Introduction
Metaplastic carcinoma of the breast is a rare form
of breast cancer and possesses a poorer prognosis than other common
types of breast cancer (1).
Metaplastic carcinoma exhibits the metaplastic transformation of
glandular epithelium to squamous epithelium and mesenchymal tissue,
and accounts for <5% of all breast cancers (2) and may contain glandular and
non-glandular components with mixed epithelial and mesenchymal
tissue. Involvement of the axillary lymph node is rare, with
hematogenous metastasis occurring more commonly in cases of
metaplastic carcinoma (1,3). Metaplastic carcinoma demonstrates a
poorer prognosis and a higher risk of recurrence compared with
other types of breast cancer (3). It
typically presents as triple negative, therefore the effects of
hormonotherapy are limited (3,4). Due to
the heterogeneity of metaplastic carcinoma and its increased
complexity compared with more common types of breast cancer, mixed
chemotherapy regimens and dose schedules may be more effective and
appropriate (2). Due to the
distinction in surgical treatment and chemotherapy between
metaplastic carcinoma and other breast cancers, it is particularly
important to diagnose the tumor correctly (2). Metaplastic carcinoma demonstrates a
number of benign features similar to invasive ductal carcinoma in
mammograms and sonograms, and subsequently may be misdiagnosed as
benign lesions (4). Therefore, the
pre-operative differential diagnosis is particularly important as
each form of cancer warrants specific management. Although there
have been numerous clinical and pathological features reported
regarding metaplastic carcinoma, to the best of our knowledge, few
imaging features have been described (5). Therefore, the aim of the present study
is to demonstrate imaging features of metaplastic carcinoma of the
breast and associate these with pathological and
immunohistochemical results.
Materials and methods
Patient characteristics
The present study retrospectively reviewed data
collected from 15 patients with metaplastic carcinoma of the breast
treated at The Affiliated Hospital of Qingdao University (Qingdao,
China) between March 2012 and May 2014. In total, 2 cases were
excluded from the review of imaging features due to a lack of
mammography and sonography images; therefore, 13 patients were
retrospectively reviewed for mammography and sonography features.
Immunohistochemical results were reviewed for all 15 patients. The
patients were aged 37–80 years (mean, 49 years). All the patients
originally presented with a palpable mass in the breast, the
duration of which varied between 15 days and 1 year.
Mammographic examination and image
analysis
Mediolateral-oblique and craniocaudal images of each
breast were obtained with standard compression using the
Selenia® Dimensions® Mammography System
(Hologic, Inc., Marlborough, MA, USA). The mammography images were
retrospectively reviewed by 2 radiologists with >5 years
individual experience of breast imaging. The 2013 American College
of Radiology (ACR) breast imaging reporting and data system lexicon
(BI-RADS) was used to review the images (6), as follows: The shape of the lesion may
be classified as round, oval, lobulated or irregular; the margin
surrounding the lesion may be classified as circumscribed (>75%
of the margin is well defined), micro-lobulated, obscured
indistinct or spiculated; and the density of the lesion may be
classified as high, iso or low.
Sonographic examination and image
analysis
The ultrasound images of each breast were obtained
using a Siemens Acuson S2000 and EBU 7500 10–14 MHz linear probe
(Siemens AG, Munich, Germany). The sonography images were
retrospectively reviewed by 2 radiologists with >8 years
individual experience in breast sonography imaging, according to
the 2013 ACR BI-RADS lexicon, and were distinguished by shape,
margin, boundary, echo pattern and the posterior echo feature.
Color Doppler flow imaging was used to observe the shape and
distribution of blood flow in and surrounding the mass.
