Introduction
Breast cancer (BC) is the most common malignancy in
women worldwide. Novel breast cancer cases and cancer-associated
mortalities accounted for 29 and 15%, respectively, of all female
cancers in 2015 (1). Lifestyle is
considered an important risk factor for BC. All types of physical
activity appear to reduce the risk of BC, although the evidence of
this association is stronger for BC occurring in post-menopausal
women than pre-menopausal women (2,3).
Studies have shown that the risk of BC is ~25% lower
in the most active trained women compared with sedentary women
(4,5).
The BC risk is 17% higher in sedentary women compared with women
that perform physical activity (6).
In addition, the risk of BC decreases by 5% for every 2 h per week
in women performing moderate or vigorous recreational activity
(7). Physical activity has also been
demonstrated to reduce the risk of BC recurrence in BC survivors
(8,9).
Therefore, The American Cancer Society recommends that cancer
survivors partake in 150 min of physical activity per week
(10,11).
The mechanism underlying the health benefits of
regular exercise may involve the cumulative anti-inflammatory
effects of repeated physical exercise (12,13).
Regular exercise promotes the synthesis of myokines that modulate
the inflammatory response (14). In
addition, exercise may affect the levels of matrix
metalloproteinases (MMPs) (15,16).
MMPs are a family of structurally and functionally
related proteinases that are characterized by their ability to
degrade the extracellular matrix (ECM), and their involvement in
the normal functioning of various tissues during growth,
development and aging (16,17). MMP expression is induced by a number
of factors, including inflammatory cytokines, hormones, growth
factors and oncogenes (18,19). In addition, MMPs are implicated in
tumor invasion and metastasis (20,21). MMP-2
and −9 have been reported to exhibit an important ECM homeostatic
function during muscle growth, development and repair processes
(16). Previous studies have
demonstrated that physical exercise affects the levels of MMPs
following acute and chronic therapies in humans (22–24). A
marginal increase in MMP-9, but not MMP-2, serum concentration has
been demonstrated to occur following acute physical exercise
(25). In particular, MMP-2 and −9
serum levels increase following exercise training that incorporates
resistance-type exercise, as the mechanical stressors result in ECM
remodeling (26). MMP-2 and −9
hydrolyze components of the basement membrane, and regulate tumor
growth and metastasis (27).
Activated MMP-2 is located in the protruding section of the
cell-penetrating matrix. Its activation facilitates the passage of
tumor cells through the ECM and the basal membrane of the blood
vessel wall, thus promoting invasion of tumor cells (28). In addition, MMP-2 and −9 are
gelatinases; thus, their role in the degradation of gelatin leads
to the release of signaling molecules from the ECM that aid cell
migration and angiogenesis (29).
Previous studies have investigated the effects of acute short
duration exercise on MMP concentrations in skeletal muscle and
plasma (30,31). However, it remains unclear whether
different exercise training programs promote different MMP
responses (32). To the best of our
knowledge, no previous studies have investigated the effect of
exercise on the modulation of MMP-2 or −9 serum concentration in BC
survivors.
In our previous study, it was demonstrated that
muscle-derived cytokines are released following a dragon boat
training program and the resulting decreased oxidative stress
conditions are responsible for the health benefits observed in
patients with BC (14). In the
present study, the effect of two different exercise training
programs on MMP-2 and −9 serum concentration was investigated in BC
survivors and healthy subjects. In addition, the association
between MMP serum concentration and lymph node metastasis was
investigated in BC survivors. The patients enrolled in the current
study were active individuals involved in dragon boat paddling or
other recreational physical activities.
Dragon boat paddling is a competitive sport that
originated in China >2,000 years ago (33). Dragon boat paddling is a repetitive,
vigorous physical exercise that increases flexibility, aerobic
capacity and strength, and provides a novel approach for upper body
rehabilitation following breast surgery and radiation treatment.
This exercise has been reported to reduce the risk of developing
lymphedema in women at the highest risk by 70% (34).
The present study may have important implications
for BC survivors, with regard to their lifestyle choices and
participation in physical activity.
Patients and methods
Patients
A total of 66 women were enrolled in the present
study, between May and December 2014, in collaboration with
Associazione Pagaie Rosa Dragon Boat Onlus (www.pagaierosa.org). The cohort included 46 women who
were BC survivors and 20 healthy subjects. Blood from patients was
drawn at the Day Hospital of Don Gnocchi Foundation (Rome, Italy).
BC survivors were divided into three different groups: Group A, 17
women who participated in recreational dragon boat paddling (mean ±
standard deviation age, 53.4±8.8 years); group B, 14 women who
participated in other recreational physical activities (age,
53.9±11.2 years); and group C, 15 sedentary women (age, 59.6±9.9
years). The 20 healthy women were divided in two groups: Group D,
10 women who participated in other recreational physical activities
(age, 49.4±7.8 years); and group E, 10 sedentary women (age,
51.0±8.1 years) (Table I). All the BC
survivors were enrolled 10±5 years post-surgery. The exclusion
criteria included cardiovascular disease, acute somatic symptoms,
including fever or infection, uncontrolled hypertension,
uncontrolled pain or any other condition that contraindicated
exercise training in BC survivors or healthy subjects (35). It was not possible to enroll a control
group of healthy subjects who participate in dragon boat racing as
there is only a small number of individuals who play this sport in
Rome. In addition, the effects of dragon boat mediated-release of
MMPs in healthy subjects was not part of the scope of the present
study.
 | Table I.Anthropometric parameters of enrolled
subjects. |
Table I.
