Prostate cancer (PCa), a common non-skin,
sex-limited cancer, is the second cause of cancer-associated
mortality (after lung cancer) in the USA (1,2) and the
second most prevalent cancer among Iranian men (3). Worldwide, PCa is the second most
commonly diagnosed cancer and, according to the International
Agency for Research on Cancer's GLOBOCAN 2012 (4) database, it is the fifth leading cause of
cancer-associated mortality in men. The incidence of PCa is
increasing worldwide, although there is a marked variation in its
incidence among different regions (5). The clinical configuration of PCa has
noticeably altered over the past few years. As a localized disease,
it is easily treated by radical radiation therapy or a
prostatectomy; however, if the tumor becomes malignant, it
transforms into a life-threatening disease (6).
The progression and application of novel
high-resolution technologies has enhanced the detection of genomic
alterations, enabling elucidation of the complex nature and
heterogeneity of PCa (7). The
differentiation of PCa tumors is typically based on the serum
expression levels of prostate-specific antigen (PSA), although, in
certain cases, PSA levels do not accurately reflect tumor burden
(8). Previous studies have identified
a number of genetic, epigenetic and environmental risk factors for
PCa (9–11). Among them, genetic aberrations and
chromosomal changes have been suggested to serve a significant role
in the development and progression of PCa (12). At present, >50 PCa susceptibility
loci have been identified using genome-wide association studies
(13,14). The emerging picture of the genomic
complexity of PCa includes frequent large-scale genomic
rearrangements (15), gene fusions
(16,17), genetic deletions (15) and gene amplifications (18).
Gene amplification, which may occur due to an
increase in copy number of certain regions of chromosomes, has been
identified in several malignancies, including PCa (18,19).
Previous studies have reported that the genetic duplication of
various genes was associated with PCa malignancy, including
androgen receptor (20), enhancer of
zeste homolog 2 (21), eukaryotic
translation initiation factor 3 (22), calcium-activated potassium channel
subunit α-1 (23), minichromosome
maintenance complex component 7 (24), prostate leucine zipper (25) and hypoxia-inducible factor 1 (26).
Human epidermal growth factor receptor 2 (HER2) is a
member of the class I receptor tyrosine kinase family and has
substantial homology to epidermal growth factor receptor, HER3 and
HER4 (27). HER2 overexpression
and/or gene amplification occur in a variety of human epithelial
tumors, particularly in breast cancer, in which the receptor and
its gene have been investigated extensively (28). Conversely, the significance of HER2
overexpression and gene amplification in PCa remains controversial.
Previous studies have used immunohistochemical analysis to evaluate
HER2 protein expression in primary prostate specimens,
demonstrating expression rates ranging from 0–100% (29–31).
Therefore, the exact prevalence of HER2 gene amplifications in
primary PCa remains unknown, likely owing to the wide range of
antibodies and methods used in these studies (32,33).
The HER2/neu proto-oncogene, which is located on
chromosome 17 (OMIM: 164870), encodes a transmembrane tyrosine
kinase growth factor receptor (34),
whose overexpression was shown to be involved in the development of
various types of human cancer, including non-small-cell lung
cancer, colon cancer and breast cancer, and may have prognostic
value (35,36). Apparent chromosome 17 polysomy,
defined by increased chromosome enumeration probe 17 (CEP17) signal
number, is a common genetic aberration in breast cancer and
represents an alternative mechanism for increasing HER2 copy number
(37). However, the prognostic value
of HER2/neu amplification in PCa remains controversial (38).
Chromosomal aberrations associated with PCa have
been evaluated using various techniques, including classical
cytogenetics (39), loss of
heterozygosity analysis (40),
fluorescence in situ hybridization (FISH) (41) and, most commonly, comparative genomic
hybridization (CGH) (42). Although
the criteria for amplification have varied between studies, they
have implicated several chromosomal regions, such as 6q, 8p, 10q,
13q, 16q and Xq, that may harbor genes involved in the
tumorigenesis of PCa (24,43).
The present study aimed to investigate the frequency
of HER2 amplification in prostate biopsies from Iranian (Tehran
province) patients using chromogenic in situ hybridization
(CISH), which permits the rapid analysis of a large number of
tumors (44). Although the FISH
method has been verified for the histological analysis of tissues,
the evaluation of tumor morphology using FISH is challenging and
the fluorescence fades quickly (45).
These limitations may be overcome by CISH, which enables
visualization of the amplification product along with morphological
features (46). Furthermore, CISH
technology is superior to high-throughput HER2 genetic testing due
its speed, although FISH remains the method of choice for rapid
low-throughput HER2 genetic testing.
