Introduction
Renal cell carcinoma (RCC) accounts for 2–3% of all
malignant tumors in adults and its incidence is increasing;
>39,000 new cases and 13,000 mortalities occurring annually in
the United States at present (1,2). Active
and passive cigarette smoking, obesity and hypertension are known
risk factors (1). In addition, RCC
appears to be more common in patients with end-stage renal failure,
acquired renal cystic disease or tuberous sclerosis, compared with
the general population (1).
Patients with RCC can present with local or systemic
symptoms; however, most presentations are incidental (1). Local signs and symptoms include
hematuria, flank pain or a palpable abdominal mass; while systemic
symptoms can be due to metastases or paraneoplastic events largely
related to secreted proteins, such as parathyroid hormone-related
protein (causing hypercalcaemia), renin (causing hypertension),
erythropoietin (causing erythrocytosis), and fever or wasting
syndromes (3). Patients suspected of
having a renal lesion should undergo complete physical examination
and laboratory studies including complete blood count, serum
chemistries, prothrombin time and partial thromboplastin time
(1). Imaging studies should include
computed tomography (CT) of the abdomen and pelvis with contrast,
chest radiography and chest CT (1).
Among all histological variants of RCC, the clear
cell type represents the most common, accounting for up to 80% of
cases (1,2). Localized RCC generally carries a good
prognosis, while extensive disease is essentially incurable; the
5-year survival rates are 91–100%, 74–96%, 59–70% and 16–32% for
stage I, II, III and IV disease, respectively (4). Typically, RCC has a strong tendency to
metastasize via the bloodstream. RCC usually metastasizes in the
lung, bones, lymph node and cerebrum (1–4).
Approximately 30–40% of patients exhibit metastatic disease at
initial presentation, and 20% present with locally advanced
disease, with the remainder having localized tumors (1,2). Around
one-third of all patients with apparently localized disease will
later develop metastasis, even a number of years after nephrectomy
(3,4).
The principal treatment for localized RCC is
surgical resection, including laparoscopic radical nephrectomy,
hand-assisted laparoscopic nephrectomy, or open or laparoscopic
partial nephrectomy (1). In the
presence of metastatic disease, a radical nephrectomy in addition
to metastasectomy may be considered (1). Compared with other cancers, chemotherapy
is rather ineffective for RCC; numerous agents have been tested,
with most showing response rates of <10% (5). Cytokine and targeted biological
therapies may represent an alternative approaches (1).
Although RCC is well-known for its propensity to
metastasize to unusual sites (6–13), the
occurrence of RCC metastasis to the head and neck region is
uncommon; this occurs primarily in the thyroid gland and in
patients with widespread dissemination (9–13). In
general, the involvement of the parathyroid gland in metastatic
tumors is a very rare event (14–28). In
the present study, a case of RCC metastasis to the parathyroid
gland is reported. To the best of our knowledge, only one case of
RCC metastasis to the parathyroid gland has been previously
reported (28); however, the present
case is the first report of intrathyroidal localization.
Case report
Patient
A 66-year-old Caucasian man was referred to the
Department of Surgery of the University Hospital of Pisa (Pisa,
Italy) in March 2013, with a preoperative fine-needle aspiration
diagnosis of a follicular lesion in the context of nodular goiter
of the thyroid gland. The previous medical history of the patient
included a right radical nephrectomy for the treatment of clear
cell RCC in February 1997. No other distant metastases were
observed during follow-up. Scintigraphic bone scan imaging was
negative for metastatic lesions. An abdominal ultrasonograpic
examination revealed a nephrectomy scar on the right side, but the
results were otherwise normal. Ultrasonographic examination of the
neck region revealed the presence of nodular goiter of the thyroid
gland with left predominance and slight deviation of the trachea
without constriction, confirmed by CT examination of the neck
region. Fine-needle aspiration was performed on two nodules of the
apical and basal portion of the left lobe of the thyroid gland,
measuring 40 and 33 mm, respectively. Cytological examination
classified the apical nodule as a follicular lesion and the basal
nodule as an unsatisfactory (non-diagnostic) smear, according to
the 2nd edition of the Guidelines for Thyroid Cancer Management
published by the British Thyroid Association (29). The patient underwent total
thyroidectomy in March 2013. Laboratory findings on admission were
as follows: Hemoglobin, 16.1 g/dl (normal range, 13.8–17.2 g/dl);
hematocrit, 45.6% (normal range, 41–50%); erythrocyte count,
5,270,000/mm3 (normal range,
4,400,000–5,800,000/mm3); leukocyte count,
9,580/mm3 (normal range, 3,800–10,800/mm3);
platelet count, 269,000/mm3 (normal range,
130,000–400,000/mm3); creatinine, 1.19 mg/dl (normal
range, ≤1.2 mg/dl); and calcium 9.8 mg/dl (normal range, 8.5–10.3
mg/dl). Urine analysis was normal. Thyroid and parathyroid function
tests were normal. Institutional approval from the ethics committee
was obtained for the present study. Informed consent was obtained
from the patient with regard to the use of the tumor samples.
