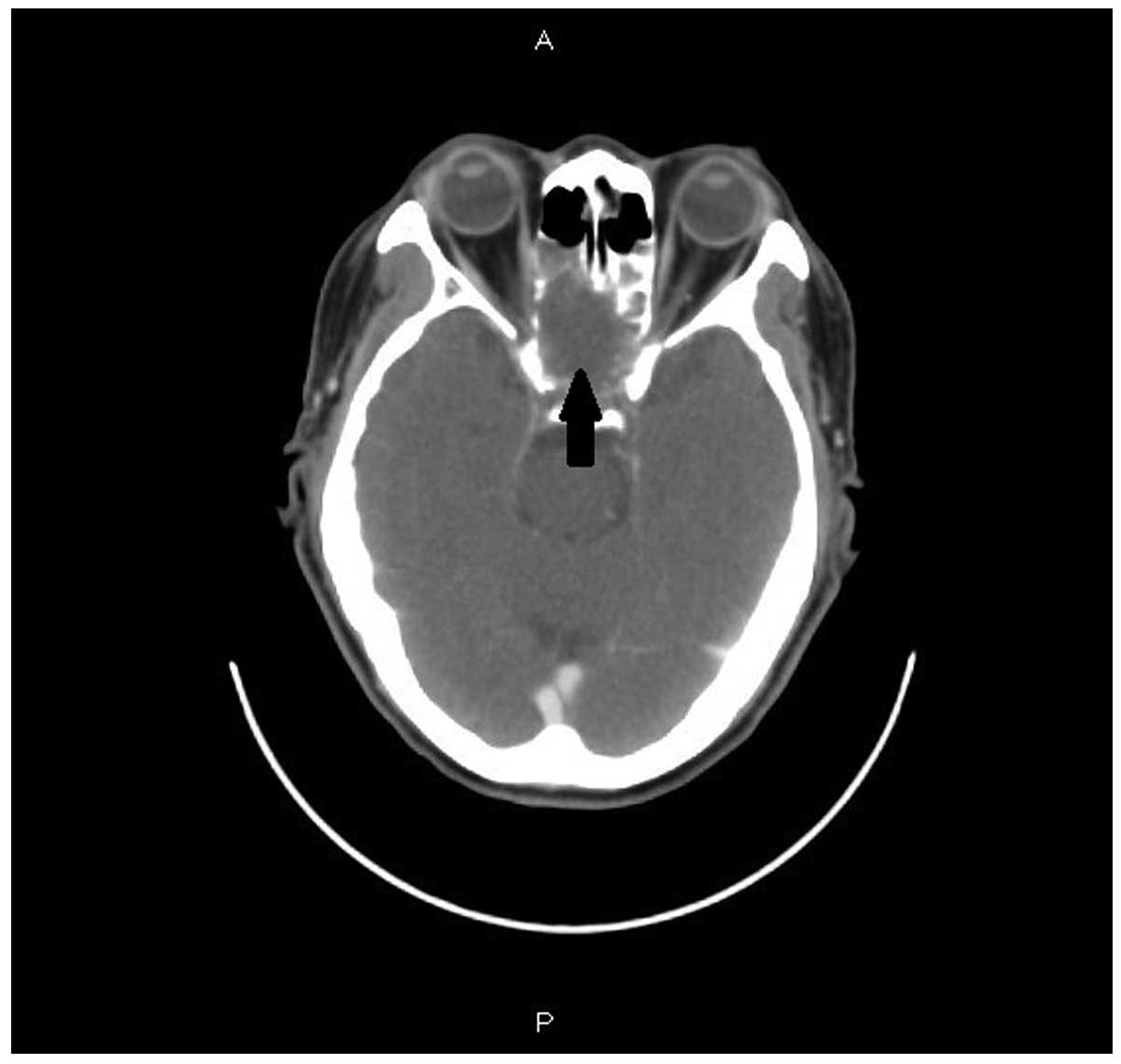
Otolaryngology (Shuang Ho Hospital) for further evaluation. Sinus
endoscopy and computed tomography (CT; light speed VCT scanner; GE
Healthcare, Milwaukee, WI, USA) scans were performed, which
revealed bilateral sinusitis involving the sphenoid sinus, with
