Introduction
Chondrosarcoma (CS) is a neoplasm of mesenchymal
origin that forms cartilage-pattern tumors of the bone and consists
of different histological subtypes (1).
This tumor is considered to be resistant to
chemotherapy and radiotherapy, and the mainstay treatment is
surgical (2,3). Several attempts have been made to
identify reliable molecular markers and therapeutic targets for CS.
However, none of these biological markers have been proven to
provide independent prognostic information (4–6).
The majority of genetic analyses performed on CS
were performed on a heterogeneous group that included all different
subtypes of CS; ploidy-analysis of CS has been described and
aneuploidy is more frequently found in high-grade CS (7,8).
There have been, to date, few studies on CS cell
lines. This may be associated with the low proliferation rates of
the tumor cells and the difficulty in reproducing an adequate
environment for CS development (9).
The centrosome is a non-membranous organelle usually
found in the periphery of the nucleus; it consists of a pair of
orthogonally arranged, barrel-shaped centrioles and numerous
different proteins that surround the pericentriolar material.
During interphase, the centrosome is responsible for organizing the
microtubule network by directing the formation of the mitotic
spindle (10). It has been
demonstrated that the centrosome amplification is linked to
chromosomal instability and the prognosis of patients with
malignant tumors (11). Centrosome
amplification has been detected in several types of malignancies
and borderline sarcomas, including osteosarcoma (7,12,13). Moskovsky et al reported that
centrosome amplification is present in benign giant cell tumors of
the bone, demonstrating that this phenomenon is not characteristic
of malignant giant cell tumors. In addition, the study showed that
centrosome amplification was prognostic for clinical behavior
(14).
The present study aimed to characterize centrosome
amplification in CS using cryopreserved tissue samples and tissue
cultures.
Materials and methods
Tumor samples
The study was conducted with cryopreserved CS tumor
tissue samples from 10 patients treated surgically in the Barretos
Cancer Hospital (Barretos, Brazil). Additionally, samples were used
from the cultures of tumors from 3 patients who underwent surgery
in the Department of Orthopedics at the Barretos Cancer Hospital.
The study was approved by the Institutional Ethical Committee of
the Barretos Cancer Hospital.
Establishment of primary cultures
In this study, centrosome amplification was
evaluated in CS using cryopreserved tissues and primary cell
cultures. A commercial culture of normal fibroblasts, lineage
CCD-1059 SK, was used as a control (Thermo Fisher Scientific Inc.,
Waltham, MA, USA). The cells from the tumor samples were cultured
for 7–25 days in an incubator with a humidified atmosphere
containing 5% CO2 at 37°C, standing for ~7 days until
confluence, prior to cytogenetic and morphological evaluation
(Fig. 1).
Tumors were reviewed by a pathologist and graded and
staged according to World Health Organization classification
(1). Primary tumor specimens were
finely minced, treated with trypsin and cultured in Dulbecco's
modified Eagle's medium (Thermo Fisher Scientific Inc.)
supplemented with 10% fetal bovine serum (Thermo Fisher Scientific
Inc.) and 1% antibiotics.
Analysis of centrosome
amplification
Immunohistochemistry/immunocytochemistry
The cells were cultured on coverslips for 3–4 days,
washed with phosphate-buffered saline, fixed with 4%
paraformaldehyde and then permeabilized with Triton-X100. An
UltraVision Plus detection system (Thermo Fisher Scientific Inc.)
was used for centrosome immunostaining and analysis.
The cells were incubated overnight with mouse
monoclonal anti-γ-tubulin (1:2,000 dilution; Sigma-Aldrich, St.
Louis, MO, USA) and blocked with Ultra-V-Block (Thermo Fisher
Scientific Inc.). All incubations were performed at 31°C with
primary antibodies for 30 min, and thereafter with the biotinylated
secondary antibody (Thermo Fisher Scientific Inc.) for 60 min.
After 3,3′-diaminobenzidine exposure, the slides were subsequently
stained with hematoxylin.
To determine centrosome numbers, the cells were
subjected to immunostaining using a mouse monoclonal anti-γ-tubulin
antibody (Sigma-Aldrich), as described previously (15).