Specimens
Specimens were surgically obtained via total
thyroidectomy. The thyroid weighed 35 g (normal range, 20–30 g) and
measured 73×65×40 mm. Thyroid tissue was fixed in 10%
neutral-buffered formalin and then dissected. A total of 13 samples
(~20×20 mm) of all nodules and collateral parenchyma were collected
and embedded in paraffin. Following slicing with a microtome,
routine hematoxylin and eosin staining was performed on the section
prior to histopathological examination according to standard
protocols (30).
Immunohistochemistry
A paraffin block for immunohistochemical study was
selected. Immunohistochemistry was performed using the
avidin-biotin-peroxidase complex method according to the
manufacturer's protocol (31). Tissue
sections (5 µm thick) were deparaffinized in xylene and rehydrated
in a graded ethanol series. Immunohistochemical analyses were
performed automatically using the Ventana Benchmark immunostaining
system (Ventana Medical Systems, Inc., Tucson, AZ, USA) with
primary antibodies (all obtained from Ventana Medical Systems,
Inc.) against the following: Thyroid transcription factor-1 (clone
SP141; #790-4756; rabbit monoclonal; 5.7 µg/ml), thyroglobulin
(clone 2H11+6E1; #760-2671; mouse monoclonal; 0.22 µg/ml), cluster
of differentiation (CD)10 (clone SP67; #790-4506; rabbit
monoclonal; 4.9 µg/ml), epithelial membrane antigen (EMA; clone
E29; #790-4463; mouse monoclonal; 0.54 µg/ml), vimentin (clone V9;
#790-2917; mouse monoclonal; 2.5 µg/ml), chromogranin A (clone
LK2H10; #760-2519; mouse monoclonal; 1 µg/ml), parathyroid hormone
(clone MRQ-31; #760-4532; mouse monoclonal; 0.08 µg/ml) and
calcitonin (clone SP17; #760-4705; rabbit monoclonal; 0.56 µg/ml).
All antibodies were pre-diluted as above. Universal UltraView
3,3′-diaminobenzidine chromogen detection system method (#760-091;
Ventana Medical Systems, Inc.) was utilized as a chromogen, and
commercial hematoxylin was used for counterstaining, according to
the manufacturer's protocol.