The present study was approved by the Ethics
Committee of Tehran University of Medical Sciences (Tehran, Iran).
Suitable patients from the oncology wards or outpatient clinics of
Imam Khomeini Hospital (Tehran, Iran) were approached for
participation in the study, and informed consent was obtained.
Inclusion criteria for the study were a PSA level of >4, a
diagnosis of progressive prostate cancer, an age of >54 years, a
Gleason score of >2 (47) and the
male gender. Formalin-fixed, paraffin-embedded (FFPE) specimens
were obtained from 32 consecutive PCa patients who underwent
surgery between May 2013 and February 2015. Adjacent normal tissue
was used as a control. To account for tumor heterogeneity, a
minimum of 3 cylindrical core biopsies, 0.6 mm in diameter, were
harvested from different regions of each tumor. A total of 15
tissue sections (2-mm thick) were sliced from each
paraffin-embedded tumor block and mounted onto glass slides. The
first tissue section was stained with hematoxylin and eosin and
visualized under a light microscope to ascertain the region of
interest. In all cases, a serum sample was measured by
Elecsys® total PSA and free PSA kits (Roche Diagnostics,
Basel, Switzerland).
The stage (extent) of prostate cancer is one of the
most important factors in choosing treatment options and predicting
prognosis. The stage is based on the prostate biopsy results
(including the Gleason score), the blood PSA level at the time of
diagnosis, the results of any other exams or tests that were
performed to determine metastasis and the pathological stage
post-surgery. There are 4 categories for describing the local
extent of a prostate tumor, ranging from T1 to T4 (48).
Red/green signals were counted manually. Data
analysis was performed using SPSS software version 18 (SPSS, Inc.,
Chicago, IL, USA). Scale variables were analyzed for normality
using the Kolmogorov-Smirnov test. Group comparisons of continuous
variables were conducted using the independent-samples
t-test. When a variable was non-normally distributed,
Mann-Whitney or Kruskal-Wallis non-parametric tests were performed.
GraphPad Prism version 5.0 software for Windows (GraphPad Software,
La Jolla, CA, USA) was used to illustrate the data through graphs.
Data are expressed as the mean ± standard deviation. P<0.05 was
considered to indicate a statistically significant difference.
For statistical analysis, patients were divided into
two groups consisting of patients with or without HER2
amplification. Variables were assessed within each group and the
results are presented in Tables
I–III. The demographic data of
patients with PCa with and without HER2 amplification are shown in
Table I. There were no associations
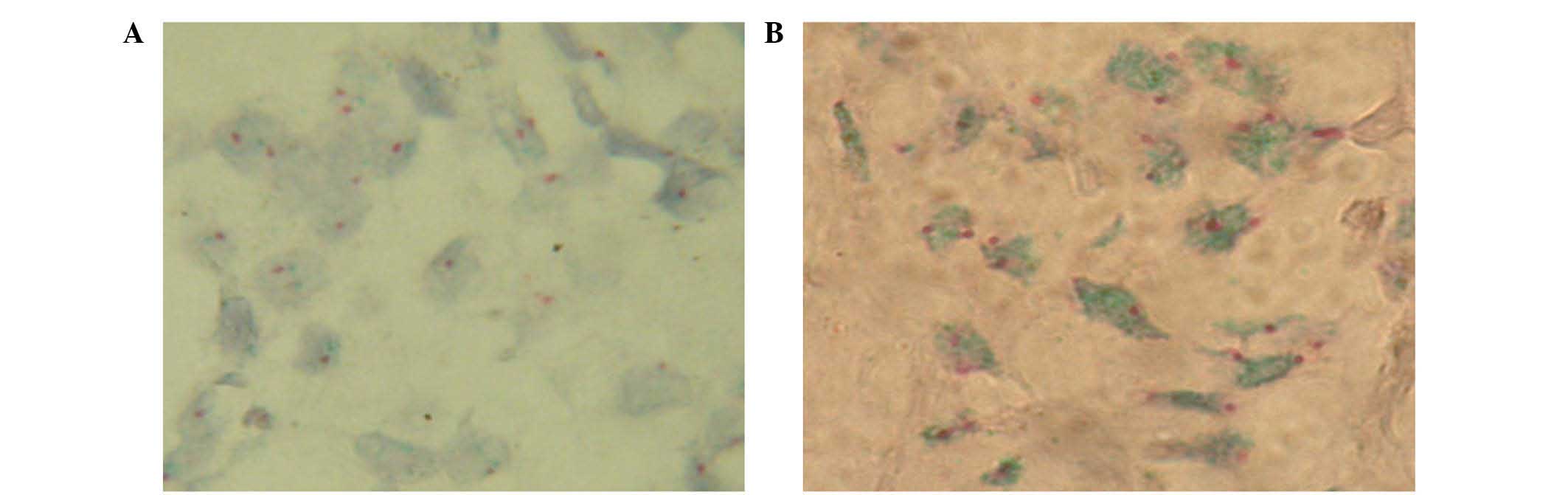
among the serum levels of PSA, green/red ratios (Fig. 1) or Gleason scores in patients without
HER2 amplification.
