Introduction
Pancreatic adenocarcinoma is the sixth cause of
cancer-associated mortalities worldwide (1). The majority of patients with pancreatic
adenocarcinoma present with an unresectable tumor or with
metastatic disease, which lead to a 5-year survival rate of ~5%.
Since the mortality rate remains close to the incidence rate, this
is a particularly dreaded form of cancer (1). For years, gemcitabine was the front-line
chemotherapy for the advanced disease due to its effects on quality
of life and overall survival (OS) (2,3). In 2011,
folinic acid, fluorouracil (5-FU), irinotecan and oxaliplatin
(folfirinox) was observed to produce better outcomes compared with
those of the standard gemcitabine chemotherapy (median OS, 11.1 vs.
6.8 months, respectively; P<0.001) (4). Henceforth, folfirinox became the
first-line treatment for patients with advanced pancreatic
adenocarcinoma who had a good Eastern Cooperative Oncology Group
(ECOG) performance status (5). More
recently, Von Hoff et al reported an improved outcome when
nanoparticle albumin-bound (nab)-paclitaxel was combined with
gemcitabine (GemBrax) compared with that of gemcitabine treatment
alone (6).
When gemcitabine was the standard first-line
treatment, an oxaliplatin-based chemotherapy was usually proposed
as the second-line chemotherapy (7).
Indeed, based on promising results from phase II studies (8–10), a
randomized-phase III study demonstrated that the median survival
time upon failure of first-line gemcitabine treatment increased to
21 weeks with oxaliplatin/folinic acid/5-fluorouracil treatment and
best supportive care (BSC) compared with only 10 weeks in patients
receiving BSC alone (7). Other
studies have reported different experiences with second-line
treatments subsequent to gemcitabine, with modest efficacy for
patients who still have a good ECOG performance status (Table I).
 | Table I.Studies available about second-line
therapies after a first-line treatment of gemcitabine for
pancreatic cancer. |
Table I.
Studies available about second-line
therapies after a first-line treatment of gemcitabine for
pancreatic cancer.
| Author, year | Trial | First-line
chemotherapy | Second-line
chemotherapy | Patients, n | Response rate,
% | Median PFS, months
(range) | Median OS, months
(range) | PFS at 6 months,
% | OS at 6 months,
% | OS at 1 year,
% | Ref. |
|---|
| Pelzer et
al, 2011 | Phase III
CONKO-003 | GEM | OFF vs. FF | 46 |
|
| 4.82 vs. 2.3 |
| 23 vs. 10 | 10 vs. 0 | (7) |
| Tsavaris et
al, 2005 | Phase II | GEM | 5-FU/AF/OX | 30 | 23.3 (PR) 30
(SD) | 5.3 (3–4.7) | 5.8 (4.7–7.7) |
|
|
| (8) |
| Cantore et
al, 2004 | Phase II | GEM-containing
treatment | IRI plus OX | 30 | 10 | 4.1 (0.7–13.1) | 5.9 |
|
| 23.3 | (9) |
| Demols et
al, 2006 | Phase II | GEM | GEMOX | 33 | 22.6 (PR) | 4.2 | 6 (0.5–21) |
|
|
| (10) |
| Boeck et al,
2006 | Phase II | GEM | Pemetrexed | 52 | 3.8 19.2 (SD) | 1.6
(0.25–14.5) | 4.7
(0.25–19.6) |
|
|
| (14) |
| Kulke et al,
2007 | Phase II | GEM | CAP plus
erlotinib | 30 | 10 (PR) | 3.4 | 6.5 |
|
| 26 | (15) |
| Xiong et al,
2008 | Phase II | GEM | CAP plus OX | 41 | 2.6 (PR) 26
(SD) | 2.3 | 5.7 |
| 44 | 21 | (37) |
| Reni et al,
2008 | Retrospective
study | GEM | PEFG | 46 | 24 (PR) | 5 | 8.3 | 34 |
| 26 | (38) |
| Boeck et al,
2007 | Phase II | GEM | CAP | 39 | 0 (PR) 15 (SD) | 2.3 (0.5–45.1) | 7.6 (0.7–45.1) |
|
|
| (39) |
| Reni et al,
2006 | Phase II | GEM | Raltitrexed plus
OX | 41 | 24 (PR) 11
(SD) | 1.8 | 5.2 | 14.6 |
| 12 | (40) |
| Burris et
al, 2005 | Phase II | Any prior
treatment | Rubitecan | 58 | 7 |
| 3 |
| 17 | 9 | (41) |
| Jacobs et
al, 2004 | Phase III | Any prior
treatment | Rubitecan | 196 | 11 (PR) 38
(SD) | 1.9 | 3.5 |
|
|
| (42) |
| Ulrich-pur et
al, 2003 | Phase II | GEM | IRI plus
raltitrexed vs. raltitrexed | 38 | 16 vs. 0 | 4 vs. 2.5 | 6.5 vs. 4.3 |
|
|
| (43) |
| Kozuch et
al, 2001 | Retrospective
study | Any prior
treatment | G-FLIP | 34 | 24 (PR) 21
(SD) | 3.9 | 10.3 |
|
|
| (44) |
| Altwegg, 2012 | Retrospective
study | GEM | All second-line
therapies | 80 | 40 (PR+SD) | 3.4 | 5.8 |
|
| 13.6 | (45) |
| Wang-Gillam et
al, 2016 | Phase III
NAPOLI-1 | GEM-containing
treatment | Nanoliposomal IRI
plus FF vs. FF | 417 | 16 (PR) vs. 1
(PR) | 3.1 vs. 1.5 | 6.1 vs. 4.2 |
|
|
| (46) |
In the phase III study by Conroy et al
(4), 47% of patients who experienced
treatment failure with folfirinox received a second-line therapy.
