Introduction
The scalp is the most frequent site of occurrence of
malignant tumors (1). The incidence
of malignant peripheral nerve sheath tumors (MPNST), which is equal
in males and females, is <0.001% (2). MPNST typically presents between the ages
of 20 and 50 years, and usually starts as a small tumor that grows
in size. In the early course of MPNST, there are no pain symptoms;
however, if the tumor continues to grow, the patient shows symptoms
of oppression of the brain. Pain initially appears in the
nerve-dominated areas associated with malignant transformation and
erosion of the nerves and surrounding tissues by the tumor mass. In
addition, patients with MPNST experience neurological dysfunction,
including feeling numb and presenting with decreased muscle
strength, muscle weakness and paralysis. MPNST may be diagnosed by
ultrasound, magnetic resonance imaging (MRI), positron emission
tomography-computed tomography (CT), CT, bone scans, fine needle
aspiration biopsies and pathological analyses (3). Therapeutic strategies include surgery,
radiotherapy and chemotherapy. The 5- and 10-year survival rates of
patients with MPNST are 34–52% and 23–34%, respectively. The local
recurrence rate is 40–65% and the distant metastasis rate is 40–68%
(4).
Adult-type fibrosarcoma (AFS) represents 1–3% of
total sarcoma cases in the world, and has an average disease course
of ~3.5 years (5). AFS is more common
in males than in females, and usually presents between the ages of
30 and 55 years (5,6). AFS typically develops slowly from highly
vascularized, painless tumors that have clear-borders and are small
in size, with localized ulcers and hemorrhaging (7). A typical AFS tumor has V-shaped bundle
formation and a herringbone pattern under a microscope (8). Comparative genomic hybridization has
demonstrated that chromosome 12q is frequently amplified in
patients with AFS (9). Surgical
intervention followed by chemoradiotherapy remains the first-line
treatment option for patients with AFS, who have a 5-year survival
rate of 39–54.4% (10).
Malignant proliferating trichilemmal tumor (MPTT)
usually presents between the ages of 60 and 70 years, and 80% of
all patients are female (11). MPTTs
grow slowly and have a long disease duration; they become malignant
when the cell growth rate increases, at which point the tumor
surface ulcerates, bleeds and exhibits necrosis. The tumor usually
has a diameter of <2 cm (12). An
accurate diagnosis of MPTT relies on a pathological examination,