Anthropometric parameters of enrolled
subjects.
| Group | Subject status | Type of physical
activity | Enrolled subjects,
n | Age,
yearsa | Height,
cma | Weight,
kga | BMIa |
|---|
| A | BC | Dragon boat
paddling | 17 | 53.4±8.8 | 161.9±7.5 | 60.2±9.4 | 22.9±2.4 |
| B | BC | Recreational
physical activity | 14 |
53.9±11.2 | 164.2±7.9 | 64.3±10.2 | 23.9±3.5 |
| C | BC | Sedentary | 15 | 59.6±9.9 | 164.1±5.8 | 67.4±9.1 | 25.0±3.3 |
| D | H | Recreational
physical activity | 10 | 49.4±7.8 | 164.3±2.5 | 61.6±5.4 | 22.9±2.4 |
| E | H | Sedentary | 10 | 51.1±8.1 | 163.3±4.1 | 56.3±6.0 | 21.2±3.0 |
Anthropometric parameters, including height, weight
and body mass index (BMI), were determined for all participants at
the beginning of the study (Table I).
The TNM status was also determined for all the patients (Table II) (36). No clinical or radiographic evidence of
distant metastases were present.
| Table II.Tumor stage and lymph node metastasis
of breast cancer survivors (n=46). |
Table II.
Tumor stage and lymph node metastasis
of breast cancer survivors (n=46).
| Parameter | Patients, n |
|---|
| Tumor stage |
|
| I | 24 |
| II | 14 |
|
III | 8 |
| Lymph node
metastasis |
|
|
Present | 25 |
|
Absent | 21 |
| Histological
type |
|
|
Ductal | 42 |
|
Lobular | 4 |
The present study was performed in accordance with
the Declaration of Helsinki and written informed consent was
provided by all subjects prior to enrolling in the study. The study
was approved by the ethics committee of the Fondazione Policlinico
Tor Vergata (Study Design DRAGON BOAT-REGISTRO SPERIMENTAZIONI
protocol number 150/13).
Training program
The present study did not involve analysis of MMPs
prior to training. Thus, the training program did not have a
specific duration, and patients could be enrolled at any time
during their training. All subjects from groups A, B and D were
already performing identical physical activities to those described
below prior to the start of the study. Sedentary subjects were only
in groups C and E.
Group A
All subjects in group A participated in recreational
dragon boat paddling once a week for 120 min, and were supervised
by an exercise trainer.
The 120-min dragon boat paddling session included a
30 min dry land warm up as activation exercise for the whole body,
followed by 90 min of dragon boat paddling training. The dragon
boat paddling training consisted of: A 20-min rowing warm up on the
right and left sides of the boat (changing side every 10 min for
symmetric training); 50 min rowing with stroke-rate regulated by
sound feedback (tambourine) and rowing technical skill exercises
(resting in relation to the intensity of the exercise); and 10 min
training on competition distances (200 or 500 meters repeated at
last twice). Finally, the subjects performed a 10 min cool-down and
10 min of stretching exercises, focusing on the upper limbs.
Groups B and D
All subjects in groups B and D participated in other
recreational physical activities (the same for the two groups) 3
times a week for 60 min, and were supervised by an exercise
trainer.
The 60-min recreational physical activities included
a 10-min warm-up, 30 min endurance training (treadmill 6.5–8.0
km/h, cyclette 55–65 rpm or aerobic dance) and 20 min strength
training (2–4 kg). The warm up involved large muscle groups with
low-intensity activities (slow run and execution of joint mobility
exercises), gradually preparing the body to pass from the rest
condition to the state of activation, with progressive increase of
intensity. Aerobic dance, performed to music, was physical exercise
that combined rhythmic aerobic exercise with strength training
routines to improve flexibility, muscular strength and
cardiovascular fitness. Finally, the subjects performed 10 min of
stretching exercises. Each subject enrolled in groups B and D
performed treadmill, cyclette or aerobic dance alternately during
the week.
Measurement of MMP-2 and −9
levels
Serum samples were obtained during the training
program. Blood was drawn without anticoagulant a total of 48 h
after training (and between two training sessions) from all
subjects between 9:00 and 10:00 a.m., following an overnight fast,
and was allowed to coagulate for 20–30 min. Blood samples were not
obtained before the training program began as the aim of the
present study was to compare the effects of various physical
activities on the circulating levels of MMP-2 and MMP-9 in
well-trained subjects. Serum was separated by centrifugation (800 ×
g for 10 min at 4°C), and all specimens were aliquoted, frozen and
stored at −80°C within 2 h of collection. Commercially available
human ELISA kits (high-sensitivity Quantikine; catalog nos., MMP200
and DMP900; R&D Systems, Inc., Minneapolis, MN, USA) were used
to determine the MMP-2 and −9 levels, according to the
manufacturer's instructions. Optical density was measured using a
microplate reader at a wavelength of 450 nm (Model 550; Bio-Rad
Laboratories, Inc., Hercules, CA, USA).
Statistical analysis
All data were initially entered into a Microsoft
Excel for Office 2007 database (Microsoft Corporation, Redmond, WA,
USA) and statistical analysis was performed using SPSS version 19.0
(IBM SPSS, Armonk, NY, USA). Data are presented as the mean ±
standard deviation for parameters with (normal) Gaussian
distributions (following confirmation with histograms and the
Kolgomorov-Smirnov test) or as frequencies (%) for occurrences.
All data obtained were compared by using one-way
analysis of variance. Significant results were examined by
Bonferroni's test for one or more factors, respectively. P<0.05
was considered to indicate a statistically significant
difference.
To determine the number of samples necessary in each
group, power analysis was performed based on an α of 5% and
variation of 40% of the variable outcome MMP-2. The t-test showed
that an amplitude of n=8 for both groups reached a power (1-β) of
94%. This was only calculated for MMP-2 as it was the only
significantly modified parameter. The variation of MMP-9
concentration was not significant.
Results
No significant differences in age or height were
observed between the groups. Conversely, the weight (group C vs.
group E, P=0.024) and BMI (group C vs. group E, P=0.035) were
significantly higher in sedentary BC survivors in comparison with
healthy sedentary women (Table I).
