Introduction
Infection with disseminated varicella zoster virus
(VZV), including cutaneous and visceral dissemination, occurs in
recipients of autologous and allogeneic hematopoietic stem cell
transplantation (HSCT) and in highly immunocompromised patients
(1). The main risk factor for
reactivation of VZV is profound disruption of the cellular immune
response, rather than severity of neutropenia or depletion of
circulating B cells (1). Allogeneic
HSCT recipients carry a 20–50% risk of developing any type of VZV
infection (1,2). The rate of VZV dissemination is 17–36%
(3,4).
However, cases of disseminated VZV in patients undergoing
conventional chemotherapy are rare, with only case reports
published, including a previous case report (5). Other previous cases with abdominal
symptoms and syndrome of inappropriate antidiuretic hormone (SIADH)
have additionally been reported (5–10). As
disseminated VZV has a high mortality rate of up to 50% (11), anti-VZV therapy such as acyclovir
should be immediately commenced. The recommended dose for adults
with VZ is 800 mg oral acyclovir five times daily, or 10 mg/kg
intravenous acyclovir every 8 hours, although higher doses (12–15
mg/kg) are sometimes used for life-threatening infections,
particularly in immunocompromised patients (1). VZV incidence increases markedly after 50
years of age, with two-thirds of herpes zoster (HZ) cases occurring
in individuals aged ≥50 years (12).
One study provided an estimated case fatality rate of 2/100,000 in
patients aged between 45–65 years, and 61/100,000 in patients aged
>65 years old (13). Although
VZV-associated mortality rate is generally low, underlying
comorbidities may increase the severity of the HZ episode and thus
the risk of mortality (14).
Recently, 2 additional patients presented with VZV infection, and
the present study reports these 3 cases of disseminated VZV and
analyzes the risk factors of VZV.
Case report
Case 1
A 61-year-old woman undergoing treatment for grade 2
follicular lymphoma, clinical stage IV, with a low International
Prognostic Index (IPI) score, presented at the National Cancer
Center Hospital (Tokyo, Japan) in December 2013, with severe upper
abdominal pain that had lasted 3 days prior to admission. The
patient had a long history of treatment for follicular lymphoma, as
follows: 6 cycles of cyclophosphamide, doxorubicin, vincristine and
prednisone [CHOP; 750 mg/m2 cyclophosphamide (day 1), 50
mg/m2 doxorubicin (day 1), 1.4 mg/m2
vincristine (day 1), and 100 mg prednisone (days 1–5)] with
rituximab; 1 course of rituximab monotherapy consisting of 8
cycles; 1 cycle of cyclophosphamide, vincristine, procarbazine and
prednisone [C-MOPP; 1 mg vincristine (days 1 and 8), 450 mg
cyclophosphamide (days 1 and 8), and 60 mg prednisone (days 1,2 and
3); procarbazine was not administered]; 5 cycles of bendamustine
(90 mg/m2 on days 1 and 2); and 6 cycles of gemcitabine
(1000 mg/m2 on days 1 and 15). The patient was on day 5
of the second cycle of salvage C-MOPP prior to admission, and had
also been taking 15 mg/day prednisolone for tumor fever since 4
months prior to admission. The cluster of differentiation (CD)4
cell count was 118 cells/mm3 on admission, and had been
<200 cells/mm3 since 10 months prior (normal range,
400–1600 cells/mm3) (Fig.
1). The serum immunoglobulin (Ig)G level was 289 mg/dl and had
been <400 mg/dl since 10 months prior (normal range, 842–1815
mg/dl).
