Introduction
Inflammatory myofibroblastic tumor (IMT) is an
uncommon type of mesenchymal tumor (1). The current World Health Organization
(WHO) classification for this rare tumor entity is a fibroblastic
sarcoma or myofibroblastoma, which is a distinctive neoplasm of
intermediate biological potential that may be malignant or
aggressive (2). The worldwide
incidence of IMT is 0.04–0.7% (3,4) and
clinical data has shown that IMTs have a 25% rate of local
recurrence, and up to a 5% rate of distant metastasis (2).
IMT mostly occurs in visceral soft tissues,
including the lungs, mesentery, omentum, retroperitoneum, pelvis
and abdominal soft tissue (5). IMT
mostly affects children and adolescents, while being scarcely
observed in old people, and generally does not exhibit any gender
preference (5). Pancreatic IMT is
rare, however previous studies have shown that this type of
occurrence may be more common in women (6,7). A total
of 60% of pancreatic IMTs are located in the head of the pancreas,
while 40% of cases are located in the body and tail (6,8). Surgery
is the primary treatment for pancreatic IMT, and in rare cases this
may be complemented by treatment with steroids and/or radiation
(7,9).
The prognosis of the disease is generally favorable, and regular
follow-up is necessary.
In the current study, the case of a 69-year-old man
who presented to the Shengjing Hospital of China Medical University
(Shenyang, China) with symptoms of anorexia, nausea and vomiting
caused by an IMT in the head of the pancreas, is reported. Surgical
resection was conducted, and the patient had a regular follow-up 3
years later. Written informed consent was obtained from the
patient.
Case report
A 69-year-old man was admitted to the Shengjing
Hospital of China Medical University on January 9, 2013 with a
3-month history of anorexia, upper abdominal distension and
vomiting. Nausea and vomiting frequently occurred following a meal.
Undigested food and bile were occasionally present in the vomitus.
Pain, fever, jaundice and melena were not reported, although the
patient had experienced a weight loss of 10 kg. His medical history
was unremarkable. Physical examination revealed absence of
tenderness in the epigastric area. Succussion splash and Murphy's
sign were negative, and the patient's bowel sounds were normal.
Laboratory tests, including complete blood count, urinalysis,
amylase test and lipase test, were normal. The levels of tumor
markers, including α-fetoprotein, 2.20 ng/ml (normal range,
0.00–9.00 ng/ml), carcinoembryonic antigen (CEA), 2.87 ng/ml
(normal range, 0.00–5.00 ng/ml), carbohydrate antigen (CA)19-9,
15.26 U/ml (normal range, 0.00–37.00 U/ml) and CA72-4, 1.30 U/ml
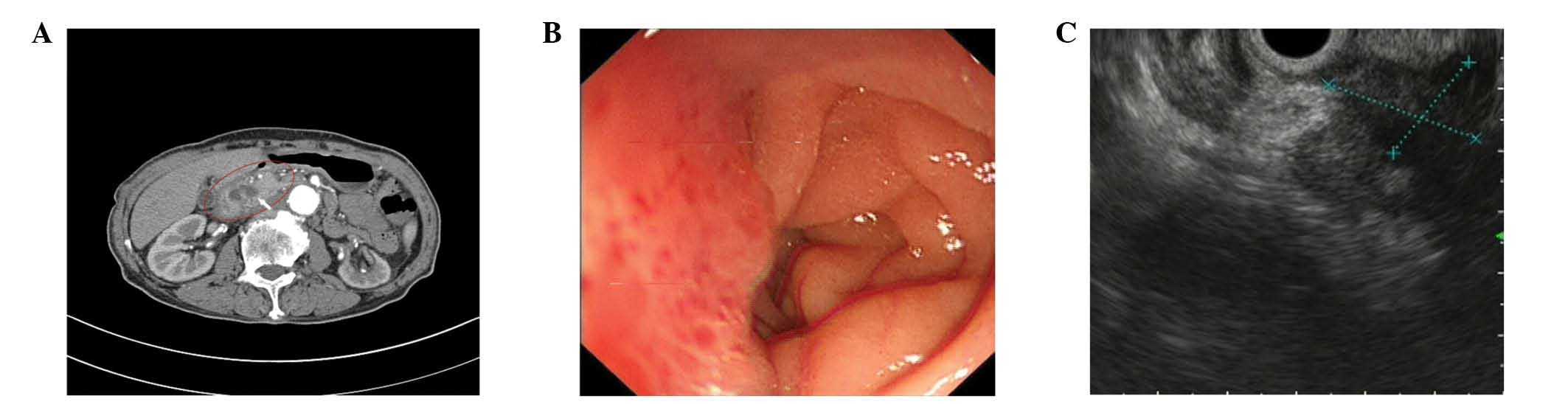
(normal range, 0.00–6.90 U/ml), were negative. Enhanced abdominal
computed tomography (CT; SOMATOM Definition AS; Siemens Healthcare,
Erlangen, Germany) examination revealed a cystic-solid tumor
located between the pancreas and the duodenum (Fig. 1A). No evidence of distant organ or
lymph node metastasis was observed. Endoscopy revealed a anabrotic
protrusion lesion located between the duodenal bulb and the
descendant duodenum (Fig. 1B).