Table II shows tumor stage and lymph
node metastasis of breast cancer survivors enrolled in the
study.
To determine the effect of physical exercise on
MMP-2 and −9 serum concentration in BC survivors and healthy
subjects, two different exercises training programs were compared.
The results revealed a difference in MMP serum concentration
between BC survivors and healthy subjects participating in
different exercise programs.
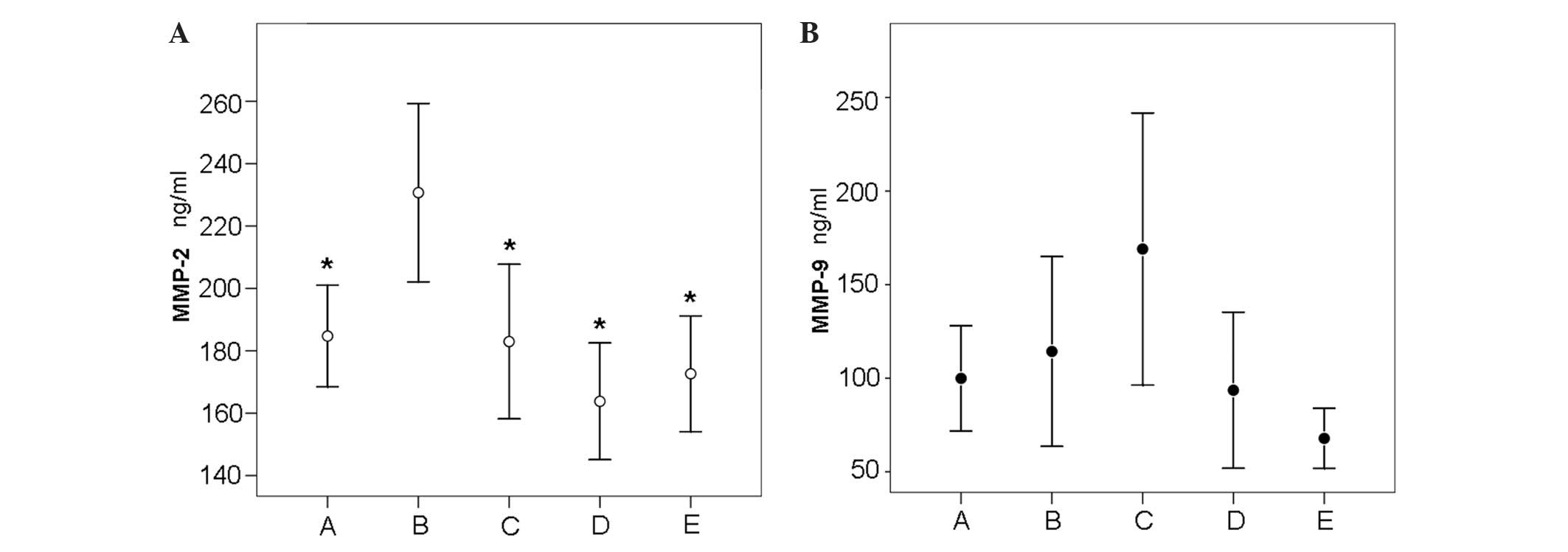
Specifically, the MMP-2 serum concentration was
significantly increased in the sera of BC survivors participating
in recreational physical activity (group B) compared with those
participating in dragon boat paddling (group A; B vs. A, P=0.028),
or with sedentary BC survivors (group C; B vs. C, P=0.008; Fig. 1A). Statistically significant
differences were observed between group B (230.7±49.5) and group A
(184.7±31.7; P=0.028) and between group B and group C (182.9±44.8;
P=0.008).
However, no significant differences in MMP-2 serum
concentration were identified between BC patients participating in
dragon boat paddling (group A) and sedentary BC survivors (group C;
P=0.999). Notably, the mean MMP-2 serum concentration was
significantly higher in BC survivors participating in recreational
physical activity (group B, 230.7±49.5) compared with healthy
subjects participating in recreational physical activity (group D;
163.8±26.1; P=0.001) and between group B and sedentary healthy
subjects in group E (172.6±25.9; P=0.021). By contrast, no
significant differences in mean MMP-2 levels were identified
between the sedentary BC survivors (group C; 182.9±44.8) and
sedentary healthy subjects (group E; 172.6±25.9; P=0.999).
The effect of exercise on MMP-9 serum concentration
revealed a different trend between BC survivors and healthy
subjects. Notably, physical exercise decreased the MMP-9 levels in
BC survivors in group A and group B compared to group C, while it
increased the MMP-9 serum levels in healthy subjects in group D
compared with group E (Fig. 1B).
Although variations in mean MMP-9 levels were
identified between dragon boat paddling BC survivors and sedentary
BC survivors (group A, 99.9±54.5; group C, 169.0±131.2; P=0.679),
recreational physical activity BC survivors and sedentary BC
survivors (group B, 114.3±87.8; group C, 169.0±131.2; P=0.999), and
healthy recreational physical activity and healthy sedentary
individuals (group D, 93.6.3±58.3; group E, 67.8±22.5; P=0.999),
these differences were not statistically significant (Table III).
| Table III.Serum matrix metalloproteinase-9
concentration in BC dragon boat group (A), BC physical activity
group (B), BC sedentary group (C), H physical activity group (D)
and H sedentary group (E). |
Table III.
