Introduction
Multiple myeloma (MM) is a malignant plasma cell
neoplasm characterized by plasma cells accumulating in the bone
marrow and subsequent destruction of bone, symptoms of bone marrow
failure and organ dysfunction (1). MM
is responsible for ~1% of all cancers and 10% of hematological
cancers (2,3). The median age at diagnosis of MM is 70
years (3). The median survival of
patients with MM was <1 year prior to the introduction of
alkylating agents (3). The
introduction of novel agents, including bortezomib, thalidomide and
lenalidomide, for the treatment of MM patients has significantly
improved clinical outcomes (1–3). However,
a concerning finding has been the increase in the incidence of
secondary malignancies (4–7). Previous studies have demonstrated that
MM patients have a higher risk of secondary myeloid malignancies
than the general population (4–6). To the
best of our knowledge, secondary B cell malignancy in MM patients
is seldom studied. In addition, acute lymphoblastic leukemia (ALL)
is often perceived as a pediatric malignancy because the peak
incidence occurs between 1 and 4 years of age. However, the
incidence of ALL has increased in the older population (8).
The present authors previously reported 3 cases of
MM who developed lymphoblastic leukemia after exposure to a variety
of agents (9). The present study
reports the case of a patient who developed B-cell lymphoblastic
leukemia 38 months after the initial diagnosis of MM. A brief
review of the literature is also provided. Written informed consent
was obtained from the patient for the publication of this case
report and any accompanying images.
Case report
Clinical characteristics
A 66-year-old male was admitted to The First
Affiliated Hospital of Sun Yat-sen University (Guangzhou, China) in
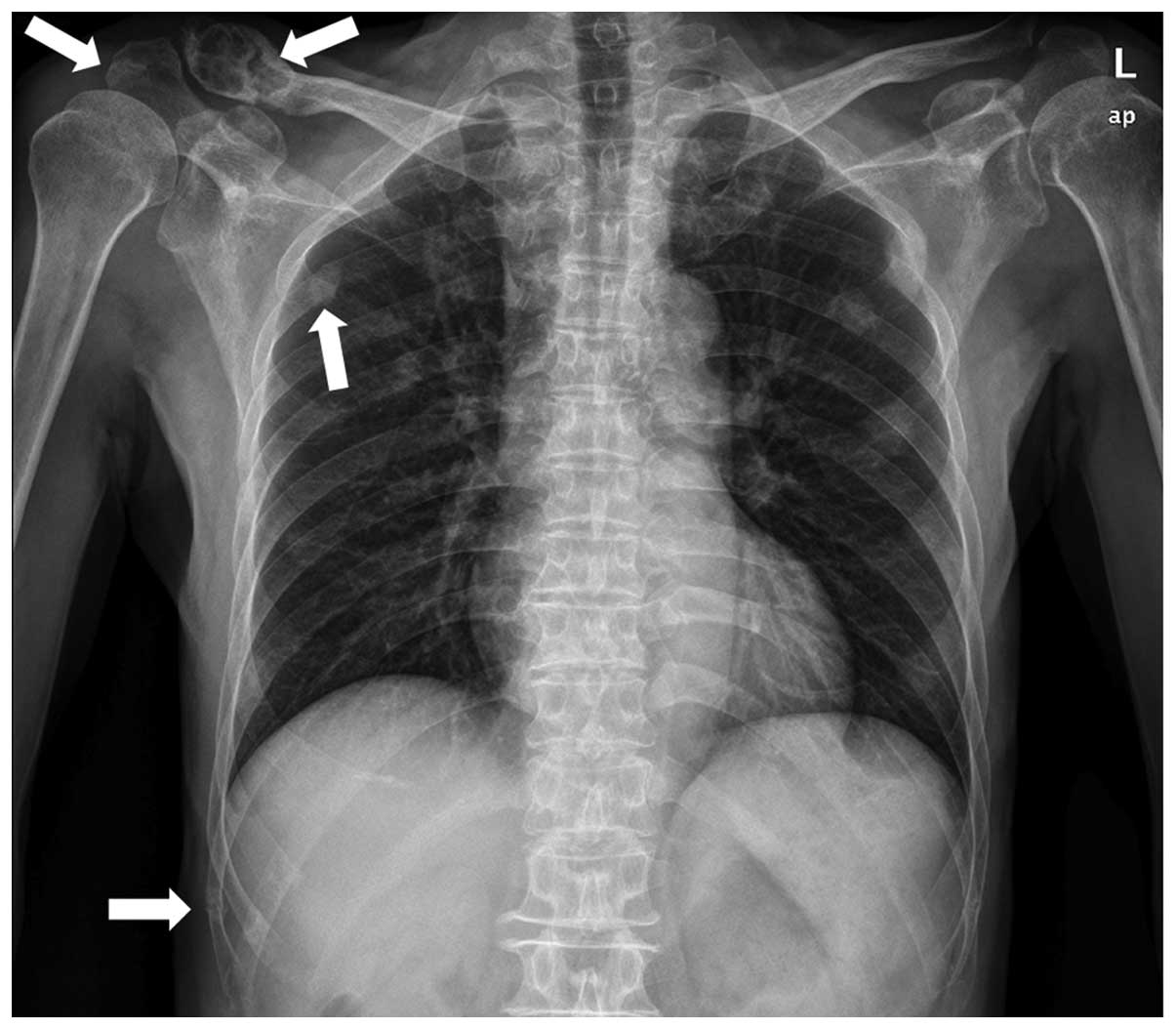
June 2010 due to bone pain. A metastatic bone survey (MBS) revealed
focal osteolytic bone lesions in the costal bones, spine, pelvis,
clavicle and scapular of the right side (Fig. 1). Complete blood counts showed normal
results for white blood cells (4.68×109 cells/l; normal
range, 4.00–10.00×109 cells/l) hemoglobin (130 g/l;
normal range, 120–160 g/l) and platelet count (172×109
cells/l; normal range, 100–300×109 cells/l). A blood
smear showed a rouleaux formation of red blood cells. Serum protein
electrophoresis revealed the presence of a monoclonal protein in
the γ region, subsequently identified as immunoglobulin (Ig) A and
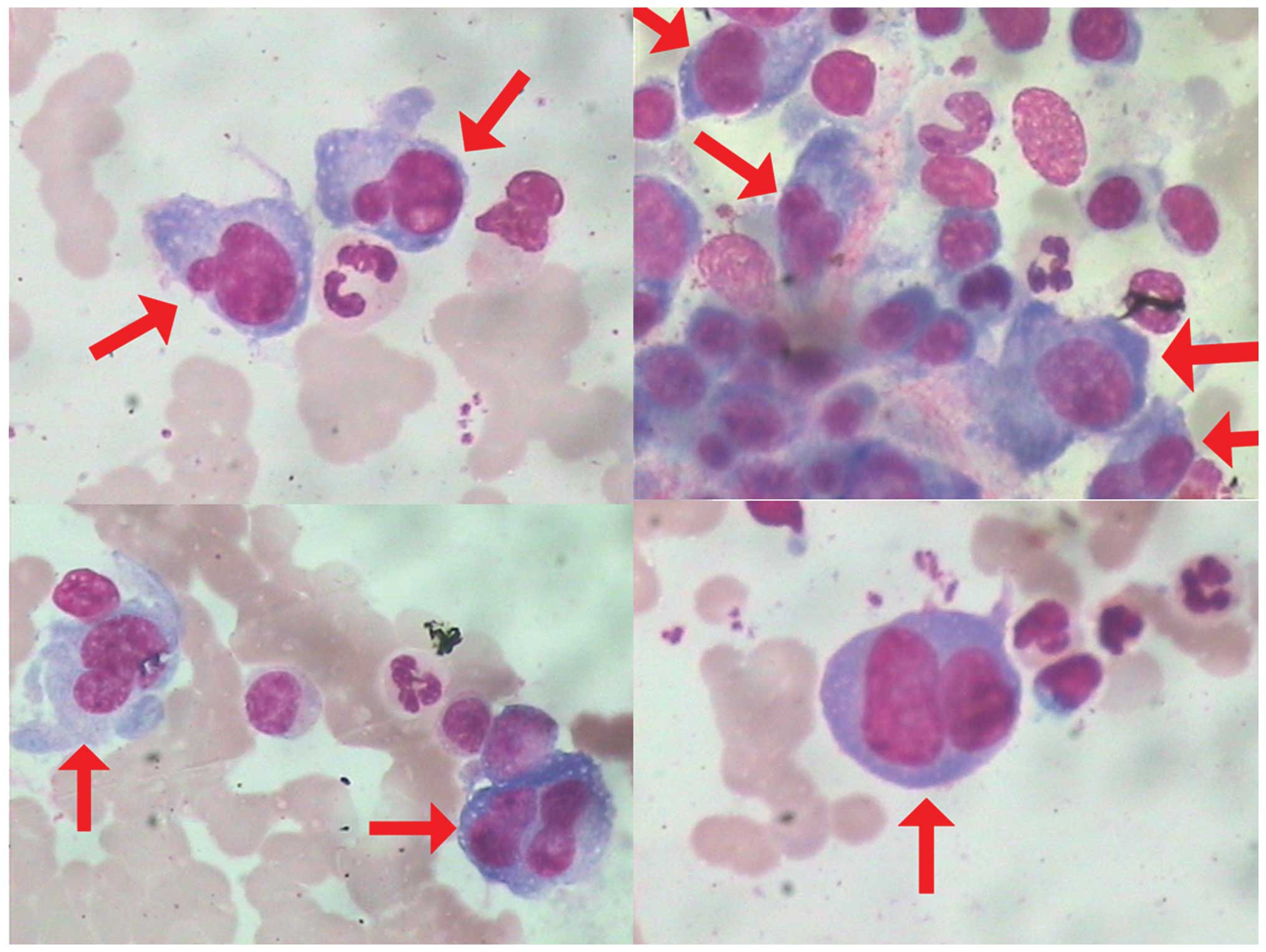
κ light chain. A total of 16.00% plasma cells (normal range,
0.00–0.02%) were found in the bone marrow smear (Fig. 2).