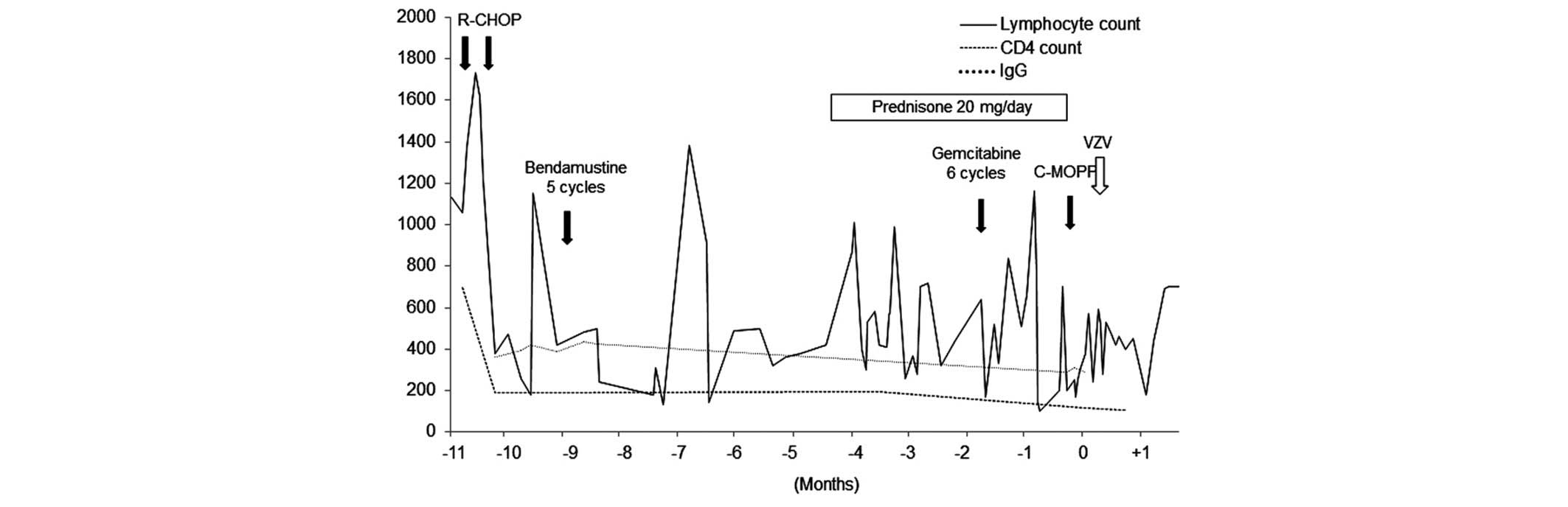 | Figure 1.Clinical course of patient 1. The CD4
count was 118 cells/mm3 on admission, and had been
<200 cells/mm3 for the 10 months prior. The serum IgG
level was 289 mg/dl and had been <400 mg/dl for the 10 months
prior. Lymphocyte count and CD4 count are measured in
cells/mm3 and IgG in mg/dl. CD4, cluster of
differentiation 4; IgG, immunoglobulin G; R-CHOP, cyclophosphamide,
doxorubicin, vincristine and prednisone with rituximab; C-MOPP,
cyclophosphamide, vincristine, procarbazine and prednisone; VZV,
varicella zoster virus. |
On examination, the patient had a slight fever of
37.4°C, but other vital signs were normal. The abdomen was
distended and tender and bowel sounds were diminished. Plain
abdominal X-ray showed dilated small and large bowels, compatible
with ileus, resulting in the suspension of oral intake. A computed
tomography (CT) scan revealed the absence of perforated bowel, but
showed wall thickening in one area of the transverse colon.
Gastrointestinal endoscopy revealed no abnormalities.
On day 4 subsequent to admission, the patient
demonstrated hyponatremia (122 mmol/l), low plasma osmolality (246
mOsm/kg H2O) and high urine osmolality (469 mOsm/kg
H2O), which is compatible with SIADH. At the same time,
the total and direct bilirubin levels started to rise, which
elevated to 4.9 and 3.1 mg/dl, respectively. An abdominal echo
showed no evidence of liver, bile tract, gallbladder or pancreas
abnormalities. On day 5, the neutrophil counts decreased to
480/mm3 and the patient was treated with third
generation cephalosporin antibiotics in case of masked bacterial
infection. Following initiation of treatment with octreotide (300
µg/day) and opioids (fentanyl; 0.96 mg/day), the abdominal pain and
distention were relieved. On day 6, the patient developed
horizontal nystagmus, nausea and delirium. Radiographic findings of
the head showed no focal lesions. Fever persisted, so antibiotics
were switched to piperacillin/tazobactam. On day 9, vesicular skin
lesions appeared on the trunk and extremities of the patient,
suggestive of disseminated HZ virus infection.