Histopathology
Histopathological results were obtained following
surgical resection. A pathological examination was performed for
all formalin-fixed (Tieta; Laiyang Far East Barrel Manufacturing
Co., Ltd.), paraffin-embedded (Taicang City Haotian Technology Co.,
Ltd., Suzhou, China) and hematoxylin-eosin (LABEST, Beijing, China)
stained representative tumor samples (3–5 µm thickness). A light
microscope with a ×40 objective lens (Olympus BX43; lens,
CH-BI45-T; Olympus, Tokyo, Japan) was used to observe tumor
tissues. Immunohistochemical (IHC) staining (SuperPolymer,
Shanghai, China) and chromogenic in situ hybridization
staining (ZytoDot® SPEC HER2 Probe Digoxigenin;
ZytoVision GmbH, Bremerhaven, Germany) for estrogen receptor (ER),
progesterone receptor (PR) and receptor tyrosine-protein kinase
erbB-2 (CerbB-2) (OriGene Technologies, Inc., Beijing, China) were
performed using the conventional peroxidase, anti-peroxidase
detection method, and peroxidase-labeled streptomycin resistance
biotin staining was used for IHC staining. Positive staining for ER
and PR was defined based on the percentage of stained nuclei, and
CerB-2 status was evaluated based on the percentage of tumor cells
and the intensity of membrane staining. The scores of HER2/CerB-2
varied between 0 and 3+, depending on the method recommended for
the DakoHercep Test (Dako Denmark A/S, Glostrup, Denmark). Tumors
with scores of 3, or with a >2.2-fold increase in HER2 gene
amplification, as determined by fluorescence in situ
hybridization (ZytoLight® SPEC HER2/CEN 17 Dual Color
Probe; ZytoVision GmbH) were considered to be positive for
HER2/CerB-2 overexpression.
The histopathology images were retrospectively
reviewed by 2 pathologists each with >5 years individual
experience in the pathological diagnosis of breast diseases. IHC
investigations for the presence of the ER and PR, CerbB-2 and P53
were performed on all masses, and axillary lymph node involvement
was assessed by pathological diagnosis.
Results
Pathological findings
Palpable masses in unilateral breasts were observed
in 13 female patients (median age, 49 years; age range 37–80
years). In total, 8 masses were identified in the left breast and 5
in the right breast. The diameter of the masses ranged between 0.9
and 6 cm.
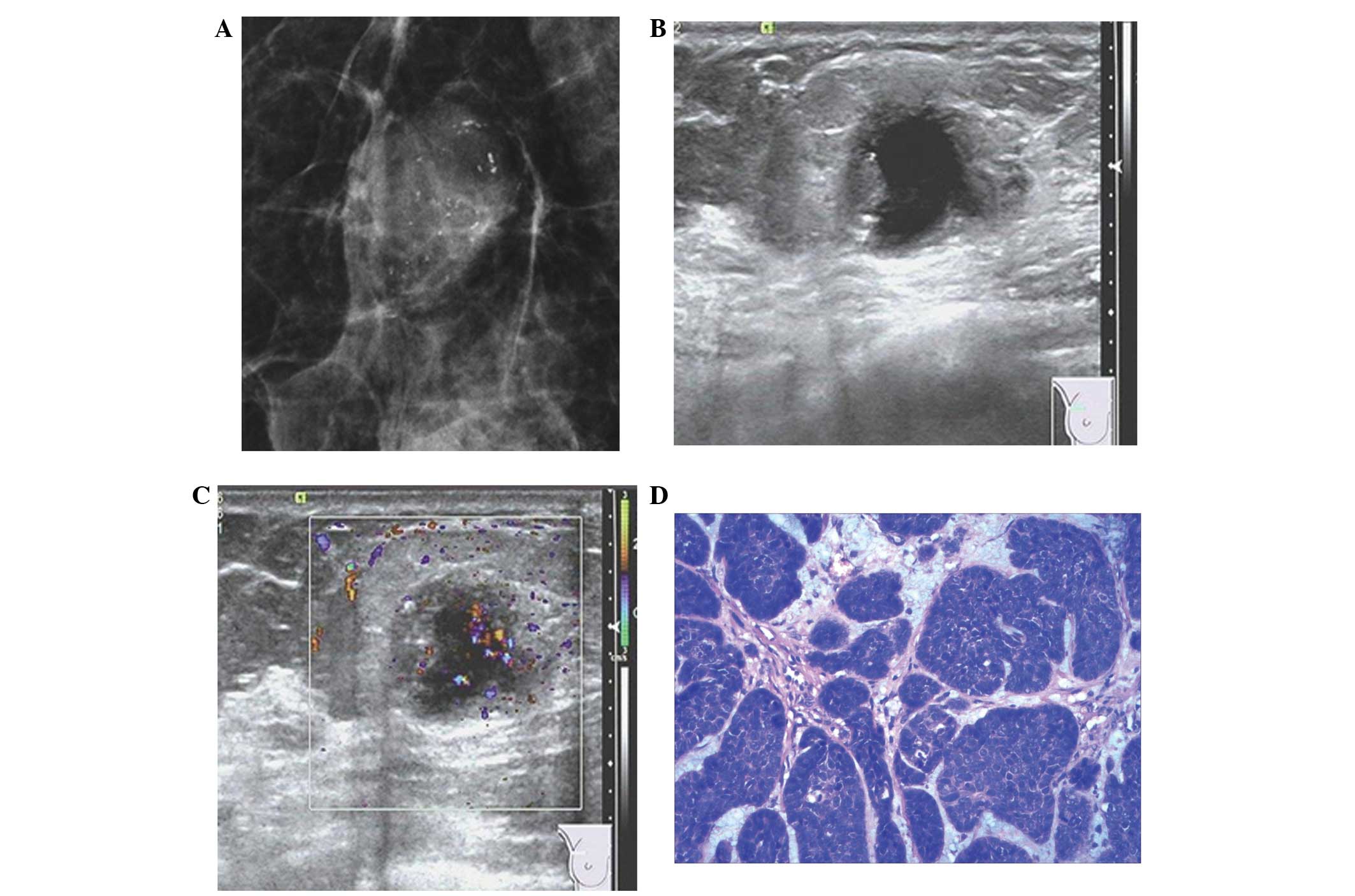
Mammography images were available for 13 patients.
In total, 84.6% had dense breasts. The mammographic features are
revealed in Table I. A representative