and therapeutic strategies include surgery, radiotherapy,
chemotherapy and cryotherapy (13–17).
Insufficient monitoring by patients or physicians
during physical examinations facilitates the development of
malignant tumors in the scalp. The present study reports 3 cases of
different types of rare giant malignant tumors of the scalp: A
peripheral nerve sheath tumor, a fibrous tumor and an MPTT. These
types of tumor are rarely observed (2,18,19), particularly in the scalp. Information
regarding the surgical treatments performed for each case is
provided, and written informed consent was obtained from all
patients.
Case report
Case 1
A 52-year-old man presented at The First Bethune
Hospital of Jilin University (Changchun, China) in December 2009
with a 5-year history of scalp tumors in the right forehead. The
tumors were originally small and had been growing slowly. The
tumors had previously been removed in August 2009 at a local
hospital and diagnosed as solitary fibrous tumors of the nervous
system. The tumors recurred and grew rapidly giving rise to an
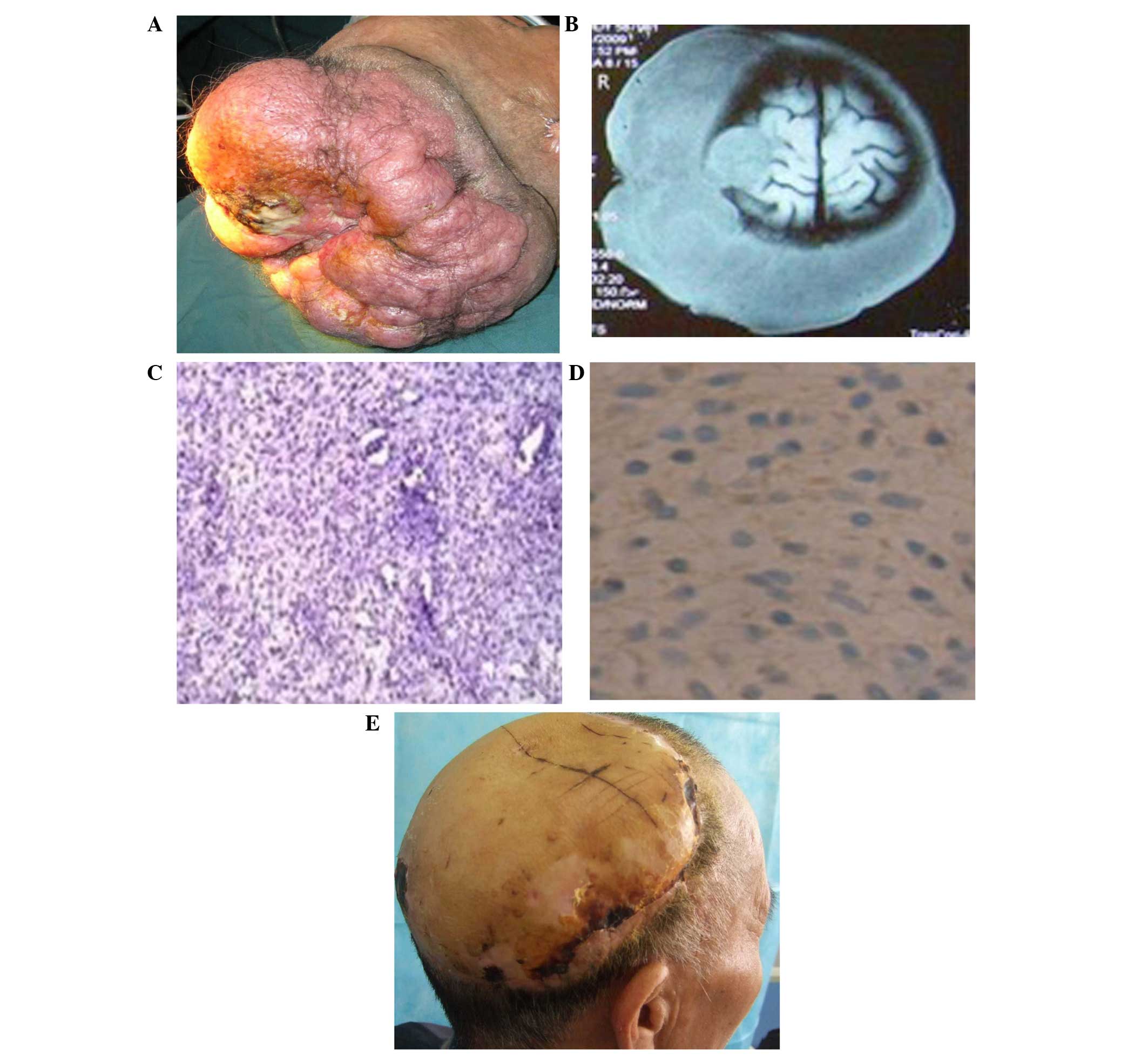
ulcer. Physical examination revealed no nerve damage. The tumors
had unequal coffee spots with clear boundaries and diffused unequal
oval nodules. Nodular red-brown tumors, 28×25×10 cm in size, were
found in the right forehead and temporal and occipital bones.
Tumors were characterized by a clear boundary and medium solidity,
but lacked compression pain, sense of volatility and vessel noise
(Fig. 1A). MRI scans indicated
extensive growth of spots or lichen-like tumors outside of the
right frontal, temporal and occipital bones. In addition, the
hat-like aponeurosis was independent and separated from the skull
plate (Fig. 1B). The lesion in the
right forehead invaded the intracranial region compressing the
associated brain tissue and destroying the skull bone tissue.
Clinical examination of the solitary fibrous tumor of the nervous
system in the right forehead indicated malignant transformation.
During the surgery, the tumors and lesion areas of the skull were
completely removed, after which the local skull deficiency was
repaired using a titanium plate and a microvascular anastomotic
anterolateral thigh flap was transplanted to cover the large scalp
defect.
A post-operative pathological examination showed
that the cellular morphology of the tumors was non-uniform. Tumor
cells exhibited a fusiform morphology with an oval nucleus.