Statistical analysis
The Lin coefficient of concordance (MedCalc Version
11.1.1.0; MedCalc Software bvba, Ostend, Belgium) was used,
considering a 95% confidence interval, as it is a test that
combines a measure of accuracy (Pearson correlation coefficient;
MedCalc Version 11.1.1.0) with another measure of accuracy (Cb) to
determine how the observed data deviate from the line of identity
(i.e., 45° line), with variance based on to the distance of the
data to the line (the accuracy of the data), and on the dispersion
of the data around the line (data accuracy). Given the number of
categories observed in the total score, the Lin concordance
coefficient was also adopted to assess the degree of agreement
between the two observers. For this coefficient, excellent
agreement was defined as a value >0.900, a suitable value ranged
from 0.600–0.900 and an unsatisfactory value was <0.600.
Results
Primary cultures
Cultures from the tumor samples of 3 patients who
underwent surgery in 2012 in Barretos Cancer Hospital were
analyzed. The clinical data are summarized in Table I. Centrosome amplification was
detected in the normal fibroblasts, with 5% of cells exhibiting
increased numbers of centrosomes.
 | Table I.Clinical data of patients with sarcoma
who underwent surgery in the Department of Orthopedics at the
Barretos Cancer hospital. |
Table I.
Clinical data of patients with sarcoma
who underwent surgery in the Department of Orthopedics at the
Barretos Cancer hospital.
| Case | Gender/age,
yearsa | Location | Ch/Rdb | Pathology | Recurrence |
|---|
| 1 | F/35 | Left humerus | Yes/no | CS-Ollier's syndrome
grade III | Yes |
| 2 | F/50 | Left distal
femur | No/no | CS grade I | No |
| 3 | M/42 | Left shoulder and
suprascapular region | No/no | CS grade III | No |
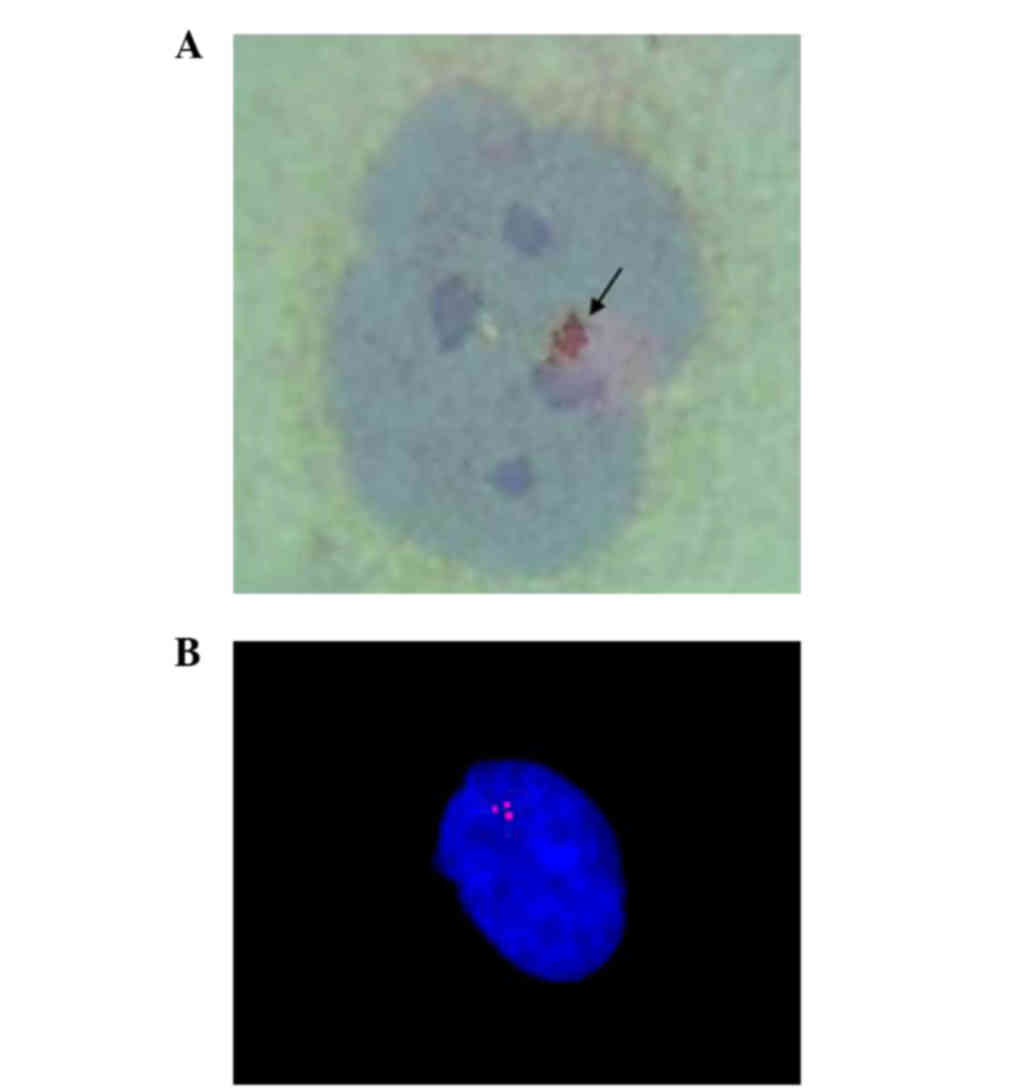
Following primary culture, to establish the
patterning process, 2 of the samples were subjected to
immunocytochemistry (Fig. 2A) and 1
samples was subjected to immunofluorescence (Fig. 2B) analysis, as indicated in Table II.