There was a weak association between the green/red
ratio and age in patients without HER2 amplification (P=0.046;
Table II), thus suggesting that
younger patients exhibited a lower tendency for HER2 amplification.
In addition, a positive correlation (P=0.004) was observed between
the serum levels of PSA and Gleason score (Table II). The associations between the
green/red ratio and PSA levels or Gleason score were not
significant (P=0.228 and 0.941, respectively; Table II).
For the analysis, patients were divided into two
separate groups based on the level of HER2 gene amplification
(i.e., with and without amplification). The first group consisted
of 19 patients and the second group consisted of 13 patients. A
high level of HER2 gene amplification was considered when the
HER2/CEP17 ratio was >2.2 (Fig.
1).
The mean ages were 73.7 and 63.3 years for patients
with left- and right-side tumors, respectively, which were not
significantly different (P=0.15; Table
III). With the exception of the serum levels of PSA (P=0.009),
there were no significant differences in any of the parameters
(green/red ratio and Gleason score) between patients with left- and
right-sided tumors. The mean Gleason score among patients was 5,
and the Gleason score showed no association with the pathologic
stage (P=0.303; Table III). The
tumors were composed of different Gleason scores, but were between
stages T2 and T5 (Table III).
Similar to the patients without HER2 amplification, there was a
significant association between the Gleason score and serum levels
of PSA in patients with HER2 amplification (P<0.001; Table IV). However, there was no significant
association between the other parameters in patients with HER2
amplification (P>0.05; Table IV).
The tumor position was not significantly associated with the mean
age, PSA levels, green/red ratio or Gleason score of patients with
HER2 amplification, although a significant correlation was observed
between the Gleason score and pathologic stage (P=0.002; Table V).
DNA ploidy has been accepted as a significant
predictor of prognosis in patients with PCa (50). In the present study, amplification and
overexpression of HER2 was demonstrated in patients with PCa, which
has previously been associated with cancer progression, a poor
prognosis and development of androgen independency (51). HER2 status is routinely assigned using
in situ hybridization to assess HER2 gene amplification, but
interpretation of in situ hybridization results may be
challenging in tumors with chromosome 17 polysomy or intratumoral
genetic heterogeneity. Apparent chromosome 17 polysomy, defined by
increased CEP17 signal number, is a common genetic aberration in
breast cancer and represents an alternative mechanism for
increasing HER2 copy number. Elevated CEP17 count (polysomy) has
been linked with adverse clinicopathologic features and HER2
overexpression, although there are numerous discrepancies in the
literature (37). HER2 overexpression
and/or amplification are recurrently reported in numerous tumor
types, and have been shown to have significant therapeutic
implications in patients with cancer (33). A meta-analysis of 5,976 patients
demonstrated that HER2/neu overexpression was associated with
mortality and recurrence in patients with PCa (52). Furthermore, it has been suggested that
HER2 overexpression at the protein level is significantly
associated with the amplification of HER2 (53). FISH is considered the gold standard
method for detecting gene amplification, and has been reported to
be more accurate than flow cytometry and immunohistochemistry
(54). An increasing number of
authors have employed the CISH method for determining gene
amplification in various types of cancer (37,55,56). CISH
is a recently developed technique in which the DNA probe is located
based on an immunoperoxidase reaction. This method is similar to
FISH, although it does not involve the use of fluorescence
microscopy. In addition, FISH signals fade within a few weeks and
the FISH results must be recorded using expensive digital systems,
which is not required for CISH staining. Owing to its resemblance
to immunohistochemistry staining (57), CISH is also easier to interpret by
pathologists who are not trained in fluorescence microscopy.
Furthermore, in previous studies, CISH was observed to be
well-correlated with FISH (46,58–60).
The present study used standard CISH to demonstrate
that HER2 was amplified in Iranian (Tehran province) patients with
PCa. Notably, HER2 amplification was observed in >50% of
patients. Similarly, using a FISH technique, a study on 44 patients
with PCa demonstrated 53 and 80% low copy amplification in
non-metastatic and metastatic samples, respectively (61). The results of the present study were
consistent with previous studies, in which HER2 amplification was
reported in 44 and 41% of 62 and 113 Americans, respectively, using
the FISH method (54,62), whereas another analysis reported no
HER2 amplification (63).