Fusiform tumor cells were mitotic and exhibited uniform arrangement
in bundles [Fig. 1C; hematoxylin and
eosin (HE) staining]. Immunochemistry showed positive staining for
S-100 [Fig. 1D; anti-S-100 monoclonal
antibody (mAb); cat. no. 16/f5; Fuzhou Maixin Biotech., Co., Ltd.,
Fuzhou, China] and cluster of differentiation (CD)34 (anti-CD34
mAb; cat. no. QBEnd/10; Fuzhou Maixin Biotech.), and negative
staining for CD68 (anti-CD68 mAb; cat. no. KP1; Fuzhou Maixin
Biotech.) and desmin (anti-desmin mAb; cat. no. D33; Fuzhou Maixin
Biotech.). The tumors were classified as grade 2 with a score of 4
based on the French Federation of Cancer Centers Sarcoma Group
grading system (20). The diagnosis
was of a malignant peripheral nerve sheath tumors. The patient was
hospitalized for 18 days without chemotherapy and the transplanted
flap survived (Fig. 1E). No
recurrence was observed in the 5-year follow-up.
Case 2
A 35-year-old man presented at The First Bethune
Hospital of Jilin University in January 2012 with a 3-year history
of a scalp tumor on the top of the head. The patient had previously
been admitted to The Central Hospital of Changchun, China in
November 2011, where the tumor had been identified. The tumor was
excised and diagnosed as a solitary fibrous tumor in February 2012.
The tumor recurred in May 2012. There was no head trauma or history
of radioactive disease. A neuronal evaluation performed did not
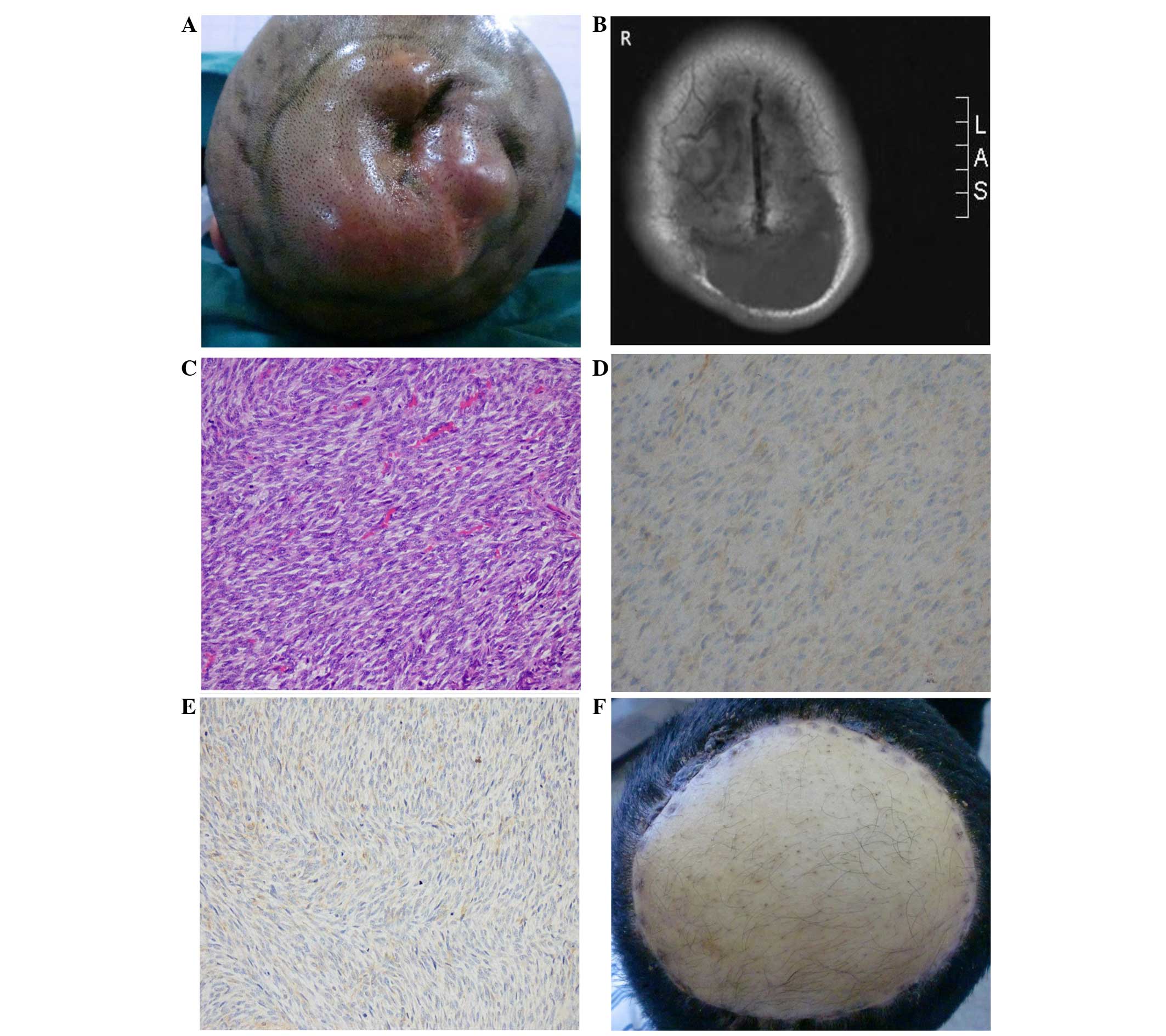
reveal any abnormalities. A tough tumor (28×25×10 cm) with a clear