nasal polyposis. The ophthalmologist scheduled an urgent head and
neck CT scan, which revealed bilateral ethmoid and sphenoid
sinusitis (Fig. 1). On the suspicion
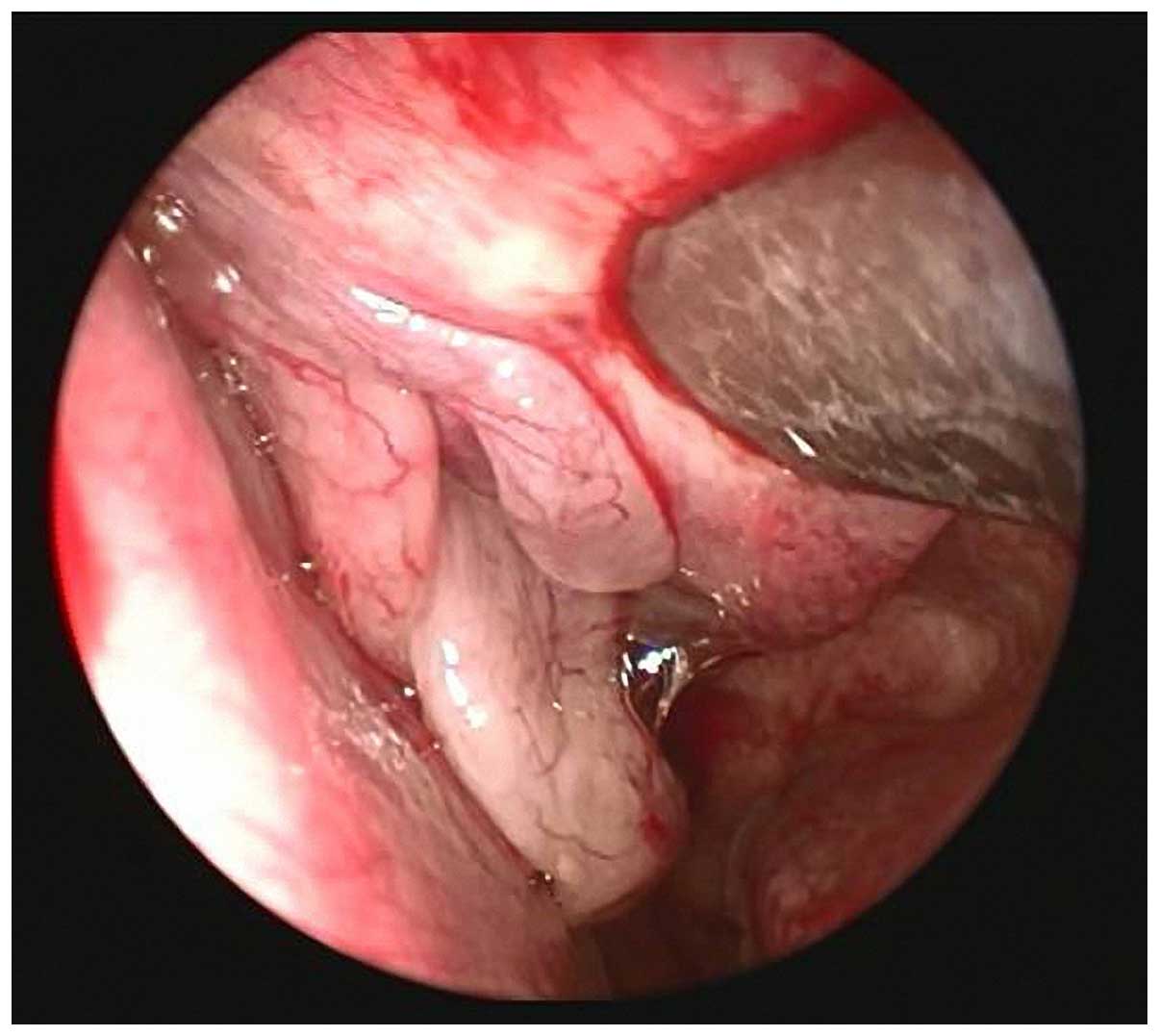
of sinusitis complicated with optic nerve involvement, endoscopic
sinus surgery was suggested and then performed on Febuary 10, 2014.
