Introduction
An estimated 231,840 novel cases of breast cancer
and 40,290 breast cancer-associated mortalities occurred among
women from the US in 2015, ranking breast cancer the most common
cancer diagnosis and the second leading cause of fatality among
American women (1). Although the
overall incidence of breast cancer is lower among African American
(AA) women compared with Caucasian women, AA breast cancer patients
of all ages are more likely to have advanced disease at diagnosis,
an increased risk of recurrence and a poorer prognosis (2–6). Racial
disparities in breast cancer mortality in the US persist, with AA
breast cancer patients experiencing higher mortality rates compared
with their Caucasian counterparts (7–9). Recent
data from the 50 largest US cities confirms the trend of increasing
racial disparities (8). Various
factors are proposed to affect this difference in outcome, with an
advanced stage at presentation, high-risk tumor biology, lower
socioeconomic status, disparity in access to care and treatment and
comorbidity typically viewed as the major associated factors
(3,4,10–14).
Tumor stage and tumor grade are the major prognostic
factors that are commonly used to define the risk of biological
aggressiveness of breast tumors (15,16). Tumor
stage and grade also contribute to racial disparity between AA and
Caucasian women (17,18). It is prudent to understand how race
associates with survival in various subgroups defined by tumor
stage and grade. In the current study, the disparity in breast
cancer mortality among AA and Caucasian women in an Arkansas
patient population was investigated. Age, tumor stage and tumor
grade were presented for each racial subtype and included in the
analysis. The aim of the present study was to examine the
interaction of race with tumor grade and with tumor stage, with
regards to survival time.
Materials and methods
Study design and population
A retrospective cohort study was conducted of
non-Hispanic AA and Caucasian women, who were treated at the
Winthrop P. Rockefeller Cancer Institute of the University of
Arkansas for Medical Sciences (UAMS; Little Rock, AR, USA). The
study was performed according to protocols approved by the UAMS
Institutional Review Board (IRB). The UAMS IRB determined the study
met the criteria for exempt status per 45 CFR 46, meaning there was
no requirement to obtain informed consent from the study subjects.
Patients of the two race groups were included if they were 18 years
of age or older, diagnosed with histologically confirmed breast
cancer between January 1997 and December 2005 and staged into
American Joint Committee on Cancer (AJCC) stage groups I, II, III
or IV (19). The cohort was followed
to assess survival until December 30, 2007. The data were provided
by the Arkansas Central Cancer Registry at the Arkansas Department
of Health (Little Rock, AR, USA). All women were residents of the
Arkansas State. The UAMS Institutional Review Board gave approval
for the use of human-subject records in the present study.
Outcome variables
Breast cancer-specific survival, measured as the
time to breast cancer-specific fatality, was used as the survival
outcome. Survival data were censored at the last contact with the
patient when the patient either remained alive or succumbed from
causes unrelated to breast cancer. Cause-of-fatality data,
classified by International Classification of Diseases (ICD) codes
(vol. 9; http://www.cdc.gov/nchs/icd/icd9.htm) were provided by
the cancer registry.
Predictor variables
Demographic and clinical variables, taken from the
Arkansas tumor registry files, included age at breast cancer
diagnosis, date of diagnosis, date of last contact or fatality,
race, tumor stage, tumor grade and cause of fatality. The hormone
receptor data were not available and therefore not included in the
analyses. Breast cancer grade at diagnosis was defined by the
AJCC's grade I (well-differentiated), grade II
(moderately-differentiated), grade III (poorly-differentiated) or
grade IV (undifferentiated). For survival analyses, grades III and
IV were combined (grade III/IV). Breast cancer stage at diagnosis
used the TNM staging system (20),
and included stages 0, I, II, III, IV and 99. Only patients with
known stage were included. Patients with stages ‘0’ (ductal
carcinoma in situ) and ‘99’ (unknown) at diagnosis were
excluded. Race (including non-Hispanic AAs and Caucasians only),
age (as a continuous variable), tumor grade (as a categorical
variable) and tumor stage (as a categorical variable) were included
as covariates.