The results of flow cytometry analysis were
consistent with the presence of clonal plasma cells. Flow cytometry
analysis of the surface and cytoplasm markers of the plasma cells
was performed on erythrocytes-lysed ethylenediaminetetraacetic acid
(EDTA)-anti-coagulated bone marrow samples using a 6-color panel of
ready to use antibodies and isotype controls conjugated to
fluorescein isothiocyanate (FITC), phycoerythrin (PE), peridinin
chlorophyll (PerCP), PE-cyanine 7 (Cy7), allophycocyanin (APC)
and/or APC-Cy7 (BD Biosciences, San Diego, CA, USA) and the
“Duo-Lyse” program of the FACS™ Lyse Wash Assistant (BD
Biosciences, Franklin Lakes, NJ, USA) according to the following
antibody combinations: For plasma cells analysis, i)
anti-CD38/CD56/CD19/CD20/CD138/CD45; ii) anti-cytoplasmic
(c)κ/cλ/CD19/CD138/CD38/CD45; iii) anti-CD38/CD54/CD138/CD45; and
iv) anti-CD38/CD45/CD56/CD19/CD20 were used, while for lymphocyte
analysis, i) anti-CD10/CD34/human leukocyte antigen-antigen D
related/CD45; ii) anti-CD20/CD22/CD45/CD5/CD19; iii)
anti-CD15/CD117/CD14/CD45/CD19; iv) anti-CD56/CD13/CD33/CD45/CD19;
v) anti-cCD3/myeloperoxidase (MPO)/CD79a/CD45; and vi)
anti-CD2/CD7/CD45/CD19/CD3 were used (Fig. 3 and Table
I). The total Bence-Jones protein level in a 24-h urine
collection was 1,740 mg (reference value, negative). Anti-nuclear
antibody and serological tests (Epstein-Barr, hepatitis B and C
viruses, cytomegalovirus and human immunodeficiency virus) were
negative. As a result of all these findings, the patient was
diagnosed with MM (Durie-Salmon IIA) (10).
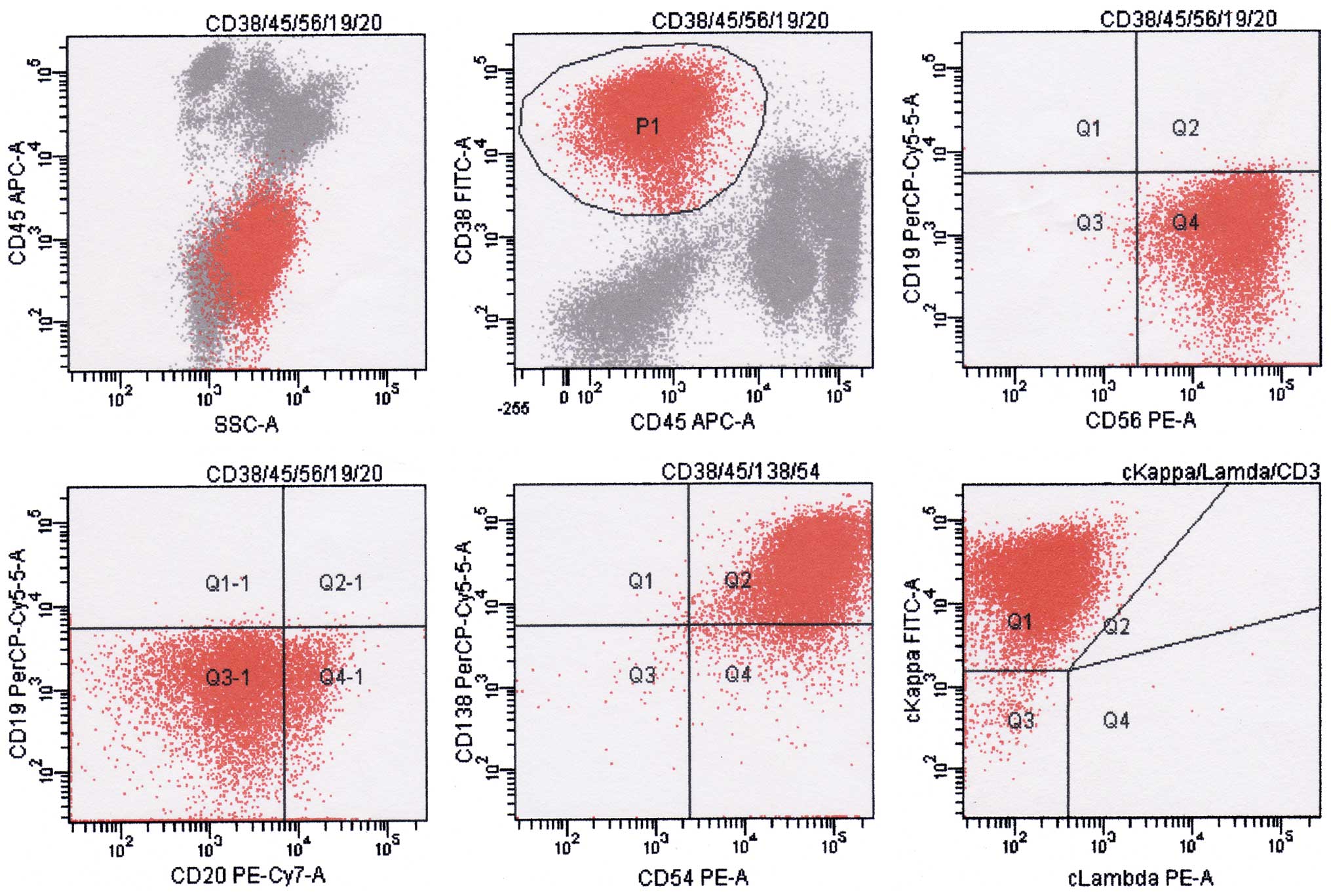 | Figure 3.Result of flow cytometry analysis at
diagnosis. P1 indicates abnormal plasma cells; the phenotype was
positive for CD38, CD138, CD56, CD54 and cκ light chain, and
negative for CD45, CD19 and CD20. Flow cytometry analysis of the
plasma cells surface and cytoplasm markers was performed on
erythrocytes-lysed ethylenediaminetetraacetic acid-anti-coagulated
bone marrow samples using the “Duo-Lyse” program of the BC FACS™
Lyse Wash Assistant according to the following combinations of
antibodies: i) Anti-CD38/CD56/CD19/CD20/CD138/CD45; ii)
anti-cκ/cλ/CD19/CD138/CD38/CD45; iii) anti-CD38/CD54/CD138/CD45;
and iv) anti-CD38/CD45/CD56/CD19/CD20. The data were analyzed with
BD FACSCanto™. The axes of the graphs represent fluorescence
intensity data collected in pulse-area measurements and plotted on
a logarithmic scale. CD, cluster of differentiation; c,
cytoplasmic; A, area; SSC, side scatter; APC, allophycocyanin; PE,
phycoerythrin; Cy, cyanine; PerCP, peridinin chlorophyll; FITC,
fluorescein isothiocyanate; Q, quadrant. |
 | Table I.Antibodies used for flow
cytometry. |
Table I.
