Introduction
Hepatocellular carcinoma (HCC) is a common malignant
tumor, with high morbidity and mortality, which affects patients
worldwide. Approximately 564,000 novel cases of HCC are diagnosed
each year (1,2). HCC is particularly common in Asia due to
a high prevalence of chronic hepatitis B virus (HBV) and hepatitis
C virus (HCV) infections. In China, HCC has been the second-leading
cause of cancer-associated mortalities since the 1990s (3). The majority of HCC patients in China
(~80%) have co-morbid cirrhosis associated with chronic HBV
infection (4,5). The paucity of methods for the early
diagnosis of HCC results in a high mortality rate (6–9). The mean
5-year survival rate of advanced liver cancer is 3–5% (10,11).
Although a combination of α-fetoprotein (AFP) assays with
ultrasound examination is used for early diagnosis of liver cancer,
only one-third of patients are accurately diagnosed and treated at
an early stage of the disease (7).
Accordingly, identifying more effective alternative methods for the
early diagnosis of hepatocellular carcinoma in patients with
HBV-associated liver cirrhosis is imperative.
HCC with HBV-associated liver cirrhosis is usually
diagnosed through a combination of patient medical history,
physical examination, imaging (ultrasound, MRI or CT scans showing
a liver mass consistent with HCC), and optionally, elevated serum
AFP level (>400 ng/ml). A suspicious lesion on the sonogram
generally requires additional imaging studies to confirm the stage
of the tumor, while their sensitivity in detecting small nodules
may be low. The addition of arterial phase imaging to conventional
CT scanning increases the number of tumor nodules detected, but in
nodular cirrhotic livers, detecting HCC is more challenging. While
the overall sensitivity of MRI is similar to that of triphasic CT
scans, in patients with nodular cirrhotic livers MRI has better
sensitivity and specificity. Confirmation of the diagnosis is made
by fine needle aspiration or biopsy. Elevation of AFP >400 ng/ml
can be used instead of fine needle cytology for diagnosis of HCC in
patients with liver cirrhosis and a focal hypervascular liver
lesion (>2 cm) in at least one imaging technique. Patients with
potentially resectable liver mass and AFP >400 ng/ml should
undergo surgery without pre-operative fine needle aspiration
cytology or biopsy. Any deterioration in liver function in a
patient with known liver cirrhosis of any etiology should raise a
suspicion of HCC. As an increasing number of cirrhotic patients
and/or HBV/HCV carriers undergo diagnostic procedures, it is likely
that, in a substantial number of patients, classical echosonography
will be the initial imaging technique that raises a suspicion of
HCC. Subsequently, the size of lesions and the presence or
otherwise of cirrhosis may affect the sequencing of tests used to
diagnose HCC. Suspect nodules <1 cm should be examined with
ultrasound at intervals of 3–6 months; nodules between 1 and 2 cm
in a cirrhotic liver should be investigated with at least two
dynamic studies (triphasic CT scan, ultrasound, or MRI with
contrast). If two techniques show a typical appearance of HCC, the
nodule should be interpreted as such; if that is not the case, the
lesion should either be biopsied when possible or be extirpated, at
the discretion of the physician. Nodules >2 cm with a typical
feature of HCC found through a dynamic imaging technique, as well
as any nodule associated with AFP concentration >400 ng/ml or
rising AFP on sequential determinations, does not require biopsy,
but should be considered as proven HCC, and appropriate treatment
should be started (12). The
Barcelona Clinic Liver Cancer (BCLC) staging system was used to
define tumor stage (12,13).
C-reactive protein (CRP) is a non-specific
acute-phase protein synthesized by the liver in response to acute
and chronic inflammation, and thus represents a molecular indicator
of inflammation, infection, trauma and tissue necrosis (14–18).
Previous studies have found that the serum CRP measurement can be
applied not only to assess the severity of liver damage and
fibrosis in cases of fatty liver and chronic HCV, but also serves
as an independent marker of poor prognosis in patients with
hepatocellular carcinoma (19–25).
Elevated CRP expression has also been detected in cancers of the
lung, ovaries, colon and prostate, as well as colorectal cancer and
HCC (26–31). Therefore, the present study proposed
that serum CRP has potential as a diagnostic and prognostic
biomarker for multiple human cancers, including HCC. However, the
usefulness of serum CRP tests in HCC and other cancers remains
unknown.
A high-sensitivity CRP (hs-CRP) assay, which gives
results in 25 min, quantifies low levels of CRP (as low as 0.04
mg/l) using laser nephelometry. This test has been applied to
detect CRP. It is not yet known, however, whether the hs-CRP assay
can improve diagnostic accuracy for HCC in patients with
HBV-associated liver cirrhosis. The present study evaluated whether
the hs-CRP assay can improve the diagnostic accuracy of HCC in
patients with cirrhosis associated with HBV. A total of 491
candidates were recruited and analyzed. The present findings may
assist clinicians in the earlier diagnosis of hepatocellular
carcinoma, in turn resulting in more effective and alternative
treatment modalities for patients with advanced hepatic
disease.