mammography scan is presented in Fig.
1A. The mammographic features observed in the 13 patients were
as follows: 7 patients (53.8%) possessed irregularly shaped masses,
while 6 patients (46.2%) possessed round or oval-shaped masses;
circumscribed margins and spicules were each identified in 4
patients; high density masses were detected in 9 patients (69.2%),
while 4 patients (30.8%) possessed iso-density masses; and
micro-calcifications were identified in 1 patient (7.7%).
 | Table I.Mammography features and tumor types
of 13 patients with breast metaplastic carcinomas. |
Table I.
Mammography features and tumor types
of 13 patients with breast metaplastic carcinomas.
|
| Pathological type of
carcinoma, n |
|
|---|
|
|
|
|
|---|
| Mammography
features | Squamous | Spindle | Matrix-producing |
Fibromatosis-like | Total, n (%) |
|---|
| Total | 7 | 3 | 2 | 1 | 13
(100.0) |
| Mass shape |
|
|
Round | 1 | 0 | 1 | 0 | 2
(15.4) |
| Oval | 1 | 2 | 1 | 0 | 4
(30.8) |
|
Lobular | 0 | 0 | 0 | 0 | 0 (0.0) |
|
Irregular | 5 | 1 | 0 | 1 | 7
(53.8) |
| Mass margin |
|
|
Circumscribed | 0 | 2 | 2 | 0 | 4
(30.8) |
|
Microlobulated | 0 | 0 | 0 | 0 | 0 (0.0) |
|
Indistinct | 4 | 1 | 0 | 0 | 5
(38.5) |
|
Spiculated | 3 | 0 | 0 | 1 | 4
(30.8) |
| Mass density |
|
| High | 5 | 2 | 1 | 1 | 9
(69.2) |
| Iso | 2 | 1 | 1 | 0 | 4
(30.8) |
| Low | 0 | 0 | 0 | 0 | 0 (0.0) |
| Calcification |
|
|
Present | 0 | 0 | 1 | 0 | 1 (7.7) |
| Not
present | 7 | 3 | 1 | 1 | 12 (92.3) |
Sonography findings
The sonographic findings are revealed in Table II. Representative sonograph images
are shown in Fig. 1B and C. The
sonographic features observed in the 13 patients were as follows:
Irregularly shaped masses were detected in 9 patients (69.2%),
while 4 patients (30.8%) possessed round or oval masses; 6 patients
(46.2%) possessed circumscribed margins, while spicules were
detected in 7 patients (53.8%); 10 patients (76.9%) demonstrated
complex echogenicity, while 3 patients (23.1%) demonstrated
homogeneous echogenicity (complex echogenicity consists of a
predominantly solid mass with certain tiny cystic regions
throughout); posterior acoustic enhancement was detected in 8
patients (61.5%); abundant blood flow was identified in 7 patients
(53.8%), while a low blood flow was detected in 3 patients (23.1%);
and little blood flow was detected in 3 patients (23.1%).
| Table II.Sonography features and tumor types of
13 patients with breast metaplastic carcinomas. |
Table II.