Antibodies used for flow
cytometry.
| Antibodies | Catalogue number | Concentration (µl/100
µl) |
|---|
|
Anti-CD38-FITC/CD56-PE-Cy/CD19-PerCP-Cy5.5 | 341132 | 20 |
| Anti-CD20-PE-Cy7 | 335793 | 5 |
| Anti-CD38
(HB-7)-APC | 345807 | 5 |
| Anti-CD54-PE | 555511 | 20 |
|
Anti-CD138-PerCP-Cy5.5 | 341087 | 20 |
| Anti-κ-FITC/λ-PE | 349516 | 20 |
| Anti-IgM-FITC | 555782 | 20 |
| Anti-IgG-FITC | 555786 | 20 |
| Anti-CD19
(SJ25C1)-APC | 340437 | 5 |
| Anti-CD22-PE | 347577 | 20 |
| Anti-CD34
(8G12)-PE | 348057 | 20 |
| Anti-CD10
(HI10a)-FITC | 340925 | 20 |
| Anti-CD20-FITC | 347673 | 20 |
| Anti-CD45-APC | 340943 | 5 |
| Anti-CD45
(2D1)-PerCP-Cy5.5 | 347464 | 20 |
| Anti-HLA-DR-APC | 559866 | 20 |
|
Anti-CD3-FITC/MPO-PE/CD79a-PerCP-Cy5.5 | 340961 | 20 |
| Anti-CD20-FITC | 555622 | 20 |
| Anti-CD2
(S5.2)-FITC | 347593 | 20 |
| Anti-CD3-PE-Cy7 | 341091 | 5 |
| Anti-CD5-APC | 340583 | 5 |
| Anti-CD7-PE | 340581 | 20 |
| Anti-MPO-FITC | 340580 | 20 |
| Anti-CD13-PE | 347837 | 20 |
| Anti-CD33-APC | 551378 | 20 |
| Anti-CD117-PE | 555714 | 5 |
| Anti-CD117
(104D2)-PerCP-Cy5.5 | 333944 | 20 |
| Anti-CD56-FITC | 340410 | 20 |
| Anti-CD15-FITC | 555401 | 20 |
Treatment process
Treatment was commenced in June 22, 2010. At first,
the patient was administered a bortezomib and dexamethasone regimen
for 2 cycles (cycle 1: 2.0 mg bortezomib on days 1, 4, 7 and 11,
and 20 mg/day dexamethasone on days 1, 2, 4, 5, 7, 8, 11 and 12,
every 28 days; and cycle 2: 2.0 mg bortezomib on days 1, 8, 15 and
22, and 20 mg/day dexamethasone on days 1, 2, 8, 9, 15, 16, 22 and
23, every 28 days). The patient achieved complete remission
(Figs. 4 and 5). Subsequent to obtaining written informed
consent, lenalidomide (10 mg/day) was administered as maintenance
therapy on days 1–21 every 28 days since September 15, 2010.
However, due to economic reasons, lenalidomide was stopped 2 months
later according to the patient's wishes. Therefore, a vincristine,
pirarubicin, dexamethasone and melphalan regimen (0.5 mg/day
vincristine, 10 mg/day pirarubicin, 20 mg/day dexamethasone and 12
mg/day melphalan, on days 1–4) was administered every 28 days as
consolidation therapy in November 16, 2010. After 1 cycle, the
melphalan was out of stock, and a vincristine, pirarubicin and
dexamethasone regimen (0.5 mg vincristine, 10 mg pirarubicin and 20
mg dexamethasone, on days 1–4, every 28 days) was administered in
December 27, 2010, for 1 cycle instead. Thalidomide (200 mg/day)
was used as maintenance therapy from February 9, 2011, to September
13, 2013, when the patient was admitted to hospital again due to
serious fatigue that had persisted for >10 days.
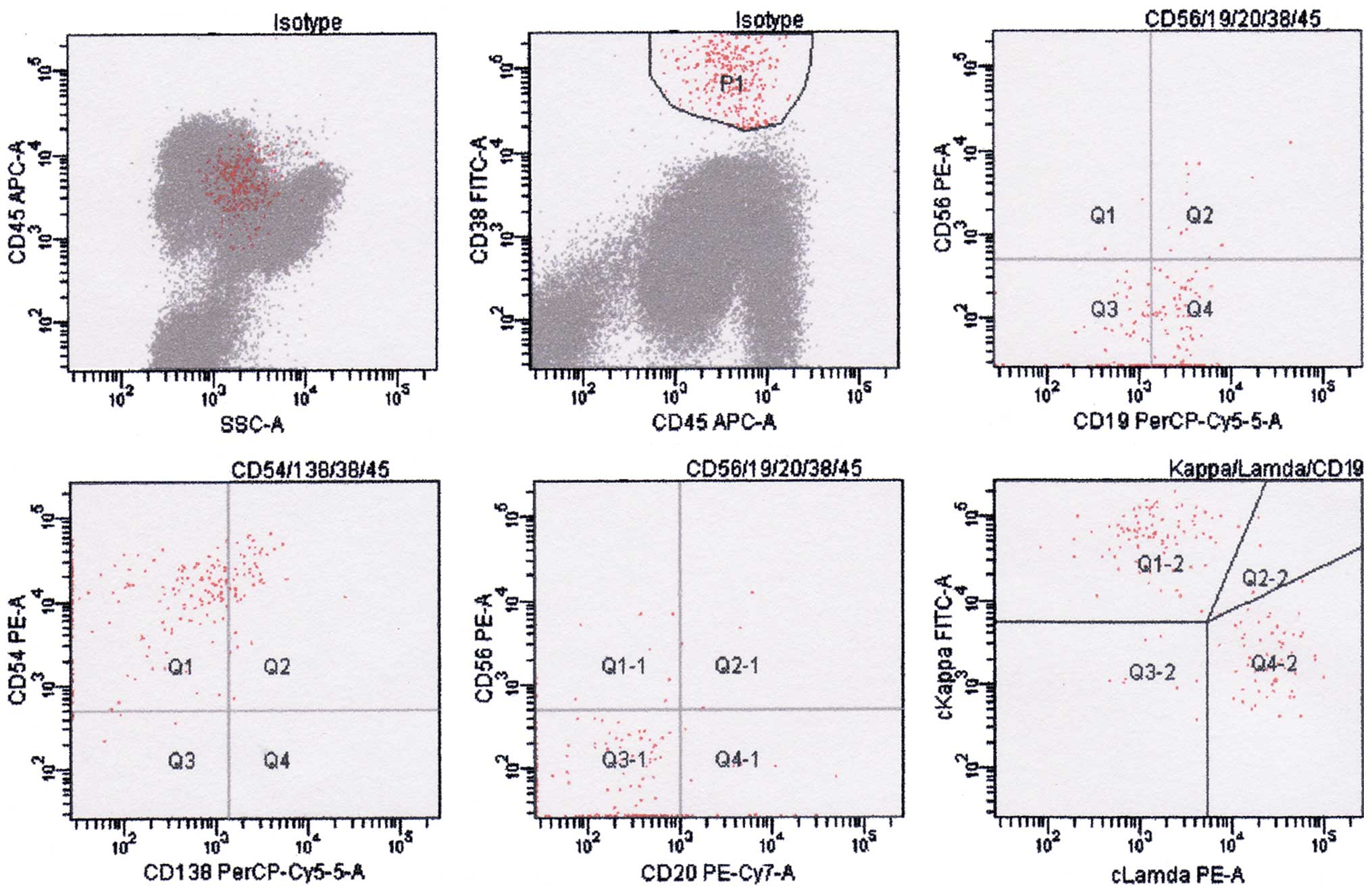 | Figure 5.Result of flow cytometry analysis
after treatment. P1 indicates plasma cells; the phenotype was
positive for CD38, CD138, CD45, CD19 and CD54, and negative for
CD56 and CD20. Flow cytometry analysis of the plasma cells surface
and cytoplasm markers was performed on erythrocytes-lysed
ethylenediaminetetraacetic acid-anti-coagulated bone marrow samples
using the “Duo-Lyse” program of the BC FACS™ Lyse Wash Assistant
according to the following combinations of antibodies: i)
Anti-CD38/CD56/CD19/CD20/CD138/CD45; ii)
anti-cκ/cλ/CD19/CD138/CD38/CD45; iii) anti-CD38/CD54/CD138/CD45;
and iv) anti-CD38/CD45/CD56/CD19/CD20. The data were analyzed with
BD FACSCanto™. The axes of the graphs represent fluorescence
intensity data collected in pulse-area measurements and plotted on
a logarithmic scale. CD, cluster of differentiation; c,
cytoplasmic; A, area; SSC, side scatter; APC, allophycocyanin; PE,
phycoerythrin; Cy, cyanine; PerCP, peridinin chlorophyll; FITC,
fluorescein isothiocyanate; Q, quadrant. |
Secondary lymphoblastic leukemia
At this time, the patient's blood counts showed a
low white blood cell count of 3.05×109/l, while the
hemoglobin level (140 g/l) and platelet count
(178×109/l) were normal. The serum protein level was
74.8 g/l (normal range 60.0–80.0 g/l; albumin, 44.8 g/l (normal
range, 40.0–55.0 g/l); and globulin, 30 g/l (normal range, 20–30
g/l). Immunoelectrophoresis showed no monoclonal increase in serum
Ig (IgA, 1.52 g/l). The patient exhibited elevated levels of
β2-microglobulin (2,358.1 µg/l; normal range, 0–2,400 µg/l), liver
enzymes [alanine transaminase, 64 U/l (normal range, 0–40 U/l); and
aspartate transaminase, 76 U/l (normal range, 0–40 U/l)] and
creatinine (77 µmol/l; normal range, 53–106 µmol/l), and a normal
calcium level (2.31 mmol/l; normal range, 2.25–2.75 mmol/l).