Upon starting intravenous acyclovir treatment at a
dose of 1,500 mg/day, the abdominal pain, SIADH and direct
bilirubin levels of the patient improved. Polymerase chain reaction
(PCR) for VZV of the peripheral blood taken prior to treatment
revealed the presence of VZV. Subsequent to 14 days of acyclovir
treatment, the skin lesions began crusting, and with relief of the
symptoms of ileus, the patient began eating again. The patient was
discharged on day 31 post-admission.
Case 2
A 72-year-old man diagnosed with peripheral T-cell
lymphoma, not otherwise specified, serum human T-lymphotropic virus
type I negative, clinical stage IVA, presented at the National
Cancer Center Hospital (Tokyo, Japan) in June 2011, with a
scattered vesicular rash accompanied by abdominal pain. The patient
had been treated with 7 cycles of C-MOPP [1 mg vincristine (days 1
and 8), 650 mg/m2 cyclophosphamide (days 1 and 8), and
60 mg prednisone (days 1, 2 and 3); procarbazine was not
administered] and had a past history of VZV infection limited to
the left limb. The previous localized VZV infection occurred in
March 2011, and lasted for 1 week. The infection was treated with
oral valacyclovir at a dose of 1000 mg 3 times daily for 7 days.
The patient had also been taking prednisolone at a dose of 20
mg/day for 3 months prior to admission. The lymphocyte count of the
patient was 160 cells/mm3 on admission, and had been
fluctuating between 200 and 800 cells/mm3 for 1 year
(normal range, 1098–2671 cells/mm3). Although data on
the CD4 cell count was not available, from the low overall
lymphocyte count, it was considered that the CD4 cell count had
been <200 cells/mm3 for ≥6 months (Fig. 2).
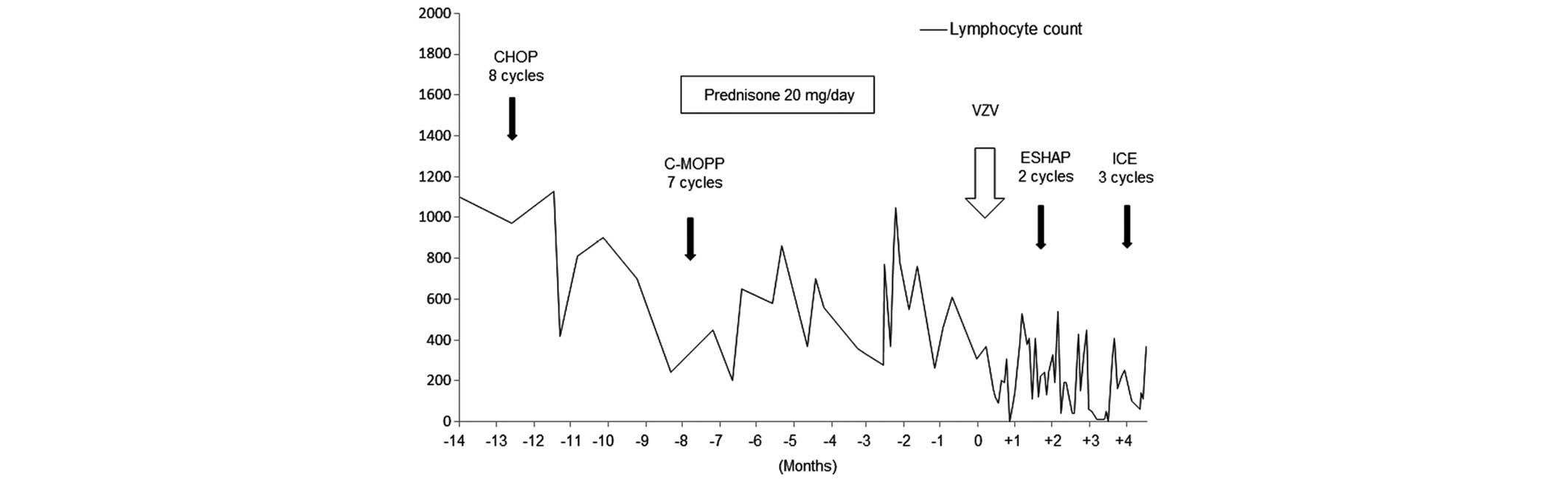 | Figure 2.Clinical course of patient 2. The
lymphocyte count was 160 cells/mm3 on admission, and it
had been fluctuating between 200 and 800 cells/mm3 for 1
year. Lymphocyte count is measured in cells/mm3. CHOP,
cyclophosphamide, doxorubicin, vincristine and prednisone; C-MOPP,
cyclophosphamide, vincristine, procarbazine and prednisone; VZV,
varicella zoster virus; ESHAP, etoposide, methylprednisolone,
cytarabine and cisplatin; ICE, ifosfamide, carboplatin and
etoposide. |
On examination, VZV infection was suspected at
admission, and 750 mg/day acyclovir, a reduced dose considering the
decreased renal function of the patient, was administered
immediately. On day 5 of treatment, the vesicles began to crust.