In the phase III study by Von Hoff et al (6), 38% of the nab-paclitaxel and gemcitabine
treatment group, and 42% of the gemcitabine alone group received
second-line chemotherapy. Notably, 6% of the gemcitabine group
received second-line treatments of nab-paclitaxel and gemcitabine,
and these patients had a longer survival rate than the patients
receiving gemcitabine treatment alone (median survival, 9.4 vs. 6.8
months, respectively; P<0.001).
Several scenarios could account for these data.
First, patients usually experience a decline in their ECOG
performance status, which may limit the therapeutic options for
second-line treatment (11). Second,
the survival benefit of second-line treatments is clinically
questionable. Certain data are in favor of second-line therapy
(12), whereas others do not
encourage its use (13). Based on
phase II data, a median survival of 4–6 months after the initiation
of second-line treatment may be achieved with salvage chemotherapy
in selected patients (14–16).
Folfirinox is currently the first-line treatment for
metastatic pancreatic cancer in our center (Centre Léon Bérard,
Lyon, France). For second-line therapy, patients are usually
treated with gemcitabine alone when clinical trials are
unavailable. The present study aimed to retrospectively analyze
this treatment approach, which has not been validated in a phase
III randomized study, in order to evaluate the clinical benefit of
this strategy and to identify any clinical or biological
characteristics that could predict the treatment outcome.
Patients and methods
Patients
The present study retrospectively reviewed 42
consecutive cases of advanced-stage pancreatic adenocarcinoma in
patients who were treated with gemcitabine as the second-line
chemotherapy (following initial treatment with folfirinox) between
January 2008 and December 2012 at the Centre Léon Bérard (Lyon,
France). Folfirinox was administered in accordance with the study
regimen reported by Conroy et al (4): Treatment was provided for 6 months (12
cycles) or until disease progression or unmanageable toxicity
occurred. When 6 months of folfirinox was achieved, discontinuation
was proposed. At the point of disease progression, folfirinox
reintroduction was considered for first-line continuation and this
treatment was included in the total number of folfirinox cycles
that were received. Clinical (age, sex, history of recent diabetes,
thromboembolic events, and body mass index and its variation during
chemotherapy) and biological [hemoglobin, total bilirubin,
lymphocyte levels, carbohydrate antigen 19–9 (CA19-9) and
carcinoembryonic antigen (CEA) levels, and their variation during
chemotherapy] data, as well as tumor characteristics [pancreas
localization, Union for International Cancer Control staging
(17) at diagnosis, number of
metastatic sites, presence of skip metastasis and computed
tomography (CT)-scan evaluation every 2 months] were collected
prior to or during gemcitabine treatment to elucidate any parameter
with a predictive value on survival. Patients who had previous
surgery and adjuvant chemotherapy were excluded. All patients
provided their informed consent for inclusion in the study and an
external Ethics Committee (Comité de Protection des Personnes LYON
SUD-EST IV) gave its approval for the project on 16th December
2015.
The side effects of gemcitabine were graded using
the Common Toxicity Criteria defined (Common Terminology Criteria
for Adverse Events scale developed by Eastern Cooperative Oncology
Group and the National Cancer Institute with last version 4.03
released in 2010; http://evs.nci.nih.gov/ftp1/CTCAE/About.html). Tumor
objective response was monitored every 2 months with a CT-scan
using the Response Evaluation Criteria in Solid Tumors (18), physical examination and assessment of
blood tumor markers. Control of the disease was defined as
achieving a complete response, partial response or disease
stabilization while on chemotherapy. OS was measured from the
initiation of treatment to the date of mortality for any reason or
to the last follow-up assessment.
Statistical analysis
Descriptive statistics are presented as medians and
ranges for the quantitative data, and as proportions for the
qualitative data. Survival data are presented as Kaplan-Meier
curves. OS was defined as the time from the initiation of
gemcitabine chemotherapy to mortality (whatever the cause).