Statistical analysis
The χ2 test was used for examining the
associations of race with other variables. Survival time was
analyzed for covariate associations using univariate and
multivariate Cox-regression analyses. Hazard ratios (HRs) and 95%
confidence intervals (CIs) were calculated for each covariate.
Two-way interactions between race and the other covariates were
evaluated. Survival curves were computed using the Kaplan-Meier
method. All P-values were two-sided and evaluated using an α=0.05
significance level. IBM SPSS statistics version 22 software (IBM
SPSS, Armonk, NY, USA) was used for statistical analyses.
Results
Characteristics of the studied
population
The cohort included a total of 1,077 breast cancer
patients, 208 (19.3%) AA and 869 (80.7%) Caucasian (Table I). AA women were significantly younger
compared with Caucasian women, as close to 1/2 (46.2%) of AA women
were diagnosed at the age of <50 years, compared with <1/3
(30.6%) of their Caucasian counterparts. A total of 230 fatalities
occurred among the 1,077 breast cancer patients during 1,605
person-years of follow-up; the median follow-up was 0.88 years. Of
the total 230 mortalities (21.3% of the cohort), 152 (66.1%)
patients succumbed due to breast cancer-specific causes. Among AA
women, 60 mortalities occurred during 316 person-years of
follow-up, 46 (76.7%) of which were breast cancer-associated. Among
Caucasian patients, 170 mortalities occurred during 1,290
person-years of follow-up, 106 (62.4%) of which were attributed to
breast cancer.
 | Table I.Characterization of the cohort
population used in the present study. |
Table I.
Characterization of the cohort
population used in the present study.
| Characteristic | Caucasian | African American | Total | P-value |
|---|
| Racea | 869 (80.7), 106 | 208 (19.3), 46 | 1,077 (100.0),
152 | NA |
| Age, years |
|
Min | 27 | 24 | 24 |
|
|
Max | 96 | 89 | 96 |
|
| Mean
(SD) | 57.6 (13.1) | 53.6 (14.9) | 56.8 (13.5) |
|
| Median | 57 | 52 | 56 |
|
| Age
groupa |
|
|
| <0.001 |
|
≤50 | 266
(30.6), 48 | 96
(46.2), 25 | 362
(33.6), 73 |
|
|
>50 | 603
(69.4), 58 | 112
(53.8), 21 | 715
(66.4), 79 |
|
| Tumor
gradea |
|
|
|
0.020 |
| Grade
I | 219 (25.2), 6 | 44
(21.2), 8 | 263
(24.4), 14 |
|
| Grade
II | 328
(37.7), 29 | 67
(32.2), 12 | 395
(36.7), 41 |
|
| Grade
III | 304
(35.0), 67 | 87
(41.8), 22 | 391
(36.3), 89 |
|
| Grade
IV | 18 (2.1), 4 | 10 (4.8), 4 | 28 (2.6), 8 |
|
| Tumor
stagea |
|
|
| <0.001 |
| Stage
I | 360
(41.4), 17 | 56
(26.9), 2 | 416
(38.6), 19 |
|
| Stage
II | 357
(41.1), 48 | 91
(43.8), 18 | 448
(41.6), 66 |
|
| Stage
III | 111
(12.8), 28 | 39
(18.8), 14 | 150
(13.9), 42 |
|
| Stage
IV | 41
(4.7), 13 | 22
(10.6), 12 | 63
(5.8), 25 |
|
Breast cancer in the study population were
classified into four grades, with grade I exhibiting the fewest and
grade IV exhibting the most histological abnormalities. In general,
higher-grade tumors are associated with more aggressive behavior,
and are considered to have increased relapse and mortality rates
(15,16). Tumors categorized as grade III or IV
were more common in AA compared with Caucasian women, while grade-I
and -II tumors were more common in Caucasian compared with AA women
(P=0.02). More Caucasian patients were diagnosed with stage I
tumors compared with AA patients, while more AA compared with
Caucasian were diagnosed with stages II, III, and IV (P<0.001)
(Table I). Distribution of various
age groups, tumor stages and grades together with the number of
breast cancer-specific deaths are summarized in Table I.