Abdominal pain also diminished, and on day 14 of treatment,
acyclovir therapy was terminated.
Case 3
This case has been previously reported in detail
(5). A 65-year-old woman undergoing
treatment for diffuse large B-cell lymphoma of the stomach,
clinical stage III, low IPI score, presented at the National Cancer
Center Hospital (Tokyo, Japan) in October 2004, with severe
abdominal pain that had lasted 2 days prior to admission. The
patient had had been treated with 3 cycles of CHOP [750
mg/m2 cyclophosphamide (day 1), 50 mg/m2
doxorubicin (day 1), 1.4 mg/m2 vincristine (day 1), and
100 mg prednisone (days 1–5)], followed by locoregional radiation
therapy at a total dose of 40.5 Gy (administered over 28
fractions), and the patient had completed the regimen 2 months
prior to the present admission. The peripheral blood CD4 cell count
was 135 cells/mm3 and had been low for >5 months. The
serum IgG level at admission was 962 mg/dl, and had been 1527 mg/dl
on February 12, 2004.
On admission, laboratory data revealed serum
hyponatremia (122 mmol/l) with low serum osmolality (262 mOsm/kg
H2O) and high urine osmolality (532 mOsm/kg
H2O), and the patient was diagnosed with SIADH. On day 6
subsequent to admission, a subtle vesicular skin lesion on the
abdomen and back of the patient developed, which indicated
disseminated HZ virus infection. Subsequent to sampling the serum
and cerebrospinal fluid (CSF) to test for VZV DNA, the patient was
immediately treated with intravenous acyclovir 1,500 mg/day.
The abdominal symptoms of the patient improved
dramatically on the following day and laboratory data reflected the
recovery of SIADH, when VZV DNA was found to be present in the
serum and CSF. The skin lesions began to crust and the patient was
discharged on day 14.
Discussion
The present study reported 3 cases of unusual
manifestation of disseminated VZV infection in patients with
lymphoma. Theses cases were unusual due to the concomitant symptoms
of visceral infection. All patients initially presented with
abdominal pain and 2 patients had SIADH, while 1 patient also
presented with acute hepatitis. Second, all patients were
undergoing conventional chemotherapy alone without HSCT. The
clinical characteristics and past therapy history for the present
patients are listed in Tables I and
II.
 | Table I.Patient Characteristics. |
Table I.
Patient Characteristics.
| Patient | Gender | Age at VZV diagnosis,
years | Primary disease | Past history | Diagnosis of VZV
infection | Symptoms | Treatment |
|---|
| 1 | Female | 61 | FL, grade 2, Stage
IV, IPI low risk | Gastric cancer
(surgical cure) | Blood: VZV-PCR
(+) | Abdominal pain,
intestinal psuedoobstruction SIADH D-Bil elevation P-Amy
elevation | ACV iv 1500 mg/day
for 14 days |
| 2 | Male | 72 | PTCL-NOS, Stage IV,
IPI high risk | VZV infection in
limited area | Blood: VZV-PCR
(+) | Abdominal pain
generalized vesicular skin lesion | ACV iv 750 mg/day for
10 days |
| 3 | Female | 65 | DLBCL, Stage II, IPI
low risk | N.P. | Blood and
cerebrospinal fluid: VZV-PCR (+) | Abdominal pain SIADH
AST/ALT elevation | ACV iv 1500 mg/day
for 5 days 750 mg/day for 9 days |
| Table II.Patient treatment history. |
Table II.