Patients alive at the last date of follow-up were censored.
Patients were defined as ‘responders’ [responders
group (RG)] to gemcitabine chemotherapy if the disease was under
control (complete or partial response, or tumor stability) during
the first evaluation of treatment efficacy (2 months after
initiation). Patients were defined as ‘non-responders’ if disease
progression or mortality was experienced prior to the first
evaluation [non-responders group (NRG)]. The association between
response (yes/no) and potential predictive factors was studied
using the χ2 or Fisher's exact tests for qualitative
variables, and the nonparametric Wilcoxon test for quantitative
variables. Due to the small sample size, a multivariate analysis
was not performed. In all cases, P<0.05 was considered to
indicate a statistically significant difference, and a P-value
between 0.05 and 0.1 was considered to indicate a trend. All
statistical analyses were performed using SAS version 9.3 software
(SAS Institute, Cary, NC, USA). The statistical methods used in the
present study were reviewed by Miss Nadia Oussaid (a biomedical
statistician at the Centre Léon Bérard).
Results
Patient characteristics
Among the 42 patients enrolled in the present study,
22 (52.4%) were males (Table II).
The majority of patients (90.5%) had a good performance status (PS)
(0 or 1) at diagnosis. In total, 50.0% of the tumors were localized
in the pancreatic head, 26.2% in the body and the remaining tumors
in the tail. In total, 5 patients (12.0%) had a recent diagnosis of
diabetes (<2 years), while 8 patients (19.1%) had jaundice at
their first consultation; the obstruction was relieved through an
endoscopic retrograde cholangiopancreatography with stent insertion
(14.3%) or biliodigestive surgical derivation (4.8%). At diagnosis,
95.2% of patients had metastatic cancer (stage 4): 28 patients
(70.0%) had 1 metastatic site; 11 patients (27.5%) had 2 metastatic
sites; and 1 patient had 3 metastatic sites. In addition, 5
patients (12.0%) had lung metastasis without any liver
localization.
| Table II.Clinical characteristics of patients
with pancreatic adenocarcinoma (n=42). |
Table II.
Clinical characteristics of patients
with pancreatic adenocarcinoma (n=42).
| Characteristic | Patients, n
(%) |
|---|
| Median age (range),
years | 63.5 (47–76) |
| Sex ratio,
male/female | 22/20 |
| TNM stage at
diagnosis, n (%) |
| 4 | 40 (95.2) |
| 3 | 0 (0.0) |
| 2 | 2 (4.8) |
| Metastatic sites at
diagnosis, n (%) |
| 0 | 2 (4.8) |
| 1 | 28 (66.6) |
| 2 | 11 (26.2) |
| 3 | 1 (2.4) |
| TNM stage at the
start of second-line gemcitabine, n (%) |
| 4 | 41 (97.6) |
| 3 | 0 (0.0) |
| 2 | 1 (2.4) |
Treatments
First-line folfirinox treatment
On average, 9.4 cycles of folfirinox were
administered as the first-line treatment (range, 2–36 cycles). A
total of 21 patients received 6 months of folfirinox and
discontinued chemotherapy for 3.2 months (range, 0–20 months)
before disease progression occurred. Overall, folfirinox treatment
induced disease stability or a partial response in 27 patients
(69.2%). During the first-line treatment, 16 patients (38.1%) had
progressed prior to receiving 6 months of folfirinox, and 7
patients (16.7%) had tumor progression at the 6-month evaluation.
Second-line chemotherapy was introduced for patients whose disease
had progressed (83.3%) or who experienced toxicity (14.3%); a
single patient (2.4%) requested early treatment discontinuation
following 8 cycles (without limiting toxicity and despite partial
response). In total, 5 patients (12.5%) received >6 months of
folfirinox: 2 did not have discontinuation and experienced
progressive disease following 16 and 17 cycles of treatment,
respectively (oxaliplatin was interrupted due to neurotoxicity
following 14 cycles and 10 cycles, respectively), while 3 patients
had a therapeutic interruptions. Of these 3 patients, 1 patient
received folfirinox again following an interruption of 4 months,
with long disease control; the other 2 patients had a 6-month and a
20-month interruption, respectively, prior to reintroduction of
first-line chemotherapy with folfiri (folinic acid, 5-fluorouracil,
irinotecan) only (due to residual neurotoxicity to oxaliplatin),
resulting in no benefit on disease control. The disease control
offered by folfirinox reintroduction led to another 4-month
therapeutic interruption following 12 additional cycles. The
disease was controlled again at the third time of folfirinox
treatment, but progression occurred following 9 cycles.