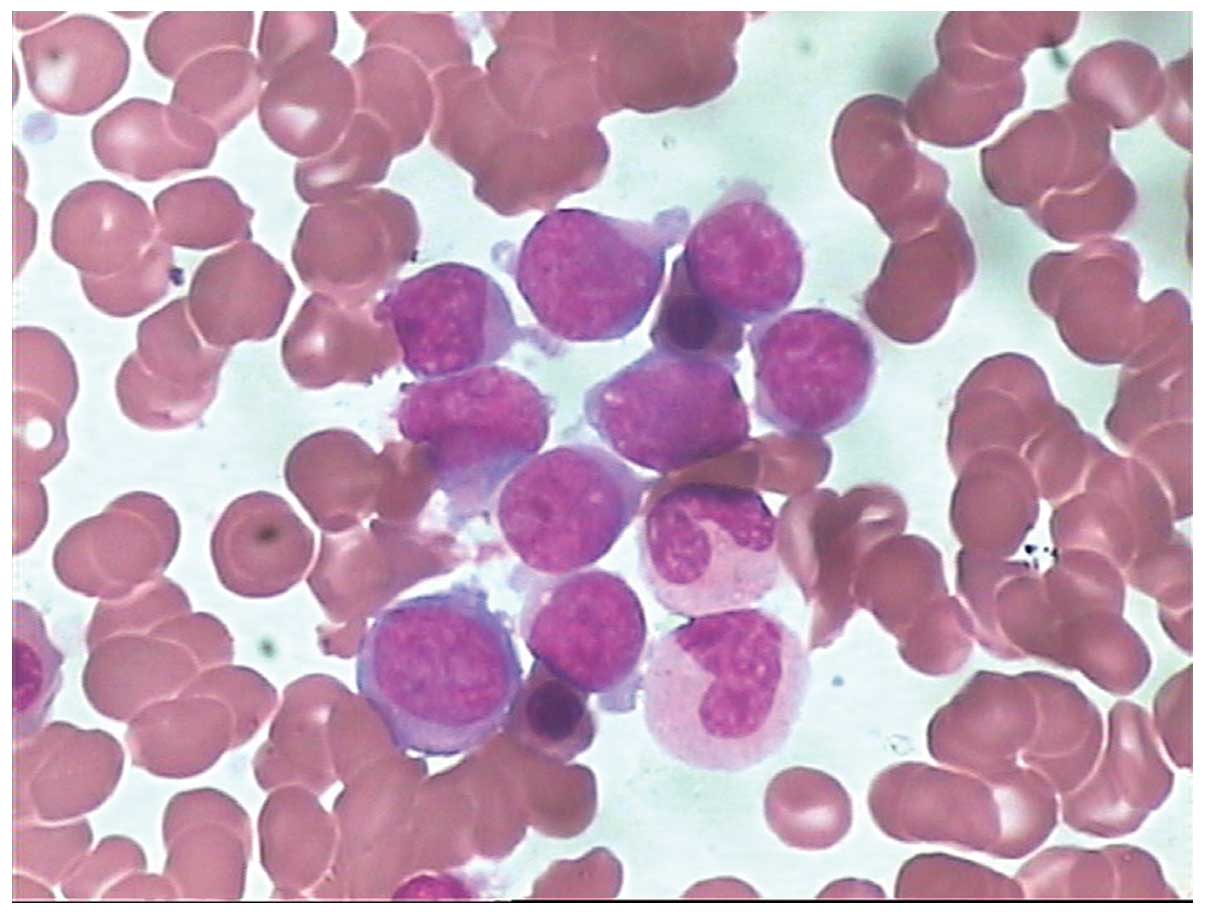
Lymphoblasts accounted for 62% of nucleated cells in
the patient's bone marrow smear (Fig.
6). The results of flow cytometry analysis [positive for CD45,
CD19, CD22, CD34 and CD79a(±); and negative for CD38, CD138, CD56
and CD54] were consistent with the presence of clonal lymphoblast
(Fig. 7). Flow cytometry analysis of
the lymphoblast surface and cytoplasm markers was performed on
erythrocytes-lysed EDTA-anti-coagulated bone marrow samples using a
6-color panel of antibodies (FITC/PE/PerCP/PE-Cy7/APC/APC-Cy7) and
the “Duo-Lyse” program of the of the FACS™ Lyse Wash Assistant
according to the following combinations of antibodies: i)
Anti-CD10/CD34/CD19/CD20/CD22/CD45 and ii)
anti-cIgM/CD79a/CD34/CD19/CD45. For each antibody, negative
staining levels were set by comparison with an isotype matched
control. A cutoff of 20% was usually accepted as evidence of
antigen expression (+). A positive percentage between 10 and 20%
was usually accepted as evidence of antigen expression (±).
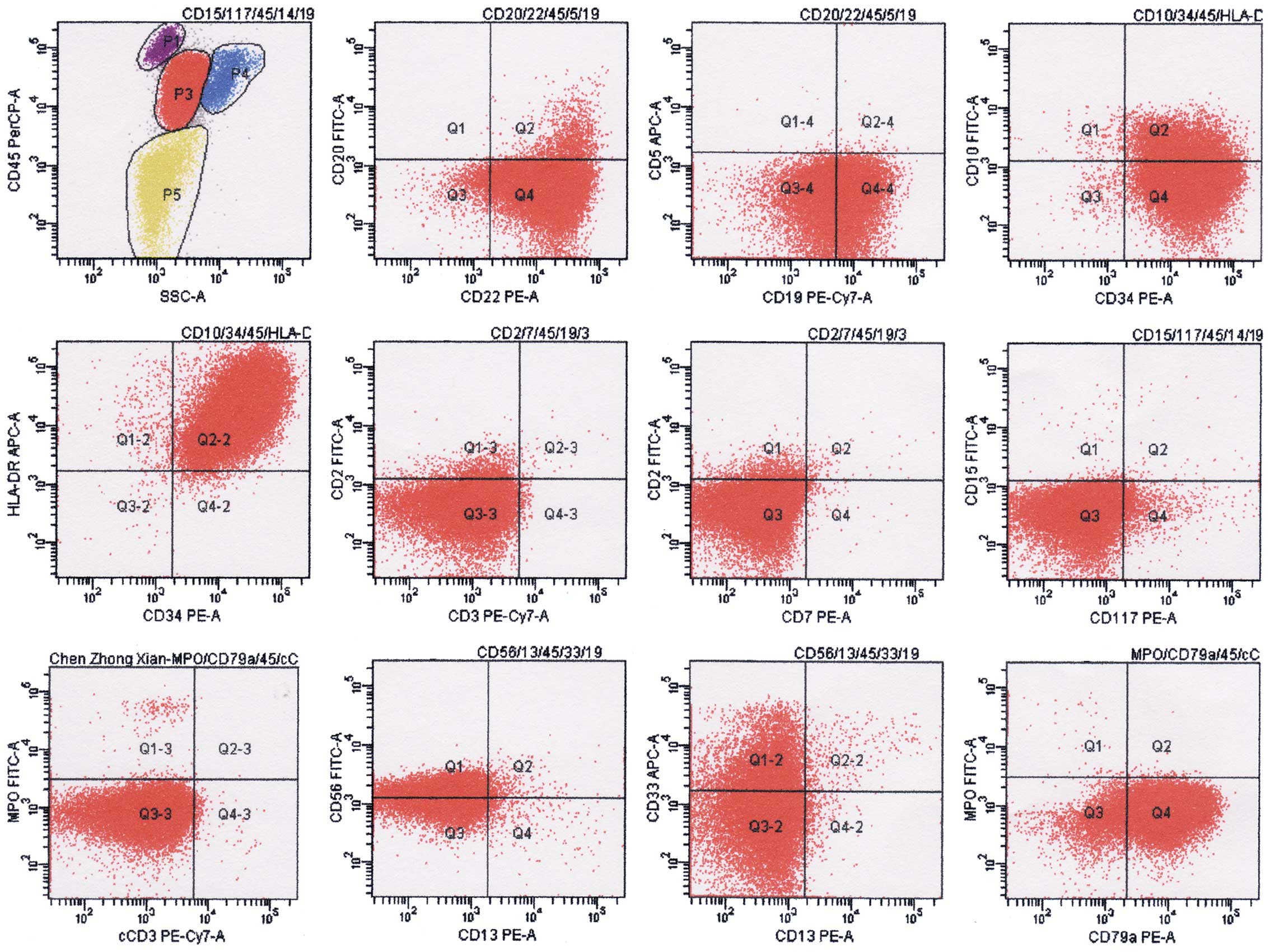 | Figure 7.Result of flow cytometry analysis at
the diagnosis of secondary malignancy. P3 indicate lymphoblasts;
the phenotype was positive for CD19, CD22, CD79a, CD34, HLA-DR,
CD56, CD10(±) and CD33(±); negative for MPO, cCD3, CD20, CD5, CD2,
CD3, CD7, CD117, CD15 and CD13. Flow cytometry analysis of the
plasma cells surface and cytoplasm markers was performed on
erythrocytes-lysed ethylenediaminetetraacetic acid-anti-coagulated
bone marrow samples using the “Duo-Lyse” program of the BC FACS™
Lyse Wash Assistant according to the following combinations of
antibodies: i) Anti-CD10/CD34/HLA-DR/CD45; ii)
anti-CD20/CD22/CD45/CD5/CD19; iii) anti-CD15/CD117/CD14/CD45/CD19;
iv) anti-CD56/CD13/CD33/CD45/CD19; v) anti-cCD3/MPO/CD79a/CD45; and
vi) anti-CD2/CD7/CD45/CD19/CD3. The data were analyzed with BD
FACSCanto™. The axes of the graphs represent fluorescence intensity
data collected in pulse-area measurements and plotted on a
logarithmic scale. CD, cluster of differentiation; c, cytoplasmic;
A, area; SSC, side scatter; APC, allophycocyanin; PE,
phycoerythrin; Cy, cyanine; PerCP, peridinin chlorophyll; FITC,
fluorescein isothiocyanate; MPO, myeloperoxidase; HLA-DR, human