Patient treatment history.
|
| Chemotherapy
regimen |
|
|---|
|
|
|
|
|---|
| Patient | 1st line | 2nd line | 3rd line | 4th line | 5th line | 6th line | Prednisolone dose,
mg/day |
|---|
| 1 | R-CHOP, 6 cycles | Rituximab, 8
cycles | C-MOPP, 1 cycle | Bendamustine, 5
cycles | Gemcitabine, 6
cycles | C-MOPP without
procarbazine, 2 cycles | 20 |
| 2 | CHOP, 8 cycles | C-MOPP, 7 cycles | ESHAP, 2 cycles | ICE, 3 cycles | – | – | 20 |
| 3 | CHOP, 3 cycles and
RT, 40 Gy |
| – |
|
|
|
|
|
|
| – |
| – | – | – | – |
Abdominal pain is considered to occur due to direct
viral infection of the enteric nervous system (ENS), resulting from
2 different pathways. Viremia, in which circulating T cells carry
VZV, and axonal transport from dorsal root ganglia are potential
routes enabling VZV to gain access to the ENS. This may result in
multiple intestinal disorders of unknown pathogenesis, such as
irritable bowel syndrome, inflammatory bowel disease, idiopathic
gastroparesis and idiopathic pseudo-obstruction (15). Acute colonic pseudo-obstruction is a
severe and uncommon finding that is associated with
immunodeficiency (15,16).
The exact cause and mechanism of SIADH remains to be
eludicated. However, this syndrome is hypothesized to result from
central nervous system (CNS) infection, which may be responsible
for stimulation of ADH release from the neurohypophyseal system
(6,17). Out of the present 2 patients with
SIADH, patient 3 showed evidence of VZV infection in the CSF. In
patient 1, although lumbar puncture was not performed, the patient
presented with horizontal nystagmus, nausea and delirium, which
suggested involvement of the CNS.
Abdominal pain and SIADH reflect viscerally
disseminated viral disease, which may occur without evidence of
cutaneous dissemination. There are studies reporting cases with
abdominal symptoms and SIADH preceding skin rash (5–10). These
viscerally disseminated VZV infections are sometimes fatal, with up
to 50% mortality (11). Due to the
high mortality rate, clinicians should consider VZV, and if VZV is
suspected, treatment should be started as soon as possible upon
sampling of VZV DNA (18). The
present patients were treated successfully, prior to the result of
the PCR test being obtained or prior to the symptoms becoming
uncontrollable.
Disseminated VZV is observed more frequently in HSCT
recipients compared with those patients undergoing conventional
chemotherapy strategies. Risk factors of clinically relevant
reactivation are considered to be profound disruption of the
cellular immune response. This risk increases with intensity and
duration of functional T-cell suppression (19). In HSCT recipients, the rate of VZV
infection is 20–50% (1–3). Among those infected, the rate of
visceral or cutaneous dissemination is 17–36% (3,4). However,
although remaining a minority, disseminated VZV infection in those
undergoing conventional chemotherapy is additionally accumulating
(5,8,20).
It was notable that all patients had low CD4 or
lymphocyte counts for a long time and 2 patients had taken oral
steroid therapy. Oral steroids, which can cause prolonged decreases
in lymphocyte count, may have contributed to development of this
unusual form of VZV.
Prophylactic antiviral therapy for HSCT recipients
has been proposed (21–23) and low-dose acyclovir of 200 mg/day or
valacyclovir 500 mg/day, 3 times/week for at least 1 year is
warranted (24,25). Previously, those treated with newer
agents, such as alemtuzumab, bendamustine or the purine analogs
fludarabine, 2-chlorodeoxyadenosine (2-CDA) and pentostatin, which
cause major cellular immunodeficiency, were also indicated for
antiviral prophylaxis (26). It is
crucial to consider that visceral disseminated VZV may occur in
patients undergoing conventional chemotherapy alone. Although
cutaneous dissemination is not life-threatening, viscerally
disseminated VZV seeding the intestine, liver, lung and CNS may be
fatal (17).