Bilateral nasal polypoid lesions were observed in the superior
meatus (Fig. 2). The left sphenoid,
ethmoid, frontal and right sphenoid sinuses were explored and
fungus ball-like components were identified. No eschar or necrotic
mucosa was found. Following surgery, the patient reported feeling
that his sight had improved.
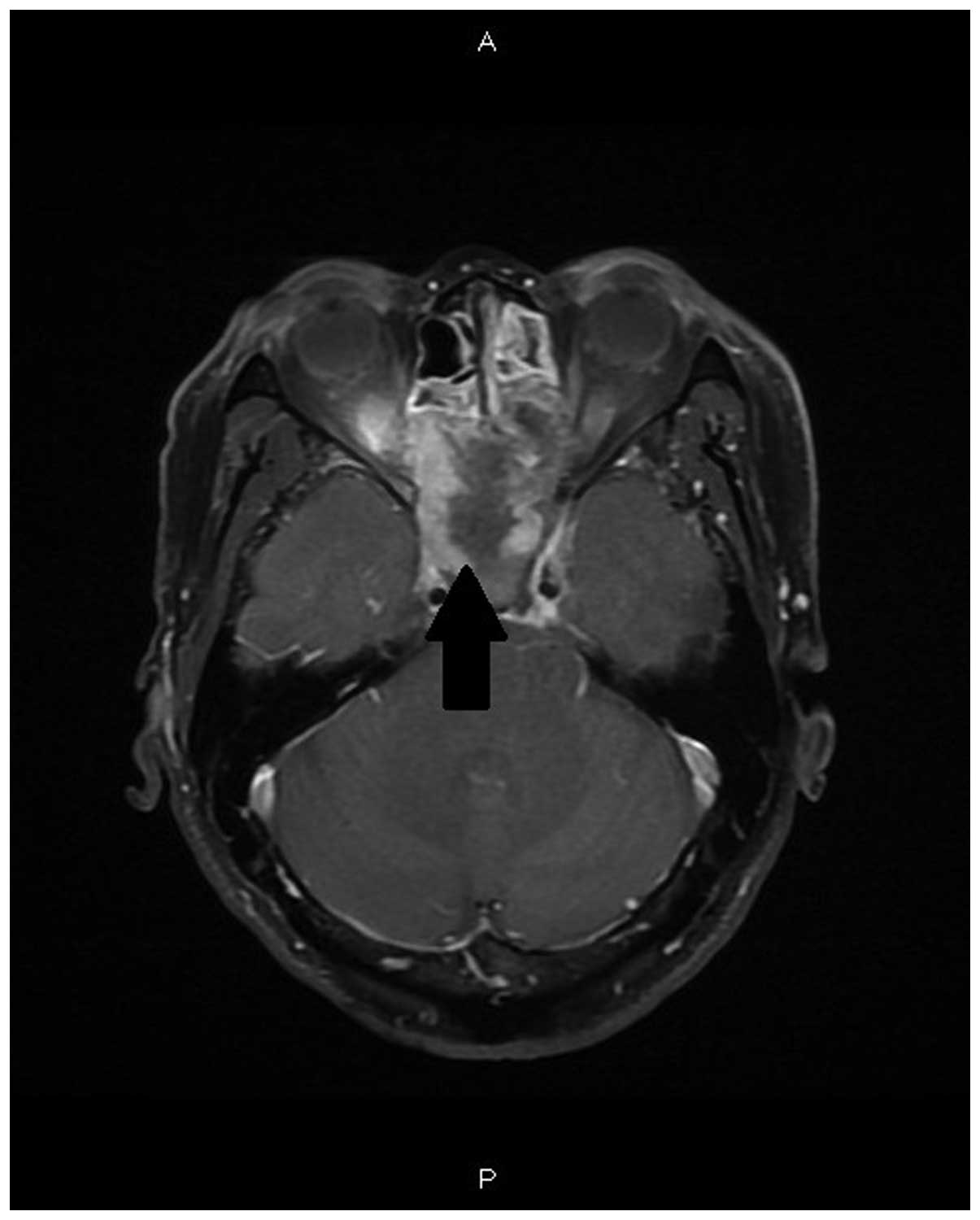
Two days after surgery, the patient again complained
of visual acuity deterioration. A postoperative magnetic resonance
imaging scan of the brain revealed soft-tissue density filling the
sphenoid sinus. The bilateral optic nerves at the intraconal region
were found to be intact; however, optic nerve involvement by the
sphenoid sinusitis was suspected near the bilateral optic canals