Serum matrix metalloproteinase-9
concentration in BC dragon boat group (A), BC physical activity
group (B), BC sedentary group (C), H physical activity group (D)
and H sedentary group (E).
| Dragon
boat/physical activity group (mean ± sd) | Sedentary group
(mean ± sd) | P-value |
|---|
| A (99.9±54.5) | C
(160.9±131.2) | 0.679 |
| B (114.3 ±
87.8) | C
(160.9±131.2) | 0.999 |
| D (93.6 ±
58.3) | E (67.8 ±
22.5) | 0.999 |
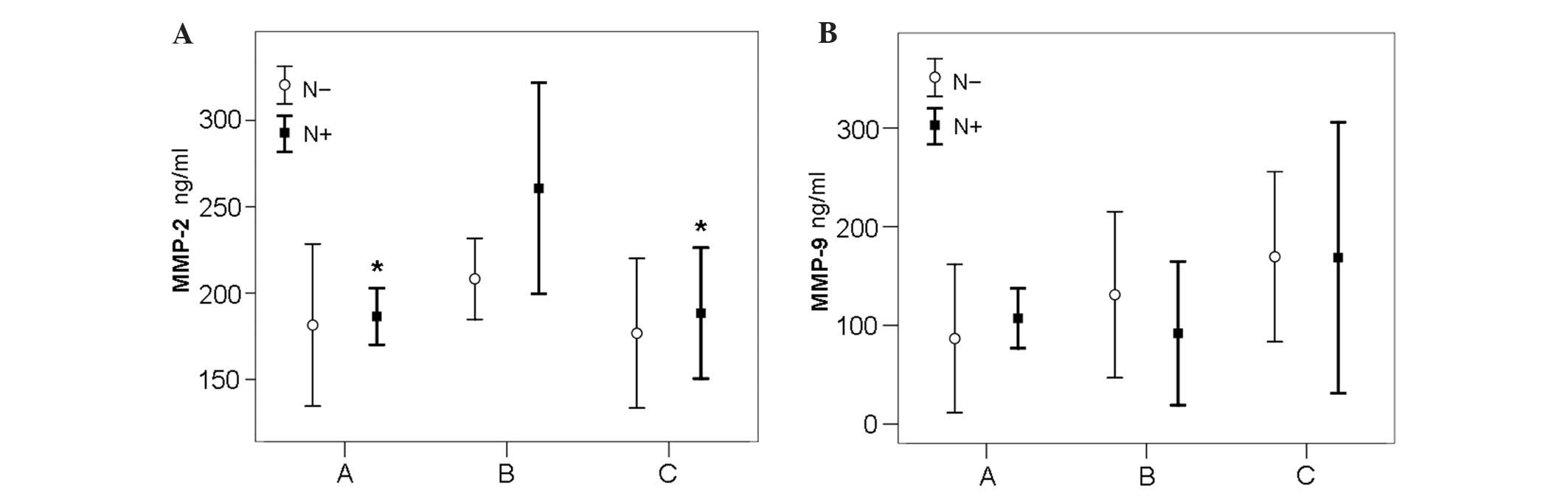
The association between MMP-2 and −9 serum levels,
and the presence of lymph node metastasis were also investigated in
groups A-C. No statistical differences in mean MMP-2 serum levels
were identified between lymph node metastasis positive (N+) BC
survivors of the dragon boat paddling group (group A; 186.5±24.4)
and N+ sedentary BC survivors (group C; 188.4±45.3) or between the
lymph node metastasis negative (N-) BC survivors of the dragon boat
paddling group (group A; 181.5±44.7) and the N- sedentary BC
survivors (group C; 176.7±46.8) (Fig.
2).
However, significant differences in mean MMP-2 serum
levels were identified between N+ BC survivors that participated in
recreational physical activity (group B; 260.7±58.2) and N+
sedentary BC survivors (group C; 188.4±45.3; P=0.013). No
significant differences were identified between N- BC survivors
participating in recreational physical activity (group B;
208.2±28.1) and N- sedentary BC survivors (group C; 176.7±46.8;
P=0.913). MMP-2 serum levels were significantly higher in N+ BC
survivors of the recreational physical activity group (group B;
260.7±58.2) compared with N+ BC survivors of the dragon boat
paddling group (group A; 186.5±24.4; P=0.007) (Fig. 2). No significant differences were
observed in MMP-9 serum levels between the N- and N+ subgroups
among groups A-C.
Discussion
Regular physical exercise improves physical
function, quality of life and reduces fatigue in BC survivors
(37,38). It also decreases the risk of BC
recurrence and reduces BC-specific mortality in BC survivors
(39,40).
Physical exercise is considered an essential factor
for improving cancer survival. Previous studies have indicated that
exercise interventions are efficacious in men with prostate cancer
(41,42) and in multiple myeloma (43,44). In
endometrial, ovarian and colorectal cancer survivors, lifestyle
interventions that include regular participation in physical
activity are associated with positive health outcomes (45,46).
Furthermore, it has been demonstrated that individuals who are
physically active after being diagnosed with breast or colon cancer
exhibit a higher rate of survival compared with those that are
physically inactive (47).
Circulating MMPs are involved in the breakdown of
the ECM in carcinogenesis and cardiovascular diseases (48). MMPs modulate the activation of growth
factors, cytokines and angiogenesis, facilitating physiological
adaptations to exercise (18,49).
However, high levels of mechanical stress, such as
that induced by high physical impact exercise, may activate the
local production of MMPs in skeletal muscle. Rullman et al
(50) reported that a single session
of exercise induces MMP-9 activation, causing a marked increase in
serum MMP-9 concentration. Kadoglou et al (24) demonstrated that exercise reduces MMP-9
serum levels, but not MMP-2 levels, in patients with type 2
diabetes. Additional studies have investigated the function of
circulating MMP-2 and MMP-9 in BC patients (51,52); the
results revealed increased MMP-9 expression and activity in
malignant tumors, and enhanced MMP-2 activity in malignant tumors
exhibiting high estrogen receptor expression. These studies
indicate that serum levels of MMP-2 or −9 may present useful
markers for the staging and prognosis of BC and other types of
cancer (53), such as prostate
adenocarcinoma, in association with prostate-specific antigen
levels, gastric cancer and lung carcinoma (54–56).