Furthermore, in a previous study, FFPE tissue blocks from 88
patients demonstrated a minor amplification rate of 9.3% (8/88
cases) (64). Similarly, Qi et
al (53) used a FISH method and
demonstrated that only 5.8% of Chinese patients with PCa had such a
genetic alteration, and an investigation of 93 cancer samples
showed that 6.5% had low levels of HER2 amplification, which was
co-amplified with the topoisomerase (DNA) II α gene (65). These conflicting results may exist due
to variation in the sample size and method used, or as a result of
genetic heterogeneity. Furthermore, the findings may suggest that
the CISH method is superior to FISH for HER2 detection in PCa
samples. CISH has also been utilized for detection of copy number
variation in the HER2/neu gene (66).
In addition, the accuracy and reproducibility of CISH has been
demonstrated in a previous study of breast carcinoma, in which the
authors suggested that CISH may be regarded as a practical
alternative for FISH (67). Other
studies have considered this matter and proposed that CISH is a
viable alternative to FISH and had similar properties; for example,
both are in situ hybridization techniques and directly
visualise the number of gene copies present in the nucleus, but
CISH is cheaper and it produces a stable record of the slide that
can be interpreted with a light microscope in the background of the
tumour histopathology (68).
Permanent staining and the absence of a fluorescent dye make CISH a
suitable replacement for FISH (69).
In addition, its usability, relative inexpensiveness and speed make
CISH more attractive than FISH for assessing HER2
amplification/overexpression (59,70).
In conclusion, to the best of our knowledge, the
present study is the first to report the amplification of HER2 in
Iranian patients (Tehran province) with PCa. Furthermore, it was
demonstrated that there were no associations among the serum levels
of PSA, green/red ratios or Gleason scores in patients without HER2
amplification. Conversely, there was a weak correlation between the
green/red ratio and age in these patients (P=0.046), which
suggested the tendency for younger patients to exhibit lower levels
of HER2 amplification. Notably, there was no association between
the green/red ratio and pathologic stage of patients without HER2
amplification (P=0.873), although the increasing trend suggested
that clinicians may consider Herceptin as a drug of choice for
patients with PCa. In addition, there was no association between
PSA levels (P=0.749) or Gleason score (P=0.057) and pathologic
stage in patients without HER2 amplification. In patients with HER2
amplification, there was a significant association between the
Gleason score and the serum level of PSA (P<0.001). However,
there was no significant association between the other parameters
in patients with HER2 amplification (P>0.05). The tumor position
was not significantly associated with the mean age, PSA level,
green/red ratio or Gleason score of the patients with HER2
amplification, although a significant correlation was observed
between the Gleason score and pathological stage (P=0.002; Table V). Finally, the present study
confirmed the results of previous studies, which suggested that the
CISH method may be considered a valuable replacement for FISH.
Further studies involving PCa samples are required in order to
validate the results of the present study.
The present study was supported by a research grant
from Tehran University of Medical Sciences (Tehran, Iran;
516478).
|
1
|
Braga-Basaria M, Dobs AS, Muller DC,
Carducci MA, John M, Egan J and Basaria S: Metabolic syndrome in
men with prostate cancer undergoing long-term androgen-deprivation
therapy. J Clin Oncol. 24:3979–3983. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Perner S, Mosquera JM, Demichelis F, Hofer
MD, Paris PL, Simko J, Collins C, Bismar TA, Chinnaiyan AM, De
Marzo AM and Rubin MA: TMPRSS2-ERG fusion prostate cancer: An early
molecular event associated with invasion. Am J Surg Pathol.
31:882–888. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kolahdoozan S, Sadjadi A, Radmard AR and
Khademi H: Five common cancers in Iran. Arch Iran Med. 13:143–146.
2010.PubMed/NCBI
|
|
4
|
Center MM, Jemal A, Lortet-Tieulent J,
Ward E, Ferlay J, Brawley O and Bray F: International variation in
prostate cancer incidence and mortality rates. Eur Urol.