Materials and methods
Patients
Ethical approval for the present study was obtained
from the Ethics Committee of the General Hospital of Ningxia
Medical University (Yinchuan, China) and written informed consent
was acquired from the candidates prior to any treatment. A total of
493 cases of patients diagnosed with HBV-associated liver disease
between July 2012 and October 2014 were recruited from the
Department of Infectious Disease, General Hospital of Ningxia
Medical University, (Yinchuan, China). Patients with liver damage
due to autoimmune status, metabolism, medication or alcohol intake,
and those with acute infection, rheumatoid arthritis, gout, asthma,
chronic lung disease, myocardial infarction or stroke, any of which
could alter serum CRP levels, were excluded. Patients with portal
vein thrombosis were also excluded from the present study. None of
the included patients had been treated with any hepatoprotective,
anti-fibrotic or anti-viral drugs prior to the serum samples being
collected. All the included patients had a complete data set,
including a full medical history, HBV markers, serum HBV DNA level,
liver function, AFP level, hs-CRP assay, and magnetic resonance
imaging (MRI), computed tomography (CT) and ultrasound imagery.
Patients, including 47 healthy individuals, were classified into
four groups: Chronic HBV (CHB) group; liver cirrhosis without HCC
(LC) group; liver cirrhosis with HCC (HCC) group; and healthy
control (CN) group. The demographic and clinical/pathological data
are summarized in Table I.
 | Table I.Patient demographic and clinical
characteristics. |
Table I.
Patient demographic and clinical
characteristics.
|
| Group |
|---|
|
|
|
|---|
| Characteristic | HC | CHB | LC | HCC |
|---|
| Total, n | 47 | 137 | 169 | 187 |
| Age, mean years ±
SD |
39±12.1 |
34±10.6 |
46±10.2 |
48±10.6 |
| Gender ratio,
M:F | 39:8 | 110:27 | 131:38 | 144:43 |
| HBeAg status,
n |
|
|
|
|
| HBeAg
positive | NA | 87 | 45 | 42 |
| HBeAg
negative | NA | 50 | 124 | 145 |
| HBV
DNA, mean logIU/ml ± SD | NA | 3.26±2.25 | 2.90±2.72 | 3.35±2.71 |
| ALT,
mean IU/l ± SD | 19.80±13.17 | 131.33±181.22 | 101.78±177.24 | 53.64±66.04 |
| AFP,
mean ng/ml ± SD | 4.48±1.29 | 16.15±43.35 | 104.08±186.30 | 492.61±544.00 |
| AFP status, n |
|
|
|
|
| AFP
negative | NA | NA | 64 | 65 |
| AFP
positive |
|
| 105 | 122 |
| hs-CRP,
mean mg/l ± SD | 0.59±0.53 | 1.53±2.70 | 2.83±3.05 | 17.34±22.61 |
| Child
class (A:B:C), % | NA | NA | 47:53:69 | 52:75:60 |
| MELD
score, mean ± SD | NA | NA | 9.0±6 | 11.5±4 |
| TNM stage, n |
|
|
|
|
|
I–II | NA | NA | NA | 109 |
|
III–IV |
|
|
| 78 |
| Metastasis, n |
|
|
|
|
|
Yes | NA | NA | NA | 123 |
| No |
|
|
| 64 |
CHB was diagnosed according to the clinical practice
guidelines criteria laid down by Asian Pacific Association for the
Study of the Liver, European Association for the Study of the Liver
and American Association for the Study of Liver Diseases (32). LC diagnosis was confirmed by clinical
symptoms, diagnostic ultrasound imaging, histopathology of liver
biopsy samples, and laboratory diagnosis, including the presence of
ascites, enlargement of the caudate lobe, collateral portal-venous
anastomoses, portal hypertension, nodular liver contour,
splenomegaly and varices (11).
In total, 47 healthy volunteers, who had no history
of alcoholism, taking medications (including traditional Chinese
medicines) that could damage the liver, or autoimmune or metabolic
disorders, and whose blood chemistry was normal, acted as a control
group.
Patients currently undergoing, or with any history
of, treatment with any hepatoprotective, anti-fibrotic, or
anti-viral drugs were excluded from the present study.
Additionally, patients and healthy volunteers with conditions such
as infection, arthritis, gout, asthma, chronic lung disease,
myocardial infarction or stroke were excluded.
Measurements
Serum hs-CRP levels were assayed by Ultra ion
immuno-turbidmetric detection kit (Shanghai Changzheng Biological
Company, Shanghai, China). Serum AFP levels were analyzed with a
chemiluminescence immunoassay analyzer detection kit (Shanghai
Abbott Pharmaceutical Co., Ltd., Shanghai, China).
Immunohistochemistry (IHC)
Liver tissue samples were stained with Masson
Trichrome (ab150686; Abcam, Cambridge, UK) and examined by two
independent liver pathologists. For CRP staining, samples were cut
into 3–5 mm sections, formalin-fixed and embedded in paraffin. The
sections were then dewaxed, rehydrated, and incubated in 3%
hydrogen peroxide to quench endogenous peroxidase activity. The
samples were incubated with anti-CRP primary antibody (dilution,
1:1,000; bs-0115R; Hotgen Biotech, Beijing, China) and secondary
antibody (HRP-labeled anti-rabbit; dilution, 1:5,000; BA1003;
BosterBio, Wuhan, China) overnight at 4°C. Subsequently,
3,3′-Diaminobenzidine Substrate Chromogen System (Dako; Agilent
Technologies, Inc., Santa Clara, CA, USA) was used to detect
positive staining. Images were captured using an Olympus E520
microscope (Olympus, Tokyo, Japan). Protein expression was
semi-quantified as follows: The positive staining intensity was
scored according to the number of cells exhibiting cytoplasmic and
nuclear staining, using the following classification system: 0, no
staining; 1, nuclear staining in <10% of cells and/or weak
cytoplasmic staining; 2, nuclear staining in 10–50% of cells and/or
distinct cytoplasmic staining; and 3, nuclear staining in >50%
of cells and/or strong cytoplasmic staining. The positive staining
intensity (scale 0–3) and the percentage of positive cells (0–100%)
were determined and multiplied to produce a final score (0–300).