and before the optic chiasm (Fig.
3).
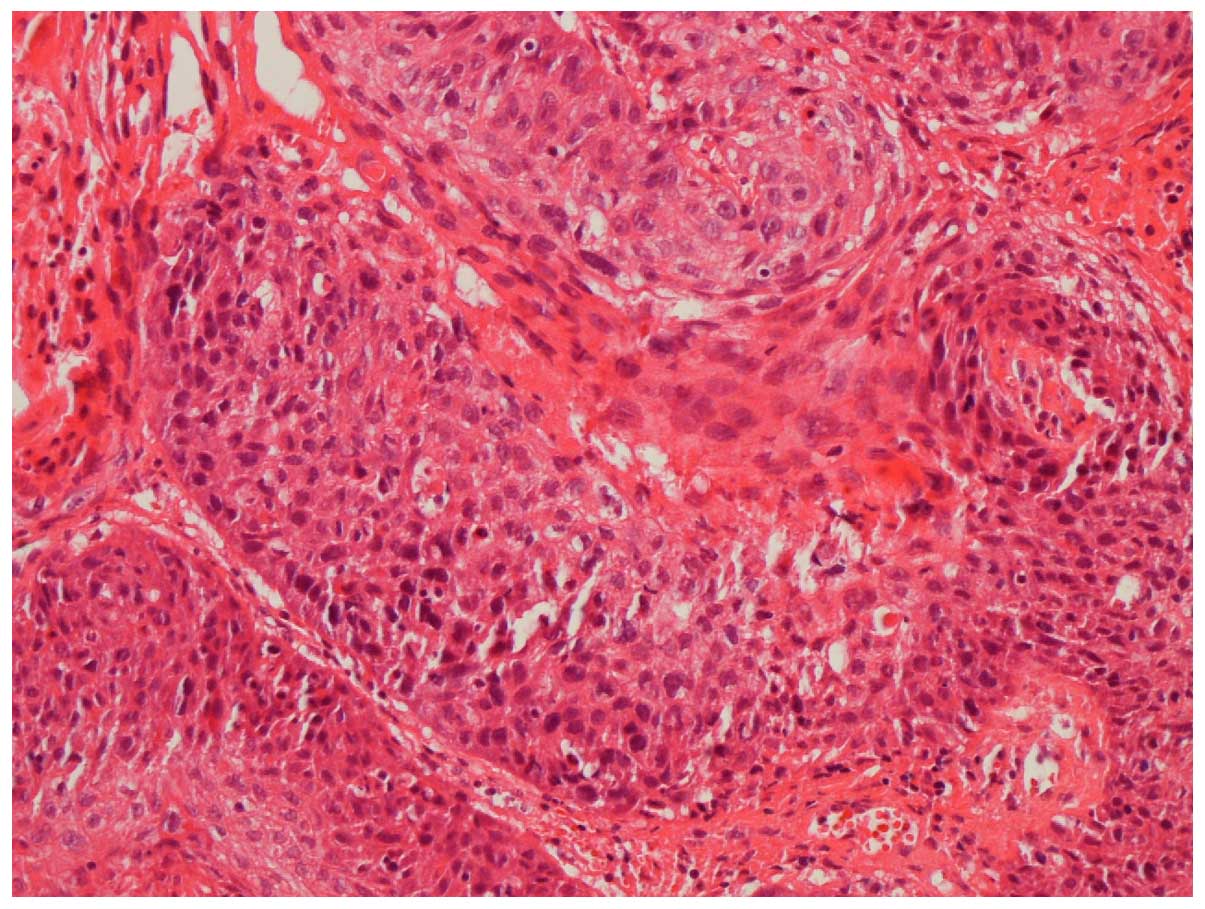
The pathological finding revealed features of
inverted papilloma in a few sections of respiratory mucosa and also
a few pleomorphic spindle cells blending with the dysplastic
squamous cells. Synchronous inverted papilloma of the sphenoid
sinus and SpCC were diagnosed. Hematoxylin and eosin staining
showed the tumor to be composed of pleomorphic spindle cells
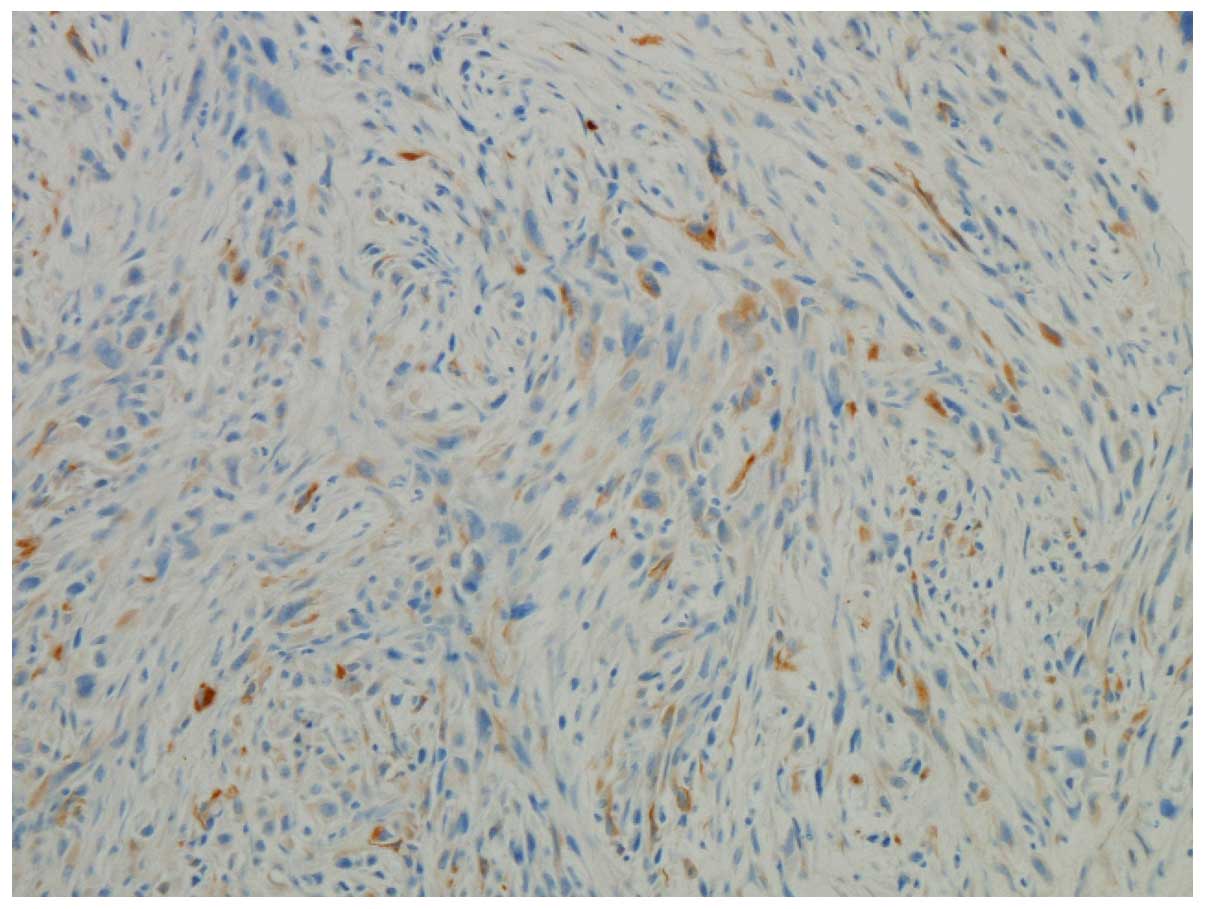
intermixed with dysplastic squamous cells (Fig. 4). An immunohistochemical study was
performed with the use of the Dako EnVision method (Dako,
Carpinteria, CA, USA), and the spindle cells showed focal positive
immunoreactivity for pan cytokeratin (monoclonal mouse anti-human