Sonography features and tumor types of
13 patients with breast metaplastic carcinomas.
|
| Pathological type of
carcinoma |
|
|---|
|
|
|
|
|---|
| Sonography
features | Squamous | Spindle | Matrix-producing |
Fibromatosis-like | Total, n (%) |
|---|
| Total, n | 7 | 3 | 2 | 1 | 13
(100.0) |
| Mass shape |
|
|
Round | 1 | 1 | 0 | 0 | 2
(15.4) |
| Oval | 0 | 1 | 1 | 0 | 2
(15.4) |
|
Lobular | 0 | 0 | 0 | 0 | 0 (0.0) |
|
Irregular | 6 | 1 | 1 | 1 | 9
(69.2) |
| Mass margin |
|
|
Circumscribed | 3 | 2 | 1 | 0 | 6
(46.2) |
|
Microlobulated | 0 | 0 | 0 | 0 | 0 (0.0) |
|
Indistinct | 0 | 0 | 0 | 0 | 0 (0.0) |
|
Spiculated | 4 | 1 | 1 | 1 | 7
(53.8) |
| Echogenicity |
|
|
Homogeneous | 3 | 0 | 0 | 0 | 3
(23.1) |
|
Complex | 4 | 3 | 2 | 1 | 10 (76.9) |
| Posterior acoustic
enhancement |
|
|
Present | 4 | 2 | 2 | 0 | 8
(61.5) |
| Not
present | 3 | 1 | 0 | 1 | 5
(38.5) |
Final pathological diagnosis
The final pathological diagnoses were obtained by
surgical biopsy for all 15 patients. In total, 8 patients were
diagnosed with squamous cell carcinoma, 3 patients with spindle
cell carcinoma, 2 patients with matrix-producing carcinoma, 1
patient with fibromatosis-like carcinoma and 1 patient with mixed
metaplastic carcinoma. The overall immunohistochemical profile for
all 15 patients is demonstrated in Table III. Briefly, 13 patients (86.7%;
13/15) did not express ER, 14 patients (93.3%; 14/15) did not
express either PR or CerbB-2 and 7 patients (63.6%; 7/11) did
express P53. Axillary lymph node involvement was observed in 1
patient.
| Table III.Immunohistochemical features and
tumor types of 15 patients with breast metaplastic carcinomas. |
Table III.
Immunohistochemical features and
tumor types of 15 patients with breast metaplastic carcinomas.
|
|
| Immunohistochemical
markers |
|---|
|
|
|
|
|---|
|
|
| ER | PR | CerbB-2 | P53a |
|---|
|
|
|
|
|
|
|
|---|
| Pathological type
of carcinoma | Total, n | + | − | + | − | + | − | + | − |
|---|
| Total, n | 15 | 2 | 13 | 1 | 14 | 1 | 14 | 7 | 4 |
| Squamous | 8 | 2 | 6 | 1 | 7 | 1 | 7 | 5 | 3 |
| Spindle | 3 | 0 | 3 | 0 | 3 | 0 | 3 | 0 | 0 |
|
Matrix-producing | 2 | 0 | 2 | 0 | 2 | 0 | 2 | 1 | 1 |
|
Fibromatosis-like | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 |
| Mixed
metaplastic | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 |
Discussion
Metaplastic carcinoma of the breast is a rare form
of ductal carcinoma, which exhibits metaplastic transformation of
glandular epithelium to non-glandular mesenchymal tissue (1–3). Numerous
studies have reported that metaplastic carcinoma of the breast may
originate from myoepithelial tissue (7). The carcinoma usually occurs among women
aged >50 years, and often presents as a palpable mass that grows
rapidly; therefore, the majority of patients present with larger
palpable masses compared to invasive ductal carcinoma (4,5).