leukocyte antigen-antigen D related; Q, quadrant. |
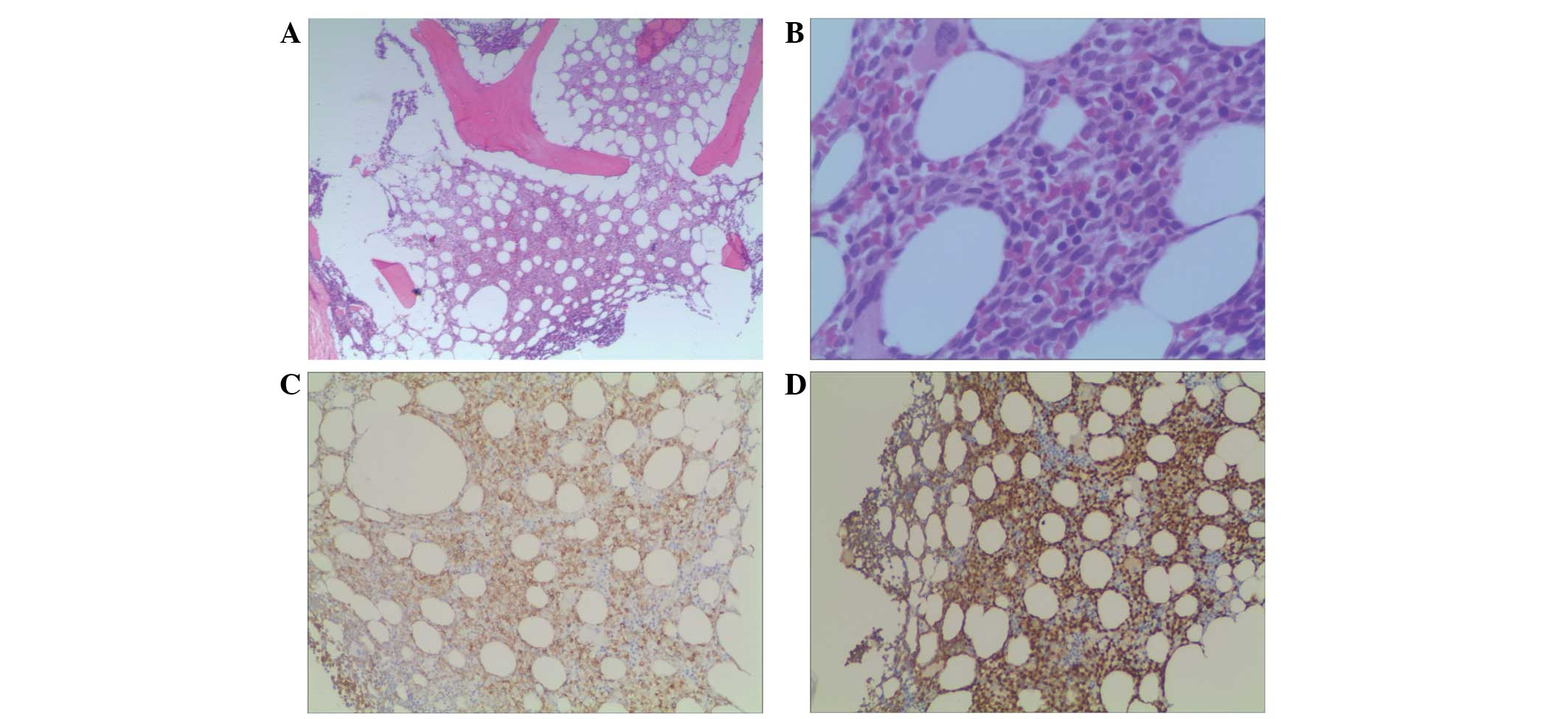
Biopsy revealed a diffuse growth pattern of
lymphoblasts in the bone marrow, and immunohistochemistry showed
the following results: Terminal deoxynucleotidyl transferase(+),
CD34(+), CD79a(±), CD3(−), CD5(−), MPO(−), CD56(−), CD138(−),
cyclin D1(−), κ(−) and λ(−) (Fig. 8).
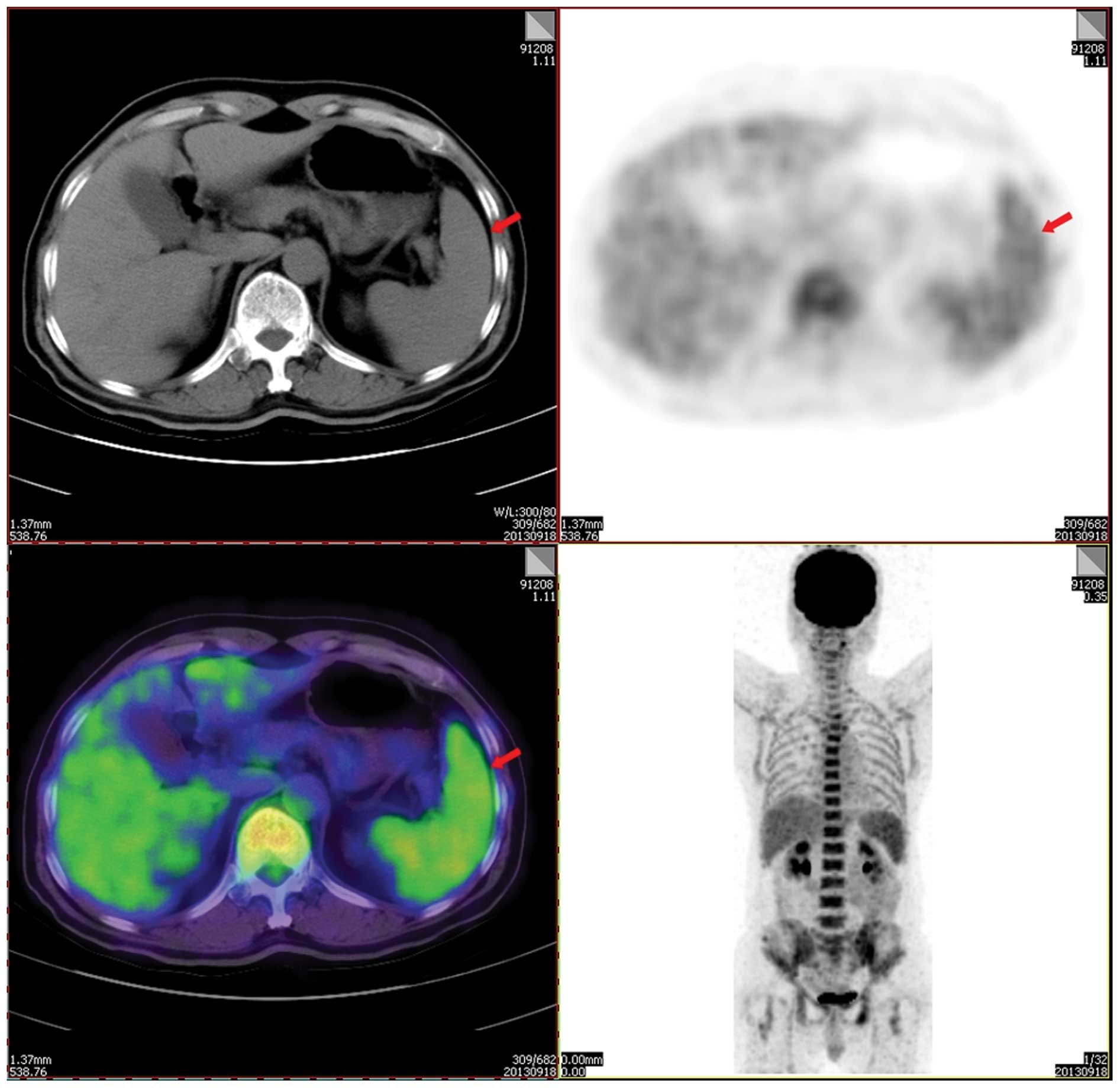
MBS showed that focal bone lesions remained, and positron emission
tomography-computed tomography revealed an elevated maximum
standardized uptake value of fluorodeoxyglucose in the axial bone
(including the skull and the vertebral column; maximum standardized
uptake value, 3.6) and the spleen (maximum standardized uptake
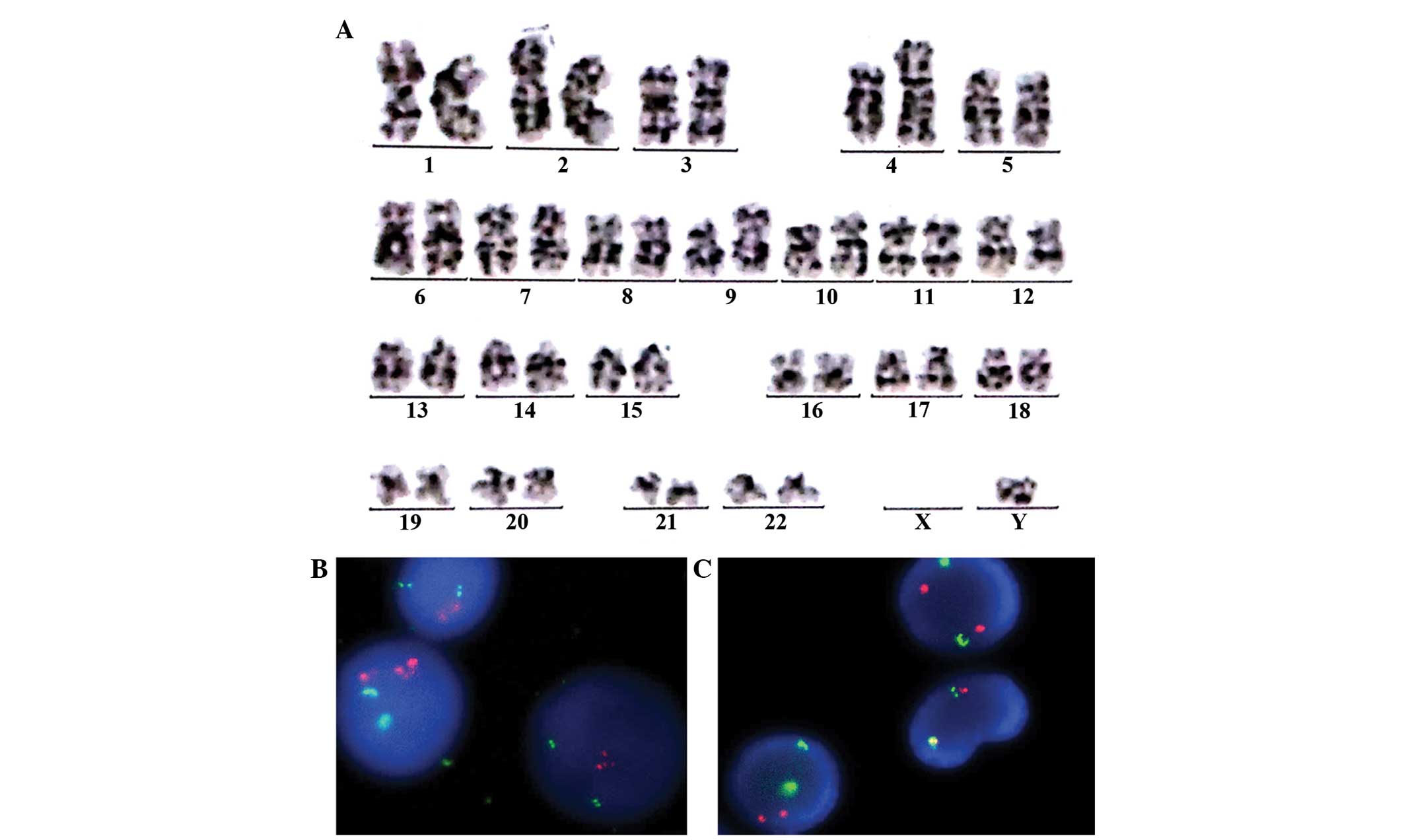
value, 2.6) (Fig. 9). The patient was
negative for the BCR/ABL and IGH/CCND1 genes on fluorescence in
situ hybridization (FISH) tests. However, on karyotype
analysis, a fragment from an unknown source that was an addition to
chromosome 4 was observed in 2 out of the 7 analyzed cells
(Fig. 10). Bone marrow metaphase
cytogenetic studies were performed on 24-h bone marrow cultures
without any colony stimulating factor. The cells were cultured in
RPMI-1640 medium (Invitrogen; Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) supplemented with 20% fetal calf serum (BD
Biosciences) and 2% L-glutamine. The cells were harvested, and cell
suspensions were stored in a freezer at ~-20°C. Conventional
cytogenetic karyotyping was performed using standard G-banding
cytogenetic methods. Seven metaphases were analysed. FISH
procedures were carried out on fixed bone marrow cells according to
the manufacturers protocol (Vysis; Abbott Molecular, Des Plaines,
IL, USA). The slide was washed in 2X saline sodium citrate for 4
min, followed by an alcohol series for dehydration. Co-denaturation
was conducted for 5 min at 75°C, followed by overnight
hybridization at 37°C. Evaluation of the FISH signals was performed
using fluorescence microscopy (Axio Imager A1; Zeiss AG,
Oberkochen, Germany) under ×1,000 magnification. For each test, a
minimum of 200 interphase cells were evaluated for signal pattern.
According to the aforementioned results, the patient was diagnosed