antibody; catalog no., 760-2135; ready to use; Ventana Medical
Systems, Inc., Tuscon, AZ, USA) (Fig.
5). No fungus was identified.
Ceftriaxone (1,000 mg by intravenous drip every 8 h)
was administered for 7 days and endoscopic sinus surgical
decompression was performed again. The patient was then referred to
the Department of Oncology (Shuang Ho Hospital) and following a
staging workup, received concurrent chemoradiotherapy with 50 mg
weekly cisplatin and 70 Gy radiotherapy in 35 fractions. The left
eye was unresponsive to light following 2 months of concurrent
chemoradiotherapy, and the patient succumbed to bone and liver
metastasis 12 months later.
Discussion
SpCC, also known as sarcomatoid carcinoma,
pseudosarcoma, and carcinosarcoma, is an unusual variant of SCC
that accounts for ~3% of all head and neck SCCs (1). It has been proposed that this biphasic
tumor may arise from conventional SCC by sarcomatous transformation
(2,3).
SpCC most commonly occurs in the fifth and sixth decades of life,
and is associated with a male preponderance. Risk factors for SpCC
include smoking, alcohol consumption and previous radiotherapy
(2,3,5). Among the
organs in the head and neck region, the larynx is the most common
site of involvement, followed by the oral cavity (1). In the sinonasal areas, maxillary sinus
involvement is commonly observed, while sphenoid sinus involvement
is considered rare (Table I)
(2–4,6–18).
 | Table I.Locations of spindle cell
carcinoma. |
Table I.
Locations of spindle cell
carcinoma.