The same experienced pathologists analyzed the IHC data to maintain
consistency.
Statistical analysis
Statistical analyses were performed using the SPSS
v17.0 software package (SPSS Inc., Chicago, IL, USA). Quantitative
data is expressed as the mean ± standard deviation. The differences
between abnormally distributed data were compared using a Wilcoxon
rank-sum test, while means from normally distributed data were
compared using Student's t-test. A χ2 test was used to
analyze the count data, while Spearman's rank correlation
coefficient was applied to analyze correlation. The area under the
curve (AUC) was calculated using receiver operator characteristic
(ROC) curve analysis. P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline demographic and clinical
characteristics
A total of 493 cases of previously untreated
patients with HBV-associated cirrhosis were recruited into the
present study. The patients were classified into CHB (137 cases,
27.79%), LC (169 cases, 34.28%) and HCC (187 cases, 37.93%) groups.
An additional 47 healthy volunteers were recruited as an
age-matched control group (Table
I).
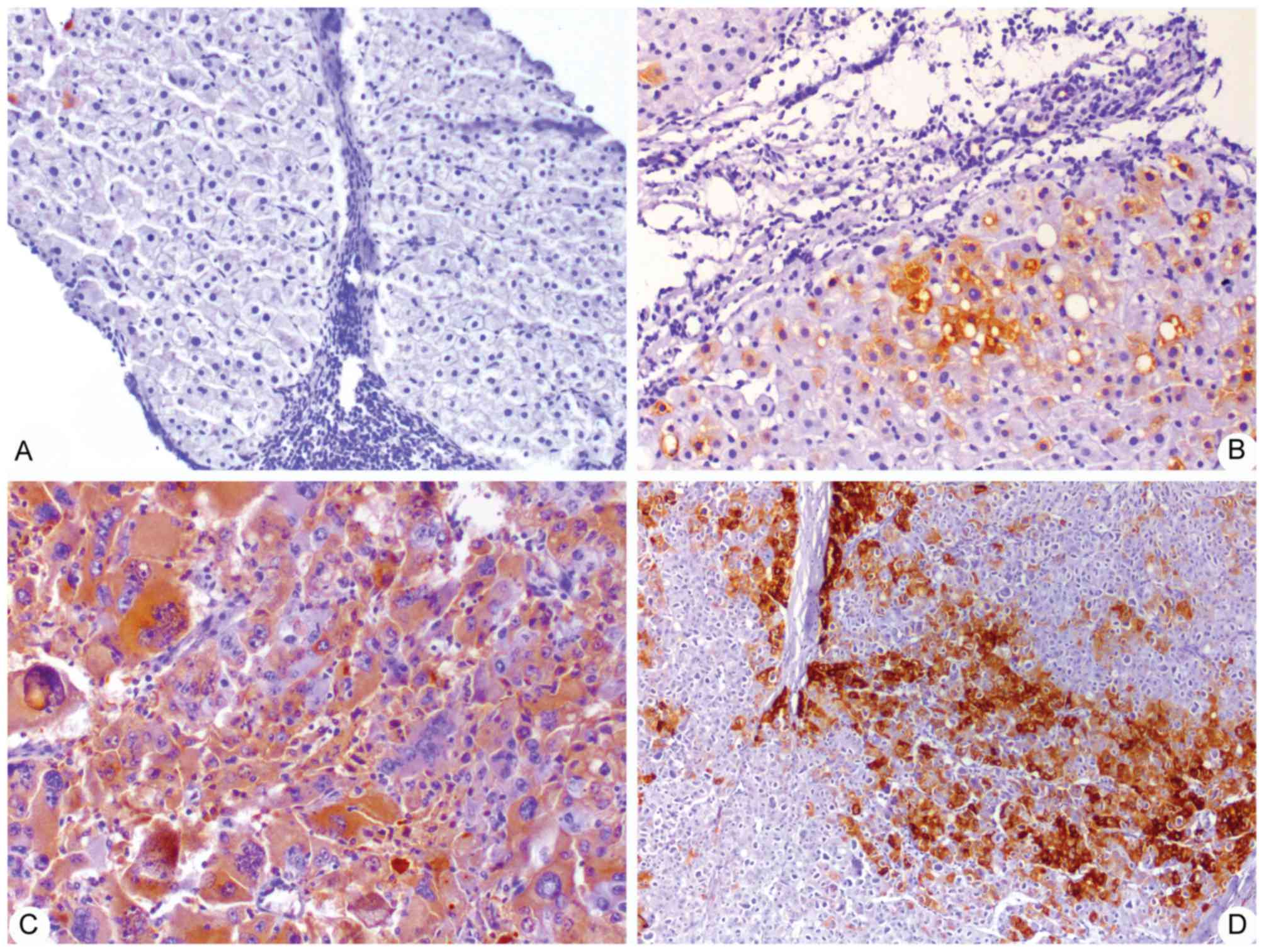
CRP expression in human tissues
To further validate CRP expression in HCC and
non-tumor liver tissues in patients, immunohistochemical analysis
was employed to detect the presence of CRP in 126 cases of
non-tumor tissue samples and 134 cases of HCC tissue samples. IHC
analysis showed that CRP is abundantly expressed in HCC tissues,
but not in non-tumor tissues. CRP-positive staining was mainly
found in parenchymal cells, but several non-parenchymal cells also
showed positive staining of CRP (Fig.