61:1079–1092. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wong MC, Goggins WB, Wang HH, Fung FD,
Leung C, Wong SY, Ng CF and Sung JJ: Global incidence and mortality
for prostate cancer: Analysis of temporal patterns and trends in 36
countries. Eur Urol. June 8–2016.(Epub ahead of print). View Article : Google Scholar
|
|
6
|
Kallioniemi OP and Visakorpi T: Genetic
basis and clonal evolution of human prostate cancer. Adv Cancer
Res. 68:225–255. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Boyd LK, Mao X and Lu YJ: The complexity
of prostate cancer: Genomic alterations and heterogeneity. Nat Rev
Urol. 9:652–664. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Heidenreich A, Bellmunt J, Bolla M, Joniau
S, Mason M, Matveev V, Mottet N, Schmid HP, van der Kwast T, Wiegel
T, et al: EAU guidelines on prostate cancer. Part 1: Screening,
diagnosis, and treatment of clinically localised disease. Eur Urol.
59:61–71. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Damaschke N, Yang B, Bhusari S, Svaren J
and Jarrard D: Epigenetic susceptibility factors for prostate
cancer with aging. The Prostate. 2013.73(16): 1721–1730. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Parent ME and Siemiatycki J: Occupation
and prostate cancer. Epidemiol Rev. 23:138–143. 2015. View Article : Google Scholar
|
|
11
|
Salmaninejad A, Sadeghi N and Ghadami S:
Alterations of KRAS exon 2 codon 12/13 mutation status in prostatic
adenocarcinoma; Bioinformatics aspects. Arch Can Res. 4:22016.
View Article : Google Scholar
|
|
12
|
Shen MM and Abate-Shen C: Molecular
genetics of prostate cancer: New prospects for old challenges.
Genes Dev. 24:1967–2000. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Eeles RA, Al Olama AA, Benlloch S,
Saunders EJ, Leongamornlert DA, Tymrakiewicz M, Ghoussaini M,
Luccarini C, Dennis J, Jugurnauth-Little S, et al: Identification
of 23 new prostate cancer susceptibility loci using the iCOGS
custom genotyping array. Nat Genet. 45:385–391, 391e1-2. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Takata R, Akamatsu S, Kubo M, Takahashi A,
Hosono N, Kawaguchi T, Tsunoda T, Inazawa J, Kamatani N, Ogawa O,
et al: Genome-wide association study identifies five new
susceptibility loci for prostate cancer in the Japanese population.
Nat Genet. 42:751–754. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Barbieri CE, Demichelis F and Rubin MA:
Molecular genetics of prostate cancer: Emerging appreciation of
genetic complexity. Histopathology. 60:187–198. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tomlins SA, Laxman B, Dhanasekaran SM,
Helgeson BE, Cao X, Morris DS, Menon A, Jing X, Cao Q, Han B, et
al: Distinct classes of chromosomal rearrangements create oncogenic
ETS gene fusions in prostate cancer. Nature. 448:595–599. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kumar-Sinha C, Tomlins SA and Chinnaiyan
AM: Recurrent gene fusions in prostate cancer. Nat Rev Cancer.
8:497–511. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Santarius T, Shipley J, Brewer D, Stratton
MR and Cooper CS: A census of amplified and overexpressed human
cancer genes. Nat Rev Cancer. 10:59–64. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Salmaninejad A, Ghadami S, Dizaji MZ,
Golchehre Z, Estiar MA, Zamani MR, Ebrahimzadeh-Vesal R, Nowroozi
MR and Shakoori A: Molecular characterization of KRAS, BRAF, and
EGFR genes in cases with prostatic adenocarcinoma; reporting
bioinformatics description and recurrent mutations. Clin Lab.
61:749–759. 2015.PubMed/NCBI
|
|
20
|
Brown RS, Edwards J, Dogan A, Payne H,
Harland SJ, Bartlett JM and Masters JR: Amplification of the
androgen receptor gene in bone metastases from hormone-refractory
prostate cancer. J Pathol. 198:237–244. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Saramäki OR, Tammela TL, Martikainen PM,
Vessella RL and Visakorpi T: The gene for polycomb group protein
enhancer of zeste homolog 2 (EZH2) is amplified in late-stage
prostate cancer. Genes Chromosomes Cancer. 45:639–645. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Saramäki O, Willi N, Bratt O, Gasser TC,
Koivisto P, Nupponen NN, Bubendorf L and Visakorpi T: Amplification
of EIF3S3 gene is associated with advanced stage in prostate
cancer. Am J Pathol. 159:2089–2094. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bloch M, Ousingsawat J, Simon R, Schraml
P, Gasser TC, Mihatsch MJ, Kunzelmann K and Bubendorf L: KCNMA1
gene amplification promotes tumor cell proliferation in human
prostate cancer. Oncogene. 26:2525–2534. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ren B, Yu G, Tseng GC, Cieply K, Gavel T,
Nelson J, Michalopoulos G, Yu YP and Luo JH: MCM7 amplification and
overexpression are associated with prostate cancer progression.