Second-line gemcitabine treatment
Gemcitabine treatment was initiated with a median
time of 1.75 months (range, 0–20 months) upon termination of
folfirinox treatment. Overall, gemcitabine treatment was well
tolerated (Table III). A single
grade 4 thrombocytopenia was recorded. In total, 6 patients
experienced a maximum of grade 2 toxicity (4 had thrombocytopenia,
1 had arthromyalgia and 2 had anemia). In addition, 4 other
patients had a maximum of grade 3 neutropenia, and 1 patient
discontinued gemcitabine treatment due to asthenia.
| Table III.Treatment characteristics in
pancreatic adeno-carcinoma patients (n=42). |
Table III.
Treatment characteristics in
pancreatic adeno-carcinoma patients (n=42).
| Treatment | Patients, n
(%) |
|---|
| Folfirinox followed
by GEM, total number of chemotherapy regimens received |
| 2 | 42 (100.0) |
| 3 | 17 (40.5) |
| 4 | 3 (7.0) |
| Folfirinox response
at 2 months |
| Disease
controlled (disease stabilization or partial response) | 28 (66.6) |
| Disease
progression | 12 (28.6) |
| NA | 2 (4.8) |
| Treatment
interruption following first-line therapy |
|
Patients, n (%) | 12 (28.6) |
| Time to
second-line therapy, months | 3.4 |
| GEM response at 2
months |
| Disease
controlled (disease stabilization or partial response) | 11 (26.0) |
| Disease
progression | 31 (74.0) |
| GEM toxicity,
maximum grade observed |
| 1 | 5 (11.9) |
| 2 | 6 (14.3) |
| 3 | 6 (14.3) |
|
Treatment interruption | 1 (2.4) |
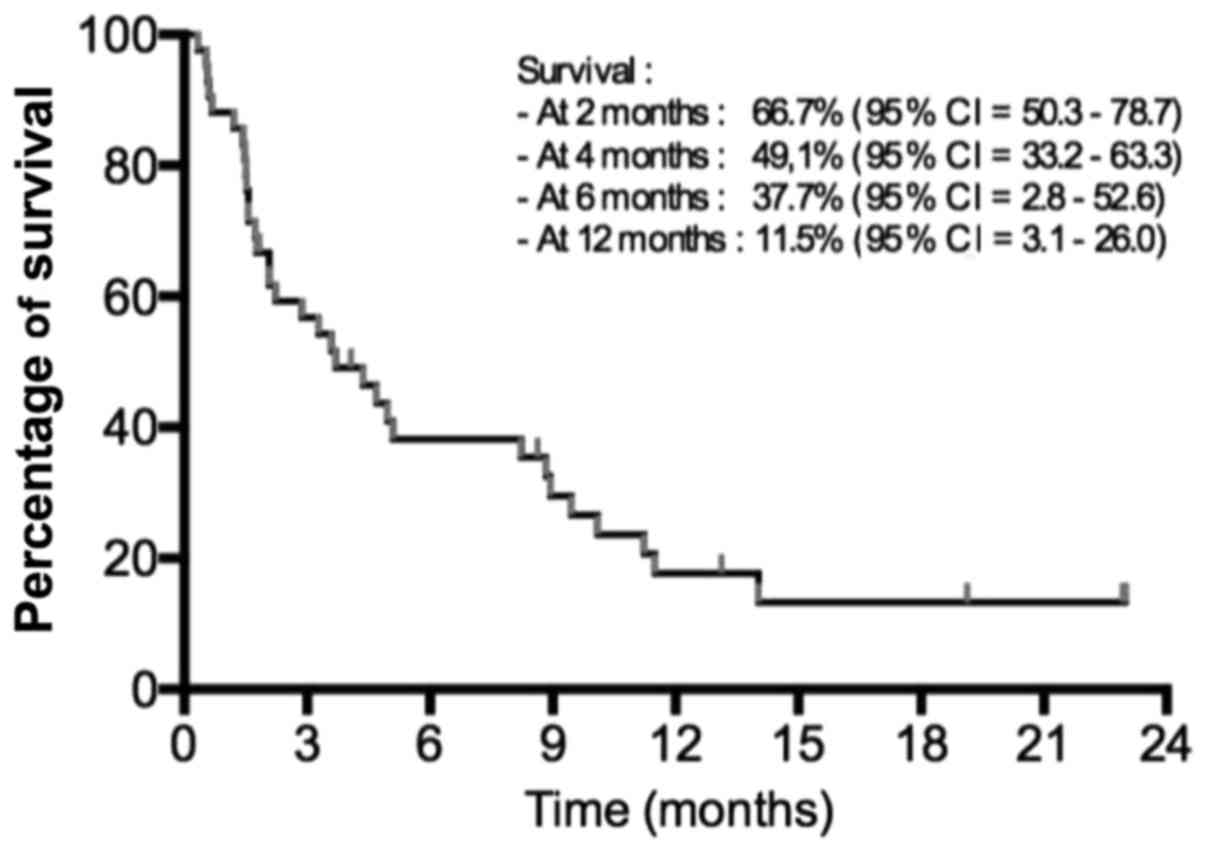
The median follow-up for the second-line treatment
was 5.8 months (range, 0.3–25.5 months). From the 42 patients, 39
(92.9%) succumbed at the cut-off analysis time. The median OS was
3.6 months [95% confidence interval (CI), 2.1–5.1] after starting
the second-line chemotherapy (Fig.