Results
Specimens were obtained from a 66-year-old man who
underwent thyroidectomy following examination and evaluation. The
gross appearance of the surgical specimen was a multinodular goiter
with two nodules of solid consistency in the left lobe measuring 33
and 40 mm, respectively; notably, the nodule measuring 33 mm
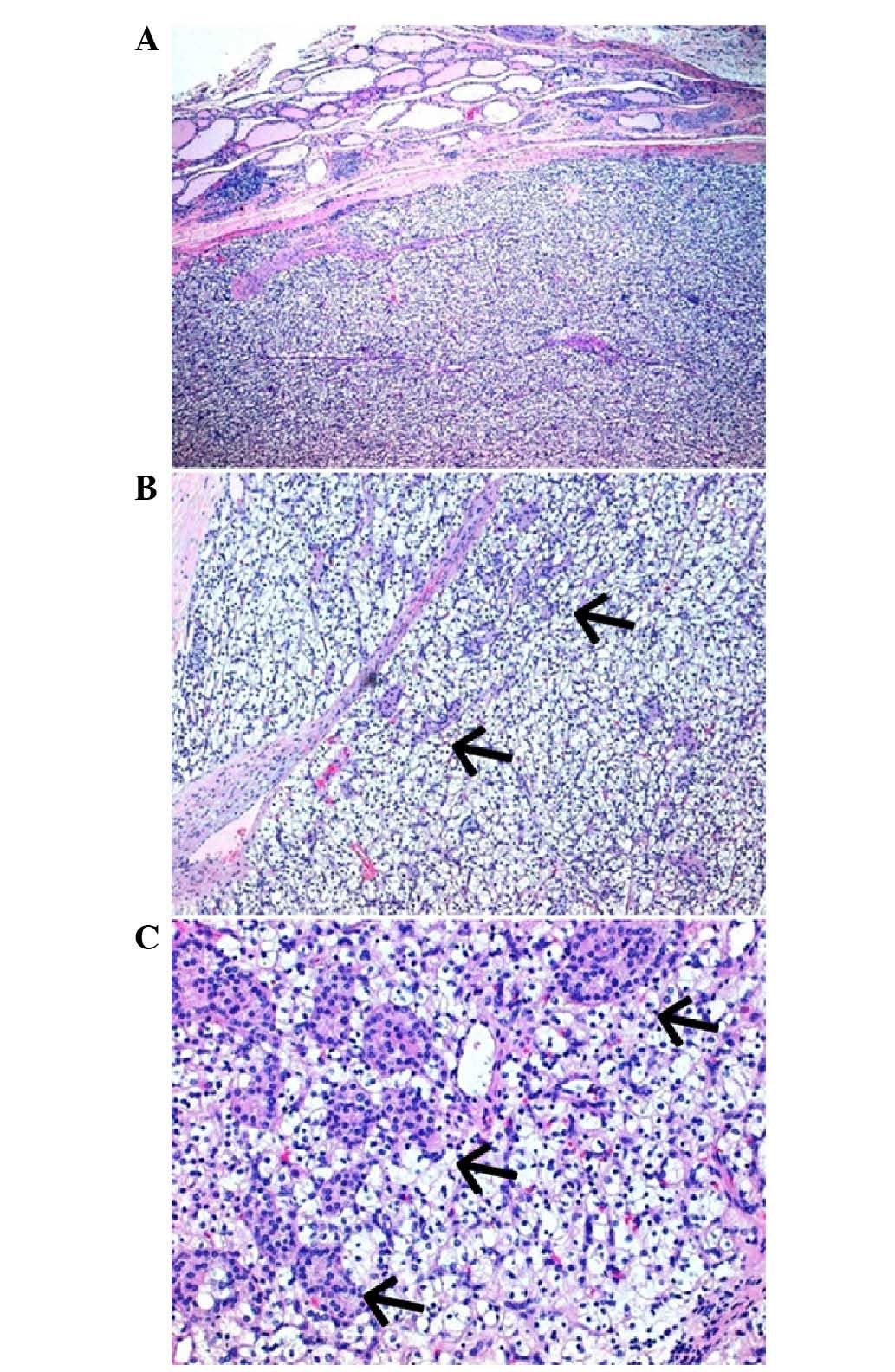
exhibited a bright yellow color. Microscopic examination (Leica
Microscope DM400B; Leica Microsystems, Wetzlar, Germany; ×4, ×10,
×20 and ×40 magnifications) revealed a multinodular goiter with
abundant colloid on the right lobe of the thyroid gland, associated
with two small foci of the classic variant of papillary thyroid
carcinoma, sized 1 and 4 mm, respectively. On the left lobe, the
nodule measuring 40 mm was an adenomatous nodule with a prevalent
microfollicular pattern of growth, while the nodule measuring 33 mm
was a completely encapsulated lesion consisting of cells with
abundant clear cytoplasm arranged in a solid pattern of growth,