At present, the effect of different exercise
training programs on MMP-9 and −2 serum levels in human subjects
remains unclear (57). It was
previously demonstrated that endurance training decreases MMP-9
concentration (58) and aerobic
training reduces MMP-2 plasma levels in individuals with
pathological conditions (25). Urso
et al (26) observed that the
variation in MMP-2 and −9 serum levels is dependent on different
exercise training regimens. Thus, understanding which type of
exercise and intensity may reduce the risk of recurrence in BC
patients is important.
The aim of the present study was to determine the
effect of two different exercise training programs on the serum
MMP-2 and −9 levels of healthy subjects and BC survivors. The
results did not identify any significant differences in MMP-2 serum
levels in healthy subjects that participated in recreational
physical activity; there were no significant differences in MMP-2
serum levels in group D compared with group E, and although MMP-9
levels increased in group D compared with group E, these
differences were not statistically significant. Among the BC
survivors, no significant differences in circulating MMP-2 levels
were identified between the dragon boat paddling (group A) and
sedentary (group C) groups. However, a significant increase in
serum MMP-2 was identified in the recreational physical activity BC
group (group B) compared with the sedentary BC group (group C).
This difference in circulating MMP-2 levels following exercise
appears to be dependent on the different exercise training programs
undertaken by the BC survivors; however, the same exercise program
did not induce significant increases in the MMP-2 levels of healthy
subjects.
MMP-9 serum levels were higher in sedentary BC
survivors (group C) than in healthy subjects (group E).
Furthermore, MMP-9 serum levels were decreased in both groups of
recreationally active BC survivors (groups A and B) compared with
sedentary BC survivors (group C). This result may be associated
with tumor necrosis factor-α (TNF-α) expression, as TNF-α is a
stimulator of MMP-9 production and is decreased following exercise
(59,60).
However, exercise increased MMP-9 serum levels in
the healthy subjects (group D vs. E). This difference reflects the
impact of exercise training and may be associated with an
inflammatory response (61). Rullman
et al (62) reported that
endurance exercise enhances MMP-9 but not MMP-2 levels in human
skeletal muscle in healthy subjects.
Our previous study regarding exercise in BC patients
contributed to the understanding of the modulatory effects of
exercise on MMP-2 and MMP-9 regulation. It was demonstrated that
muscle-derived cytokines are released following a training program,
while decreasing the oxidative stress (14). Changes in MMP serum levels may reflect
the impact of exercise on the production of inflammatory molecules.
It is hypothesized that exercise causes a reduction in free
radicals and an increase in antioxidant defenses, which may
influence the inflammatory conditions and subsequently alter MMP
serum concentrations. The different effects of exercise observed on
MMP-2 and −9 serum levels may be associated with different
dose-dependent responses to physical activity (57).
The results of the present study indicate that the
type of physical exercise (intensity, volume, frequency and length)
may effect MMP-2 and MMP-9 plasma levels. The effect of the same
exercise program was different in healthy subjects and BC
survivors. To the best of our knowledge, it remains to be
elucidated why this differential response occurs. To understand
these findings, it is helpful to analyze the weekly frequency of
exercise, as well as the period of rest and the muscle strength
applied. In the present study, exercise was performed once a week
for 120 min with a rest time of 6 days in the dragon boat paddling
group (group A). The muscle strength applied during paddling is
proportionate to an anti-gravity exercise in accordance with the
variables of hydrodynamics. The other recreational physical
activity groups (group B and D) trained 3 times a week for 60 min,
and thus the rest time was shorter than that of the dragon boat
paddling group. For groups B and D, the muscle strength applied was
proportionate to the extra load used during the exercise session
without the benefit of hypogravity. All these variables have been
shown to affect MMP-2 serum levels in BC survivors.
Coagulation enzymes are involved in MMP-2 activation
for example, urokinase plasminogen converts plasminogen to plasmin,
which promotes tumor growth and angiogenesis, degrading the ECM and
basement membrane, and activating pro-MMPs (63). MMPs and urokinase plasminogen
activators are involved in tumor invasion and metastasis. The
results of the present study demonstrated that BC survivors exhibit
increased MMP-2 levels when compared with healthy subjects. These
results may be due to an increase in urokinase plasminogen
activator expression, as it has been demonstrated that exercise
increases plasma fibrinolytic activity. Furthermore, exhaustive
exercise is associated with increased expression of plasminogen
activator in plasma (64), and
exercise-stimulated thrombin and plasmin generation were previously
identified in healthy subjects that exercised for a significantly
longer duration (65). Prolonged
physical exercise is associated with numerous changes in blood
hemostasis and higher levels of aerobic fitness are associated with
increased fibrinolytic activity (66,67), while
MMP-2 activation is inhibited by plasmin inhibitors (68).
Previous studies have reported that serum levels of
MMP-2 and MMP-9 are significantly higher in BC patients than in
control subjects (69,70). Furthermore, patients with N+ cancer
exhibit significantly higher MMP-2 and MMP-9 activity than those
with N- cancer (53). The results
obtained in the present study revealed a significant increase in
MMP-2 but not MMP-9 concentration in N+ BC survivors compared with
N- BC survivors. Furthermore, different exercise regimes exhibited
different effects on circulating MMP-2 and MMP-9 levels.
In conclusion, the contradictory results obtained in
the present study may be due to the fact that exercise of various
intensities were performed in previous studies. Therefore, further
studies are required to determine the biological significance of
MMP levels in the adaptation of skeletal muscle to physical
activity in cancer patients and to explore how different types of
physical exercise affect MMP production. Overall, the results of
the present study indicate that various physical activities
modulate the levels of circulating MMP-2 and −9 in BC survivors,
and an identical exercise program induces a contrasting effect when
undertaken by healthy subjects and BC survivors.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
World Cancer Research Fund/American
Institute for Cancer Research: Food, Nutrition, Physical Activity
and the Prevention of Cancer: A Global Perspective. AICR.