According to the histological classification of
breast tumors from the World Health Organization in 2012,
metaplastic carcinoma of the breast may be classified into several
types, as follows: Non-special type metaplastic carcinoma,
including low-grade adenosquamous, fibromatosis-like, squamous cell
and spindle cell carcinoma; metaplastic carcinoma with mesenchymal
differentiation, including chondroid and osseous alteration; mixed
metaplastic carcinoma; and myoepithelial cell carcinoma (8). Choi et al (4) reported that the most common type of
metaplastic carcinoma was squamous cell carcinoma, which accounts
for 0.5–3.7% of all types of breast cancer, followed by spindle
cell carcinoma and matrix-producing carcinoma. The present study
supports that squamous cell carcinoma is the most common type of
metaplastic carcinoma, accounting for 53.8% of all cases, followed
by spindle cell carcinoma at 20%. These findings are consistent
with previous studies (4,5).
Metaplastic carcinoma exhibits various biological
behaviors compared with invasive ductal carcinoma, and metaplastic
carcinoma demonstrates a decreased tendency to involve the axillary
lymph node (7). Leddy et al
(1) reported that the incidence of
axillary lymph node involvement ranges between 8 and 40%, which is
consistent with the findings of the present study, where axillary
lymph node metastasis was observed in 6.7% of the patients.
Metaplastic carcinoma tends to spread hematogenously to the lung
and bone, rather than through the lymphatic system (3). There is not a large involvement of the
axillary lymph node, despite the poor prognosis (1,3,5).
Various subtypes of metaplastic carcinoma exhibit
different imaging findings. Yang et al (5) reported that metaplastic carcinoma
demonstrates more benign features compared with invasive ductal
carcinoma, which often exhibits an oval or rounded shape, and the
authors state that metaplastic carcinomas usually possess a
circumscribed margin without malignant calcification in the mass.
Leddy et al (1) revealed that
metaplastic carcinomas may exhibit irregular shapes, indistinct or
spiculated margins with certain amorphous or pleomorphic
calcification. Previous studies have reported different views
concerning the imaging findings of metaplastic carcinoma (4,5).
Consequently, in the present study, the most common mammographic
findings of squamous carcinoma were an irregular shaped mass with a
spiculated margin and a high density, while spindle cell carcinoma
and matrix-producing carcinoma exhibited an oval shaped mass with
circumscribed margin and a slightly high density. On sonography,
according to a previous study (9),
metaplastic carcinoma usually demonstrates benign features with an
oval or roundly shaped mass, a circumscribed margin and a
homogeneous echogenicity with posterior acoustic enhancement.
However, in the present study the most common sonographic features
observed were a lobular or irregular shape, spiculated margin,
heterogeneous echogenicity and posterior acoustic enhancement.
Therefore, the present results are not consistent
with those of previous studies (9,10). This
may be due to the majority of patients in the present study
possessing squamous cell carcinoma (53.8%), the biological behavior
of which is similar to that of invasive ductal carcinoma with
invasive growth. Therefore, squamous cell carcinoma consistently
demonstrates malignant features (3).
In addition, since a fibrous capsule usually surrounds the mass of
spindle cell carcinoma, spindle cell carcinoma consistently
exhibits benign features (8).
Therefore, the present study suggests that the imaging features of
various subtypes of metaplastic carcinoma have certain
characteristics. Few imaging features of metaplastic carcinoma of
the breast have been reported, and since the number of patients
reviewed in the present study is limited, additional investigation
is required.
Metaplastic carcinoma demonstrates a poorer
prognosis and lower survival rate compared with invasive ductal
carcinoma (1). Esbah et al
(2) revealed that the poor prognosis
of metaplastic carcinoma may be explained by the increased tumor
size, higher proliferation index, histopathological tumor
heterogeneity, triple negative feature and lack of effective
targeted therapies. Previous studies (4,10,11) demonstrate that a more regular and more
circumscribed mass may reflect a higher histological grade, while
those lesions that appear benign may reflect tumor aggressiveness
associated with a poorer prognosis and a low survival rate. This
may be due to the association with the triple negativity of
metaplastic carcinoma of the breast. Out of the 15 patients in the
present study, only 2 patients expressed ER, 1 patient expressed PR
and 1 patient expressed CerbB-2, which is similar to the results
from previous studies (1,4,8). The
absence of hormone receptor expression on tumors restricts the
application of hormonal therapy. Chao et al (12) reported no survival advantage of
post-operative radiotherapy and various neoadjuvant chemotherapy
regimens; however, different and/or mixed chemotherapy regimens and
dose schedules may be more effective. Therefore, traditional
surgery is the preferred treatment choice (2). However, Song et al (3) identified that local tumor recurrence was
common following a simple mastectomy; therefore, surgical
techniques, including radical mastectomy and modified radical
mastectomy, such as axillary dissection, may improve the prognosis
and survival rate of a patient. Additionally, local and distant
metastases are more frequent than other types of breast cancer
during the follow-up subsequent to surgery (1). Therefore, a systematic evaluation
concerning local recurrence and surgical techniques is
essential.