Endoscopic ultrasound (PENTAX EG-2970K and PENTAX EG-3870UTK;
Pentax, Tokyo, Japan) examination revealed a 23.0×19.0-mm
protrusive low-echo mass, which had unclear boundaries with the
adjacent pancreas, located between the duodenal bulb and the
descendant duodenum (Fig. 1C). The
endoscopic biopsy of the mass was inconclusive, since it
demonstrated a fibrous lesion containing inflammatory cells without
any evidence of malignancy. Since malignant pancreatic head
enlargement with duodenum metastasis was suspected, the patient
underwent an operation in order to establish a diagnosis by
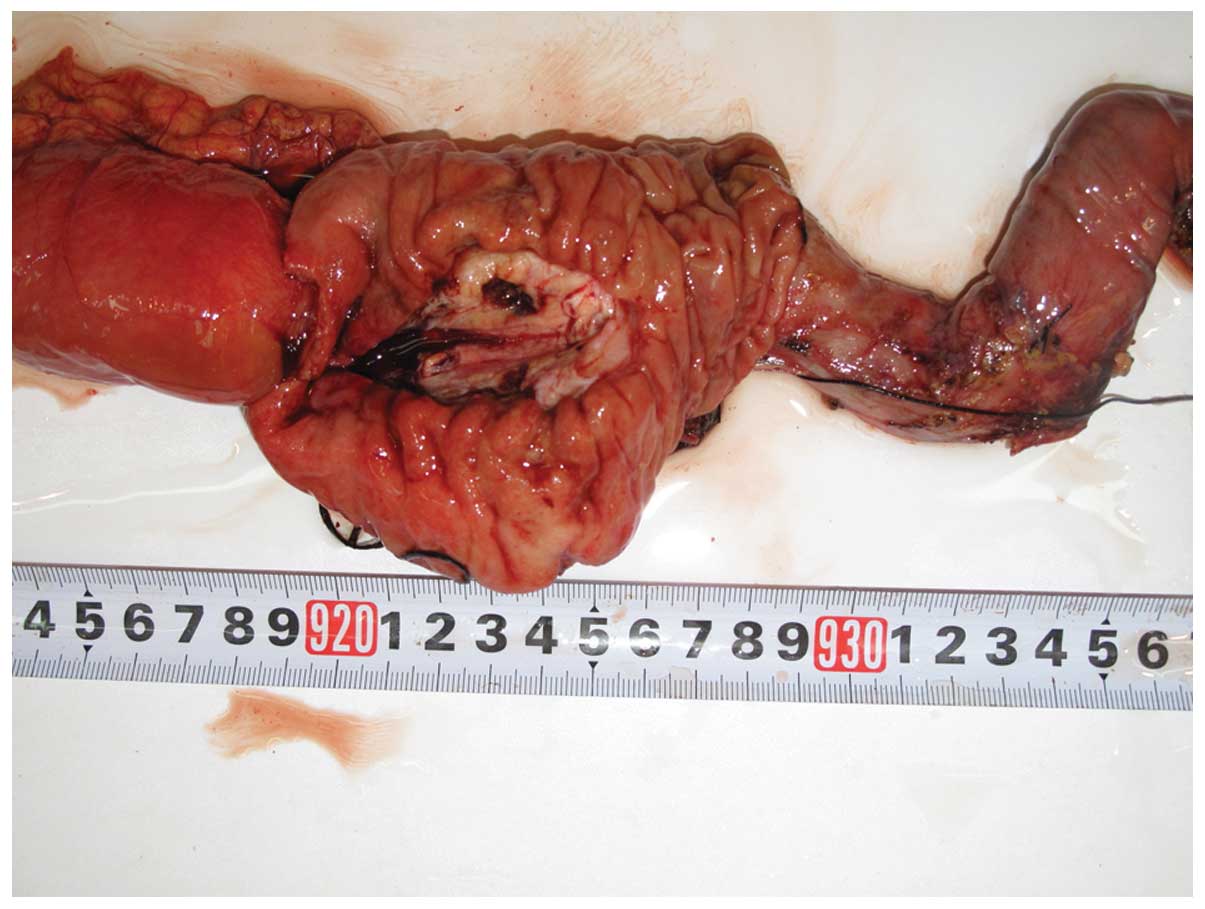
operative pathological biopsy. During the operation, a large, hard
mass with a diameter of ~4.0×3.0 cm, which was located in the head
of the pancreas and metastasized into the duodenum, was identified.