with a prominent sinusoidal vascular network. In the context of
this lesion, there was intermingling of the clear cells with
scattered small solid nests of cells with differing morphology
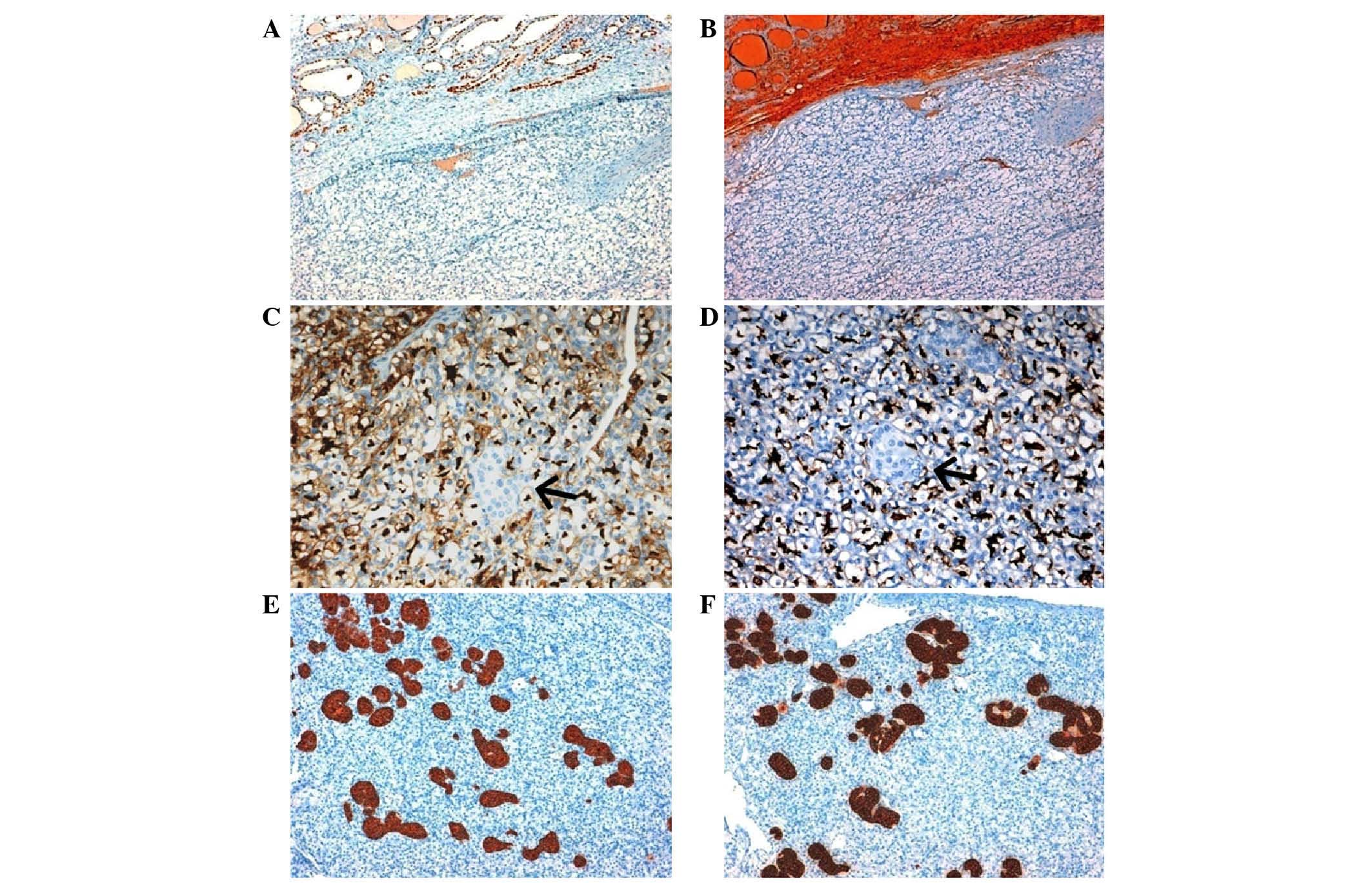
(abundant deeply granular and eosinophilic cytoplasm; Fig. 1). Immunohistochemical analyses
revealed that the neoplastic population with clear cell morphology
was completely negative for thyroid transcription factor-1,
thyroglobulin, chromogranin A, calcitonin and parathyroid hormone,
and strongly positive for CD10, EMA and vimentin (Fig. 2). Notably, the small nests of cells
intermixed with clear cells were strongly positive for chromogranin
A and parathyroid hormone and negative for all other antibodies
(Fig. 2). Taken together, the
morphological and immunohistochemical data suggested a definitive
histological diagnosis of metastatic clear cell RCC to the
parathyroid gland, likely with intrathyroidal localization.