1). Staining defined as ‘negative’, ‘weak positive’, ‘moderate
positive’ and ‘strong positive’ was found in 21.43, 33.33, 25.40
and 19.18%, and 7.46, 4.48, 41.79 and 46.27% of non-tumor and HCC
tissue samples, respectively. In addition, the total positive rates
of CRP expression in non-tumor and HCC tissues samples were 78.57
and 92.54%, respectively (Table II).
Additionally, IHC scores for CRP were significantly increased in
tumor tissue samples (64.04±91.52) compared with non-tumor tissue
samples (21.40±38.72) (P<0.05; Table
II).
| Table II.CRP expression in non-tumor and HCC
tissue samples. |
Table II.
CRP expression in non-tumor and HCC
tissue samples.
|
|
| CRP staining
intensity, n (%) |
|
|
|---|
|
|
|
|
|
|
|---|
| Tissue type | n | − | + | ++ | +++ | Total positive
rate, % | CRP staining
score |
|---|
| Non-tumor | 126 | 27 (21.43) | 42 (33.33) | 32 (25.40) | 25 (19.84) | 78.57 | 21.40±38.72 |
| HCC | 134 | 10 (7.46) | 6 (4.48) | 56 (41.79) | 62 (46.27) | 92.54 | 64.04±91.52 |
Serum hs-CRP and AFP levels
Serum hs-CRP and AFP levels were found to be
significantly elevated in the HCC group compared to those in the
LC, CHB and CN groups (P<0.01). The mean levels of hs-CRP and
AFP in the HCC group (17.34±22.61 and 492.61±544.15 ng/ml) were
significantly increased with the levels in the LC (2.83±3.05 and
104.08±186.3 nm/l), CHB (1.53±2.7 and 16.15±43.35 ng/ml) and CN
(0.59±0.53 and 4.48±1.29 ng/ml) groups (P<0.05; Table I).
Correlation between serum hs-CRP level
and HCC clinical parameters
The clinical parameters of patients with HCC were
AFP, tumor Edmondson grade and tumor-node-metastasis (TNM) stage.
The differences among the groups were analyzed by χ2
test. To evaluate clinical relevance, the association between serum
hs-CRP concentration and the pathological characteristics of HCC
patients were examined. Analysis of the correlation between serum
hs-CRP level and HCC clinical parameters indicated that there was
no correlation between hs-CRP serum levels and tumor Edmondson
grade (r=0.238, P=0.229), TNM stage (r=0.159, P=0.498) or AFP
status (r=0.336, P=0.737) (Table
III).
| Table III.Correlation between serum hs-CRP
concentration and AFP status, TNM stage and tumor Edmondson grading
in hepatocellular carcinoma patients. |
Table III.
Correlation between serum hs-CRP
concentration and AFP status, TNM stage and tumor Edmondson grading
in hepatocellular carcinoma patients.
| Parameter | n | hs-CRP
concentration, mg/l | r | P-value |
|---|
| AFP status |
|
| 0.336 | 0.737 |
| AFP
negative | 65 |
15.51±22.016 |
|
| AFP
positive | 122 |
17.24±22.044 |
| TNM stage |
|
| 0.238 | 0.229 |
| I | 40 | 18.24±19.39 |
|
| II | 69 | 19.37±21.06 |
|
III | 45 | 20.40±26.37 |
| IV | 33 | 32.71±32.41 |
| Edmondson
grading |
|
| 0.159 | 0.498 |
| Early
stages (I–II) | 109 | 19.02±19.81 |
|
|
Advanced stages (III–IV) | 78 | 24.02±27.82 |
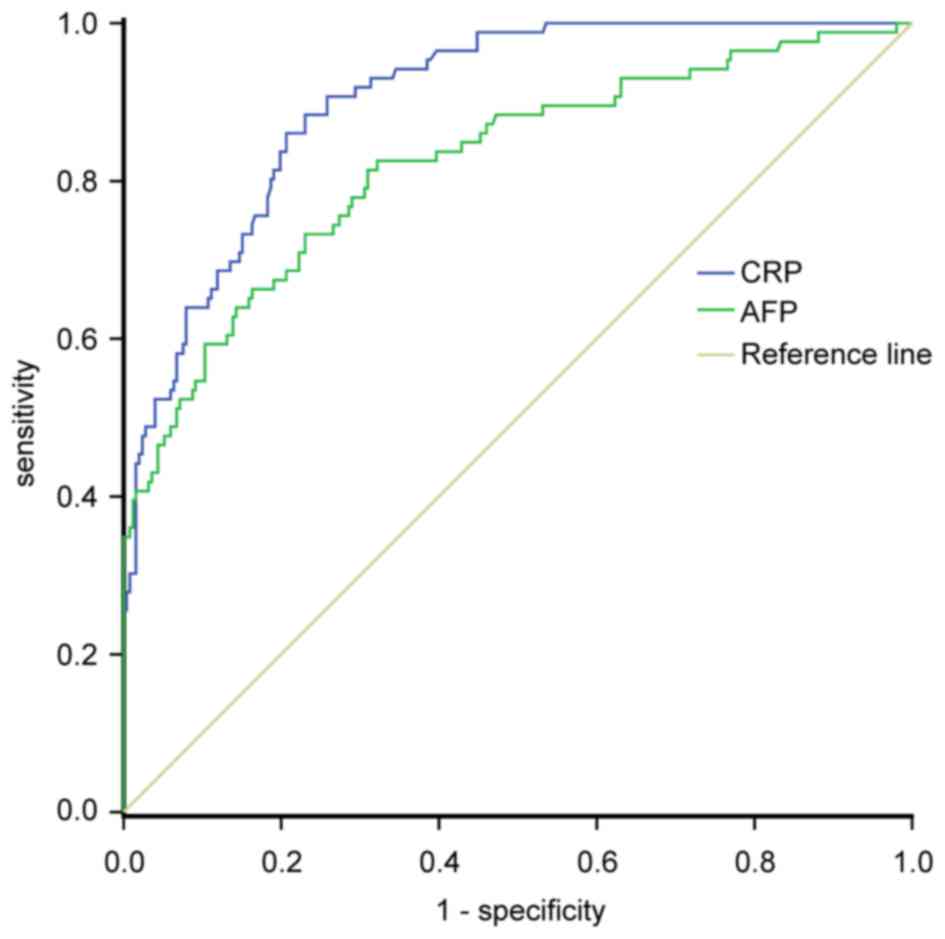
ROC curve analyses of serum hs-CRP and
AFP levels for the diagnosis of HCC
ROC curve analysis was used to clarify the optimal
cut-off value of CRP expression in the diagnosis of HCC. The ROC
curve showed that the sensitivity and specificity of serum hs-CRP
levels for the diagnosis of HCC were 84.16 and 61.59%, respectively
[95% confidence interval (CI), 0.867–0.933], while those of serum
AFP for HCC diagnosis were 74.42 and 55.63%, respectively (95% CI,
0.778–0.864). The AUC of CRP and AFP levels for HCC diagnosis were
0.903 and 0.824, respectively. The optimal cut-off levels for serum
CRP and AFP in the diagnosis of HCC were 2.17 mg/l and 20 ng/ml,
respectively (Fig. 2). ROC analysis
showed that measurement of serum hs-CRP could differentiate between
HCC and HBV-associated liver cirrhosis and increase the diagnostic
accuracy for HCC. Additionally, measurement of hs-CRP and AFP
together improved the diagnostic accuracy for HCC compared with all
controls and either test alone (Table
IV).
| Table IV.Assessment of serum hs-CRP, AFP and
CRP+AFP in the diagnosis of hepatocellular carcinoma. |
Table IV.
Assessment of serum hs-CRP, AFP and
CRP+AFP in the diagnosis of hepatocellular carcinoma.