1). The median OS from the diagnosis was 13.4 months (range,
3.3–30.7 months).
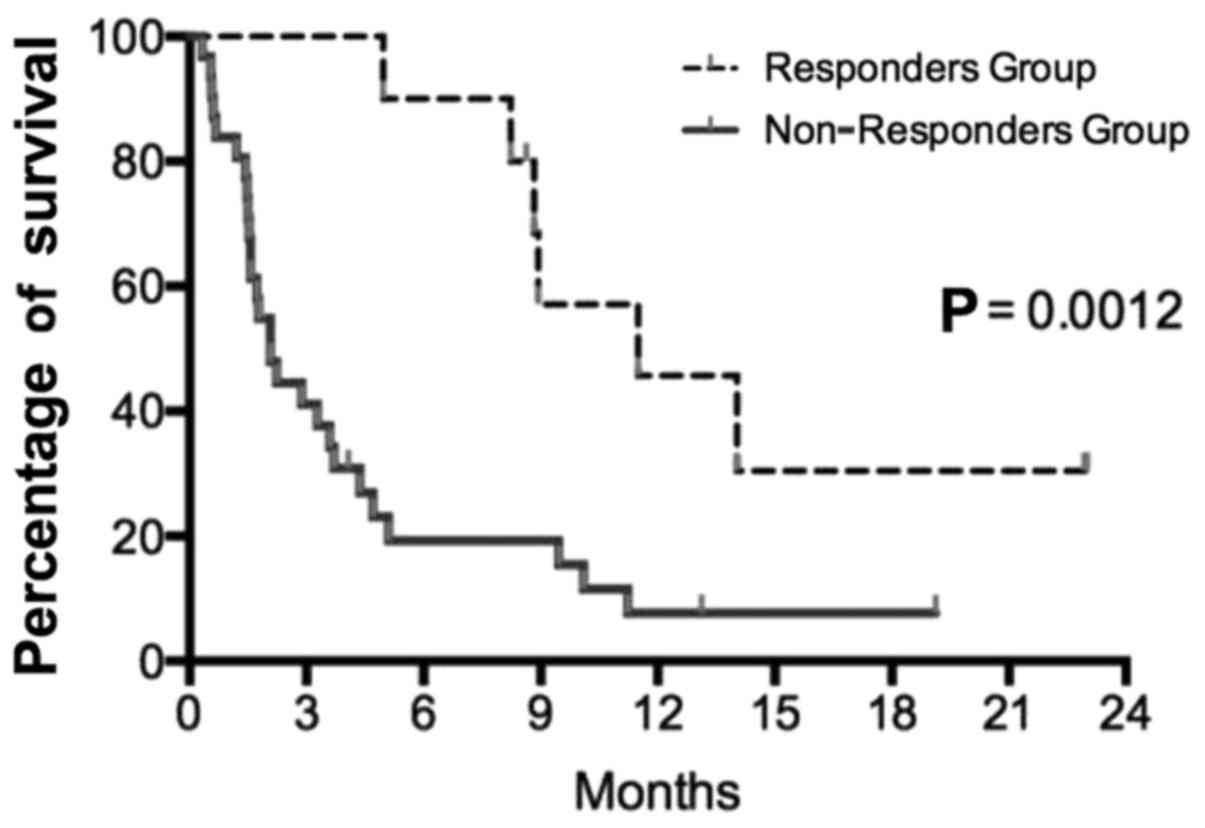
A median of 4.5 gemcitabine infusions were
administered (range, 1–40 infusions); the median length of the
treatment was 1.5 months (range, 0.3–13.3 months). After 2 months
of gemcitabine chemotherapy, only 11 patients (26.2%) had the
disease under control (mainly stable disease) and continued with
treatment. Disease control at the first evaluation was the only
identified significant prognostic factor for OS (P=0.0012)
(Fig. 2). A total of 31 patients
(74.0%) experienced disease progression at the first
evaluation.
Clinical, biological and tumor data analyses
The present study attempted to identify predictive
biological or clinical characteristics explaining gemcitabine's
efficacy. General characteristics such as PS were evaluated. This
parameter was not different between the two groups; all the
patients had a PS of 0–1 in the RG, and 27/31 patients (87.0%) had
the same score in the NRG (P=0.350). The body mass index prior to
the second-line treatment or its variation during therapy did not
differ between the RG and NRG. The overall median body mass index
preceding the second-line chemotherapy was 23.34 kg/m2
(range, 17.20–36.20 kg/m2). Similarly, the age at
diagnosis and sex were not different between the two groups.