Racial disparity in survival and
interaction of race with tumor grade, tumor stage and age
Association of race with breast cancer-specific
survival was evaluated. AA women experienced shorter survival (HR,
1.74; 95% CI, 1.23–2.46; P<0.002). Two-way interactions of race
with age, race with age groups, race with tumor grade, and race
with tumor stage were then analyzed for breast cancer-specific
survival (Table II). The only
statistically significant interaction observed was between race and
tumor grade (P<0.001). No significant interactions with race
were detected for tumor stage (P=0.71), age (P=0.41) or age groups
(P=0.44).
| Table II.Summary of the results of the
interaction analyses between race and other covariates regarding
survival endpoint. |
Table II.
Summary of the results of the
interaction analyses between race and other covariates regarding
survival endpoint.
| Interaction | Wald
χ2 | dfa | P-value |
|---|
| Race-x-Grade | 15.83 | 2 | <0.001 |
| Race-x-Stage |
1.38 | 3 |
0.710 |
| Race-x-Age |
0.68 | 1 |
0.410 |
| Race-x-Age
groups |
0.59 | 1 |
0.440 |
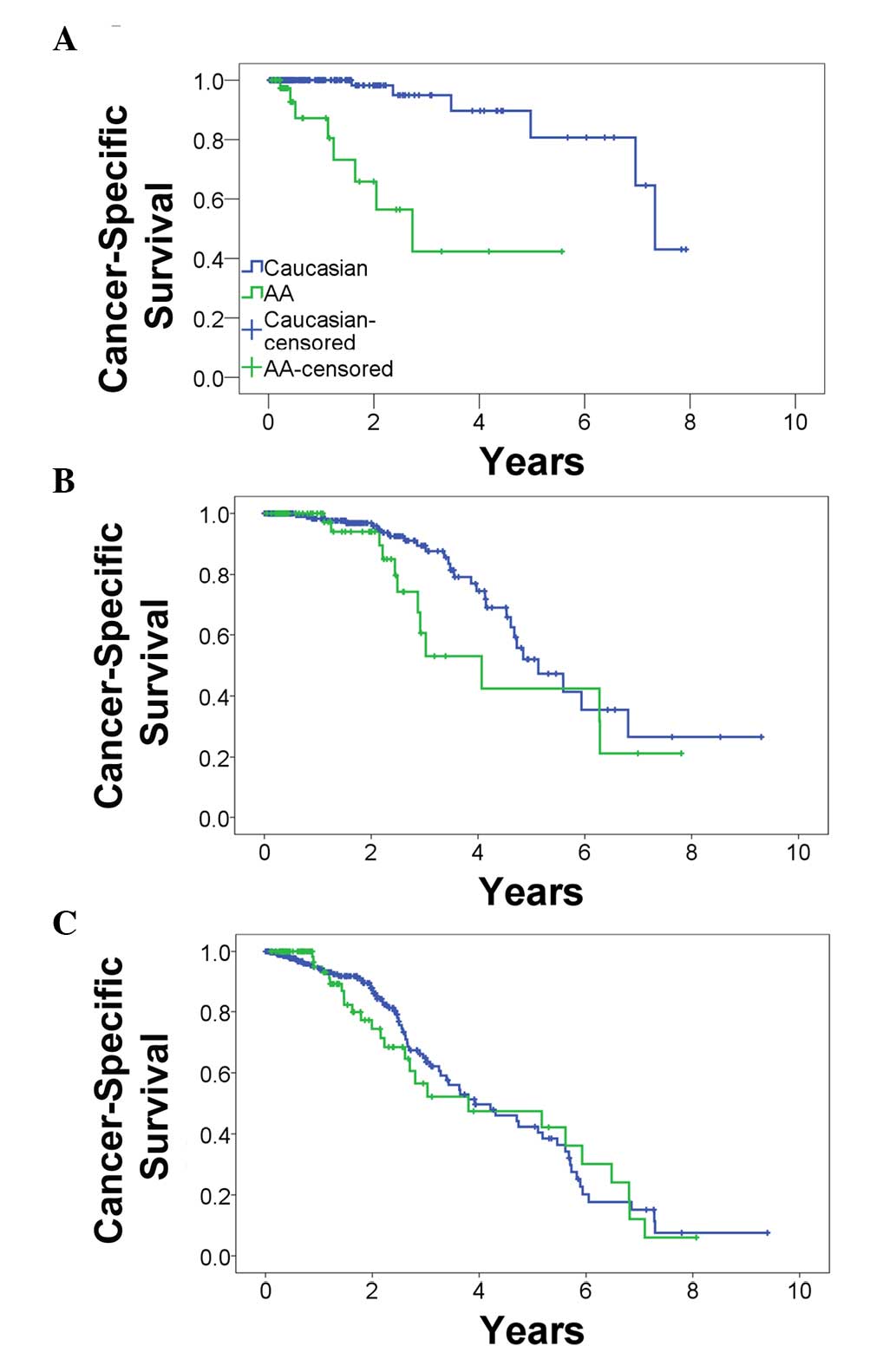
Association of race with survival in
tumor-grade subgroups
Due to the significant interaction between race and
tumor grade and the association with breast cancer-specific
survival, survival disparity between Caucasian and AA women was
visualized in each tumor-grade subgroup by Kaplan-Meier graphs
(Fig. 1). AA showed a dramatic
increase in mortality risk compared with Caucasian women when
diagnosed with a grade I tumor (Fig.
1A). Since race is associated with tumor grade and stage, and
as the survival outcomes are associated with grade, stage and age
in addition to race, a multivariate Cox-regression analysis was
performed for each tumor-grade subgroup in order to study the
effect of race, while adjusting for the other factors (Table III). A statistically significant