| Table II.Frequency of centrosome amplification
in primary cultures of CS. |
Table II.
Frequency of centrosome amplification
in primary cultures of CS.
|
| Presence of
centrosomes per cell (%) | Clusters (%) |
|---|
|
|
|
|
|---|
| Subtype | Normal | Amplified | 1 Cluster | 2 Clusters | 3 Clusters |
|---|
| CS-Ollier's syndrome
grade III | 36 | 64 | 15 | 2 | 0 |
| CS-Ollier's syndrome
grade III (sample of recurrence) | 24 | 76 | 16 | 5 | 1 |
| CS grade I | 52 | 48 | 5 | 1 | 0 |
| CS grade III | 85 | 15 | 8 | 0 | 0 |
Centrosome amplification, assessed using the
immunocytochemistry technique (Fig.
2A), was observed in 64% of grade III CS Ollier's syndrome
cells and in 76% of cells from the recurrence in the same patient
(case 1). Amplification occurred in 48% of the grade I cells (case
2). Using the fluorescence technique, amplification was observed in
15% of the grade III CS cells (case 3).
Cluster formation was also observed in the cultures.
In case 1, one cluster occurred in 15% of the cells and two
clusters occurred in 2%. In the recurrence, 16% of cells exhibited
one cluster, 5% exhibited two clusters and 1% exhibited three
clusters. In grade I CS, one cluster was observed in 5% of nuclei
and two clusters were observed in 1% of nuclei. As observed using
the immunofluorescence technique, 8% of cells in the grade III CS
(case 4) exhibited one cluster.
A commercial culture of normal fibroblasts (CCD-1059
SK lineage) was also established that served as a negative control;
the amplification of centrosomes was observed in 5% of the control
cells, as observed using immunocytochemistry.
Cryopreserved tissue
A total of 10 samples of cryopreserved CS tumor
tissue samples stored in the tumor bank were selected. The clinical
data of the 10 patients who provided these samples are summarized
in Table III.
| Table III.Main clinical data of the