| Parameter | AUC | Sensitivity, % | Specificity, % | PPV, % | NPV, % |
|---|
| AFP | 0.824 | 74.42 | 55.63 | 51.60 | 89.00 |
| CRP | 0.903 | 84.16 | 61.59 | 59.44 | 85.32 |
| CRP+AFP | 0.998 | 94.06 | 37.75 | 81.36 | 90.00 |
Comparison of positive rates of serum
CRP and AFP expression
In the present study, 20 ng/ml AFP and 2.17 mg/l
hs-CRP were regarded as the optimal cut-off levels. The results
showed that 161 patients (86.1%) were positive for CRP, whereas 130
patients (69.52%) were positive for AFP (187 patients;
χ2=14.881; P<0.001) (Table
V). The CRP positive rate in HCC patients was increased
compared with liver cirrhosis patients (χ2=93.761;
P<0.001) (Table IV), while the
positive rate of AFP in patients with HCC was similar to that in
patients with liver cirrhosis (χ2=2.16; P>0.01)
(Table V). The positive rate of CRP
in AFP-positive patients with liver cirrhosis was increased
compared with that in AFP-negative patients with liver cirrhosis,
while the positive rate of CRP in AFP-positive patients with HCC
was similar to that of AFP-negative patients with HCC (Table VI). Overall, these data indicate that
serum hs-CRP measurement can raise the diagnostic accuracy for
AFP-negative HCC in patients with HBV-associated liver
cirrhosis.
| Table V.Comparison between the positive rate
of serum CRP and AFP expression. |
Table V.
Comparison between the positive rate
of serum CRP and AFP expression.
| Group | n | CRP positive, n
(%) | AFP positive, n
(%) |
|---|
| HC | 47 | 0 | 0 |
| CHB | 137 | 16
(11.68) | 17
(12.41) |
| LC | 169 | 71
(42.01) | 105 (62.13) |
| HCC | 187 | 161 (86.10) | 130 (69.52) |
| Table VI.Serum hs-CRP positive rate in
AFP-negative or AFP-positive patients with liver cirrhosis and
HCC. |
Table VI.
Serum hs-CRP positive rate in
AFP-negative or AFP-positive patients with liver cirrhosis and
HCC.
| Patient group | Total, n | CRP positive,
n | CRP positive rate,
% | χ2 | P-value |
|---|
| LC | 169 |
|
| 6.422 | 0.011 |
| AFP
negative | 64 | 19 | 29.69 |
|
|
| AFP
positive | 105 | 52 | 49.52 |
| HCC | 187 |
|
| 0.183 | 0.669 |
| AFP
negative | 65 | 55 | 84.62 |
|
|
| AFP
positive | 122 | 106 | 86.89 |
|
|
Discussion
Chronic inflammation has been reported to be
involved in tumor initiation, promotion, progression, invasion, and
metastasis (33–41). HBV-associated HCC is a typical
inflammation-associated malignancy (42–44). CRP
is a sensitive acute-phase reactant and a particularly sensitive
marker of inflammation and tissue damage in the liver (37–40). At
present, several studies have described elevated CRP expression in
cancer cells and tissues, including HCC (25–31), but
whether CRP expression plays a role in the development or
progression of HBV-associated HCC remains unknown. The present
study aimed to determine whether CRP is expressed in the tissue of
HBV-associated HCC with liver cirrhosis, and whether there is any
difference in serum CRP levels between HBV-associated HCC with
liver cirrhosis, HBV-associated liver cirrhosis without HCC, CHB
patients and healthy control subjects. The present study found that
CRP is strongly expressed in HCC tissues [including AFP (−) and (+)
HCC patients], but not in non-tumor tissues. Additionally, IHC
scores for CRP were significantly increased in tumor tissue samples
compared with non-tumor tissue samples (P<0.05). It was also
observed that serum CRP levels were significantly increased in
patients with HBV-associated HCC compared with patients with
HBV-associated liver cirrhosis without HCC, CHB patients, and the
healthy control group (P<0.05). On the basis of the
aforementioned data, the present study hypothesizes that CRP plays
an important role in the development and progression of HCC, and
serum CRP level has potential as a diagnostic and prognostic
biomarker for HCC. However, earlier studies have indicated that
serum CRP measurement is not a good diagnostic marker for HCC
(21–23). It was found that serum CRP levels in
earlier studies were measured with a commercial kit by a
nephelometric method, whose lower accuracy limits its diagnostic
efficacy.