Washington DC: 2007.
|
|
3
|
Hildebrand JS, Gapstur SM, Campbell PT,
Gaudet MM and Patel AV: Recreational physical activity and
leisure-time sitting in relation to postmenopausal breast cancer
risk. Cancer Epidemiol Biomarkers Prev. 22:1906–1912. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Friedenreich CM, Neilson HK and Lynch BM:
State of the epidemiological evidence on physical activity and
cancer prevention. Eur J Cancer. 46:2593–2604. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Eliassen AH, Hankinson SE, Rosner B,
Holmes MD and Willett WC: Physical activity and risk of breast
cancer among postmenopausal women. Arch Intern Med. 170:1758–1764.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shen D, Mao W, Liu T, Lin Q, Lu X, Wang Q,
Lin F, Ekelund U and Wijndaele K: Sedentary behavior and incident
cancer: A meta-analysis of prospective studies. PLoS One.
9:e1057092014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wu Y, Zhang D and Kang S: Physical
activity and risk of breast cancer: A meta-analysis of prospective
studies. Breast Cancer Res Treat. 137:869–882. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Holmes MD, Chen WY, Feskanich D, Kroenke
CH and Colditz GA: Physical activity and survival after breast
cancer diagnosis. JAMA. 293:2479–2486. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Holick CN, Newcomb PA, Trentham-Dietz A,
Titus-Ernstoff L, Bersch AJ, Stampfer MJ, Baron JA, Egan KM and
Willett WC: Physical activity and survival after diagnosis of
invasive breast cancer. Cancer Epidemiol Biomarkers Prev.
17:379–386. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schmid D and Leitzmann MF: Association
between physical activity and mortality among breast cancer and
colorectal cancer survivors: A systematic review and meta-analysis.
Ann Oncol. 25:1293–1311. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rock CL, Doyle C, Demark-Wahnefried W,
Meyerhardt J, Courneya KS, Schwartz AL, Bandera EV, Hamilton KK,
Grant B, McCullough M, et al: Nutrition and physical activity
guidelines for cancer survivors. CA Cancer J Clin. 62:243–274.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pinto A, Di Raimondo D, Tuttolomondo A,
Buttà C, Milio G and Licata G: Effects of physical exercise on
inflammatory markers of atherosclerosis. Curr Pharm Des.
18:4326–4349. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Crisafulli A, Tocco F, Melis F, Milia R
and Concu A: Natural killer cells responsiveness to physical
exercise: A brief review. Open J Immunol. 3:190–200. 2013.
View Article : Google Scholar
|
|
14
|
Tresoldi I, Foti C, Masuelli L, Frajese
GV, Rossi P, Modesti A, Bei R and Giganti MG: Effects of dragon
boat training on cytokine production and oxidative stress in breast
cancer patients: A pilot study. Open J Immunol. 4:22–29. 2014.
View Article : Google Scholar
|
|
15
|
Ramin A, Abbas M, Ali Abbas G, Asghar R,
Amir L, Farshid S and Hussein B: Effects of exhaustive aerobic
exercise on matrix metaloproteases activity in athletes and
non-athletes. World J Sport Sci. 4:185–191. 2011.
|
|
16
|
Madden MC, Byrnes WC, Lebin JA, Batliner
ME and Allen DL: Plasma matrix metalloproteinase-9 response to
eccentric exercise of the elbow flexors. Eur J Appl Physiol.
111:1795–1805. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Carmeli E, Moas M, Reznick AZ and Coleman
R: Matrix metalloproteinases and skeletal muscle: A brief review.
Muscle Nerve. 29:191–197. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Benz CC: Transcriptional factors and
breast cancer. Endoc Rel Cancer. 5:271–282. 1998. View Article : Google Scholar
|
|
19
|
Giunciuglio D, Culty M, Fassina G,
Masiello L, Melchiori A, Paglialunga G, Arand G, Ciardiello F,
Basolo F, Thomson EW, et al: Invasive phenotype of MCF10A cells
overexpressing c-Ha-ras and c-erbB-2 oncogenes. Int J Cancer.
63:815–822. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chambers AF and Matrisian LM: Changing
views of the role of matrix metalloproteinases in metastasis. J
Natl Cancer Inst. 89:1260–1270. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cocket MI, Murohy G, Birch ML, O'Connell
JP, Crabbe T, Millican AT, Hart IR and Dochery AJ: Matrix
metalloproteinase and metastatic cancer. Biochem Soc Symp.
63:295–313. 1998.PubMed/NCBI
|
|
22
|
Lucotti P, Monti LD, Setola E, Galluccio
E, Gatti R, Bosi E and Piatti P: Aerobic and resistance training
effects compared to aerobic training alone in obese type2 diabetic
patients on diet treatment. Diabetes Res Clin Pract. 94:395–403.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bellafiore M, Battaglia G, Bianco A,
Farina F, Palma A and Paoli A: The involvement of MMP-2 and MMP-9
in heart exercise-related angiogenesis. J Transl Med. 11:2832013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kadoglou NP, Vrabas IS, Sailer N,
Kapelouzou A, Fotiadis G, Noussios G, Karayannacos PE and
Angelopoulou A: Exercise ameliorates serum MMP-9 and TIMP-2 levels
in patients with type 2 diabetes. Diabetes Metab. 36:144–151. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Koskinen SO, Höyhtyä M,
Turpeenniemi-Hujanen T, Martikkala V, Mäkinen TT, Oksa J, Rintamäki
H, Löfberg M, Somer H and Takala TE: Serum concentrations of
collagen degrading enzymes and their inhibitors after downhill
running. Scand J Med Sci Sports. 11:9–15. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Urso ML, Pierce JR, Alemany JA, Harman EA
and Nindl B: Effects of exercise training on the matrix
metalloprotease response to acute exercise. Eur J Appl Physiol.