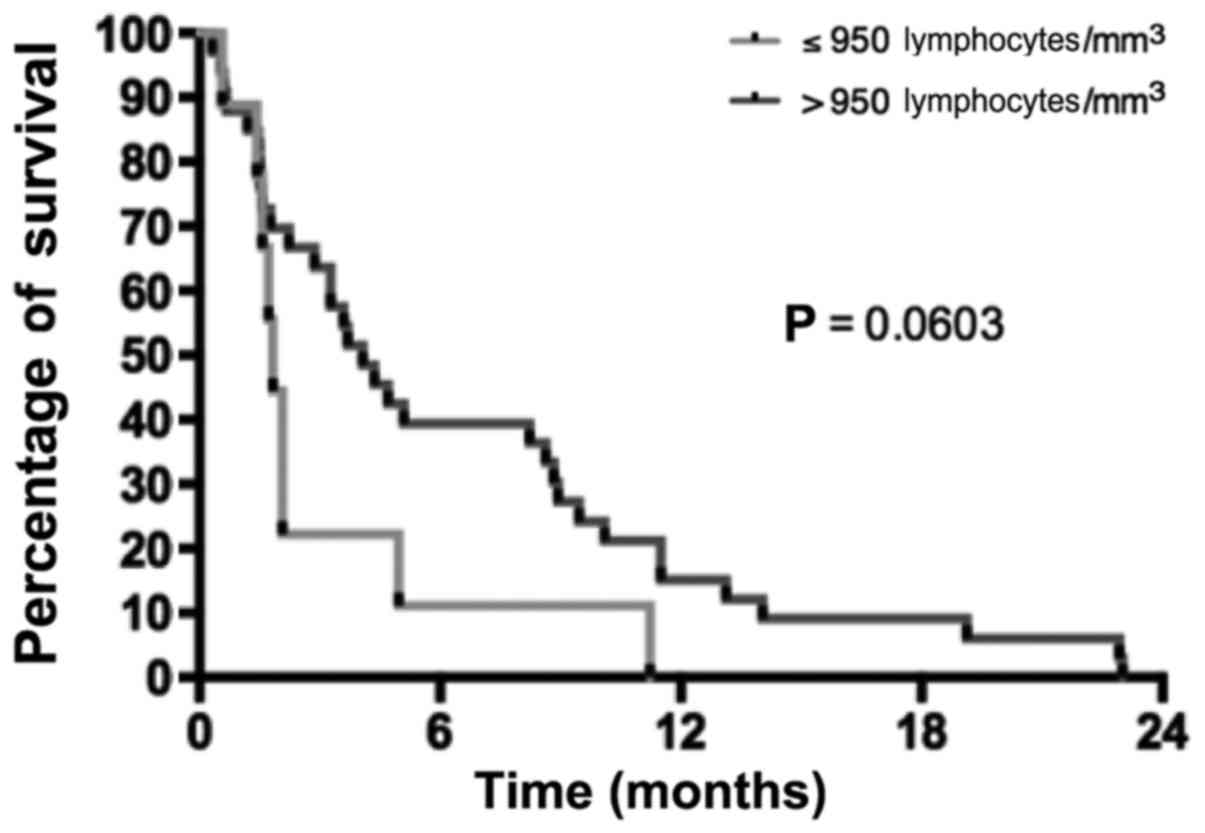
Various biological parameters were also compared
between the two groups. The albumin level at diagnosis tended to be
higher in the RG than in the NRG (median, 41 g/l in RG vs. 35 g/l
in NRG; P=0.063). The lymphocyte levels prior to the second-line
chemotherapy were not different between the NRG and RG (the mean
lymphocyte levels were 1,349.5 and 1,593.8
lymphocytes/mm3, respectively; P=0.640). A value of 950
lymphocytes/mm3 was used as the cut-off to separate RG
and NRG patients, and it was observed that patients with lymphocyte
levels <950 lymphocytes/mm3 had poorer survival than
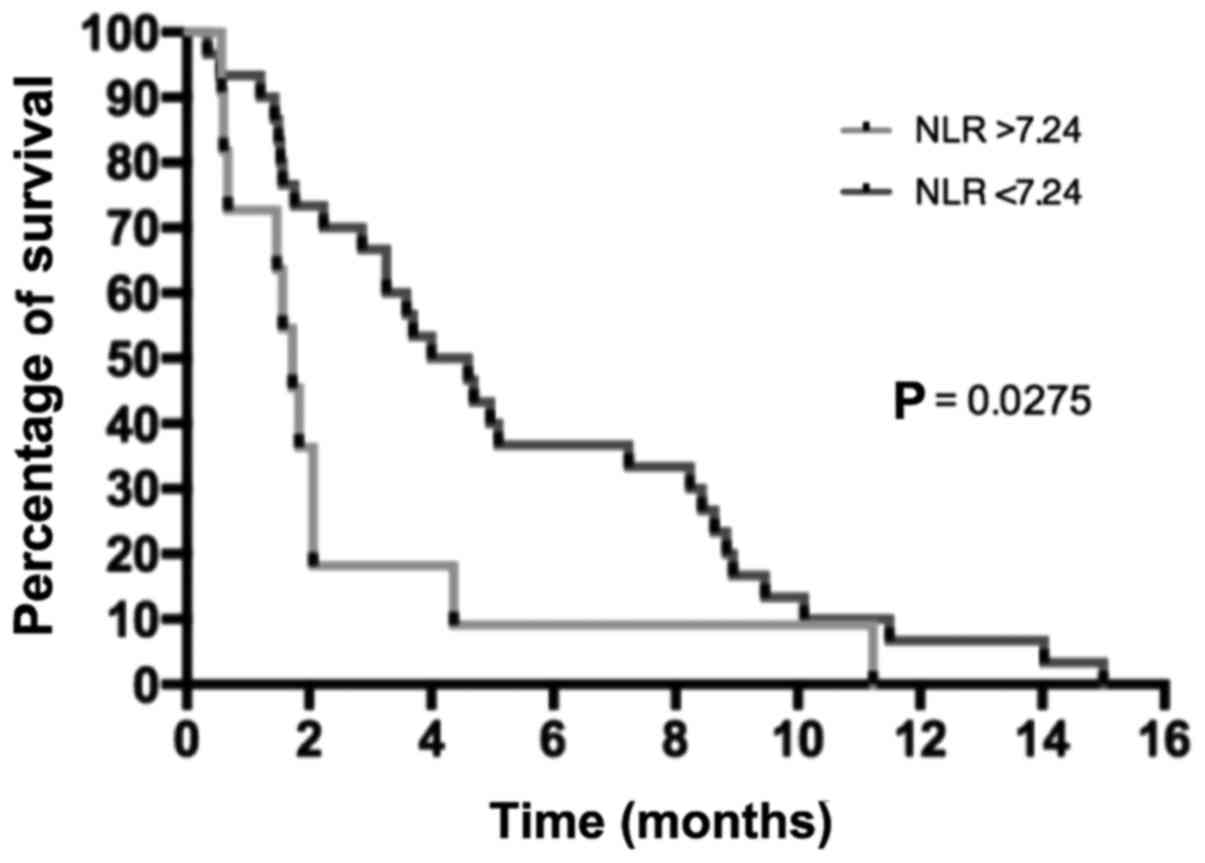
patients with lymphocyte levels above this cut-off (Fig. 3). The neutrophil/lymphocyte ratio
(NLR) preceding the second-line chemotherapy was 7.24 and 3.56 in
RG and NRG, respectively, suggesting a trend between lower NLR and
RG (P=0.200), while a significant higher survival percentage was
observed in patients with a NLR <7.24 (P=0.030) (Fig. 4). The tumor burden was also analyzed.
The number of metastatic sites prior to initiating the second-line
treatment tended to be higher in the NRG than in the RG, although
the difference was not significant (90.0% of RG patients had 1
metastatic site vs. 63.3% of patients in the NRG; P=0.420). There
was also a trend for higher average CEA levels in the NRG than in
the RG (156.3×10−6 vs. 44.3×10−6 g/l,
respectively; P=0.330). The mean CA19-9 levels did not differ
between the two groups (24,311.6 kU/l in the RG vs. 17,109 kU/l in
the NRG; P=0.250).
Patients with primary resistance to
folfirinox
Of the 11 patients in the RG, 6 exhibited primary
resistance to folfirinox and had early disease progression.
Patients whose disease progressed during folfirinox treatment had a
higher probability of responding to gemcitabine (54.5 vs. 21.4%,
respectively; P=0.061; Table IV). By
contrast, only 3/15 patients whose disease was well controlled with
folfirinox (20.0%) experienced any disease control with second-line
gemcitabine treatment. In the RG, of the 6 patients who exhibited
primary resistance to folfirinox, 2 received a prolonged benefit
under gemcitabine treatment, and their cancer remained under
control for 6 months.
| Table IV.Correlation between folfirinox and
gemcitabine responses in pancreatic adenocarcinoma patients
(n=42). |
Table IV.