hs-CRP, an ultra-sensitive detection technology, can
accurately detect low concentrations of CRP; however, whether
hs-CRP measurement can improve diagnostic accuracy for HCC in
patients with HBV-associated liver cirrhosis remains unknown. To
further clarify the optimal cut-off value of CRP for diagnosing HCC
in patients with HBV-associated liver cirrhosis, ROC curve analysis
was performed. The results showed that the sensitivity and
specificity of serum hs-CRP for HCC diagnosis were 84.16 and
61.59%; those of serum AFP for HCC diagnosis were 74.42 and 55.63%
respectively. The areas under ROC curve of CRP and AFP were 0.903
and 0.824, respectively. The optimal cut-off levels for serum CRP
and AFP in the diagnosis of HCC were 2.17 mg/l and 20 ng/ml,
respectively. ROC analysis indicated that measurement of serum
hs-CRP could differentiate HCC from HBV-associated liver cirrhosis
and increase the diagnostic accuracy for HCC. Additionally,
measurement of hs-CRP and AFP together improved the diagnostic
accuracy for HCC compared with all controls compared with either
test alone.
Since the identification of AFP in the 1970s, AFP
has been the only serologic marker widely used in HCC diagnosis.
However, its diagnostic power has been continuously questioned and
debated. For example, elevated serum AFP was only observed in
60–70% of HCC patients, while the proportion was just 33–65% in
patients harboring HCCs <3 cm in diameter (7,8). In
addition, the non-specific elevation of serum concentrations of AFP
may be present in patients with non-malignant chronic liver
disease, such as patients with chronic HBV (15–58%) and patients
with liver cirrhosis (11–47%) (7,8,11,28,45).
Therefore, the efficacy of AFP as a biomarker for HCC diagnosis has
been questioned. The development of more effective alternative
diagnostic methods to complement AFP is urgently required to
improve clinical outcomes. In the present study, 20 ng/ml AFP and
2.17 mg/l hs-CRP were regarded as the optimal cut-off levels for
the diagnosis of HCC. The results showed that 86.1% of HCC patients
were positive for CRP, whereas 69.52% of HCC patients were positive
for AFP. The CRP positive rate in HCC patients was increased
compared with liver cirrhosis patients, while the positive rate of
AFP in patients with HCC was similar to patients with liver
cirrhosis. The positive rate of CRP in AFP-positive HCC patients
was similar to the rate in AFP-negative HCC patients. These results
indicated that serum hs-CRP measurement is able to differentiate
between HCC and HBV-associated liver cirrhosis, and the diagnostic
accuracy for AFP-negative HCC with HBV-associated liver cirrhosis
was increased. However, the association between CRP and
HBV-associated HCC is more complicated than expected. Serum AFP and
CRP are also frequently elevated in patients with chronic HBV and
HBV-associated liver cirrhosis who do not have HCC. Yang et
al (46) recently reported that
in cases where there is a delayed response in AFP levels to
entecavir in patients with elevated AFP levels, this delay acts as
an indicator of high HCC risk (46,47).
However, the clinical significance of CRP response to antiviral
treatments remains to be fully studied. Thus, the diagnostic value
of serum CRP level for HCC diagnosis requires additional
investigation.
Serum hs-CRP level may be an effective diagnostic
metric to complement AFP level in diagnosing HCC and improving the
identification of patients with AFP-negative HCC in cases of
HBV-associated liver cirrhosis. The present findings may improve
the early diagnosis of hepatocellular carcinoma, permitting more
effective and alternative treatment modalities for patients with
advanced hepatic disease.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81460301), the
Natural Science Foundation of Ningxia (grant nos. NZ09115 and
NZ11199), the Scientific and Technological Foundation of Ningxia
(grant no. NZI5134), and Chinese Foundation for Hepatitis Wang
Bao-en Liver Fibrosis Fund (grant no. xjs).
Glossary
Abbreviations
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
HBV
|
hepatitis B virus
|
|
CRP
|
C-reactive protein
|
|
CHB
|
chronic hepatitis B virus
|
References
|
1
|
El-Serag HB: Epidemiology of viral
hepatitis and hepatocellular carcinoma. Gastroenterology.