The gross specimen was fleshy, with a white cut surface. Necrosis
and hemorrhage were observed (Fig.
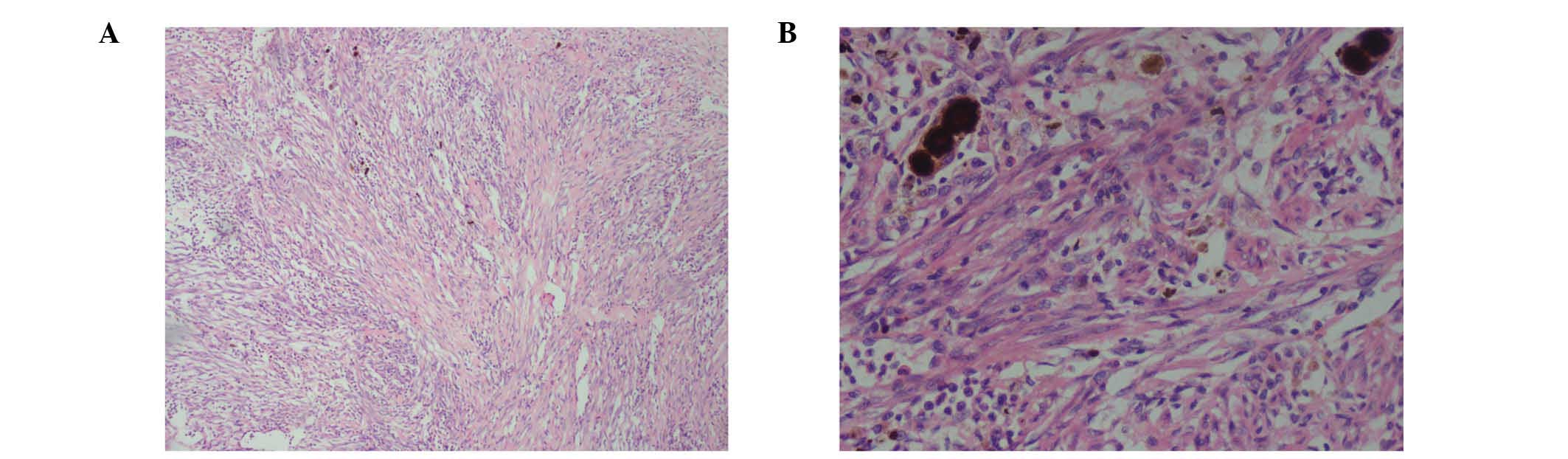
2). Histopathologically, the tumor cells were arranged mainly
in a fusiform pattern with an inflammatory infiltrate of
lymphocytes and eosinophils (Fig. 3).
Samples were stained with hematoxylin and eosin (Sigma-Aldrich, St.
Louis, MO, USA) and visualized using a microscope (Eclipse E800;
Olympus Corporation, Tokyo, Japan). Immunohistochemical staining
was performed with the following antibodies: mouse monoclonal
anti-human smooth muscle actin (SMA; cat. no. ZM-0003; dilution,
1:50; Beijing Zhongshan Jinqiao Biological Technology Co., Ltd.,
Beijing, China), mouse monoclonal anti-human desmin (cat. no.