In patients with a prolonged low lymphocyte count or
long-term use of steroids, prophylactic acyclovir treatment may be
required.
References
|
1
|
Arvin A and Abendroth A: VZV:
Immunobiology and host response. Human Herpesviruses: Biology,
Therapy, and Immunoprophylaxis. Arvin A, Campadelli-Fiume G,
Mocarski E, Moore PS, Roizman B, Whitley R and Yamanishi K:
Cambridge University Press. (Cambridge). 700–712. 2007. View Article : Google Scholar
|
|
2
|
Blennow O, Fjaertoft G, Winiarski J,
Ljungman P, Mattsson J and Remberger M: Varicella-zoster
reactivation after allogeneic stem cell transplantation without
routine prophylaxis-the incidence remains high. Biol Blood Marrow
Transplant. 20:1646–1649. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Koc Y, Miller KB, Schenkein DP, Griffith
J, Akhtar M, DesJardin J and Snydman DR: Varicella zoster virus
infections following allogeneic bone marrow transplantation:
Frequency, risk factors and clinical outcome. Biol Blood Marrow
Transplant. 6:44–49. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Locksley RM, Flournoy N, Sullivan KM and
Meyers JD: Infection with varicella-zoster virus after marrow
transplantation. J Infect Dis. 152:1172–1181. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ohara F, Kobayashi Y, Akabane D, Maruyama
D, Tanimoto K, Kim SW, Watanabe T and Tobinai K: Abdominal pain and
syndrome of inappropriate antidiuretic hormone secretion as a
manifestation of visceral varicella zoster virus infection in a
patient with non-Hodgkin's lymphoma. Am J Hematol. 82:4162007.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ingraham IE Jr, Estes NA, Bern MM and
DeGirolami PC: Disseminated varicella-zoster virus infection with
the syndrome of inappropriate antidiuretic hormone. Arch Intern
Med. 143:1270–1271. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vinzio S, Lioure B, Enescu I, Schlienger
JL and Goichot B: Severe abdominal pain and inappropriate
antidiuretic hormone secretion preceding varicella-zoster virus
reactivation 10 months after autologous stem cell transplantation
for acute myeloid leukaemia. Bone Marrow Transplant. 35:525–527.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Szabo F, Horvath N, Seimon S and Hughes T:
Inappropriate antidiuretic hormone secretion, abdominal pain and
disseminated varicella-zoster virus infection: An unusual triad in
a patient 6 months post mini-allogeneic peripheral stem cell
transplant for chronic myeloid leukemia. Bone Marrow Transplant.
26:231–233. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rau R, Fitzhugh CD, Baird K, Cortez KJ, Li
L, Fischer SH, Cowen EW, Balow JE, Walsh TJ, Cohen JI and Wayne AS:
Triad of severe abdominal pain, inappropriate antidiuretic hormone
secretion and disseminated varicella-zoster virus infection
preceding cutaneous manifestations after hematopoietic stem cell
transplantation: Utility of PCR for early recognition and therapy.
Pediatr Infect Dis J. 27:265–268. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Grant RM, Weitzman SS, Sherman CG, Sirkin
WL, Petric M and Tellier R: Fulminant disseminated Varicella Zoster
virus infection without skin involvement. J Clin Virol. 24:7–12.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
David DS, Tegtmeier BR, O'Donnell MR, Paz
IB and McCarty TM: Visceral varicella-zoster after bone marrow
transplantation: Report of a case series and review of the
literature. Am J Gastroenterol. 93:810–813. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yawn BP, Saddier P, Wollan PC, St Sauver
JL, Kurland MJ and Sy LS: A population-based study of the incidence
and complication rates of herpes zoster before zoster vaccine
introduction. Mayo Clin Proc. 82:1341–1349. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brisson M and Edmunds WJ: Epidemiology of
varicella-zoster virus in England and Wales. J Med Virol. 70(Suppl
1): S9–S14. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gil A, Gil R, Alvaro A, San Martín M and
González A: Burden of herpes zoster requiring hospitalization in
Spain during a seven-year period (1998-2004). BMC Infect Dis.