boundary was identified on the top of the occipital lobe (Fig. 2A). The tumor was non-movable. MRI
revealed that the tumor had an irregular surface, as shown by
gadolinium-diethylenetriamine penta-acetic acid images, and that it
was hypointense on T1-weighted imaging (Fig. 2B). Clinical diagnosis identified the
recurrence of the fibrous tumor in the scalp. The scalp tumor and
lesions were surgically removed, and local deficiencies and
large-scale defects were repaired using titanium plates and a
microvascular anastomotic anterolateral thigh flap. Tumor cells
were found to be fusiform with oval nuclei. Fusiform tumor cells
were mitotic and exhibited a uniform arrangement in bundles
(Fig. 2C; HE staining).
Immunochemistry identified the positive expression of CD99
(Fig. 2D; anti-CD99 mAb; cat. no.
O13; Fuzhou Maixin Biotech.), vimentin (Fig. 2E; anti-vimentin mAb; cat. no. V9;
Fuzhou Maixin Biotech.) and cytokeratin (anti-cytokeratin mAb; cat.
no. AE1/AE3; Fuzhou Maixin Biotech.). No expression was noted for
S-100, CD34, desmin, smooth muscle actin (anti-SMA mAb; cat. no.
1A4; Fuzhou Maixin Biotech.), epithelial membrane antigen (anti-EMA
mAb; cat. no. E29; Fuzhou Maixin Biotech.), B-cell lymphoma 2
(anti-Bcl-2 mAb; cat. no. SP66; Fuzhou Maixin Biotech.) and
calponin (anti-calponin mAb; cat. no. SP13; Fuzhou Maixin
Biotech.). Correspondingly, the tumor was diagnosed as an AFS with
moderate differentiation. The patient remained hospitalized for 18
days, but did not receive chemotherapy. The transplanted flap
survived (Fig. 2F) and no recurrence
was observed in the 3-year follow-up.