ZM-0091; dilution, 1:50; Beijing Zhongshan Jinqiao Biological
Technology Co., Ltd.), mouse monoclonal anti-human β-catenin (cat.
no. ZM-0442; dilution, 1:50; Beijing Zhongshan Jinqiao Biological
Technology Co., Ltd.), mouse monoclonal anti-human cluster of
differentiation (CD)34 (cat. no. ZM-0046; dilution, 1:50; Beijing
Zhongshan Jinqiao Biological Technology Co., Ltd.), mouse
monoclonal anti-human CD117 (cat. no. ZM-0437; dilution, 1:50;
Beijing Zhongshan Jinqiao Biological Technology Co., Ltd.) and
mouse monoclonal anti-human DOG-1 (cat. no. ZM-0371; dilution,
1:50; Beijing Zhongshan Jinqiao Biological Technology Co., Ltd.).
Phosphate-buffered saline (Beijing Zhongshan Jinqiao Biological
Technology Co., Ltd.) was used as the dilution buffer and tissue
sections were incubated with the primary antibodies overnight at
4°C. The sections were then washed twice and incubated with
horseradish peroxidase-conjugated goat anti-mouse IgG secondary
antibodies (cat. no. SP-9002; ready to use; Beijing Zhongshan
Jinqiao Biological Technology Co., Ltd.) for 60 min at room
temperature. Staining was visualized using a microscope (Eclipse
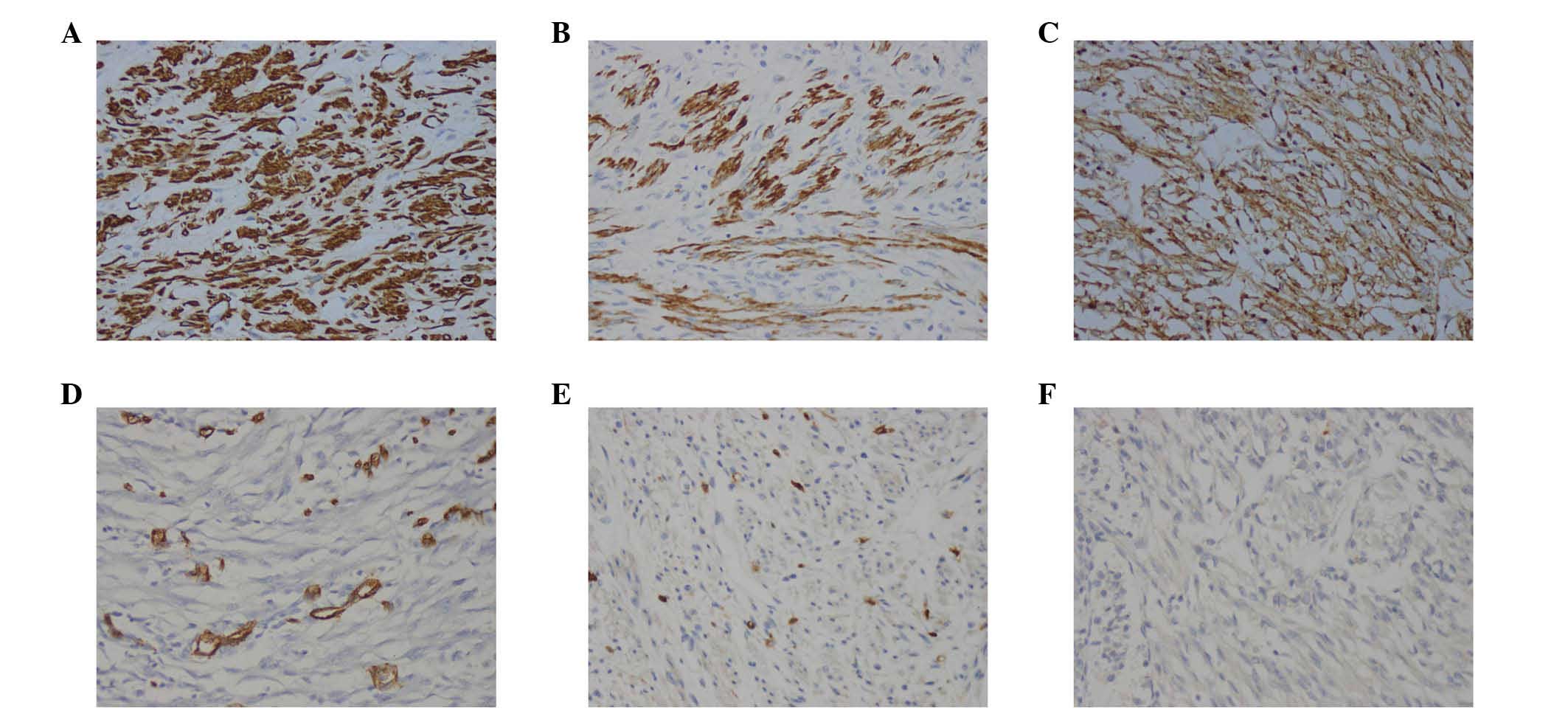
E800; Olympus Corporation). Immunohistochemically, the tumor was
positive for SMA (Fig. 4A), desmin
(Fig. 4B) and β-catenin (Fig. 4C), but negative for CD34 (Fig. 4D), CD117 (Fig. 4E) and DOG-1 antibody (Fig. 4F). A pathological diagnosis of IMT was
established based on the histology and immunohistochemistry
results. The postoperative course was uneventful, and the patient
was discharged from hospital on January 30, 2013. No adjuvant
treatment was administered following surgical excision of the
tumor, and no evidence of a recurrent tumor was observed during the
3 year follow-up.