Oncogene. 25:1090–1098. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang R, Xu J, Saramäki O, Visakorpi T,
Sutherland WM, Zhou J, Sen B, Lim SD, Mabjeesh N, Amin M, et al:
PrLZ, a novel prostate-specific and androgen-responsive gene of the
TPD52 family, amplified in chromosome 8q21. 1 and overexpressed in
human prostate cancer. Cancer Res. 64:1589–1594. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Saramäki OR, Savinainen KJ, Nupponen NN,
Bratt O and Visakorpi T: Amplification of hypoxia-inducible factor
1alpha gene in prostate cancer. Cancer Genet Cytogenet. 128:31–34.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rimawi MF, Mayer IA, Forero A, Nanda R,
Goetz MP, Rodriguez AA, Pavlick AC, Wang T, Hilsenbeck SG, et al:
Multicenter phase II study of neoadjuvant lapatinib and trastuzumab
with hormonal therapy and without chemotherapy in patients with
human epidermal growth factor receptor 2–overexpressing breast
cancer: TBCRC 006. J Clin Oncol. 31:1726–1731. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cobleigh MA, Vogel CL, Tripathy D, Robert
NJ, Scholl S, Fehrenbacher L, Wolter JM, Paton V, Shak S, Lieberman
G and Slamon DJ: Multinational study of the efficacy and safety of
humanized anti-HER2 monoclonal antibody in women who have
HER2-overexpressing metastatic breast cancer that has progressed
after chemotherapy for metastatic disease. J Clin Oncol.
17:2639–2648. 1999.PubMed/NCBI
|
|
29
|
Poovassery JS, Kang JC, Kim D, Ober RJ and
Ward ES: Antibody targeting of HER2/HER3 signaling overcomes
heregulin-induced resistance to PI3K inhibition in prostate cancer.
Int J Cancer. 137:267–277. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rao K, Gaughan L, Robson C and McCracken
S: The role of the HER2 and HER3 in prostate cancer and their
potential as therapeutic targets. Eur J Cancer. 61:S177–S178. 2016.
View Article : Google Scholar
|
|
31
|
Baek KH, Hong ME, Jung YY, Lee CH, Lee TJ,
Park ES, Kim MK, Yoo JH and Lee SW: Correlation of AR, EGFR, and
HER2 expression levels in prostate cancer: Immunohistochemical
analysis and chromogenic in situ hybridization. Cancer Res Treat.
44:50–56. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Reese DM, Small EJ, Magrane G, Waldman FM,
Chew K and Sudilovsky D: HER2 protein expression and gene
amplification in androgen-independent prostate cancer. Am J Clin
Pathol. 116:234–239. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yan M, Schwaederle M, Arguello D, Millis
SZ, Gatalica Z and Kurzrock R: HER2 expression status in diverse
cancers: Review of results from 37,992 patients. Cancer Metastasis
Rev. 34:157–164. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yamanaka Y, Friess H, Kobrin MS, Büchler
M, Kunz J, Beger HG and Korc M: Overexpression of HER2/neu oncogene
in human pancreatic carcinoma. Hum Pathol. 24:1127–1134. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nuciforo PG, Pellegrini C, Fasani R,
Maggioni M, Coggi G, Parafioriti A and Bosari S: Molecular and
immunohistochemical analysis of HER2/neu oncogene in synovial
sarcoma. Hum Pathol. 34:639–645. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Salmaninejad A, Estiar MA, Gill RK, Shih
JH, Hewitt S, Jeon HS, Fukuoka J, Shilo K, Shakoori A and Jen J:
Expression analysis of p16, c-Myc, and mSin3A in non-small cell
lung cancer by computer aided scoring and analysis (CASA). Clin
Lab. 61:549–559. 2015.PubMed/NCBI
|
|
37
|
Hanna WM, Rüschoff J, Bilous M, Coudry RA,
Dowsett M, Osamura RY, Penault-Llorca F, van de Vijver M and Viale
G: HER2 in situ hybridization in breast cancer: clinical
implications of polysomy 17 and genetic heterogeneity. Mod Pathol.
27:4–18. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Bar-Shira A, Pinthus JH, Rozovsky U,
Goldstein M, Sellers WR, Yaron Y, Eshhar Z and Orr-Urtreger A:
Multiple genes in human 20q13 chromosomal region are involved in an
advanced prostate cancer xenograft. Cancer Res. 62:6803–6807.