Case 3
A 42-year-old man presented at The First Bethune
Hospital of Jilin University in November 2012 with an 11-year
history of scalp tumors on the top of the occipital lobe. The
patient had been hospitalized earlier in the month and the tumors
had been surgically removed. The post-operative pathological
findings were inconclusive. The tumors recurred 1 month later, and
grew rapidly and became ulcerated. No nerve damage was detected and
the tumors were diagnosed as solitary fibrous tumors. The tumors
had recurred in the same location as previously. There was no head
trauma or radioactive disease history, and no nerve damage was
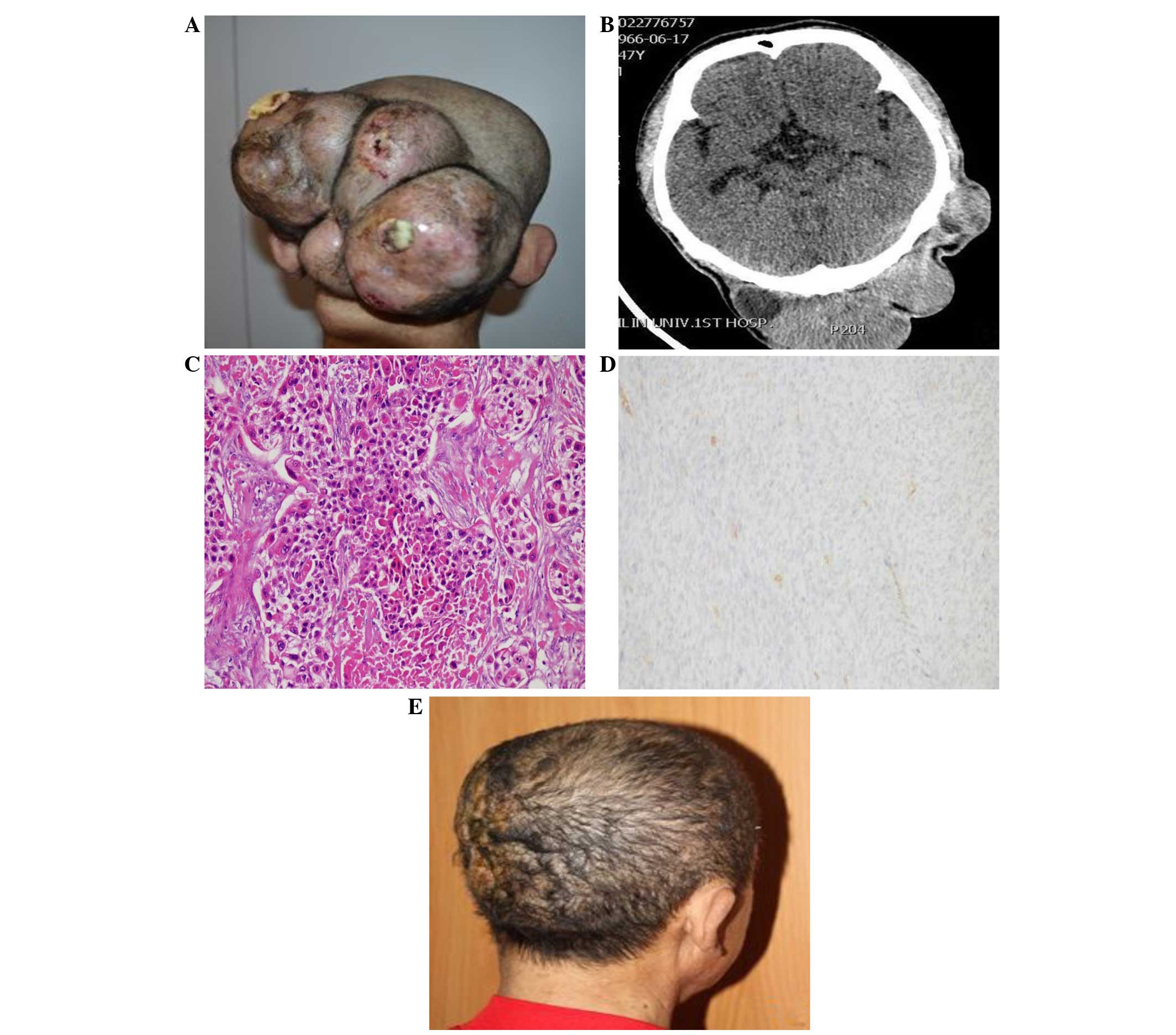
observed. The tumors (22×17×19 cm) were located in the top
occipital region and had a clear boundary (Fig. 3A). A head computed tomography scan
revealed sheet-like, irregular giant malignant tumors (Fig. 3B) and suggested the diagnosis of
solitary fibrous tumors of the nervous system. Five tumors were
surgically excised and local skull deficiencies were repaired using
titanium plates and local skin flaps. Post-operative pathological
examination revealed regions of basal cells surrounding the tumors
in a palisade arrangement. A keratosis sheath of the outer hair
root, and cell atypia and mitosis were observed (Fig. 3C; HE staining). The tumor cells
stained positively for CD34 (Fig.
3D). The tumor was diagnosed as an MPTT. The patient was
hospitalized for 25 days and the transplanted flap survived
(Fig. 3E). No recurrence was observed
in the 28-month follow-up.