Discussion
IMT, which is clinically rare, was considered to be
a reactionary inflammatory lesion following trauma, surgery or
infection, and was previously referred to as an inflammatory
pseudotumor, plasma cell granuloma, xanthomatous pseudotumor,
xanthoma or histiocytoma (10,11).
Subsequent studies have identified that IMT is a neoplasm with
frequent clonal alterations in the chromosome 2p23 and with the
potential for local aggressiveness, recurrence, metastasis,
malignant transformation and myofibroblastic differentiation
(11–13). The current WHO classification for this
rare tumor entity is a fibroblastic sarcoma or myofibroblastoma,
which is a distinctive neoplasm of intermediate biological
potential that may be malignant or aggressive (2,10,14). IMT principally affects young patients,
and does not exhibit any gender preference. IMT may occur in the
whole body, although the most common sites are the lungs, head,
neck, extremities, intra-abdominal and retroperitoneal soft tissues
(10,11,15). To
the best of our knowledge, a rare case of a pancreatic IMT that
caused intestinal obstruction in an old man has been previously
published (8). Despite being
previously regarded as a reactive lesion, IMT is currently
considered to be a neoplastic process (10,11).
Therefore, its correct diagnosis is critical for offering the
patients the appropriate disease management and subsequent
treatment.
The clinical presentation of IMT varies depending on
its anatomic location and whether it involves vital organs
(16). For patients with IMT,
pancreatic involvement is often inconclusive, since patients may
generally present with nonspecific symptoms such as abdominal pain,
weight loss and jaundice (11). In
rare cases, IMT may present with anemia, fatigue, sudden diabetes
or a palpable mass that resembles pancreatic carcinoma,
periampullary carcinoma, lymphoma and endocrine tumors (11). The radiological features of IMT are
nonspecific, and exhibit variable characteristics (6). Ultrasound and CT examinations reveal a
solid, or occasionally cystic-solid, mass in the pancreas, which is
usually sized between 5.0 and 10.0 cm and may be well-demarcated or
metastatic (7).
Due to its nonspecific symptoms and imaging
findings, definitive diagnosis of IMT relies on histological
evaluations (6). However, it is often
difficult to obtain enough tissue using a transendoscopic biopsy to
establish a definitive histological diagnosis (17). In the present patient, a gastroscopic
biopsy of the lesion was inconclusive, and surgical resection of
the tissues aided to obtain the final diagnosis of IMT.
The histology results of the present case revealed
the presence of an independent cell type between smooth muscle
cells and fibroblasts, in addition to mixed spindle cells scattered
among a large number of inflammatory cells, mostly lymphocytes,
plasma cells, organized cells, eosinophils and neutrophils
(14). It has been previously
reported that three histological patterns may coexist variably
within the same tumor, namely myxoid/vascular, compact spindle cell
and fibrous hypocellular (15,18–20).
Immunohistochemically, the majority of cases of IMT express SMA,
desmin and cytokeratin (15,17,21).
Anaplastic lymphoma kinase (ALK) immunostaining is detected in
40–60% of cases, and involves rearrangements or translocations of
the ALK receptor tyrosine kinase on the chromosome 2p23 (16,21). In
previous studies, the histological features of IMT did not
correlate with its clinical behavior (2). In addition, the risk of malignant
transformation or metastasis has been described in certain cases,
and remains low (<5%) (2). In the
present case, the tumor exhibited a compact spindle cell
histological pattern, and there were no obvious signs of malignancy
in the histology. Immunohistochemical staining demonstrated the
tumor to be SMA+, desmin+,
β-catenin+, CD34−, CD117− and
DOG-1−. During a regular 3 year follow-up, the patient
was observed to be healthy.