with secondary B-cell lymphoblastic leukemia in MM.
Findings in reviewing the bone marrow
smears
After secondary lymphoblastic leukemia was
diagnosed, all the records of the patient were reviewed, notable
among these were the bone marrow smears. The patient had six marrow
sampling during maintenance therapy. All the bone marrow smears
appeared in a good state, and the percentage and morphology of the
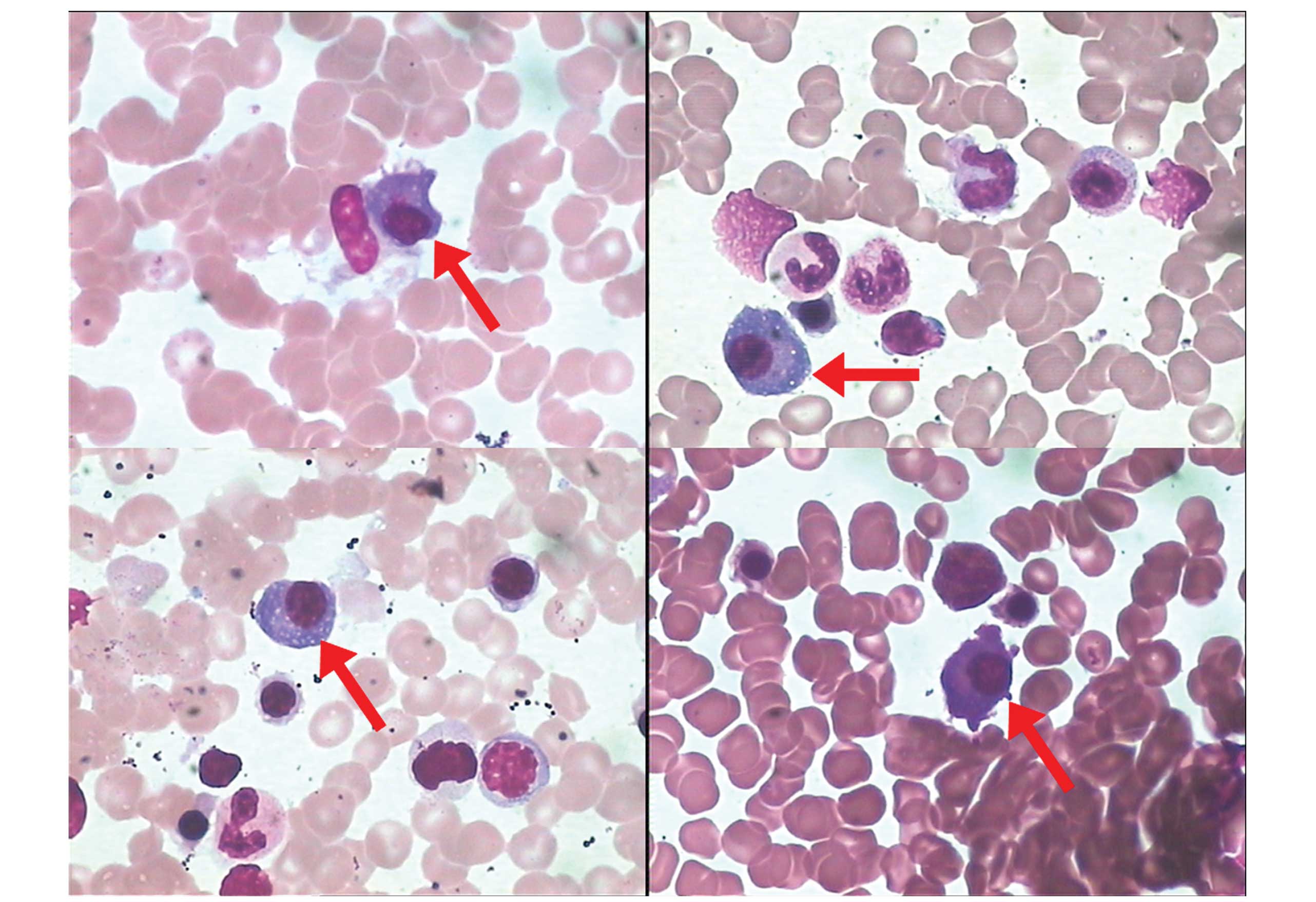
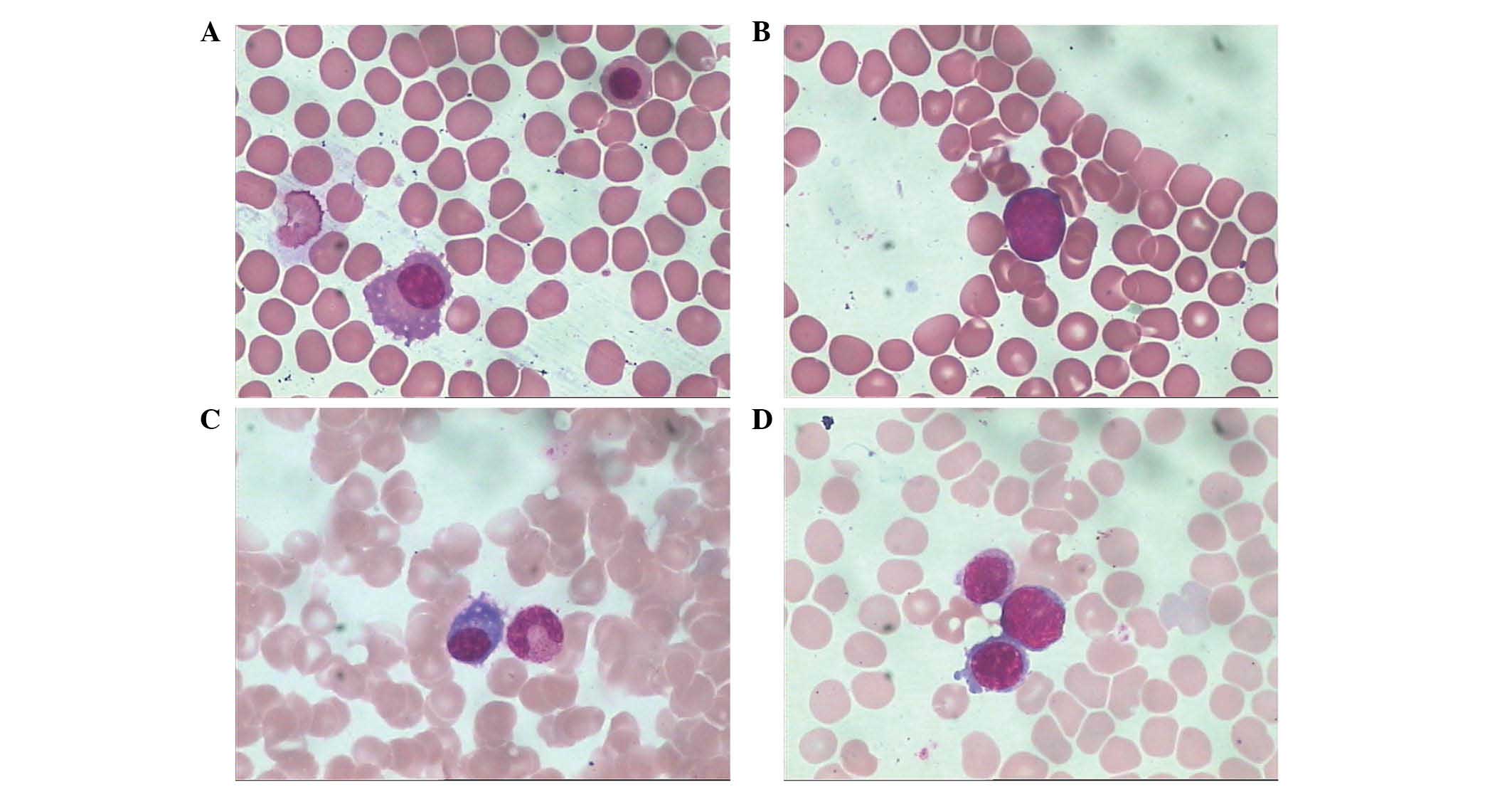
plasma cells were normal. Unexpectedly, an extremely low percentage
(<0.01%) of blast cells was found in all the bone marrow smears
during the maintenance therapy (Fig.
11). The blast cells had scant agranular cytoplasm, no Auer
rods, coarse to fine chromatin and indistinct nucleoli. The blast
cells were not noticed during maintenance therapy due to their low
percentage.
The patient was then administered CHOP regimen
(cyclophosphamide, 1.2 g on day 1; pirarubicin; 60 mg on day 1,
vincristine, 2 mg on day 1; and prednisone, 30 mg bid on days 1–5)
for 1 cycle. However, the regimen had poor efficiency, and the
lymphoblasts still accounted for 48% of all nucleated cells in the
patients bone marrow smear. Subsequently, the patient discontinued
the treatment and was not further followed up. The patient
succumbed to disease on April 2014.
Discussion
In recent years, the application of novel agents has
prolonged the survival time of MM patients, but a concerning
finding has been the increase in the incidence of secondary
malignancies (4–7). In the reported cases, the majority of
secondary malignancies in MM were acute myelocytic leukemia (AML),
myelodysplastic syndrome (MDS) and solid tumors (4–7). In a
previous study, the present authors reported 3 cases of MM who
developed lymphoblastic leukemia after exposure to a variety of
agents (9). The present study reports
the case of a patient who developed secondary lymphoblastic
leukemia 38 months after the initial MM diagnosis.
It has been hypothesized that plasma cell dyscrasias
exhibited a higher risk of associated AML/MDS. A number of immune
system defects have been described in MM, although the clinical
importance of these defects remains unclear. The more well-known of
these immune defects include impaired lymphocyte function,