Discussion
MPNST are rare nerve malignancies that exhibit an
incidence of <0.001% (2). These
tumors occur in the peripheral, cranial and sympathetic nerves and
account for 3–10% of soft-tissue tumors. The tumors occur mainly in
the buttocks, thighs and paraspinal region, but rarely on the top
of the head (21). It has recently
been reported that 2–29% of solitary fibrous tumors of the nervous
system will transform into MPNSTs (22). Malignancy is marked by rapid cell
growth and an increase in tumor volume, with symptoms of unbearable
pain, a tough tumor surface, nerve function loss and sphincter
disorders (22). Surgical resection
is an available therapeutic option; however, tumors with a tight
correlation to a cranial nerve are difficult to resect (23) and have a less favorable prognosis
(24,25). The prognosis of MPNST is associated
with the tumor's size, location, biological behaviour and history
of radiation exposure (26). MPNST
can metastasize to the adjacent tissues or distant organs,
including the lungs and bones; therefore, the 5-year survival rate
is <20%, and 50% of patients experience recurrence (27).
There are two types of fibrosarcoma, adult and
infantile, both of which are rare. AFS accounts for 1–3% of adult
soft-tissue sarcomas, with the peak incidence between the ages of
30 and 55 years in male patients. This type of tumor, which is
mostly localized in the limbs and the torso, and rarely in the head
or face, has a high recurrence rate (18,28). Risk
factors include oxidative stress, pollution, chemical reactions and
high-calorie diets (29–31). The early phase of the disease is
characterized by painless nodules that gradually increase in size
and become visible on the surface of the skin with a medium
solidity (32). In the late phases,
the tumor grows fast, giving rise to pain and partial ulceration.
If the tumor is not removed it will become malignant. Histological
indicators of poor prognosis include tumor grade, density of cell
growth, low levels of collagen, necrosis and a mitotic index
>20. Fibrosarcoma in the head and neck should be distinguished
from spindle cell tumors that occur in different tissues such as
the thyroid, salivary glands and lymph nodes (32). The 5-year survival rate for AFS is
39–54.4%, which is closely associated with the prognosis and
histological grade of the tumor. In essence, low-level tumor grades
have a 5-year survival rate of 58%, while high-level tumor grades
have a 5-year survival rate of 21–34%. The occurrence rate of blood
metastasis is ≤17.8% in the case of fibrosarcoma with a lymphatic
metastasis rate of 2% (33).
MPTT is a rare type of malignant tumor that
originates from the outer root sheath of a hair follicle. It is
mainly observed in the scalp and face of 60- to 70-year-old female
patients (19,34). The majority of these tumors display
isolated characteristics. Tumors grow slowly and have a long
disease duration; they become malignant when the cell growth rate
increases, at which point the tumor surface ulcerates, bleeds and
exhibits necrosis (35). An accurate
diagnosis relies on the pathological examination. The differential
diagnosis of MPTT includes skin squamous cell carcinoma, outer root
sheath cancer, metastatic renal cell carcinoma and clear cell
carcinoma of the sweat glands (12,36). MPTTs
can ulcerate and display symptoms similar to those of squamous cell
carcinoma (12). MPTTs transform into
multiple tumors and invade the cranial cavity. In certain cases,
these tumors may transfer to the ipsilateral lymph nodes and, at
the later phases, systemic metastases may occur.
The best treatment for giant malignant tumors of the
scalp is surgical resection; therefore, a complete resection is
critical. Chemotherapy following resection does not appear to have
an added benefit for disease-free recovery. In the present study, 3
rare cases of giant malignant tumors with similar surgical
requirements were discussed. The treatment plan includes a careful
and specific diagnosis, maintenance of the blood supply during
surgery and the reduction of intraoperative bleeding, maintenance
of hemodynamic stability during surgery using controlled
hypotension and artificial hypothermia anesthesia, and surgical
resection, which should remove the tumor with a 3-cm margin. If the
tumor invades the skull, the tumor base should be resected. During
the operation, the method of incision, hemostasis and edge
separation should be applied. The resection should start from the
lower galeal and snake in the direction of the normal scalp.
Isolating tumor depth surface is not recommended, as it can lead to
uncontrollable bleeding.
The repair of large areas of scalp deficiency is a
post-operative challenge. Clinical methods such as use of localized
flaps, scalp expansion, free skin, pedicle (free) flaps or muscle
flap repair are recommended to promote recovery. In our opinion the
anterolateral thigh flap has certain advantages, such as not
sacrificing the main vessel to provide a sufficiently large flap,
the consistent anatomical location of the blood vessels that supply
blood for the flap, and a large enough blood vessel and vascular
pedicle.