increase in AA mortality risk was observed even after controlling
for age at diagnosis (adjusted HR, 20.08; 95% CI, 4.95–81.52;
P<0.001), tumor stage (adjusted HR, 6.80; 95% CI, 1.82–25.42;
P=0.004), and age and stage together (adjusted HR, 9.07; 95% CI,
2.11–38.95; P=0.003). When diagnosed with grade II (Fig. 1B) or grade III/IV tumors (Fig. 1C), no significant race disparity was
observed in the presence of age and tumor stage (Table III). Therefore, a substantial and
statistically significant increase in mortality risk for patients
with lower grade tumors was observed for AA compared with Caucasian
breast cancer women.
| Table III.Hazard ratios for the association
between race (African American vs. Caucasian) and breast cancer
survival in each tumor grade subgroup. |
Table III.
Hazard ratios for the association
between race (African American vs. Caucasian) and breast cancer
survival in each tumor grade subgroup.
|
| Hazard ratio (95%
confidence interval) P-value |
|---|
|
|
|
|---|
| Model | Grade I | Grade II | Grade III/IV |
|---|
| Crude | 12.77
(3.82–42.66) | 1.82
(0.92–3.61) | 1.13
(0.72–1.77) |
|
| P<0.001 | P=0.090 | P=0.600 |
| Adjusted for
age | 20.08
(4.95–81.52) | 1.61
(0.80–3.21) | 1.14
(0.73–1.79) |
|
| P<0.001 | P=0.180 | P=0.570 |
| Adjusted for tumor
stage | 6.80
(1.82–25.42) | 1.17
(0.56–2.45) | 0.98
(0.62–1.54) |
|
| P=0.004 | P=0.690 | P=0.920 |
| Adjusted for age
and tumor stage | 9.07
(2.11–38.95) | 1.00
(0.46–2.16) | 0.98
(0.62–1.56) |
|
| P=0.003 | P=1.000 | P= 0.950 |
Discussion
The present study, in keeping with published data,
suggests that AA breast cancer patients exhibit a shorter survival
time compared with Caucasian patients (5,8,20). The results are consistent with
previously published data from the same institution on data
recorded between 1980 and 1998 (21).