cryopreserved tissue using immunohistochemistry. |
Table III.
Main clinical data of the
cryopreserved tissue using immunohistochemistry.
| Case | Gender/age,
years | Follow-up time,
months | Location | Pathology | Metastasis | Surgical type | Functional status of
the member | Last information |
|---|
| 1 | M/65 | 29.31 | Pelvis | Classical grade I,
primary | Yes, after
diagnosis | Simple resection | With limitation | Succumbed to
cancer |
| 2 | F/56 | 65.08 | Chest | Classical grade I,
primary | No | Simple resection | Not applicable | Alive without
disease |
| 3 | F/21 | 9.66 | Pelvis | Classical grade II,
primary | Yes, at
diagnosis | Not operated | Unknown | Alive without
disease |
| 4 | F/41 | 39.39 | Lower limb | Myxoid grade I,
primary | Yes, at
diagnosis | Amputated | Amputated | Alive without
disease |
| 5 | F/52 | 65.41 | Pelvis | Myxoid grade I,
primary | No | Simple resection | Functional | Alive without
disease |
| 6 | F/46 | 38.44 | Shoulder girdle | Classical grade II,
secondary | No | Simple resection | Functional | Alive without
disease |
| 7 | M/27 | 42.25 | Upper limb | Classical grade I,
secondary | No | Amputated | Amputated | Alive without
disease |
| 8 | F/37 | 30.46 | Lower limb | Classical grade II,
secondary | No | Resection and
prosthesis | With limitation | Alive without
disease |
| 9 | F/25 | 1.05 | Shoulder girdle | Classical grade I,
secondary | No | Simple resection | Functional | Alive without
disease |
| 10 | M/42 | 17.74 | Shoulder
girdle | Classical grade
III, primary | Yes, at
diagnosis | Amputated | Amputated | Alive without
disease |
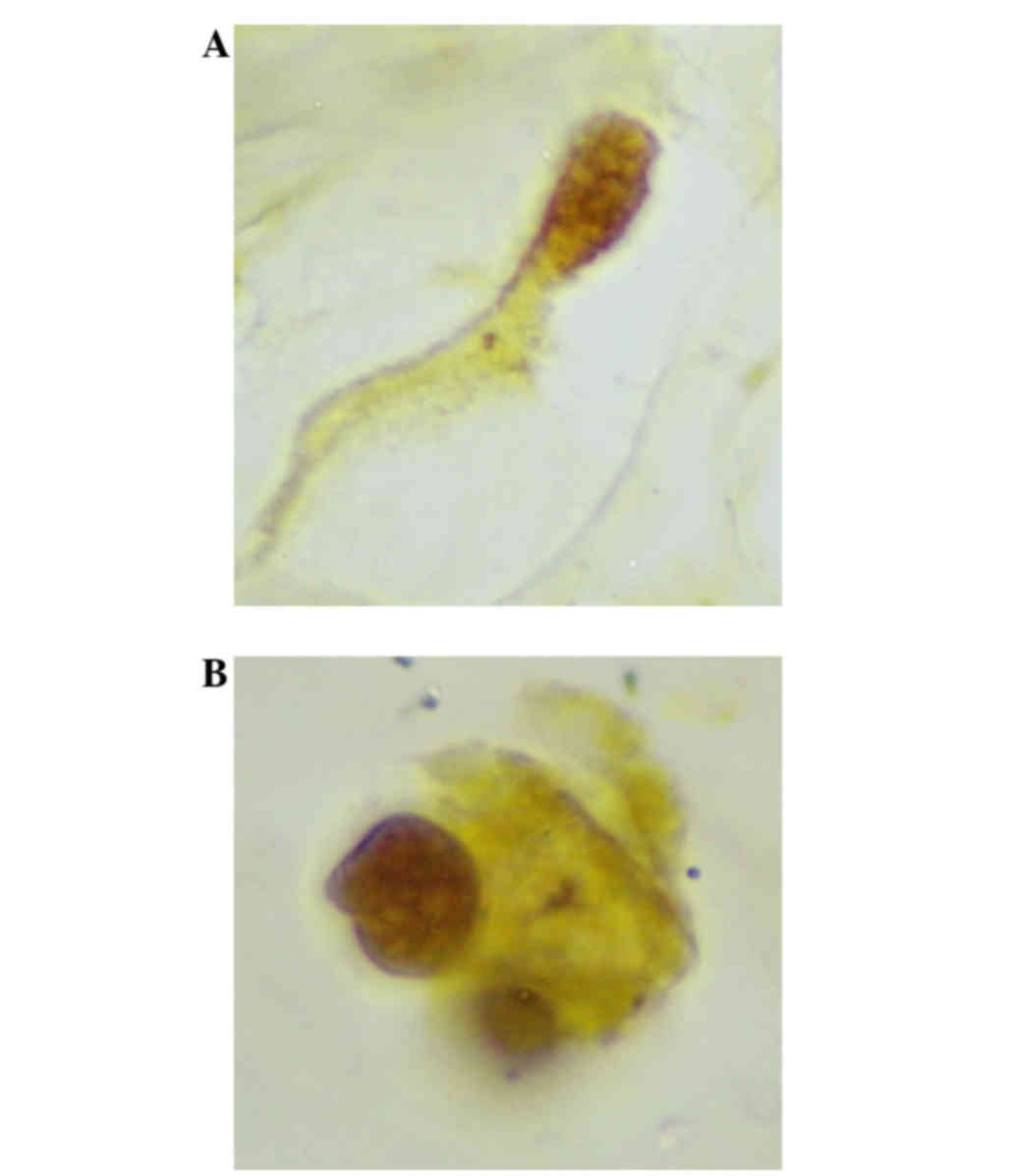
Centrosome amplification
The centrosomes were analyzed using an optical
microscope (×1,000 magnification). Two independent observers
analyzed each sample and counted the cells stained with γ-tubulin,
verifying the percentage of affected cells (Fig. 3).