In the present study, vascularized free
anterolateral thigh flap surgery was applied in 2 cases of scalp
giant malignant tumors. The third case employed a local flap to
repair a large defect of the scalp. Post-operatively, the skin
grafts survived and pathological examination did not identify any
tumor cells. Chemotherapy was not administered in any of the 3
cases and no recurrence was observed at the 5-year, 3-year and
28-month follow-ups, respectively. The patients remain under
periodical follow-up to monitor their health status.
References
|
1
|
Richmond HM, Duvic M and Macfarlane DF:
Primary and metastatic malignant tumors of the scalp: An update. Am
J Clin Dermatol. 11:233–246. 2010.PubMed/NCBI
|
|
2
|
Hajdu SI: Peripheral nerve sheath tumors.
Histogenesis, classification, and prognosis. Cancer. 72:3549–3552.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jia X and Yang J: Progress of malignant
peripheral nerve sheath tumors study. Int J Orthop. 35:164–166.
2014.
|
|
4
|
Gousias K, Boström J, Kovacs A, Niehusmann
P, Wagner I and Kristof R: Factors of influence upon overall
survival in the treatment of intracranial MPNSTs: Review of the
literature and report of a case. Radiat Oncol. 5:1142010.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fletcher CDM, Unni KK and Mertens F: World
Health Organization Classification of TumoursPathology and Genetics
of Tumours of Soft Tissue and Bone. IARC Press; Lyon: 2002
|
|
6
|
Fisher C: The value of electronmicroscopy
and immunohistochemistry in the diagnosis of soft tissue sarcomas:
A study of 200 cases. Histopathology. 16:4411990. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Weiss SW and Goldblum JR:
FibrosarcomaEnzinger and Weiss's Soft Tissue Tumors. 4th. Mosby;
St. Louis, MO: pp. 409–418. 2001
|
|
8
|
Stout AP: Fibrosarcoma. The malignant
tumor of fibroblasts. Cancer. 1:30–63. 1948. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schmidt H, Taubert H, Würl P, Kappler M,
Lange H, Bartel F, Bache M, Holzhausen HJ and Hinze R: Gains of 12q
are the most frequent genomic imbalances in adult fibrosarcoma and
are correlated with a poor outcome. Genes Chromosomes Cancer.
34:69–77. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pritchard DJ, Soule EH, Taylor WF and
Ivins JC: Fibrosarcoma - a clinicopathologic and statistical study
of 199 tumors of the soft tissues of the extremities and trunk.
Cancer. 33:888–897. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sethi S and Singh UR: Proliferating
trichilemmal cyst: Report of two cases, one benign and the other
malignant. J Dermatol. 29:214–220. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cao YT, Wang XY, Xuan M and Gao QH: Facial
multiple malignant proliferating tricholemmoma: A case report. Hua
Xi Kou Qiang Yi Xue Za Zhi. 27:466–468. 2009.(In Chinese).
PubMed/NCBI
|
|
13
|
Takenaka H, Kishimoto S, Shibagaki R,
Nagata M, Noda Y and Yasuno H: Recurrent malignant proliferating
trichilemmal tumor: Local management with ethanol injection. Br J
Dermatol. 139:726–729. 1998.PubMed/NCBI
|
|
14
|
Arico M, La Rocca E, Noto G, Pravata G and
Rodolico V: Proliferating tricholemmal tumor with lymph node
metastasis. Br J Dermatol. 121:793–797. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Park BS, Yang SG and Cho KH: Malignant
proliferating trichilemmal tumor showing distant metastasis. Am J
Dermatopathol. 19:536–539. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Saida T, Oohara K, Hori Y and Tsuchiya S:
Development of a malignant proliferating trichilemmal cyst in a
patient with multiple trichilemmal cysts. Dermatologica.
166:203–208. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yoleri L, Baŝer NT and Kandiloğlu AR:
Malignant proliferating trichilemmal tumor arising in multiple
trichilemmal cysts. Ann Plast Surg. 43:575–576. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bahrami A and Folpe AL: Adult-type
fibrosarcoma: A reevaluation of 163 putative cases diagnosed at a
single institution over a 48-year period. Am J Surg Pathol.
34:1504–1513. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brownstein MH and Arluk DJ: Proliferating
trichilemmal cyst: A simulant of squamous cell carcinoma. Cancer.