While AA women tend to be diagnosed with high-grade
tumors, and high tumor grade is considered to contribute to
survival disadvantage of AA patients (18,22), the
finding of a strong race-by-grade interaction in the present study
indicates that tumor grade is an effect modifier for AA-Caucasian
disparity over breast cancer-specific survival. This intriguing
observation is supported by the subgroup analysis, which suggests
that diagnosis at a lower tumor grade, regardless of tumor stage
and patient's age at diagnosis, increases AA patients' risk for
poor survival. A study reported significant racial disparity among
stage I breast cancer patients (23).
Tumor grade is considered a determinant for inherent biological
differences in tumor aggressiveness that can be controlled by gene
expression profile. The data in the present study suggest that AA
women experience an additional risk of mortality from breast
cancer, but no additional risk compared with Caucasian patients
that are already considered high risk due to high tumor grade. The
genetic differences between AA and Caucasian women, which remain to
be fully explored, may be important in the progression of the
cancer and its response to treatment (24–28).
Therefore, intrinsic differences in the biology of tumors or the
host could be speculated as being involved in observed disparity.
Future studies are required to explore such a possibility.
Alternatively, it is possible that variations in pharmacogenomics
between AA and Caucasian women explain disparity in outcome through
differences in responsiveness to chemotherapy or other treatment
modalities (29,30). The increased mortality of AA with
low-grade tumors may also be due to nonbiological factors like
disproportional delays in treatment (31,32),
various treatment options (10,33),
nonadherence to therapy (34) or
health care availability (22). The
database used in the present study did not contain this
information, and future studies are required to establish the
associations between race, tumor grade, treatment response and
socioeconomic factors.
The increased prevalence of high tumor grade and
high tumor stage among AA women and younger age at diagnosis are
reported in other studies (14,17,22,35,36).
Therefore, the association of race with survival in each grade
subgroup may have arisen through confounding with age or tumor
stage. However, after controlling for tumor stage and age in the
present study, the association of race with cancer-specific
survival remained high and statistically significant. This suggests
that confounding with age and stage is not sufficient to explain
the disparity observed in grade I breast cancer patients between AA
and Caucasians. However, due to the relatively low number of
cancer-specific fatalities among patients diagnosed with grade I,
it is imperative to conduct larger studies on patients with grade I
tumors in order to determine whether the present results can be
generalized.
Women whose breast cancers are diagnosed as hormone
receptor-positive have better survival rates compared with women
with receptor-negative tumors, which is most likely associated with
the response of tumors to targeted therapies. Diagnosis for
triple-negative disease (tumors negative for estrogen receptor,
progesterone receptor and human epidermal growth factor receptor
2-neu) is particularly common in young AA patients, who are more
likely to suffer a recurrence, be diagnosed with distant metastasis
and have a poor prognosis (35,37–39).
Despite numerous reports showing that AA breast-cancer women have
poorer survival regardless of hormone-receptor status (40,41), there
is a possibility that the racial disparity observed in the current
cohort could be due to an increased frequency of triple-negative
patients in AA women. The hormone-receptor details required to
identify basal-like disease were not available for the present
study; as a result, the contributions of breast cancer subtypes in
the observed racial disparity could not be ruled in or out.
Although the possibility that differences in the prevalence of
triple-negative cancers contributed to the poorer survival among AA
women diagnosed with grade I cannot be excluded in the present
study, race disparity is likely to have been even more evident
between patients with high grade cancers if triple-negative
diagnosis was a contributing factor. Particularly, as a previous
study has shown, the increased incidence of basal-like tumors in AA
women is associated with higher-grade tumors (42). In other words, the ratio of
triple-negative to hormone-receptor positive patients is expected
to increase as tumor grade increases. Racial disparity was not
observed in grade-II or -III/IV patients; therefore, it is unlikely
that the racial disparity observed is due to an increased frequency
of triple-negative patients in AA women.