decreased γ globulin levels and steroid-associated
lymphopenia/immunosuppression (4,11). These
alterations are likely to predispose MM patients to other
malignancies.
Bortezomib was the main drug used in induction
therapy for the present study patient. There is little literature
on the secondary malignancies that are triggered by bortezomib, and
available studies show that bortezomib exhibits a relatively low
incidence of secondary malignancies (12,13). The
present patient had only a short exposure time to bortezomib (<2
months).
The consolidation and maintenance therapy of the
patient was somehow complicated, since after complete remission was
achieved, lenalidomide, maphalan and thalidomide were successively
administered for consolidation and maintenance therapy.
According to contemporary research, exposure to
melphalan (11,13–15) and
lenalidomide (15–21) may cause immunosuppression, and may be
associated with a higher frequency of secondary malignancies.
However, the exposure times to lenalidomide and melphalan in the
present study were short (4 days and 2 months, respectively).
In the present study, the relatively long exposure
time to thalidomide (31 months as maintenance therapy) was
considered as an important potential risk factor. The clinical
observation of patients treated with thalidomide has suggested that
this agent could exert immunostimulatory and immunosuppressive
activities (22,23). However, thalidomide has been
associated with a relatively low incidence of secondary
malignancies in MM (24,25).
According to the aforementioned analysis, it was
difficult to determine whether any of the single agents that were
used in the treatment were the cause of the secondary lymphoblastic
leukemia in the present patient. It is worth noting that the
treatment of the patient was somehow complex, since bortezomib,
dexamethasone, lenalidomide, vincristine, pirarubicin, melphalan
and thalidomide were used successively in the induction therapy,
consolidation therapy and maintenance therapy. Owing to the
exposure of the patient to a variety of agents, it could be
inferred that multiple immune defects may exist and may play an
important role in the secondary lymphoblastic leukemia that was
diagnosed.