48:1207–1214. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Trojani M, Contesso G, Coindre JM, Rouesse
J, Bui NB, de Mascarel A, Goussot JF, David M, Bonichon F and
Lagarde C: Soft tissue sarcomas of adults; study of pathological
prognostic variables and definition of a histopathological grading
system. Int J Cancer. 33:37–42. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
González-Orús Álvarez-Morujo R, García
Leal R, Vázquez JM Lasso and Yurrita B Scola: Malignant peripheral
nerve sheath tumour of the infra-orbital nerve. Neurocirugia
(Astur). 25:240–243. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wick MR, Swanson PE, Scheithauer BW and
Manivel JC: Malignant peripheral nerve sheath tumor. An
immunohistochemical study of 62 cases. Am J Clin Pathol.
87:425–433. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen L, Mao Y, Chen H and Zhou LF:
Diagnosis and management of intracranial malignant peripheral nerve
sheath tumors. Neurosurgery. 62:825–832; discussion 832. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Anghileri M, Miceli R, Fiore M, Mariani L,
Ferrari A, Mussi C, Lozza L, Collini P, Olmi P, Casali PG, et al:
Malignant peripheral nerve sheath tumors: Prognostic factors and
survival in a series of patients treated at a single institution.
Cancer. 107:1065–1074. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zou C, Smith KD, Liu J, Lahat G, Myers S,
Wang WL, Zhang W, McCutcheon IE, Slopis JM, Lazar AJ, et al:
Clinical, pathological, and molecular variables predictive of
malignant peripheral nerve sheath tumor outcome. Ann Surg.
249:1014–1022. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
L'heureux-Lebeau B and Saliba I: Updates
on the diagnosis and treatment of intracranial nerve malignant
peripheral nerve sheath tumors. Onco Targets Ther. 6:459–470.
2013.PubMed/NCBI
|
|
27
|
Aydin MD, Yildirim U, Gundogdu C, Dursun
O, Uysal HH and Ozdikici M: Malignant peripheral nerve sheath tumor
of the orbit: Case report and literature review. Skull Base.
14:109–113; discussion 113–114. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Plaza G, Ferrando J and Pinedo F:
Sinonasal fibrosarcoma: A case report. Eur Arch Otorhinolaryngol.
263:641–643. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Cattaneo F, Iaccio A, Guerra G, Montagnani
S and Ammendola R: NADPH-oxidase-dependent reactive oxygen species
mediate EGFR transactivation by FPRL1 in WKYMVm-stimulated human
lung cancer cells. Free Radic Biol Med. 51:1126–1136. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Testa D, Guerra G, Marcuccio G, Landolfo
PG and Motta G: Oxidative stress in chronic otitis media with
effusion. Acta Otolaryngol. 132:834–837. 2012.PubMed/NCBI
|
|
31
|
Conti V, Russomanno G, Corbi G, Guerra G,
Grasso C, Filippelli W, Paribello V, Ferrara N and Filippelli A:
Aerobic training workload affects human endothelial cells redox
homeostasis. Med Sci Sports Exerc. 45:644–653. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cozzolino I, Caleo A, Di Crescenzo V,
Cinelli M, Carlomagno C, Garzi A and Vitale M: Cytological
diagnosis of adult-type fibrosarcoma of the neck in an elderly
patient. Report of one case and review of the literature. BMC Surg.
13(Suppl 2): S422013.
|
|
33
|
Orbach D, Rey A, Cecchetto G, Oberlin O,
Casanova M, Thebaud E, Scopinaro M, Bisogno G, Carli M and Ferrari
A: Infantile fibrosarcoma: Management based on the European
experience. J Clin Oncol. 28:318–323. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Markal N, Kurtay A, Velidedeoğlu H and
Hücümenoğlu S: Malignant transformation of a giant proliferating
trichilemmal tumor of the scalp: Patient report and literature
review. Ann Plast Surg. 41:314–316. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Uchida N, Tsuzuki Y, Ando T, Mochida Y,
Yoshikawa M, Sekihara M, Kobayashi M, Ide M, Ohno Y and Kuwano H:
Malignant proliferating trichilemmal tumor in the skin over the
breast: A case report. Breast Cancer. 7:79–82. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chaichamnan K, Satayasoontorn K,
Puttanupaab S and Attainsee A: Malignant proliferating trichilemmal
tumors with CD34 expression. J Med Assoc Thai. 93(Suppl 6):
S28–S34. 2010.PubMed/NCBI
|