Discussion
In the present study, a rare case of nodular goiter
of the thyroid gland concurrent with metastatic RCC involving an
intrathyroidal parathyroid gland, without disseminated systemic
metastasis and without clinical signs of parathyroid disease, was
reported. Typically, RCC exhibits a high metastatic potential, and
most commonly metastasizes via the bloodstream, although lymphatic
metastasis also occurs (1,2). In order of frequency, RCC more commonly
metastasizes to the lung, bone, liver, brain and skin (1,2). RCC is
well-known for its propensity to metastasize to unusual sites, even
a number of years after nephrectomy (6–13).
Metastases from RCC to the head and neck region are very rare
(9–13), with the thyroid gland accounting for a
large percentage of cases (32–34).
Several studies have indicated that thyroid glands
affected by various pathologies (nodular goiter, thyroiditis,
benign and malignant neoplasms) are more likely to harbor
metastatic disease compared with normal glands, most likely due to
an abnormal blood supply leading to decreased oxygen and iodine
content (32–34). The actual incidence of parathyroid
gland involvement in neoplastic patients with widespread metastases
largely remains to be elucidated (21). Even in cases of diffuse systemic
dissemination of neoplastic disease, the observation of parathyroid
involvement is very rare, perhaps because parathyroid gland are
seldom evaluated at autopsy (21).
In a previous study, the incidence of parathyroid
gland involvement with metastatic tumors has been between 0.2 and
11.9% among patients with a known history of cancer (21). In autopsy studies, the metastatic
involvement of parathyroid gland has typically been observed in
patients with systemic dissemination (18,21).
Furthermore, as parathyroid involvement occurred in patients with
extensive metastases in other organs, it has been suggested that
this event may represent a symptom of late-stage cancers (18). In clinical series, the metastatic
involvement of the parathyroid gland occurred more commonly as a
solitary lesion without systemic dissemination (24–27). The
previously reported cases of metastatic carcinoma affecting the
parathyroid gland originated from the breast, lung, skin (malignant
melanoma), liver and hemolymphatic system (chronic lymphocytic
leukemia) (14–27).
The metastatic involvement of the parathyroid gland
may be associated with altered parathyroid function, including
hypoparathyroidism (17,19) and hyperparathyroidism (24–27). In
certain circumstances, metastasis to the parathyroid gland has been
proposed as an alternative mechanism of ‘malignant hypercalcemia’,
occurring in a peculiar subgroup of patients with widespread
metastatic malignant neoplasm (22).
By contrast, the occurrence of hypoparathyroidism and hypocalcemia
in metastatic cancers affecting the parathyroid gland as result of
parathyroid destruction by the tumor is rarely observed (17,19). The
occurrence of metastasis in parathyroid glands affected by other
pathologies, primarily adenoma and hyperplasia, may be justified by
the abnormal blood supply as compared with normal parathyroid
tissue (15,16,20,25,26).
Secondary involvement of the parathyroid gland may be the
consequence not only of distant metastasis but also of direct
extension, more commonly by thyroid and laryngeal carcinomas
(32,35,36).
Involvement of the parathyroid gland with papillary thyroid
carcinoma has been observed in 20/911 cases, primarily due to
direct extension, however, 2% were due to metastasis (36).
In the present case, the patient underwent total
thyroidectomy, due to a preoperative diagnosis of a follicular
lesion in the context of nodular goiter of the thyroid gland.
Histopathological examination highlighted the presence of an
encapsulated clear cell lesion in the context of nodular goiter,
associated with the presence of small foci of papillary thyroid
microcarcinoma. Initially, the differential diagnosis between a
thyroid lesion with clear cell morphology and a metastatic
localization was taken into consideration. Data from the initial
immunohistochemical tests uncovered the metastatic nature of the
lesion, supported by the absence of immunoreactivity for thyroid
transcription factor-1 and thyroglobulin and the presence of
immunoreactivity for CD10, EMA and vimentin. Notably, additional
immunohistochemical analyses revealed the atypical immunoprofile of
the scattered solid nests, which were strongly positive for
chromogranin A and parathyroid hormone.