142:1264–1273.e1. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Luk JM and Liu AM: Proteomics of
hepatocellular carcinoma in Chinese patients. OMICS. 15:261–266.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tang ZY: Hepatocellular carcinoma-cause,
treatment and metastasis. World J Gastroenterol. 7:445–454. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lin CL and Kao JH: Risk stratification for
hepatitis B virus related hepatocellular carcinoma. J Gastroenterol
Hepatol. 28:10–17. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gao Y, Jiang Q, Zhou X, Ding B, Wang R,
Zhao G and Chen Y: HBV infection and familial aggregation of liver
cancer: An analysis of case-control family study. Cancer Causes
Control. 15:845–850. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fu WM, Zhang JF, Wang H, Xi ZC, Wang WM,
Zhuang P, Zhu X, Chen SC, Chan TM, Leung KS, et al: Heat shock
protein 27 mediates the effect of
1,3,5-trihydroxy-13,13-dimethyl-2H-pyran [7,6-b] xanthone on
mitochondrial apoptosis in hepatocellular carcinoma. J Proteomics.
75:4833–4843. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Patel M, Shariff MI, Ladep NG,
Thillainayagam AV, Thomas HC, Khan SA and Taylor-Robinson SD:
Hepatocellular carcinoma: Diagnostics and screening. J Eval Clin
Pract. 18:335–342. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shariff MI, Cox IJ, Gomaa AI, Khan SA,
Gedroyc W and Taylor-Robinson SD: Hepatocellular carcinoma: Current
trends in worldwide epidemiology, risk factors, diagnosis and
therapeutics. Expert Rev Gastroenterol Hepatol. 3:353–367. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Xu C, Lee SA and Chen X: RNA interference
as therapeutics for hepatocellular carcinoma. Recent Pat Anticancer
Drug Discov. 6:106–115. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Siegel R, Naishadham D and Jemal A: Cancer
Statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shen Q, Fan J, Yang XR, Tan Y, Zhao W, Xu
Y, Wang N, Niu Y, Wu Z, Zhou J, et al: Serum DKK1 as a protein
biomarker for the diagnosis of hepatocellular carcinoma: A
large-scale, multicentre study. Lancet Oncol. 13:817–826. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jelic S and Sotiropoulos GC: ESMO
Guidelines Working Group: Hepatocellular carcinoma: ESMO clinical
practice guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 21:(Suppl 5). v59–v64. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Llovet JM, Di Bisceglie AM, Bruix J,
Kramer BS, Lencioni R, Zhu AX, Sherman M, Schwartz M, Lotze M,
Talwalkar J, et al: Design and endpoints of clinical trials in
hepatocellular carcinoma. J Natl Cancer Inst. 100:698–711. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shameem M, Bhargava R, Ahmad Z, Saad T,
Fatima N and Malik A: Association between serum C-reactive protein
levels and other important predictive markers of outcome in COPD.
Acta Med Iran. 49:18–20. 2011.PubMed/NCBI
|
|
15
|
Tanrıverdi H, Tor MM, Kart L, Altın R,
Atalay F and SumbSümbüloğlu V: Prognostic value of serum
procalcitonin and C-reactive protein levels in critically ill
patients who developed ventilator-associated pneumonia. Ann Thorac
Med. 10:137–142. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Garcia-Rio F, Miravitlles M, Soriano JB,
Muñoz L, Duran-Tauleria E, Sánchez G, Sobradillo V and Ancochea J:
EPI-SCAN Steering Committee: Systemic inflammation in chronic
obstructive pulmonary disease: A population-based study. Respir
Res. 11:632010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Abd TT, Eapen DJ, Bajpai A, Goyal A,
Dollar A and Sperling L: The role of C-reactive protein as a risk
predictor of coronary atherosclerosis: Implications from the
JUPITER trial. Curr Atheroscler Rep. 13:154–161. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Peisajovich A, Marnell L, Mold C and Du
Clos TW: C reactive protein at the interface between innate
immunity and inflammation. Expert Rev Clin Immunol. 4:379–390.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lin ZY, Wang LY, Yu ML, Chen SC, Chuang
WL, Hsieh MY, Tsai JF and Chang WY: Role of serum C-reactive
protein as a marker of hepatocellular carcinoma in patients with
cirrhosis. J Gastroenterol Hepatol. 15:417–421. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fabris C, Pirisi M, Soardo G, Falleti E,
Pezzetta F, Vitulli D, Toniutto P, Bortolotti N, Gonano F and
Bartoli E: Value of serum C-reactive protein measurement in the
detection of hepatocellular carcinoma superimposed on liver
cirrhosis. J Cancer Res Clin Oncol. 120:229–232. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee FY, Lee SD, Tsai YT, Wu JC, Lai KH and
Lo KJ: Serum C-reactive protein as a serum marker for the diagnosis
of hepatocellular carcinoma. Cancer. 63:1567–1571. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Andreozzi P, Viscogliosi G, Colella F,
Subic M, Cipriani E, Marigliano B, Verrusio W, Servello A, Ettorre
E and Marigliano V: Predictors of liver fibrosis in patients with
non-alcoholic fatty liver disease. The role of metabolic syndrome,
insulin-resistance and inflammation. Recenti Prog Med. 103:570–574.
2012.(In Italian). PubMed/NCBI
|
|
23
|
Komoriya T, Inoue N, Yoshimune K, Ogawa M,
Moriyama M and Kohno H: Use of a highly sensitive latex reagent
with amino acid spacer for determination of C-reactive protein
concentration in a variety of liver diseases. J Biosci Bioeng.
114:560–563. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Atta M, Cabral M, Santos G, Paraná R and
Atta A: Inflammation biomarkers in chronic hepatitis C: Association
with liver histopathology, HCV genotype and cryoglobulinemia.