2002.PubMed/NCBI
|
|
39
|
Sattler HP, Lensch R, Rohde V, Zimmer E,
Meese E, Bonkhoff H, Retz M, Zwergel T, Bex A, Stoeckle M and
Wullich B: Novel amplification unit at chromosome 3q25-q27 in human
prostate cancer. Prostate. 45:207–215. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Elo JP and Visakorpi T: Molecular genetics
of prostate cancer. Ann Med. 33:130–141. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Edwards J, Mukherjee R, Munro AF, Wells
AC, Almushatat A and Bartlett JM: HER2 and COX2 expression in human
prostate cancer. Eur J Cancer. 40:50–55. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Edwards J, Krishna NS, Witton CJ and
Bartlett JM: Gene amplifications associated with the development of
hormone-resistant prostate cancer. Clin Cancer Res. 9:5271–2581.
2003.PubMed/NCBI
|
|
43
|
Nupponen NN, Kakkola L, Koivisto P and
Visakorpi T: Genetic alterations in hormone-refractory recurrent
prostate carcinomas. Am J Pathol. 153:141–148. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Lass U, Hartmann C, Capper D, Herold-Mende
C, von Deimling A, Meiboom M and Mueller W: Chromogenic in situ
hybridization is a reliable alternative to fluorescence in situ
hybridization for diagnostic testing of 1p and 19q loss in
paraffin-embedded gliomas. Brain Pathol. 23:311–318. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhang Y, Perez T, Blondin B, Du J, Liu P,
Escarzaga D, et al: Identification of FISH biomarkers to detect
chromosome abnormalities associated with prostate adenocarcinoma in
tumour and field effect environment. BMC Cancer. 14:1292014.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Arnould L, Denoux Y, MacGrogan G,
Penault-Llorca F, Fiche M, Treilleux I, Mathieu MC, Vincent-Salomon
A, Vilain MO and Couturier J: Agreement between chromogenic in situ
hybridisation (CISH) and FISH in the determination of HER2 status
in breast cancer. Br J Cancer. 88:1587–1591. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Brimo F, Montironi R, Egevad L,
Erbersdobler A, Lin DW, Nelson JB, Rubin MA, van der Kwast T, Amin
M and Epstein JI: Contemporary grading for prostate cancer:
Implications for patient care. Eur Urol. 63:892–901. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Heidenreich A, Bastian PJ, Bellmunt J,
Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T,
Zattoni F and Mottet N: European Association of Urology: EAU
guidelines on prostate cancer. Part 1: Screening, diagnosis, and
local treatment with curative intent - update 2013. Eur Urol.
65:124–137. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Tanner M, Gancberg D, Di Leo A, Larsimont
D, Rouas G, Piccart MJ and Isola J: Chromogenic in situ
hybridization: A practical alternative for fluorescence in situ
hybridization to detect HER-2/neu oncogene amplification in
archival breast cancer samples. Am J Pathol. 157:1467–1472. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Lennartz M, Minner S, Brasch S, Wittmann
H, Paterna L, Angermeier K, Öztürk E, Shihada R, Ruge M, Kluth M,
et al: The combination of DNA ploidy status and PTEN/6q15 deletions
provides strong and independent prognostic information in prostate
cancer. Clin Cancer Res. 22:2802–2811. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Di Lorenzo G, Tortora G, D'Armiento FP, De
Rosa G, Staibano S, Autorino R, D'Armiento M, De Laurentiis M, De
Placido S, Catalano G, et al: Expression of epidermal growth factor
receptor correlates with disease relapse and progression to
androgen-independence in human prostate cancer. Clin Cancer Res.
8:3438–3444. 2002.PubMed/NCBI
|
|
52
|
Neto AS, Tobias-Machado M, Wroclawski ML,
Fonseca FL, Teixeira GK, Amarante RD, Wroclawski ER and Del Giglio
A: Her-2/neu expression in prostate adenocarcinoma: A systematic
review and meta-analysis. J Urol. 184:842–850. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Qi M, Yang X, Zhang F, Lin T, Sun X, Li Y,
Yuan H, Ren Y, Zhang J, Qin X and Han B: ERG rearrangement is
associated with prostate cancer-related death in Chinese prostate
cancer patients. PLoS One. 9:e849592014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Ross JS, Sheehan C, Hayner-Buchan AM,
Ambros RA, Kallakury BV, Kaufman R, Fisher HA and Muraca PJ:
HER-2/neu gene amplification status in prostate cancer by
fluorescence in situ hybridization. Hum Pathol. 28:827–833. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Valtorta E, Misale S, Sartore-Bianchi A,
Nagtegaal ID, Paraf F, Lauricella C, Dimartino V, Hobor S, Jacobs
B, Ercolani C, et al: KRAS gene amplification in colorectal cancer
and impact on response to EGFR-targeted therapy. Int J Cancer.