To the best of our knowledge, this is the second
case reported in the literature of solitary metastasis confined to
the parathyroid gland from clear cell RCC, which occurred 16 years
after nephrectomy in a patient with no clinical signs of
parathyroid disease.
References
|
1
|
Nelson EV, Evans CP and Lara PN Jr: Renal
cell carcinoma: Current status and emerging therapies. Cancer Treat
Rev. 33:299–313. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Novick AC: Kidney cancer: Past, present,
and future. Urol Oncol. 25:188–195. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gupta K, Miller JD, Li JZ, Russell MW and
Charbonneau C: Epidemiologic and socioeconomic burden of metastatic
renal cell carcinoma (mRCC): A literature review. Cancer Treat Rev.
34:193–205. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pantuck AJ, Zisman A and Belldegrun AS:
The changing natural history of renal cell carcinoma. J Urol.
166:1611–1623. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lilleby W and Fosså SD: Chemotherapy in
metastatic renal cell cancer. World J Urol. 23:175–179. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sountoulides P, Metaxa L and Cindolo L:
Atypical presentations and rare metastatic sites of renal cell
carcinoma: A review of case reports. J Med Case Rep. 5:4292011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Papachristodoulou A, Mantas D, Kouskos E,
Hatzianastassiou D and Karatzas G: Unusual presentation of renal
cell carcinoma metastasis. Acta Chir Belg. 104:229–230. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
King DH, Centeno AS, Saldivar VA and
Sarosdy MF: Renal cell carcinoma metastatic to the gallbladder or
prostate: Two case reports. Urology. 46:722–725. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Langille G, Taylor SM and Bullock MJ:
Metastatic renal cell carcinoma to the head and neck: Summary of 21
cases. J Otolaryngol Head Neck Surg. 37:515–521. 2008.PubMed/NCBI
|
|
10
|
Marioni G, Gaio E, Poletti A, Derosas F
and Staffieri A: Uncommon metastatic site of renal adenocarcinoma:
The oral tongue. Acta Otolaryngol. 124:197–201. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gil-Julio H, Vázquez-Alonso F,
Fernández-Sánchez AJ, Puche-Sanz I, Flores-Martín JF and Cózar JM:
Metastasis of renal cell carcinoma to the buccal mucosa 19 years
after radical nephrectomy. Case Rep Oncol Med.
2012:8230422012.PubMed/NCBI
|
|
12
|
Ray A, Bhattacharya J and Ganguly S: Renal
cell carcinoma presenting with oral tongue metastasis: A rare case
presentation. J Cancer Res Ther. 9:117–118. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ozkiriş M, Kubilay U and Sezen OS:
Cervical lymph node metastasis in renal cell carcinoma. J Oral
Maxillofac Pathol. 15:211–213. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
DeLellis RA: Miscellaneous lesionsAtlas of
Tumor Pathology. Tumors of the parathyroid gland. 3rd. Armed Forces
Institute of Pathology; Washington, DC: pp. 93–94. 1993
|
|
15
|
Woolner LB, Keating FR Jr and Black BM:
Primary hyperparathyroidism and metastatic breast carcinoma: A case
in which breast carcinoma metastasized to a parathyroid adenoma.
Cancer. 11:975–979. 1958. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Margolis CI and Goldenberg VE: Breast
carcinoma metastatic to parathyroid adenoma. NY State J Med.
69:702–703. 1969.
|
|
17
|
Horwitz CA, Myers WP and Foote FW Jr:
Secondary malignant tumors of the parathyroid glands. Report of two
cases with associated hypoparathyroidism. Am J Med. 52:797–808.
1972. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cifuentes N and Pickren JW: Metastases
from carcinoma of mammary gland: An autopsy study. J Surg Oncol.
11:193–205. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
de la Monte SM, Hutchins GM and Moore GW:
Endocrine organ metastases from breast carcinoma. Am J Pathol.