The results are shown in Table IV. Analyst A found the percentage of
cells with amplifications ranged between 4 and 19% (mean, 14%),
while analyst B found that the percentage of cells with
amplification ranged between 7 and 22% (mean, 14%).
| Table IV.Frequency of centrosome amplification
and the frequency of clusters in 10 cryopreserved chondrosarcoma
tissues (analysis conducted by two independent observers). |
Table IV.
Frequency of centrosome amplification
and the frequency of clusters in 10 cryopreserved chondrosarcoma
tissues (analysis conducted by two independent observers).
|
| Percentage
frequency of centrosome amplification | Number of clusters
of centrosomes |
|---|
|
|
|
|
|---|
| Case | Analyst A (%) | Analyst B (%) | Analyst A | Analyst B |
|---|
| 1 | 18.0 | 22.0 | 0 | 0 |
| 2 | 21.0 | 20.0 | 3 | 6 |
| 3 | 13.9 |
6.9 | 1 | 1 |
| 4 |
9.3 |
9.3 | 0 | 0 |
| 5 | 19.0 | 20.0 | 1 | 1 |
| 6 | 17.0 | 13.0 | 2 | 1 |
| 7 | 10.0 | 10.0 | 0 | 0 |
| 8 | 16.0 | 13.0 | 0 | 0 |
| 9 | 14.0 | 11.0 | 0 | 0 |
| 10 |
4.0 | 10.0 | 1 | 1 |
With regard to the formation of clusters, analyst A
found 0–3 clusters per slide (mean, 0.8 clusters) and analyst B
found between 0 and 6 clusters (mean, 1 cluster).
Data analysis
For the 10 cases evaluated, the data were analyzed
using the Lin concordance coefficient. With regard to the
percentage of cells with amplification, the estimates ranged from
0.2205–0.9211 with 95% confidence. The concordance correlation
coefficient was 0.7213.
With regard to the number of clusters, the data were
analyzed using the Lin concordance coefficient, and with 95%
confidence, it is estimated that the range was from 0.4948–0.8861.
The concordance correlation coefficient was 0.7500.
Discussion
The data in the present study revealed that the CS
genetic profile adopts several alterations associated with
centrosome amplification, as previously supposed (10–12). The
present study describes arguments in favor of the premise that
centrosome amplification is a critical biological event for the
development of this malignancy. The study of centrosome alterations
is multifaceted and time consuming, and accordingly requires
appropriate expertise of the professionals involved and tests to
evaluate the results. The technical procedures to maintain primary
cultures of cancer offer varying degrees of difficulty and so the
results are not always satisfactory. Sarcoma cultures are even more
complex and difficult to effectively conduct. Therefore, the
establishment of primary cultures of CS produces a working model
that is quite promising. In the present study, the primary cultures
of CS were prepared using samples from three cases with different
histopathological classifications: 1 grade I case, 1 grade III case
and 1 grade III case with CS recurrence.
In general, the findings demonstrated that in the
cases of primary cultures stained with the immunocytochemistry
technique using fluorescent development, the assessment of
centrosomes was clear, without any ill-defined images. The
amplified centrosomes were positively demonstrated in all cases
when compared with normal fibroblasts, with demonstrated
percentages of amplified centrosomes ranging from 15–64%. Notably,
even the grade I CS showed amplified centrosomes, implying that the
amplification of centrosomes can be hypothesized as a precursor to
malignant transformation. A sample of recurrent tumor revealed
amplified centrosomes, as was previously observed in the primary CS
sample of the same patient, but with an increased number of
malignant cells with more than two centrosomes. Another case
exhibited a low rate of centrosome amplification, showing only 15%
of cells with amplification. This finding is not unexpected, as
centrosome amplification in bone and soft tissue tumors has been
observed in tumors classified as benign or with local
aggressiveness (as in giant cell tumors) or even in malignant bone
tumors such as osteosarcoma (14).
Analysis of the cryopreserved tissues showed
amplification percentages ranging from 4–19% (mean, 14%), which is
lower compared with the primary culture. This difference may be due
to the quality of the sample, and the fact that the primary culture
tended to be the most similar to the tumor in vivo. The
presence of centrosome amplification can also be represented by the
formation of clustering, but the mechanism is not fully understood.
Abnormalities in centrosome organization are under investigation in
oncology settings and the findings have been observed in in
vivo samples and cultured cells (12). In the present study, 2 cases showed
single clusters occurring in 15 and 16% of the cells, respectively,
compared with the normal fibroblasts, which showed a maximum of 3%.