| First author/s,
year | Cases, n | Locationa | Reference |
|---|
| Howell et al,
1978 | 13 | Sinonasal cavity | (6) |
| Leventon and Evans,
1981 | 1 | Maxillary sinus | (7) |
| Benninger et
al, 1992 | 2 | Maxillary sinus | (8) |
| Asbury et al,
1992 | 1 | Maxillary sinus | (9) |
| Berthelet et
al, 1994 | 1 | Nasal cavity | (10) |
| Ahluwalia et
al, 1996 | 1 | Nasal cavity | (11) |
| Mills et al,
1997 | 18 | Sinonasal cavity | (12) |
| Sadaba et al,
2006 | 1 | Maxillary sinus | (13) |
| Howard et al,
2007 | 1 | Maxillary sinus | (4) |
| Kumar et al,
2008 | 1 | Maxillary sinus | (14) |
| Minton and Goyal,
2009 | 1 | Maxillary sinus | (15) |
| Viswanathan et
al, 2010 | 6 | Maxillary sinus | (3) |
| Doshi et al,
2010 | 19 | Sinonasal cavity | (16) |
| Terada, 2011 | 1 | Maxillary sinus and
nasal cavity | (17) |
| Terada and Kawasaki,
2011 | 1 | Nasal cavity | (18) |
| Gupta et al,
2011 | 1 | Nasal cavity | (2) |
Viswanathan et al (3) reported 103 cases of head and neck SpCC,
and found that 46.6% presented with obvious epithelial
differentiation and 33% with epithelial differentiation at the
immunohistochemical level, while 20.4% displayed no evidence of
either. The majority of patients with sinonasal SpCC present with
excessive tearing, nasal obstruction, facial swelling and numbness,
and nasal purulence (2). Orbital
symptoms are less commonly observed (1,2). In
addition, to the best of our knowledge, only one case of sinus SpCC
presenting with orbital apex syndrome has been reported (13). The symptoms of the 45-year-old male
patient included left eyelid swelling, diplopia and proptosis.
Visual acuity was initially 20/20. Imaging scans revealed that a
left maxillary sinus mass had eroded the floor of the left orbit
and extended to the left retrobulbar region, apex of the orbit and
optic chiasm. Orbital involvement appears to be associated with a
poor prognosis, as the left eye of this patient was unresponsive to
light following 2 months of concurrent chemoradiotherapy, and he
succumbed to bone and liver metastasis 12 months later (13).
In contrast to the aforementioned case, the patient
in the present study presented with no obvious signs of gross tumor
invasion into the orbital cavity, despite also initially
complaining of vision loss. Among all sphenoid lesions with ocular
manifestations, benign sphenoid mucoceles are the most commonly
reported, with the majority of the ocular manifestations, including
visual acuity, recovering following lesion resolution (19,20);
however, one case of extramedullar plasmacytoma in the sphenoid
sinus presenting with optic nerve compression failed to regain
visual acuity following pressure relief by surgery (21).
Following a literature review of sinonasal SpCC
cases (Table I) (2–4,6–18), it was
concluded that there does not appear to be an association between
the lesion and the presence of sinonasal inverted papilloma;
however, since the inverted papilloma can potentially transform
into SCC, it is likely that it can also transform into SpCC, as it
is a variant of SCC. We believe that the chronicity of inverted
papilloma is associated with the induction of SpCC transformation.
To the best of our knowledge, this is the first reported case of
inverted papilloma of the synchronous sphenoid sinus and SpCC
presenting with optic nerve compression.
In conclusion, SpCC of sinonasal origin is
relatively rare and clinically aggressive. In the majority of
cases, maxillary sinus involvement was observed, while sphenoid
sinus involvement was more rare. The presentation of orbital
symptoms has been associated with a relatively poor prognosis and,
therefore, the clinical management of such patients should be more
aggressive. The value of surgical decompression in these cases
remains unclear.
References
|
1
|
Thompson LDR: Squamous cell carcinoma
variants of the head and neck. Curr Diagn Pathol. 9:384–396. 2003.
View Article : Google Scholar
|
|
2
|
Gupta S, Santoriello D, Wieczorek R and De
Lacure MD: Spindle cell carcinoma of the nasal cavity. Rare Tumors.