Diagnosing metaplastic carcinoma cannot rely on
imaging features alone. Core needle biopsy and aspiration cytology
may aid in a pre-operative diagnosis, but the probability of
misdiagnosis would increase in the presence of hemorrhage or
necrosis due to inadequate sampling or a poor choice of puncture
region (1). In the majority of cases,
the transition foci between metaplastic carcinoma and invasive
ductal carcinoma were only observed following surgical biopsy
(1,3,9,11). Therefore, extensive sampling by
surgical biopsy and immunohistochemical examination should be
performed to avoid misdiagnosis.
In conclusion, metaplastic carcinoma is a rare form
of breast cancer with various subtypes. It is important to
differentiate metaplastic carcinoma from invasive ductal carcinoma,
as the prognosis for metaplastic carcinoma is poor and the survival
rate is low. Multimodality imaging examinations have certain
imaging features, and combined with the observation of posterior
acoustic enhancement and an absence of hormone receptor expression,
may aid the differential diagnosis of metaplastic carcinoma and the
development of a novel treatment strategy.
References
|
1
|
Leddy R, Irshad A, Rumboldt T, Cluver A,
Campbell A and Ackerman S: Review of metaplastic carcinoma of the
breast: Imaging findings and pathologic features. J Clin Imaging
Sci. 2:212012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Esbah O, Turkoz FP, Turker I, Durnali A,
Ekinci AS, Bal O, Sonmez OU, Budakoglu B, Arslan UY and Oksuzoglu
B: Metaplastic breast carcinoma: Case series and review of the
literature. Asian Pac J Cancer Prev. 13:4645–4649. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Song Y, Liu X, Zhang G, Song H, Ren Y, He
X, Wang Y, Zhang J, Zhang Y, Sun S, et al: Unique
clinicopathological features of metaplastic breast carcinoma
compared with invasive ductal carcinoma and poor prognostic
indicators. World J Surg Oncol. 11:129–138. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Choi BB and Shu KS: Metaplastic carcinoma
of the breast: Multimodality imaging and histopathologic
assessment. Acta Radiol. 53:5–11. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yang WT, Hennessy B, Broglio K, Mills C,
Sneige N, Davis WG, Valero V, Hunt KK and Gilcrease MZ: Imaging
differences in metaplastic and invasive ductal carcinomas of the
breast. AJR Am J Roentgenol. 189:1288–1293. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mercado CL: BI-RADS update. Radiol Clin
North Am. 52:481–487. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pitts WC, Rojas VA, Gaffey MJ, Rouse RV,
Esteban J, Frierson HF, Kempson RL and Weiss LM: Carcinomas with
metaplasia and sarcomas of the breast. Am J Clin Pathol.
95:623–632. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shin HJ, Kim HH, Kim SM, Kim DB, Kim MJ,
Gong G, Im SA and Cha ES: Imaging Features of Metaplastic Carcinoma
with Chondroid Differentiation of the Breast. AJR. 188:691–697.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Oberman HA: Metaplastic carcinoma of the
breast. A clinicopathologic study of 29 patients. Am J Surg Pathol.
11:918–929. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Park JM, Han BK, Moon WK, Choe YH, Ahn SH
and Gong G: Metaplastic carcinoma of the breast: Mammographic and
sonographic findings. J Clin Ultrasound. 28:179–186. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kaas R, Kroger R, Hendriks JH, Besnard AP,
Koops W, Pameijer FA, Prevoo W, Loo CE and Muller SH: The
significance of circumscribed malignant mammographic masses in the
surveillance of BRCA 1/2 gene mutation carriers. Eur Radiol.
14:1647–1653. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chao TC, Wang CS, Chen SC and Chen MF:
Metaplastic carcinomas of the breast. J Surg Oncol. 71:220–225.
1999. View Article : Google Scholar : PubMed/NCBI
|