Another limitation of the present study is the
relatively short follow-up time that may potentially affect the
outcome of the study. Patients diagnosed with receptor-positive
tumors have a relatively better prognosis compared with patients
with triple-negative tumors. However this phenomenon is limited to
the first 5 years following diagnosis; as time passes, the positive
prognostic effect of estrogen receptor status fades away (43). Thus, a short follow-up tends to
capture early mortalities compared with a much longer follow-up
where the assessment of mortality would be inclusive of early and
delayed mortalities. Therefore, the mortality data in the present
study could benefit Caucasian over AA women due to a decreased
frequency of triple-negative tumors among Caucasian patients.
However, as no significant race disparity for grades II and III/IV
was observed, the likelihood of a triple-negative diagnosis
contributing to the observed racial disparity is diminished.
Nevertheless, caution should be exercised when interpreting the
results of the present study.
In conclusion, AA breast cancer patients displayed a
shorter breast cancer-specific survival time when diagnosed with
low-grade tumors. The results of the present study potentially
provide significant clinical and public health implications and
justify further investigation in larger cohorts.
Acknowledgements
The authors would like to thank the Winthrop P.
Rockefeller Cancer Institute (Little Rock, AR, USA) for supporting
the current project.
References
|
1
|
American Cancer Society: Cancer Facts
& Figures 2015. American Cancer Society, Inc. Atlanta, GA:
2015.
|
|
2
|
Ademuyiwa FO and Olopade OI: Racial
differences in genetic factors associated with breast cancer.
Cancer Metastasis Rev. 22:47–53. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chlebowski RT, Chen Z, Anderson GL, Rohan
T, Aragaki A, Lane D, Dolan NC, Paskett ED, McTiernan A, Hubbell
FA, et al: Ethnicity and breast cancer: Factors influencing
differences in incidence and outcome. J Natl Cancer Inst.
97:439–448. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Polite BN and Olopade OI: Breast cancer
and race: A rising tide does not lift all boats equally. Perspect
Biol Med. 48(Suppl 1): S166–S175. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
American Cancer Society: Breast Cancer
Facts & Figures 2013–2014. American Cancer Society, Inc.
Atlanta, GA: 2013.
|
|
6
|
Keeton KM, Jones ES and Sebastian S:
Breast cancer in Mississippi: Impact of race and residential
geographical setting on cancer at initial diagnosis. South Med J.
107:510–512. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
DeLancey JO, Thun MJ, Jemal A and Ward EM:
Recent trends in Black-White disparities in cancer mortality.
Cancer Epidemiol Biomarkers Prev. 17:2908–2912. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hunt BR, Whitman S and Hurlbert MS:
Increasing black: White disparities in breast cancer mortality in
the 50 largest cities in the United States. Cancer Epidemiol.
38:118–123. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
McCarthy AM, Yamartino P, Yang J, Bristol
M, Conant EF and Armstrong K: Racial differences in false-positive
mammogram rates: Results from the ACRIN digital mammographic
imaging screening trial (DMIST). Med Care. 53:673–678. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li CI, Malone KE and Daling JR:
Differences in breast cancer stage, treatment, and survival by race
and ethnicity. Arch Intern Med. 163:49–56. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Porter PL, Lund MJ, Lin MG, Yuan X, Liff
JM, Flagg EW, Coates RJ and Eley JW: Racial differences in the
expression of cell cycle-regulatory proteins in breast carcinoma.