5:102013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Viswanathan S, Rahman K, Pallavi S, Sachin
J, Patil A, Chaturvedi P, D'Cruz A, Agarwal J and Kane SV:
Sarcomatoid (spindle cell) carcinoma of the head and neck mucosal
region: A clinicopathologic review of 103 cases from a tertiary
referral cancer centre. Head Neck Pathol. 4:265–275. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Howard SN, Bond WR, Hong IS and Foss RD:
Right maxillary sinus sarcomatoid carcinoma (sarcomatoidspindle
cell carcinoma). Otolaryngol Head Neck Surg. 137:355–357. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chang NJ, Kao DS, Lee LY, Chang JW, Hou
MM, Lam WL and Cheng MH: Sarcomatoid carcinoma in head and neck: A
review of 30 years of experience-clinical outcomes and
reconstructive results. Ann Plast Surg. 71(Suppl 1): S1–S7. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Howell JH, Hyams VJ and Sprinkle PM:
Spindle cell carcinoma of the nose and paranasal sinuses. Surg
Forum. 29:565–568. 1978.PubMed/NCBI
|
|
7
|
Leventon GS and Evans HL: Sarcomatoid
squamous cell carcinoma of the mucous membranes of the head and
neck: A clinicopathologic study of 20 cases. Cancer. 48:994–1003.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Benninger MS, Kraus D, Sebek B, Tucker HM
and Lavertu P: Head and neck spindle cell carcinoma: An evaluation
of current management. Cleve Clin J Med. 59:479–482. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Asbury L, Candelaria S, Rudak F, Stutzman
CD and Lake DE: High dose rate treatment of a maxillary sarcomatoid
carcinoma: A case report. Med Dosim. 17:129–133. 1992.PubMed/NCBI
|
|
10
|
Berthelet E, Shenouda G, Black MJ,
Picariello M and Rochon L: Sarcomatoid carcinoma of the head and
neck. Am J Surg. 168:455–458. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ahluwalia H and Gupta SC and Gupta SC:
Pathology in focus. Spindle-cell carcinoma of the nasal septum. J
Laryngol Otol. 110:284–287. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mills S, Gaffey M and Frierson H Jr: Armed
Forces Institute Of Pathology: Spindle cell carcinoma. Tumors of
the Upper Aerodigestive Tract and Ear [Atlas Of Tumor Pathology
(AFIP) 3rd Series]. Armed Forces Institute of Pathology.
(Washington, DC). 76–80. 1997.
|
|
13
|
Sadaba LM, Garcia-Layana A, Garcia-Gomez
PJ and Salinas-Alaman A: Sarcomatoid carcinoma and orbital apex
syndrome. Eur J Ophthalmol. 16:608–610. 2006.PubMed/NCBI
|
|
14
|
Kumar M, Bahl A, Sharma DN, Agarwal S,
Halanaik D, Kumar R and Rath GK: Sarcomatoid squamous cell
carcinoma of uterine cervix: Pathology, imaging and treatment. J
Cancer Res Ther. 4:39–41. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Minton TJ and Goyal P: Endoscopic
treatment of a maxillary sinus spindle cell carcinoma. J
Otolaryngol Head Neck Surg. 38:E45–E50. 2009.PubMed/NCBI
|
|
16
|
Doshi DV, Tripathi U, Dave RI, Pandya SJ,
Shukla HK and Parikh BC: Rare tumors of sinonasal track. Indian J
Otolaryngol Head Neck Surg. 62:111–117. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Terada T: Pure sarcomatoid carcinoma of
maxillary sinus and nasal cavity simulating malignant fibrous
histiocytoma. Am J Clin Pathol. 135:128–131. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Terada T and Kawasaki T: Spindle cell
carcinoma of the nasal cavity. Int J Clin Oncol. 16:165–168. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hejazi N, Witzmann A and Hassler W: Ocular
manifestations of sphenoid mucoceles: Clinical features and
neurosurgical management of three cases and review of the
literature. Surg Neurol. 56:338–343. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yoon TM, Kim K and Lim SC: Visual outcome
after endoscopic decompression surgery for sphenoid sinus disease:
How we do it. Clin Otolaryngol. 33:480–484. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ozdemir S, Tarkan O, Tuncer U, Sürmelioğlu
O, Doğrusöz M and Ergin M: A case of extramedullary plasmacytoma in
the sphenoid sinus with unilateral loss of vision. J
Craniomaxillofac Surg. 41:140–143. 2013. View Article : Google Scholar : PubMed/NCBI
|