Currently, despite the difficulty of obtaining a
definitive diagnosis based on biopsies and radiological
examinations, surgery with complete excision remains the primary
therapeutic option for IMT, although no real consensus regarding
the treatment of IMT exists (7,9). The low
risk of malignant transformation or metastasis has been described
in previous cases of IMT, but if the excision is incomplete, the
risk increases from <5 to 25% (2).
Due to the possibility of malignancy and relapse, a number of
authors have reported that a simple tumor excision is uncertain
(8). Wide excision may be appropriate
if the patient's physical condition is adequate (7,9). However,
whether radical resection for such intermediate, low-grade lesions
is appropriate requires further clinical study. In the present
report, the case of an elderly, infirm man who had IMT of the head
of the pancreas with unclear boundaries with the adjacent duodenum,
was presented. During surgery, no evidence of blood vessels, lymph
node or other abdominal organs metastasis (except adjacent
duodenum) was observed. In consequence, a duodenopancreatectomy was
performed. For similar patients, a surgical approach on a
case-by-case basis may be considered in the future. For
non-excisable lesions, several medical treatments, including
chemotherapy, radiation therapy, nonsteroidal anti-inflammatory
drugs, corticosteroids and antitumor necrosis factor-binding
antibodies, have been previously administered to palliate or shrink
these IMTs to a resectable size and configuration (6,7,9). However, the medical treatment is not
clearly defined due to a lack of strong statistical evidence, and
palliative treatment programs cannot be recommended as a standard
regimen (22,w). Based on the recent advances in ALK inhibitors and
other ALK target genes, these therapies may be more effective, and
thus may be offered to patients with IMT instead (16). Whether surgical resection or drug
therapy is the selected treatment, the prognosis of the disease is
favorable, with distant metastases occurring rarely, and a 5-year
survival rate of 91% (10,11,15).
However, close, long-term follow-up is necessary due to the
probability of malignancy, distant metastasis and recrudescence
exhibited by IMT (15).
In conclusion, in this study the rare case of
pancreatic head IMT in a 69-year-old man, with aggressive behavior
and metastasis to the duodenum was presented. However, the
patient's clinical symptoms and imaging findings were nonspecific
and diagnosis relied on histopathological examination and
immunohistochemistry. Complete surgical resection is the preferred
treatment for IMT. The prognosis of the disease is generally
favorable, and regular follow-up is necessary.
Glossary
Abbreviations
Abbreviations:
|
ALK
|
anaplastic lymphoma kinase
|
|
CEA
|
carcinoembryonic antigen
|
|
CT
|
computed tomography
|
|
H&E
|
hematoxylin and eosin
|
|
IMT
|
inflammatory myofibroblastic tumor
|
|
SMA
|
smooth muscle actin
|
|
WHO
|
World Health Organization
|
References
|
1
|
Patnana M, Sevrukov AB, Elsayes KM,
Viswanathan C, Lubner M and Menias CO: Inflammatory pseudotumor:
The great mimicker. AJR Am J Roentgenol. 198:W217–W227. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fletcher CDM, Bridge JA, Hogendoorn P and
Mertens F: World Health Organization Classification of Tumours of
Soft Tissue and Bone. World Health Organization Classification of
Tumors. 5:(4th). IARC Press. (Lyon). 2013.
|
|
3
|
Pinilla I, Herrero Y, Torres MI, Nistal M
and Pardo M: Myofibroblastic inflammatory tumor of the lung.
Radiologia. 49:53–55. 2007.(In Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Panagiotopoulos N, Patrini D, Gvinianidze
L, Woo WL, Borg E and Lawrence D: Inflammatory myofibroblastic
tumour of the lung: A reactive lesion or a true neoplasm? J
Thoracic Dis. 7:908–911. 2015.
|
|
5
|
Zhang T, Yuan Y, Ren C, DU S, Chen J, Sun
Q and Liu Z: Recurrent inflammatory myofibroblastic tumor of the
inguinal region: A case report and review of the literature. Oncol
Lett. 10:675–680. 2015.PubMed/NCBI
|
|
6
|
Sim A, Lee MW and Nguyen GK: Inflammatory
myofibroblastic tumour of the pancreas. Can J Surg. 51:E23–E24.