Cancer. 100:2533–2542. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Amend K, Hicks D and Ambrosone CB: Breast
cancer in African-American women: Differences in tumor biology from
European-American women. Cancer Res. 66:8327–8330. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sarker M, Jatoi I and Becher H: Racial
differences in breast cancer survival in women under age 60. Breast
Cancer Res Treat. 106:135–141. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Baquet CR, Mishra SI, Commiskey P, Ellison
GL and DeShields M: Breast cancer epidemiology in blacks and
whites: Disparities in incidence, mortality, survival rates and
histology. J Natl Med Assoc. 100:480–488. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rakha EA, Reis-Filho JS, Baehner F, Dabbs
DJ, Decker T, Eusebi V, Fox SB, Ichihara S, Jacquemier J, Lakhani
SR, et al: Breast cancer prognostic classification in the molecular
era: The role of histological grade. Breast Cancer Res.
12:2072010.PubMed/NCBI
|
|
16
|
Soerjomataram I, Louwman MW, Ribot JG,
Roukema JA and Coebergh JW: An overview of prognostic factors for
long-term survivors of breast cancer. Breast Cancer Res Treat.
107:309–330. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Henson DE, Chu KC and Levine PH:
Histologic grade, stage and survival in breast carcinoma:
Comparison of African American and Caucasian women. Cancer.
98:908–917. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cunningham JE and Butler WM: Racial
disparities in female breast cancer in South Carolina: Clinical
evidence for a biological basis. Breast Cancer Res Treat.
88:161–176. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Edge S, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual (7th).
Springer-Verlag. New York, NY: 2010.
|
|
20
|
Albain KS, Unger JM, Crowley JJ, Coltman
CA Jr and Hershman DL: Racial disparities in cancer survival among
randomized clinical trials patients of the southwest oncology
group. J Natl Cancer Inst. 101:984–992. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mancino AT, Rubio IT, Henry-Tillman R,
Smith LF, Landes R, Spencer HJ, Erkman L and Klimberg VS: Racial
differences in breast cancer survival: The effect of residual
disease. J Surg Res. 100:161–165. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Danforth DN Jr: Disparities in breast
cancer outcomes between Caucasian and African American women: A
model for describing the relationship of biological and
nonbiological factors. Breast Cancer Res. 15:2082013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Iqbal J, Ginsburg O, Rochon PA, Sun P and
Narod SA: Differences in breast cancer stage at diagnosis and
cancer-specific survival by race and ethnicity in the United
States. JAMA. 313:165–173. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Balan V, Nangia-Makker P, Schwartz AG,
Jung YS, Tait L, Hogan V, Raz T, Wang Y, Yang ZQ, Wu GS, et al:
Racial disparity in breast cancer and functional germ line mutation
in galectin-3 (rs4644): A pilot study. Cancer Res. 68:10045–10050.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Field LA, Love B, Deyarmin B, Hooke JA,
Shriver CD and Ellsworth RE: Identification of differentially
expressed genes in breast tumors from African American compared
with Caucasian women. Cancer. 118:1334–1344. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Singh Kalla S, Tan QW, Brito C, De León M
and De León D: Insulin-like growth factors I and II receptors in
the breast cancer survival disparity among African-American women.
Growth Horm IGF Res. 20:245–254. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Stewart PA, Luks J, Roycik MD, Sang QX and
Zhang J: Differentially expressed transcripts and dysregulated
signaling pathways and networks in African American breast cancer.
PLoS One. 8:e824602013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Quan L, Gong Z, Yao S, Bandera EV, Zirpoli
G, Hwang H, Roberts M, Ciupak G, Davis W, Sucheston L, et al:
Cytokine and cytokine receptor genes of the adaptive immune
response are differentially associated with breast cancer risk in
American women of African and European ancestry. Int J Cancer.
134:1408–1421. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Walko CM, Combest AJ, Spasojevic I, Yu AY,
Bhushan S, Hull JH, Hoskins J, Armstrong D, Carey L, Collicio F and
Dees EC: The effect of aprepitant and race on the pharmacokinetics
of cyclophosphamide in breast cancer patients. Cancer Chemother
Pharmacol. 69:1189–1196. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Makhoul I, Klimberg VS, Korourian S,
Henry-Tillman RS, Siegel ER, Westbrook KC and Hutchins LF: Combined
neoadjuvant chemotherapy with bevacizumab improves pathologic
complete response in patients with hormone receptor negative
operable or locally advanced breast cancer. Am J Clin Oncol.