133:1259–1265. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Park YS, Hwang HS, Park HJ, Ryu M-H, Chang
H-M, Yook JH, Kim BS, Jang SJ and Kang YK: Comprehensive analysis
of HER2 expression and gene amplification in gastric cancers using
immunohistochemistry and in situ hybridization: Which scoring
system should we use? Hum Pathol. 43:413–422. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Jacquemier J, Spyratos F, Esterni B,
Mozziconacci M-J, Antoine M, Arnould L, Lizard S, Bertheau P,
Lehmann-Che J, Fournier CB, et al: SISH/CISH or qPCR as alternative
techniques to FISH for determination of HER2 amplification status
on breast tumors core needle biopsies: A multicenter experience
based on 840 cases. BMC Cancer. 13:3512013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Horii R, Matsuura M, Iwase T, Ito Y and
Akiyama F: Comparison of dual-color in-situ hybridization and
fluorescence in-situ hybridization in HER2 gene amplification in
breast cancer. Breast Cancer. 21:598–604. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Rosa FE, Santos RM, Rogatto SR and
Domingues MA: Chromogenic in situ hybridization compared with other
approaches to evaluate HER2/neu status in breast carcinomas. Braz J
Med Biol Res. 46:207–216. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Kiyose S, Igarashi H, Nagura K, Kamo T,
Kawane K, Mori H, Ozawa T, Maeda M, Konno K, Hoshino H, et al:
Chromogenic in situ hybridization (CISH) to detect HER2 gene
amplification in breast and gastric cancer: comparison with
immunohistochemistry (IHC) and fluorescence in situ hybridization
(FISH). Pathol Int. 62:728–734. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Liu HL, Gandour-Edwards R, Lara PN Jr, de
Vere White R and LaSalle JM: Detection of low level HER-2/neu gene
amplification in prostate cancer by fluorescence in situ
hybridization. Cancer J. 7:395–403. 2001.PubMed/NCBI
|
|
62
|
Ross JS, Sheehan CE, Hayner-Buchan AM,
Ambros RA, Kallakury BV, Kaufman RP Jr, Fisher HA, Rifkin MD and
Muraca PJ: Prognostic significance of HER-2/neu gene amplification
status by fluorescence in situ hybridization of prostate carcinoma.
Cancer. 79:2162–2170. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Sadasivan R, Morgan R, Jennings S,
Austenfeld M, Van Veldhuizen P, Stephens R and Noble M:
Overexpression of Her-2/neu may be an indicator of poor prognosis
in prostate cancer. J Urol. 150:126–131. 1993.PubMed/NCBI
|
|
64
|
Mark HF, Feldman D, Das S, Kye H, Mark S,
Sun CL and Samy M: Fluorescence in situ hybridization study of
HER-2/neu oncogene amplification in prostate cancer. Exp Mol
Pathol. 66:170–178. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Murphy AJ, Hughes CA, Barrett C, Magee H,
Loftus B, O'Leary JJ and Sheils O: Low-level TOP2A amplification in
prostate cancer is associated with HER2 duplication, androgen
resistance, and decreased survival. Cancer Res. 67:2893–2898. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Savinainen KJ, Saramäki OR, Linja MJ,
Bratt O, Tammela TL, Isola JJ and Visakorpi T: Expression and gene
copy number analysis of ERBB2 oncogene in prostate cancer. Am J
Pathol. 160:339–345. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Loring P, Cummins R, O'Grady A and Kay EW:
HER2 positivity in breast carcinoma: A comparison of chromogenic in
situ hybridization with fluorescence in situ hybridization in
tissue microarrays, with targeted evaluation of intratumoral
heterogeneity by in situ hybridization. Appl Immunohistochem Mol
Morphol. 13:194–200. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
van de Vijver M, Bilous M, Hanna W,
Hofmann M, Kristel P, Penault-Llorca F and Rüschoff J: Chromogenic
in situ hybridisation for the assessment of HER2 status in breast
cancer: An international validation ring study. Breast Cancer Res.
9:R682007. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Elliott K, Hamilton PW and Maxwell P:
Fluorescence (FISH) and chromogenic (CISH) in situ hybridisation in
prostate carcinoma cell lines: Comparison and use of virtual
microscopy. Br J Biomed Sci. 65:167–171. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Penault-Llorca F, Bilous M, Dowsett M,
Hanna W, Osamura RY, Rüschoff J and van de Vijver M: Emerging
technologies for assessing HER2 amplification. Am J Clin Pathol.
132:539–548. 2009. View Article : Google Scholar : PubMed/NCBI
|