2008.PubMed/NCBI
|
|
7
|
Dagash H, Koh C, Cohen M, Sprigg A and
Walker J: Inflammatory myofibroblastic tumor of the pancreas: A
case report of 2 pediatric cases - steroids or surgery? J Pediatr
Surg. 44:1839–1841. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pungpapong S, Geiger XJ and Raimondo M:
Inflammatory myofibroblastic tumor presenting as a pancreatic mass:
A case report and review of the literature. JOP. 5:360–367.
2004.PubMed/NCBI
|
|
9
|
Tomazic A, Gvardijancic D, Maucec J and
Homan M: Inflammatory myofibroblastic tumor of the pancreatic head
- a case report of a 6 months old child and review of the
literature. Radiol Oncol. 49:265–270. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fragoso AC, Eloy C, Estevão-Costa J,
Campos M, Farinha N and Lopes JM: Abdominal inflammatory
myofibroblastic tumor a clinicopathologic study with reappraisal of
biologic behavior. J Pediatr Surg. 46:2076–2082. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gleason BC and Hornick JL: Inflammatory
myofibroblastic tumours: Where are we now? J Clin Pathol.
61:428–437. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ernst CW, Van Der Werff Ten Bosch J,
Desprechins B, de Mey J and De Maeseneer M: Malignant
transformation of an abdominal inflammatory myofibroblastic tumor
with distant metastases in a child. JBR-BTR. 94:78–80.
2011.PubMed/NCBI
|
|
13
|
Fisher C: Myofibroblastic malignancies.
Adv Anat Pathol. 11:190–201. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Coindre JM: New WHO classification of
tumours of soft tissue and bone. Ann Pathol. 32(Suppl 5):
S115–S116. 2012.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Coffin CM, Watterson J, Priest JR and
Dehner LP: Extrapulmonary inflammatory myofibroblastic tumor
(inflammatory pseudotumor). A clinicopathologic and
immunohistochemical study of 84 cases. Am J Surg Pathol.
19:859–872. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Butrynski JE, D'Adamo DR, Hornick JL, Dal
Cin P, Antonescu CR, Jhanwar SC, Ladanyi M, Capelletti M, Rodig SJ,
Ramaiya N, et al: Crizotinib in ALK-rearranged inflammatory
myofibroblastic tumor. N Engl J Med. 363:1727–1733. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Khakural P, Sapkota R, Shrestha UK and
Sayami P: Successful surgical management of a rare esophageal
inflammatory myofibroblastic tumour: A case report. J Cardiothorac
Surg. 10:1122015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chan JK, Cheuk W and Shimizu M: Anaplastic
lymphoma kinase expression in inflammatory pseudotumors. Am J Surg
Pathol. 25:761–768. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hussong JW, Brown M, Perkins SL, Dehner LP
and Coffin CM: Comparison of DNA ploidy, histologic and
immunohistochemical findings with clinical outcome in inflammatory
myofibroblastic tumors. Mod Pathol. 12:279–286. 1999.PubMed/NCBI
|
|
20
|
Makhlouf HR and Sobin LH: Inflammatory
myofibroblastic tumors (inflammatory pseudotumors) of the
gastrointestinal tract: How closely are they related to
inflammatory fibroid polyps? Hum Pathol. 33:307–315. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cook JR, Dehner LP, Collins MH, Ma Z,
Morris SW, Coffin CM and Hill DA: Anaplastic lymphoma kinase (ALK)
expression in the inflammatory myofibroblastic tumor: A comparative
immunohistochemical study. Am J Surg Pathol. 25:1364–1371. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Germanidis G, Xanthakis I, Tsitouridis I,
Zaramboukas T, Kiskinis D, Konstantaras C, Miliaras S, Sirakos T
and Pagkalos E: Regression of inflammatory myofibroblastic tumor of
the gastrointestinal tract under infliximab treatment. Dig Dis Sci.
50:262–265. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Applebaum H, Kieran MW, Cripe TP, Coffin
CM, Collins MH, Kaipainen A, Laforme A and Shamberger RC: The
rationale for nonsteroidal anti-inflammatory drug therapy for
inflammatory myofibroblastic tumors: A Children's Oncology Group
study. J Pediatr Surg. 40:999–1003. 2005. View Article : Google Scholar : PubMed/NCBI
|