After scrutinizing the patient's bone marrow smears
during the maintenance therapy, an extremely low percentage of
blast cells was unexpectedly found each time. As the blast cells
were at a low percentage, they were not noticed during the
maintenance therapy. Therefore, flow cytometry and peroxidase
staining were not performed at this time, and it was impossible to
identify whether the blast cells were lymphoblasts or myeloblasts
by immunophenotype. However, according to the morphology of the
blast cells (scant agranular cytoplasm, no Auer rods, coarse to
fine chromatin and indistinct nucleoli), we speculated that the
blast cells may be lymphoblasts. It could be inferred that the
patient was possibly in an early stage of lymphoblastic leukemia
during the maintenance therapy of MM. If the bone marrow smears had
been scrutinized carefully, and if flow cytometry had been used, an
early stage of lymphoblastic leukemia could have been identified
and interventional treatment could have been applied.
The present authors previously reported 3 cases of
MM who developed secondary lymphoblastic leukemia. A very low
percentage of similar blast cells were found in the bone marrow
smears during maintenance therapy in all those 3 cases (9). It is not known whether the subsequent
occurrence of secondary B-cell lymphoblastic leukemia represents a
transformation of MM into a less differentiated B-cell malignancy,
a biclonal neoplasm arising from an oncogenic event in a common
B-cell precursor, or an independent oncogenic event due to the
defect in immune dysregulation (4,6–9). However, if a low percentage of blast
cells is noticed early on, flow cytometry may be introduced and
provide further evidence of disease, and the patient may also have
a chance for early intervention. The previous 3 cases and the
present case illustrate the value of microscopic examination and
flow cytometry detection in identifying secondary malignancies in
MM.
In summary, the present study reports a rare case of
secondary B-cell lymphoblastic leukemia that occurred 38 months
after the primary diagnosis of MM, the cause of which may be
associated with exposure to a variety of agents. Microscopic
examination and flow cytometry detection were important in
identifying the secondary malignancy in this MM case.
Glossary
Abbreviations
Abbreviations:
|
MM
|
multiple myeloma
|
|
MBS
|
metastatic bone survey
|
|
CD
|
cluster of differentiation
|
|
AML
|
acute myeloid leukemia
|
|
MDS
|
myelodysplastic syndromes
|
References
|
1
|
Junxun L, Juan L, Xiuzhen T, Juan O,
Bohuang Z and Junru L: Comparing five diagnostic criteria for
multiple myeloma: A retrospective study of 227 cases. Tumori.
100:207–213. 2014.PubMed/NCBI
|
|
2
|
Smith L, McCourt O, Henrich M, Paton B,
Yong K, Wardle J and Fisher A: Multiple myeloma and physical
activity: A scoping review. BMJ Open. 5:e0095762015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li J, Chen S, Hu Y and Cai J:
Bortezomib-induced severe pulmonary complications in multiple
myeloma: A case report and literature review. Ocol Lett.
11:2255–2260. 2016.
|
|
4
|
Mailankody S, Pfeiffer RM, Kristinsson SY,
Korde N, Bjorkholm M, Goldin LR, Turesson I and Landgren O: Risk of
acute myeloid leukemia and myelodysplastic syndromes after multiple
myeloma and its precursor disease (MGUS). Blood. 118:4086–4092.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pan B and Lentzsch S: The application and
biology of immunomodulatory drugs (IMiDs) in cancer. Pharmacol
Ther. 136:56–68. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ormerod A, Fausel CA, Abonour R and Kiel
PJ: Observations of second primary malignancy in patients with
multiple myeloma. Clin Lymphoma Myeloma Leuk. 12:113–117. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Srivastava G, Rana V, Lacy MQ, Buadi FK,
Hayman SR, Dispenzieri A, Gertz MA, Dingli D, Zeldenrust S, Russell
S, et al: Long-term outcome with lenalidomide and dexamethasone
therapy for newly diagnosed multiple myeloma. Leukemia.
27:2062–2066. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gökbuget N: How I treat older patients
with ALL. Blood. 122:1366–1375. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Junxun L, Junru L, Meilan C, Chujia L,
Shaoqian C, Jieyu Z, Zhuangjian Y, Fan Z, Juan O, Jing C and Juan
L: Three patients with multiple myeloma developing secondary
lymphoblastic leukemia: Case reports and review of the literature.
Tumori. Jul 2–2015.(Epub ahead of print). doi: 10.5301/tj.5000377.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Katzel JA, Hari P and Vesole DH: Multiple
myeloma: Charging toward a bright future. CA Cancer J Clin.
57:301–318. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schütt P, Brandhorst D, Stellberg W, Poser
M, Ebeling P, Müller S, Buttkereit U, Opalka B, Lindemann M,
Grosse-Wilde H, Seeber S, et al: Immune parameters in multiple
myeloma patients: Influence of treatment and correlation with
opportunistic infections. Leuk Lymphoma. 47:1570–1582. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chanan-Khan A, Sonneveld P, Schuster MW,
Stadtmauer EA, Facon T, Harousseau JL, Ben-Yehuda D, Lonial S,
Goldschmidt H, Reece D, et al: Analysis of herpes zoster events
among bortezomib-treated patients in the phase III APEX study. J
Clin Oncol. 26:4784–4790. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
San Miguel JF, Schlag R, Khuageva NK,
Dimopoulos MA, Shpilberg O, Kropff M, Spicka I, Petrucci MT,
Palumbo A, Samoilova OS, et al: Persistent overall survival benefit
and no increased risk of second malignancies with
bortezomib-melphalan-prednisone versus melphalan-prednisone in
patients with previously untreated multiple myeloma. J Clin Oncol.
31:448–455. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cuzick J, Erskine S, Edelman D and Galton
DA: A comparison of the incidence of the myelodysplastic syndrome
and acute myeloid leukaemia following melphalan and
cyclophosphamide treatment for myelomatosis. A report to the
Medical Research Council's working party on leukaemia in adults. Br
J Cancer. 55:523–529. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bergsagel DE, Bailey AJ, Langley GR,
MacDonald RN, White DF and Miller AB: The chemotherapy on
plasma-cell myeloma and the incidence of acute leukemia. N Engl J
Med. 301:743–748. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dasanu CA: Immune alterations in untreated
and treated multiple myeloma. J Oncol Pharm Pract. 18:257–263.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tai YT, Li XF, Catley L, Coffey R,
Breitkreutz I, Bae J, Song W, Podar K, Hideshima T, Chauhan D, et
al: Immunomodulatory drug lenalidomide (CC-5013, IMiD3) augments
anti-CD40 SGN-40-induced cytotoxicity in human multiple myeloma:
Clinical implications. Cancer Res. 65:11712–11720. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dasanu CA and Alexandrescu DT: A case of
severe aplastic anemia secondary to treatment with lenalidomide for
multiple myeloma. Eur J Haematol. 82:231–234. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Attal M, Lauwers-Cances V, Marit G,
Caillot D, Moreau P, Facon T, Stoppa AM, Hulin C, Benboubker L,
Garderet L, et al: IFM Investigators: Lenalidomide maintenance
after stem-cell transplantation for multiple myeloma. N Engl J Med.
366:1782–1791. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
McCarthy PL, Owzar K, Hofmeister CC, Hurd
DD, Hassoun H, Richardson PG, Giralt S, Stadtmauer EA, Weisdorf DJ,
Vij R, et al: Lenalidomide after stem-cell transplantation for
multiple myeloma. N Engl J Med. 366:1770–1781. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Palumbo A, Hajek R, Delforge M, Kropff M,
Petrucci MT, Catalano J, Gisslinger H, Wiktor-Jędrzejczak W,
Zodelava M, Weisel K, et al: MM-015 Investigators: Continuous
lenalidomide treatment for newly diagnosed multiple myeloma. N Engl
J Med. 366:1759–1769. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Haslett PA, Corral LG, Albert M and Kaplan
G: Thalidomide costimulates primary human T lymphocytes,
preferentially inducing proliferation, cytokine production, and
cytotoxic responses in the CD8+ subset. J Exp Med.
187:1885–1892. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Verbon A, Juffermans NP, Speelman P, van
Deventer SJ, ten Berge IJ, Guchelaar HJ and van der Poll T: A
single oral dose of thalidomide enhances the capacity of
lymphocytes to secrete gamma interferon in healthy humans.
Antimicrob Agents Chemother. 44:2286–2290. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Usmani SZ, Sexton R, Hoering A, Heuck CJ,
Nair B, Waheed S, Al Sayed Y, Chauhan N, Ahmad N, Atrash S, et al:
Second malignancies in total therapy 2 and 3 for newly diagnosed
multiple myeloma: Influence of thalidomide and lenalidomide during
maintenance. Blood. 120:1597–1600. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stewart AK, Trudel S, Bahlis NJ, White D,
Sabry W, Belch A, Reiman T, Roy J, Shustik C, Kovacs MJ, et al: A
randomized phase 3 trial of thalidomide and prednisone as
maintenance therapy after ASCT in patients with MM with a
quality-of-life assessment: The National Cancer Institute of Canada
Clinicals Trials Group Myeloma 10 Trial. Blood. 121:1517–1523.
2013. View Article : Google Scholar : PubMed/NCBI
|