9:552009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen JJ, Gershon AA, Li Z, Cowles RA and
Gershon MD: Varicella zoster virus (VZV) infects and establishes
latency in enteric neurons. J Neurovirol. 17:578–589. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pui JC, Furth EE, Minda J and Montone KT:
Demonstration of varicella-zoster virus infection in the muscularis
propria and myenteric plexi of the colon in an HIV-positive patient
with herpes zoster and small bowel pseudo-obstruction (Ogilvie's
syndrome). Am J Gastroenterol. 96:1627–1630. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Moses A and Streeten D: Disorders of the
neurohypophysis. Syndromes associated with vasopressin excess.
Harrison's Principles of Internal Medicine. Isselbacher K,
Braunwald E, Wilson J, Martin J, Fauci A and Kasper D: 2:(13th).
McGraw-Hill. (New York, NY). 1928–1930. 1994.
|
|
18
|
Ishizaki Y, Tezuka J, Ohga S, Nomura A,
Suga N, Kuromaru R, Kusuhara K, Mizuno Y, Kasuga N and Hara T:
Quantification of circulating varicella zoster virus-DNA for the
early diagnosis of visceral varicella. J Infect. 47:133–138. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Storek J, Gooley T, Witherspoon RP,
Sullivan KM and Storb R: Infectious morbidity in long-term
survivors of allogeneic marrow transplantation is associated with
low CD4 T cell counts. Am J Hematol. 54:131–138. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Okamoto A, Abe A, Okamoto M, Kobayashi T,
Terazawa T, Inaguma Y, Tokuda M, Yanada M, Morishima S, Kanie T, et
al: Severe hepatitis associated with varicella zoster virus
infection in a patient with diffuse large B cell lymphoma treated
with rituximab-CHOP chemotherapy. Int J Hematol. 96:516–520. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kanda Y, Mineishi S, Saito T, Saito A,
Yamada S, Ohnishi M, Chizuka A, Niiya H, Suenaga K, Nakai K, et al:
Long-term low-dose acyclovir against varicella-zoster virus
reactivation after allogeneic hematopoietic stem cell
transplantation. Bone Marrow Transplant. 28:689–692. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Erard V, Guthrie KA, Varley C, Heugel J,
Wald A, Flowers ME, Corey L and Boeckh M: One-year acyclovir
prophylaxis for preventing varicella-zoster virus disease after
hematopoietic cell transplantation: No evidence of rebound
varicella-zoster virus disease after drug discontinuation. Blood.
110:3071–3077. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kawamura K, Wada H, Yamasaki R, Ishihara
Y, Sakamoto K, Ashizawa M, Sato M, Machishima T, Terasako K, Kimura
S, et al: Prophylactic role of long-term ultra-low-dose acyclovir
for varicella zoster virus disease after allogeneic hematopoietic
stem cell transplantation. Int J Infect Dis. 19:26–32. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Oshima K, Takahashi T, Mori T, Matsuyama
T, Usuki K, Asano-Mori Y, Nakahara F, Okamoto S, Kurokawa M and
Kanda Y: One-year low-dose valacyclovir as prophylaxis for
varicella zoster virus disease after allogeneic hematopoietic stem
cell transplantation. A prospective study of the Japan Hematology
and Oncology Clinical Study Group. Transpl Infect Dis. 12:421–427.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Asano-Mori Y, Kanda Y, Oshima K, Kako S,
Shinohara A, Nakasone H, Sato H, Watanabe T, Hosoya N, Izutsu K, et
al: Long-term ultra-low-dose acyclovir against varicella-zoster
virus reactivation after allogeneic hematopoietic stem cell
transplantation. Am J Hematol. 83:472–476. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sandherr M, Einsele H, Hebart H, Kahl C,
Kern W, Kiehl M, Massenkeil G, Penack O, Schiel X, Schuettrumpf S,
et al: Antiviral prophylaxis in patients with haematological
malignancies and solid tumours: Guidelines of the Infectious
diseases working party (AGIHO) of the German society for hematology
and oncology (DGHO). Ann Oncol. 17:1051–1059. 2006. View Article : Google Scholar : PubMed/NCBI
|