114:131–136. 1984.PubMed/NCBI
|
|
20
|
Inoshita T and Laurain AR: Tumor-to-tumor
metastasis: Malignant melanoma metastatic to parathyroid adenoma.
Mil Med. 150:323–325. 1985.PubMed/NCBI
|
|
21
|
Gattuso P, Khan NA, Jablokow VR and
Kathuria S: Neoplasms metastatic to parathyroid glands. South Med
J. 81:14671988. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Benisovich VI, Rybak BJ and Ross FA: A
case of adenocarcinoma of the lung associated with a neck mass and
hypercalcemia. Cancer. 68:1106–1108. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bumpers HL, Hassett JM Jr, Penetrante RB,
Hoover EL and Holyoke ED: Endocrine organ metastases in subjects
with lobular carcinoma of the breast. Arch Surg. 128:1344–1347.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Venkatraman L, Kalangutkar A and Russell
CF: Primary hyperparathyroidism and metastatic carcinoma within
parathyroid gland. J Clin Pathol. 60:1058–1060. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee HE, Kim DH, Cho YH, Kim K, Chae SW and
Sohn JH: Tumor-to-tumor metastasis: Hepatocellular carcinoma
metastatic to parathyroid adenoma. Pathol Int. 61:593–597. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fulciniti F, Pezzullo L, Chiofalo MG,
Butera D, Losito NS, Tommaselli AP and Botti G: Metastatic breast
carcinoma to parathyroid adenoma on fine needle cytology sample:
Report of a case. Diagn Cytopathol. 39:681–685. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lee SH, Kim BH, Bae MJ, Yi YS, Kim WJ,
Jeon YK, Kim SS, Kim YK and Kim IJ: Concurrence of primary
hyperparathyroidism and metastatic breast carcinoma affected a
parathyroid gland. J Clin Endocrinol Metab. 98:3127–3130. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ofo E, Mandavia R, Jeannon JP, Odell E and
Simo R: Renal cell carcinoma metastasis to the parathyroid gland: A
very rare occurrence. Int J Surg Case Rep. 5:378–380. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
British Thyroid Association; Royal College
of Physicians of London, . Fine needle aspiration
cytologyGuidelines for the Management of Thyroid Cancer. Perros P:
2nd. Lavenham Press; Lavenham, Suffolk: pp. 9–10. 2007
|
|
30
|
Thompson SW: Selected histochemical and
histopathological methods. 1st. C. C. Thomas; Springfield, IL: pp.
24–160. 1966
|
|
31
|
Elias JM, Gown AM, Nakamura RM, Wilbur DC,
Herman GE, Jaffe ES, Battifora H and Brigati DJ: Quality control in
immunohistochemistry. Report of a workshop sponsored by the
Biological Stain Commission. Am J Clin Pathol. 92:836–843. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Chung AY, Tran TB, Brumund KT, Weisman RA
and Bouvet M: Metastases to the thyroid: A review of the literature
from the last decade. Thyroid. 22:258–268. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kobayashi K, Hirokawa M, Yabuta T,
Fukushima M, Masuoka H, Higashiyama T, Kihara M, Ito Y, Miya A,
Amino N and Miyauchi A: Metastatic carcinoma to the thyroid gland
from renal cell carcinoma: Role of ultrasonography in preoperative
diagnosis. Thyroid Res. 17:42015. View Article : Google Scholar
|
|
34
|
Heffess CS, Wenig BM and Thompson LD:
Metastatic renal cell carcinoma to the thyroid gland: A
clinicopathologic study of 36 cases. Cancer. 95:1869–1878. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tang W, Kakudo K, Nakamura MDY, Nakamura
M, Mori I, Morita S and Miyauchi A: Parathyroid gland involvement
by papillary carcinoma of the thyroid gland. Arch Pathol Lab Med.
126:1511–1514. 2002.PubMed/NCBI
|
|
36
|
Ito Y, Kakudo K, Hirokawa M, Fukushima M,
Tomoda C, Inoue H, Kihara M, Higashiyama T, Uruno T, Takamura Y, et
al: Clinical significance of extrathyroid extension to the
parathyroid gland of papillary thyroid carcinoma. Endocr J.
56:251–255. 2009. View Article : Google Scholar : PubMed/NCBI
|