106:655–663. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jacob A, Jing J, Lee J, Schedin P, Gilbert
SM, Peden AA, Junutula JR and Prekeris R: Rab40b regulates
trafficking of MMP2 and MMP9 during invadopodia formation and
invasion of breast cancer cells. J Cell Sci. 126:4647–4658. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu RR, Li MD, Li T, Tan Y, Zhang M and
Chen JC: Matrix metalloproteinase 2 (MMP2) protein expression and
laryngeal cancer prognosis: A meta analysis. Int J Clin Exp Med.
8:2261–2266. 2015.PubMed/NCBI
|
|
29
|
Jacob A and Prekeris R: The regulation of
MMP targeting to invadopodia during cancer metastasis. Front Cell
Dev Biol. 3:42015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Mackey AL, Donnelly AE, Swanton A, Murray
F and Turpeenniemi-Hujanen T: The effects of impact and non-impact
exercise on circulating markers of collagen remodeling in humans. J
Sports Sci. 24:843–848. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mackey AL, Donnelly AE,
Turpeeniemi-Hujanen T and Proper HP: Skeletal muscle collagen
content in humans after high-force eccentric contractions. J Appl
Physiol (1985). 97:197–203. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Niessner A, Richter B, Penka M, Steiner S,
Strasser B, Ziegler S, Heeb-Elze E, Zorn G, Leitner-Heinschink A,
Niessner C, et al: Endurance training reduces circulating
inflammatory markers in persons at risk of coronary events: Impact
plaque stabilization? Atheroscleorosis. 186:160–165. 2006.
View Article : Google Scholar
|
|
33
|
Harris SR: “We're all in the same boat”: A
review of the benefits of dragon boat racing for women living with
breast cancer. Evid Based Complement Alternat Med. 2012:1676512012.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lane K, Jespersen D and McKenzie DC: The
effect of a whole body exercise programme and dragon boat training
on arm volume and arm circumference in women treated for breast
cancer. Eur J Cancer Care (Engl). 14:353–358. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lucia A, Earnest C and Pérez M:
Changed-related fatigue: Can exercise physiology assist oncologys?
Lancet Oncol. 4:616–625. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Sobin LH, Gospodarowicz MK and Wittekind
Ch: TNM Classification of Malignant Tumors (7th). Wiley-Blackwell.
Oxford: 4–15. 2009.
|
|
37
|
Irwin ML: Physical activity interventions
for cancer survivors. Br J Sports Med. 43:32–38. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Winters-Stone KM, Schwartz A and Nail LM:
A review of exercise interventions to improve bone health in adult
cancer survivors. J Cancer Surviv. 4:187–201. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Holmes MD, Chen WY, Feskanich D, Kroenke
CH and Colditz GA: Physical activity and survival after breast
cancer diagnosis. JAMA. 293:2479–2486. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Irwin ML, Crumley D, McTiernan A,
Bernstein L, Baumgartner R, Gilliland FD, Kriska A and
Ballard-Barbash R: Physical activity levels before and after a
diagnosis of breast carcinoma: The health, eating, activity and
lifestyle (HEAL) study. Cancer. 97:1746–1757. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Nilsen TS, Thorsen L, Kirkegaard C,
Ugelstad I, Fosså SD and Raastad T: The effect of strength training
on muscle cellular stress in prostate cancer patients on ADT.
Endocr Connect. 5:74–82. 2016.PubMed/NCBI
|
|
42
|
Skinner TL, Peeters GG, Croci I, Bell KR,
Burton NW, Chambers SK and Bolam KA: Impact of a brief exercise
program on the physical and psychosocial health of prostate cancer
survivors: A pilot study. Asia Pac J Clin Oncol. Feb 28–2016.(Epub
ahead of print). View Article : Google Scholar
|
|
43
|
Shallwani S, Dalzell MA, Sateren W and
O'Brien S: Exercise compliance among patients with multiple myeloma
undergoing chemotherapy: A retrospective study. Support Care
Cancer. 23:3081–3088. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Jones LW, Courneya KS, Vallance JK, Ladha
AB, Mant MJ, Belch AR, Stewart DA and Reiman T: Association between
exercise and quality of life in multiple myeloma cancer survivors.
Support Care Cancer. 12:780–788. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Smits A, Lopes A, Das N, Bekkers R,
Massuger L and Galaal K: The effect of lifestyle interventions on
the quality of life of gynaecological cancer survivors: A
systematic review and meta-analysis. Gynecol Oncol. 139:546–552.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Meyerhardt J, Heseltine D, Niedzwiecki D,
Hollis D, Saltz LB, Mayer RJ, Thomas J, Nelson H, Whittom R, Hantel
A, et al: Impact of physical activity on cancer recurrence and
survival in patients with stage III colon cancer: Findings from
CALGB 89803. J Clin Oncol. 24:3535–3541. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Bourke L, Smith D, Steed L, Hooper R,
Carter A, Catto J, Albertsen PC, Tombal B, Payne HA and Rosario DJ:
Exercise for men with prostate cancer: A systematic review and
meta-analysis. Eur Urol. 26:693–703. 2016. View Article : Google Scholar
|
|
48
|
Parks WC and Mecham RP: Matrix
metaloproteinasis. Academic Press. San Diego: 299–356. 1998.
|
|
49
|
Carmeli E, Haimovitch TG and Nemcovsky CE:
Expression of matrix metalloproteinase 2 and heat shock protein-72
in immobilized muscle in rats. J Musculoskelet Neuronal Interact.
6:96–102. 2006.PubMed/NCBI
|
|
50
|
Rullman E, Olsson K, Wagsater D and
Gustafsson T: Circulating MMP-9 during exercise in humans. Eur J
Appl Physiol. 113:1249–1255. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Somiari SB, Somiari RI, Heckman CM, Olsen
CH, Jordan RM, Russell SJ and Shriver CD: Circulating MMP2 and MMP9
in breast cancer: Potential role in classification of patients into
low risk, high risk, benign disease and breast cancer categories.