Inflamm Res. 61:1101–1106. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sjöwall C, Cardell K, Boström EA, Bokarewa
MI, Enocsson H, Ekstedt M, Lindvall L, Frydén A and Almer S: High
prevalence of autoantibodies to C-reactive protein in patients with
chronic hepatitis C infection: Association with liver fibrosis and
portal inflammation. Hum Immunol. 73:382–388. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rocha P, Morgan CJ, Templeton AJ, Pond GR,
Naik G and Sonpavde G: Prognostic impact of C-reactive protein in
metastatic prostate cancer: A systematic review and meta-analysis.
Oncol Res Treat. 37:772–776. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Shibutani M, Maeda K, Nagahara H, Ohtani
H, Sugano K, Ikeya T, Kimura K, Amano R, Kubo N, Tanaka H, et al:
Elevated preoperative serum C-reactive protein levels are
associated with poor survival in patients with colorectal cancer.
Hepatogastroenterology. 61:2236–2240. 2014.PubMed/NCBI
|
|
28
|
Chen W, Wang JB, Abnet CC, Dawsey SM, Fan
JH, Yin LY, Yin J, Taylor PR, Qiao YL and Freedman ND: Association
between C-reactive protein, incident liver cancer, and chronic
liver disease mortality in the Linxian nutrition intervention
trials: A nested case-control study. Cancer Epidemiol Biomarkers
Prev. 24:386–392. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hefler LA, Concin N, Hofstetter G, Marth
C, Mustea A, Sehouli J, Zeillinger R, Leipold H, Lass H, Grimm C,
et al: Serum C-reactive protein as independent prognostic variable
in patients with ovarian cancer. Clin Cancer Res. 14:710–714. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Xu M, Zhu M, Du Y, Yan B, Wang Q, Wang C
and Zhao J: Serum C-reactive protein and risk of lung cancer: A
case-control study. Med Oncol. 30:3192013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Nozoe T, Matsumata T, Kitamura M and
Sugimachi K: Significance of preoperative elevation of serum
C-reactive protein as an indicator for prognosis in colorectal
cancer. Am J Surg. 176:335–338. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Alberti A and Caporaso N: HBV therapy:
Guidelines and open issues. Dig Liv Dis. 43:(Suppl 1). S57–S63.
2011. View Article : Google Scholar
|
|
33
|
Balkwill F and Mantovani A: Inflammation
and cancer: Back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Okada F: Inflammation-related
carcinogenesis: Current findings in epidemiological trends, causes
and mechanisms. Yonago Acta Med. 57:65–72. 2014.PubMed/NCBI
|
|
35
|
Feng JF, Huang Y and Chen QX: A new
inflammation index is useful for patients with esophageal squamous
cell carcinoma. Onco Targets Ther. 7:1811–1815. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Nishikawa H, Arimoto A, Wakasa T, Kita R,
Kimura T and Osaki Y: Pre-treatment C-reactive protein as a
prognostic factor for recurrence after surgical resection of
hepatocellular carcinoma. Anticancer Res. 33:1181–1188.
2013.PubMed/NCBI
|
|
37
|
Zhao X, Luo J, Li B, Liu S and Li D: The
association between preoperative serum C-reactive protein and
hepatocellular carcinoma recurrence in patients with chronic
hepatitis B virus HBV infection-a retrospective study. PLoS One.
10:e01169092015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
He X, Wang Y, Zhang W, Li H, Luo R, Zhou
Y, Liao CL, Huang H, Lv X, Xie Z and He M: Screening differential
expression of serum proteins in AFP-negative HBV-related
hepatocellular carcinoma using iTRAQ-MALDI-MS/MS. Neoplasma.
61:17–26. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Imai N, Kinoshita A, Onoda H, Iwaku A,
Oishi M, Tanaka K, Fushiya N, Koike K, Nishino H and Tajiri H:
Persistent elevated C-reactive protein after treatment is an
independent marker of a poor prognosis in patients with
hepatocellular carcinoma. Clin Transl Oncol. 15:575–581. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Sieghart W, Pinter M, Hucke F, Graziadei
I, Schöniger-Hekele M, Müller C, Vogel W, Trauner M and
Peck-Radosavljevic M: Single determination of C-reactive protein at
the time of diagnosis predicts long-term outcome of patients with
hepatocellular carcinoma. Hepatology. 57:2224–2234. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Liu C, Zhang Y, Zhan J, Zhao Y, Wan Q,
Peng H and Zhu W: Interleukin-23A is associated with tumor growth
in Helicobacter-pylori-related human gastric cancer. Cancer Cell
Int. 14:1042014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Szabo G and Lippai D: Molecular hepatic
carcinogenesis: Impact of inflammation. Dig Dis. 30:243–248. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Morales-Sánchez A and Fuentes-Pananá EM:
Human Viruses and Cancer. Viruses. 6:4047–4079. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chen Y, Williams V, Filippova M, Filippov
V and Duerksen-Hughes P: Viral carcinogenesis: Factors inducing DNA
damage and virus integration. Cancers (Basel). 6:2155–2186. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Sherman M and Colombo M: Hepatocellular
carcinoma screening and diagnosis. Semin Liver Dis. 34:389–397.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yang SW, Kim GH, Chung JW, Sohn HR, Lee
SS, Hong S, Chung SM, Jang ES, Jeong SH and Kim JW: Prediction of
risk for hepatocellular carcinoma by response of serum
α-fetoprotein to entecavir therapy. J Gastroenterol Hepatol.
30:1175–1182. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Triolo M, Corte C Della and Colombo M:
Impact of HBV therapy on the incidence of hepatocellular carcinoma.
Liver Int. 34:(Suppl 1). S139–S145. 2014. View Article : Google Scholar
|