38:74–79. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gwyn K, Bondy ML, Cohen DS, Lund MJ, Liff
JM, Flagg EW, Brinton LA, Eley JW and Coates RJ: Racial differences
in diagnosis, treatment and clinical delays in a population-based
study of patients with newly diagnosed breast carcinoma. Cancer.
100:1595–1604. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
George P, Chandwani S, Gabel M, Ambrosone
CB, Rhoads G, Bandera EV and Demissie K: Diagnosis and surgical
delays in African American and white women with early-stage breast
cancer. J Womens Health (Larchmt). 24:209–2017. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Griggs JJ, Culakova E, Sorbero ME,
Poniewierski MS, Wolff DA, Crawford J, Dale DC and Lyman GH: Social
and racial differences in selection of breast cancer adjuvant
chemotherapy regimens. J Clin Oncol. 25:2522–2527. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Partridge AH, Wang PS, Winer EP and Avorn
J: Nonadherence to adjuvant tamoxifen therapy in women with primary
breast cancer. J Clin Oncol. 21:602–606. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Morris GJ, Naidu S, Topham AK, Guiles F,
Xu Y, McCue P, Schwartz GF, Park PK, Rosenberg AL, Brill K and
Mitchell EP: Differences in breast carcinoma characteristics in
newly diagnosed African-American and Caucasian patients: A
single-institution compilation compared with the national cancer
institute's surveillance, epidemiology and end results database.
Cancer. 110:876–884. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Barcenas CH, Wells J, Chong D, French J,
Looney SW and Samuel TA: Race as an independent risk factor for
breast cancer survival: Breast cancer outcomes from the medical
college of georgia tumor registry. Clin Breast Cancer. 10:59–63.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ihemelandu CU, Naab TJ, Mezghebe HM,
Makambi KH, Siram SM, Leffall LD Jr, Dewitty RL Jr and Frederick
WA: Basal cell-like (triple-negative) breast cancer, a predictor of
distant metastasis in African American women. Am J Surg.
195:153–158. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ihemelandu CU, Leffall LD Jr, Dewitty RL,
Naab TJ, Mezghebe HM, Makambi KH, Adams-Campbell L and Frederick
WA: Molecular breast cancer subtypes in premenopausal and
postmenopausal African-American women: Age-specific prevalence and
survival. J Surg Res. 143:109–118. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lund MJ, Trivers KF, Porter PL, Coates RJ,
Leyland-Jones B, Brawley OW, Flagg EW, O'Regan RM, Gabram SG and
Eley JW: Race and triple negative threats to breast cancer
survival: A population-based study in Atlanta, GA. Breast Cancer
Res Treat. 113:357–370. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Menashe I, Anderson WF, Jatoi I and
Rosenberg PS: Underlying causes of the black-white racial disparity
in breast cancer mortality: A population-based analysis. J Natl
Cancer Inst. 101:993–1000. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Schinkel JK, Zahm SH, Jatoi I, McGlynn KA,
Gallagher C, Schairer C, Shriver CD and Zhu K: Racial/ethnic
differences in breast cancer survival by inflammatory status and
hormonal receptor status: An analysis of the surveillance,
epidemiology and end results data. Cancer Causes Control.
25:959–968. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Carey LA, Perou CM, Livasy CA, Dressler
LG, Cowan D, Conway K, Karaca G, Troester MA, Tse CK, Edmiston S,
et al: Race, breast cancer subtypes, and survival in the Carolina
breast cancer study. JAMA. 295:2492–2502. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Bentzon N, Düring M, Rasmussen BB,
Mouridsen H and Kroman N: Prognostic effect of estrogen receptor
status across age in primary breast cancer. Int J Cancer.
122:1089–1094. 2008. View Article : Google Scholar : PubMed/NCBI
|