Int J Cancer. 119:1403–1411. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Jinga DC, Blidaru A, Condrea I, Ardeleanu
C, Dragomir C, Szegli G, Stefanescu M and Matache C: MMP-9 and
MMP-2 gelatinases and TIMP-1 and TIMP-2 inhibitors in breast
cancer: Correlations with prognostic factors. J Cell Mol Med Vol.
10:499–510. 2006. View Article : Google Scholar
|
|
53
|
Li HC, Cao DC, Liu Y, Hou YF, Wu J, Lu JS,
Di GH, Liu G, Li FM, Ou ZL, et al: Prognostic value of matrix
metalloproteinase (MMP-2 and MMP-9) in patients with lymph
node-negative breast carcinoma. Breast Cancer Res Treat. 88:75–85.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Morgia G, Falsaperla M, Malaponte G,
Madonia M, Indelicato M, Travali S and Mazzarino MC: Matrix
metalloproteinases as diagnostic (MMP-13) and prognostic (MMP-2,
MMP-9) markers of prostate cancer. Urol Res. 33:44–50. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Mönig SP, Baldus SE, Hennecken JK,
Spiecker DB, Grass G, Schneider PM, Thiele J, Dienes HP and
Hölscher AH: Expression of MMP-2 is associated with progression and
lymph node metastasis of gastric carcinoma. Histopathology.
39:597–602. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Hoikkala S, Pääkkö P, Soini Y, Mäkitaro R,
Kinnula V and Turpeenniemi-Hujanen T: Tissue MMP-2 and MMP-9
[corrected] are better prognostic factors than serum
MMP-2/TIMP-2-complex or TIMP-1 [corrected] in stage [corrected]
I–III lung carcinoma. Cancer Lett. 236:125–132. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Nascimento Dda C, Durigan Rde C, Tibana
RA, Durigan JL, Navalta JW and Prestes J: The response of matrix
metalloproteinase-9 and −2 to exercise. Sports Med. 45:269–278.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Niessner A, Richter B, Penka M, Steiner S,
Strasser B, Ziegler S, Heeb-Elze E, Zorn G, Leitner-Heinschink A,
Niessner C, et al: Endurance training reduces circulating
inflammatory markers in persons at risk of coronary events: Impact
on plaque stabilization? Atherosclerosis. 186:160–165. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Steenport M, Khan KM, Du B, Barnhard SE,
Dannenberg AJ and Falcone DJ: Matrix metalloproteinase (MMP)-1 and
MMP-3 induce macrophage MMP-9: Evidence for the role of TNF-alpha
and cyclooxygenase-2. J Immunol. 183:8119–8127. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Gleeson M, Bishop NC, Stensel DJ, Lindley
MR, Mastana SS and Nimmo MA: The anti-inflammatory effects of
exercise: Mechanisms and implications for the prevention and
treatment of disease. Nat Rev Immunol. 11:607–615. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Heinemeier KM, Olesen JL, Haddad F,
Langberg H, Kjaer M, Baldwin KM and Schjerling P: Expression of
collagen and related growth factors in rat tendon and skeletal
muscle in response to specific contraction types. J Physiol.
582:1303–1316. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Rullman E, Norrbom J, Strömberg A,
Wågsäter D, Rundqvist H, Haas T and Gustafsson T: Endurance
exercise activates matrix metalloproteinases in human skeletal
muscle. J Appl Physiol (1985). 106:804–812. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Roomi MW, Kalinovsky T, Rath M and
Niedzwiecki A: Down-regulation of urokinase plasminogen activator
and matrix metalloproteinases and up-regulation of their inhibitors
by a novel nutrient mixture in human prostate cancer cell lines
PC-3 and DU-145. Oncol Rep. 26:1407–1413. 2011.PubMed/NCBI
|
|
64
|
Booth NA, Walker E, Maughan R and Bennett
B: Plasminogen activator in normal subjects after exercise and
venous occlusion: t-PA circulates as complexes with C1-inhibitor
and PAI-1. Blood. 69:1600–1604. 1987.PubMed/NCBI
|
|
65
|
Small M, Simpson I, McGhie I, Douglas JT,
Lowe GD and Forbes CD: The effect of exercise on thrombin and
plasmin generation in middle-aged men. Haemostasis. 17:371–376.
1987.PubMed/NCBI
|
|
66
|
Francis RM, Romeyn CL, Coughlin AM,
Nagelkirk PR, Womack CJ and Lemmer JT: Age and aerobic training
status effects on plasma and skeletal muscle tPA and PAI-1. Eur J
Appl Physiol. 114:1229–1238. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Sumann G, Fries D, Griesmacher A,
Falkensammer G, Klingler A, Koller A, Streif W, Greie S,
Schobersberger B and Schobersberger W: Blood coagulation activation
and fibrinolysis during a downhill marathon run. Blood Coagul
Fibrinolysis. 18:435–440. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Baramova EN, Bajou K, Remacle A, L'Hoir C,
Krell HW, Weidle UH, Noel A and Foidart JM: Involvement of
PA/plasmin system in the processing of pro-MMP-9 and in the second
step of pro-MMP-2 activation. FEBS Lett. 405:157–162. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Ranuncolo SM, Armanasco E, Cresta C, Bal
De Kier Joffe E and Puricelli L: Plasma MMP-9 (92 kDa-MMP) activity
is useful in the follow-up and in the assessment of prognosis in
breast cancer patients. Int J Cancer. 106:745–751. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
La Rocca G, Pucci-Minafra I, Marrazzo A,
Taormina P and Minafra S: Zymographic detection and clinical
correlations of MMP-2 and MMP-9 in breast cancer sera. Br J Cancer.
90:1414–1421. 2004. View Article : Google Scholar : PubMed/NCBI
|