However, a reduced number of clusters was also observed in CS, with
1 case exhibiting 5% of malignant cells with one cluster and 1% of
malignant cells with two clusters. The remaining case showed only
8% of malignant cells with one cluster each. This significant
variation in centrosome clusters suggests that cluster formation is
not a pivotal phenomenon for CS behavior. Setoguchi et al
observed similar findings in sarcomas of dogs (16). Different types of sarcomas have shown
hyperamplification of centrosomes associated with chromosome
instability, which was credited as a novel tumor marker (12).
In this study, cryopreserved tissues in the
percentages of clusters were smaller than those found in culture,
ranging from 1 to 6% of cells with clusters. This difference may be
occurring due to the characteristic of the sample; the cell culture
would be the closest representation of the tumor in vivo.
Another fact that was found is that the clusters found in the
cryopreserved tissues were smaller than those in the cell
cultures.
Centrosome amplification may predict the aggressive
behavior of tumors, and other findings in the literature have
associated this process with an alteration of centrosomes, with
chromosomal instabilities found in other bone tumors such as
osteosarcoma, as anticipated (12).
The present results support these premises and concur that
centrosome amplification is widely found in CS and likely
represents a major mechanism underlying the generation of
multipolar mitoses, chromosome instabilities and aneuploidy.
References
|
1
|
Fletcher CDM, Bridge JA, Hogendoorn PCW
and Mertens F: World Health Organization Classification of Tumours:
Pathology and Genetics of Tumors of Soft Tissue and Bone. IARC
Press; Lyon: 2002
|
|
2
|
Heck RKJ: Malignant tumors of the bone.
Campbells Orthopedic Surgery. 827–858. 2006.(In Portuguese).
|
|
3
|
Própero D: Producers neoplasms of
cartilaginous tissue. Bone Tumors. ROCA; São Paulo, Brazil: pp.
45–91. 2001, (In Portuguese).
|
|
4
|
Chow WA: Update on chondrosarcoma. Curr
Opin Oncol. 19:371–376. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jamil N, Howie S and Salter DM:
Therapeutic molecular target in human chondrosarcoma. Int J Exp
Pathol. 91:387–393. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Onishi AC, Hincker A and Lee FY:
Surmounting chemoterapy and radioresistance in chondrosarcoma:
Molecular mechanisms and therapeutic targets. Sarcoma.
2011:3815642010.PubMed/NCBI
|
|
7
|
Gisselsson D, Pålsson E, Yu C, Mertens F
and Mandahl N: Mitotic instability associated with late genomic
changes in bone and soft tissue tumors. Cancer Lett. 206:69–76.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim MJ, Cho KJ, Ayala AG and Ro JY:
Chondrosarcoma: With updates on molecular genetics. Sarcoma.
2011:4054372011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Monderer D, Luseau A, Bellec A, et al: New
chondrossarcoma cell lines and mouse models to study the link
between chondrogenesis and chemoresistence. Lab Invest. 1100–1114.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fukasawa K: Aberrante activation of cell
cycle reguators, centrossome amplification, and mitotic defects.
Horm Cancer. 2:104–112. 2010. View Article : Google Scholar
|
|
11
|
Chan JY: A clinical overview of
centrossome amplication in human cancers. Int J Biol Sci.
7:1122–1144. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Al-Romaih K, Bayani J, Vorobyova J, et al:
Chromosomal instability in osteosarcoma and its association with
centrosome abnormalities. Cancer Genet Cytogenet. 144:91–99. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Perucca-Lostanlen DRP, Grosgeorge J,
Marcie S, Gaudray P and Turccarrel C: Distinct MDM2 and PI4ARF
expression and centrosome amplification in well-differentiated
liposarcomas. Genes Chrom Canc. 39:99–109. 2004. View Article : Google Scholar
|
|
14
|
Moskovszky L, Dezsö K, Athanasou N,
Szendröi M, Kopper L, Kliskey K, Picci P and Sápi Z: Centrossome
abnormalities in giant cell tumour of bone: Possible association
with chromosomal instability. Mod Pathol. 23:359–366. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yamamoto Y, Misumi T, Eguchi S, et al:
Centrosome amplification as a putative prognostic biomarker for the
classification of urothelial carcinomas. Hum Pathol,. 42:1923–1930.
2011. View Article : Google Scholar
|
|
16
|
Setoguchi A, Okuda M, Nishida E, et al:
Results of hyperamplification of centrosomes in naturally
developing tumors of dogs. Am J Vet Res. 62:1134–1141. 2001.
View Article : Google Scholar : PubMed/NCBI
|