Correlation between folfirinox and
gemcitabine responses in pancreatic adenocarcinoma patients
(n=42).
|
| Gemcitabine |
|
|
|---|
|
|
|
|
|
|---|
| Folfirinox | Controlled disease,
n (%) | Resistant disease,
n (%) | Total, n (%) | Fisher's exact
test |
|---|
| Controlled
disease | 5 (45.5) | 22 (78.6) | 27 (69.2) | P=0.061 |
| Resistant
disease | 6 (54.5) | 6 (21.4) | 12 (30.8) |
|
Third-line treatments
Of the patients whose disease progressed while
receiving gemcitabine, 19 patients (45.0%) were administered a
third-line chemotherapy regimen and 3 patients received a
fourth-line chemotherapy treatment (Table III). Among these patients, 15
received >1 cycle of therapy, while 8 patients received >3
cycles. During the third-line treatment, only 2 patients
experienced prolonged disease control with gemcitabine-oxaliplatin
(15 cycles prior to disease progression) and with folinic acid,
5-FU and oxaliplatin (14 cycles prior to discontinuation and
surveillance). The latter patients experienced disease progression
after 6 months of treatment, but were able to control the cancer
with 5-FU and folinic acid combination prior to discontinuation and
surveillance.
Discussion
There is a lack of prospective data about
second-line treatments for metastatic pancreatic ductal
adenocarcinoma (PDAC) patients. This is partially due to the recent
changes in first-line chemotherapy treatments (4,19). Despite
this dearth of information, a significant proportion of PDAC
patients are eligible for second-line therapy. In the Action to
Control Cardiovascular Risk in Diabetes 11 study, 47% of patients
who received folfirinox were eligible for second-line chemotherapy,
and the majority of them received gemcitabine (4). In the Metastatic Pancreatic
Adenocarcinoma Clinical Trial, 38% of patients received second-line
chemotherapy (19). The published
data that suggest that second-line chemotherapy is beneficial are
mainly derived from studies on gemcitabine-refractory patients
(20,21).
When folfirinox treatment fails to improve a
patient's cancer, gemcitabine monotherapy appears to be a
convenient treatment option due to its safety profile (3); however, there are no prospective data
available or studies planned to address its efficacy according to
the website (https://clinicaltrials.gov/). The present study
reports the findings on a single center cohort of patients who
received second-line gemcitabine treatment for advanced-stage
pancreatic adenocarcinoma. A survival of 3.6 months with
second-line chemotherapy was observed, which is in agreement with
previous published data (Table I)
(7–10,14,15,22–31).
Response to gemcitabine therapy at the first follow-up evaluation
(at 2 months) impacted significantly the OS of the patients.
Notably, the present study demonstrated that
gemcitabine was able to control cancer in patients who were
resistant to folfirinox treatment, suggesting that there is no
cross-resistance between folfirinox and gemcitabine regimens.
Indeed, it was observed that patients who were resistant to
first-line folfirinox treatment tended to respond well to
gemcitabine treatment (54.5 vs. 21.4%, respectively). These data
strengthen the argument for gemcitabine treatment, particularly if
the patient displays primary resistance to folfirinox, and also
support the requirement for more effective drug combinations.
Predictive factors of successful gemcitabine
treatment were also analyzed; however, no predictive biological
markers were identified, which may be due to the small cohort size.
CA19-9 level did not display a predictive value during second-line
treatment, whereas it does have a predictive value for first-line
treatment (11). Other biomarkers
were not evaluated, including the Glasgow prognostic score or its
modified version, which is an inflammation-based prognostic score
using standard laboratory measurements of albumin and C-reactive
protein (32,33). This score is able to identify systemic
inflammatory responses responsible for poor survival due to tumor
growth stimulation and catabolic effects on the host's metabolism
at every stage of the disease for resectable, unresectable and
metastatic pancreatic cancer (33–35). The
measurement of pre-treatment plasma circulating DNA KRAS mutation
load and CA19-9 level has also been recently shown to be a strong
prognostic factor for PDAC patients who receive gemcitabine or
folfirinox (36). It has also been
suggested that human equilibrative nucleoside transporter 1 (hENT1)
expression may select patients for gemcitabine treatment (37). However, there are issues regarding the
evaluation of its expression by immunohistochemistry, since two
different antibodies are usually employed: 10D7G2 monoclonal murine
antibody (not commercialized) and SP120 rabbit monoclonal antibody
(commercialized by Ventana Medical Systems, Inc., Tucson, AZ, USA).
All studies using the above murine antibody demonstrated a
significant predictive value in response to gemcitabine in an
adjuvant setting only (38–40) whereas those using the aforementioned
rabbit monoclonal antibody did not (41). Data on advanced pancreatic cancer are
scarce, with only two studies published to date, both of which used
the SP120 rabbit monoclonal antibody to measure hENT1 expression,
and no evidence of predictive value was identified (42,43). Thus,
the role of hENT1 as a predictive marker of gemcitabine efficacy
remains unclear, particularly in a metastatic pancreatic cancer
setting.
The main limitations of the present study are its
retrospective design and the small sample size. Another limitation
is the use of a monotherapy treatment. Various clinicians use a
dual-therapy regimen such as gemcitabine and cisplatin or GemBrax
subsequent to first-line folfirinox treatment, despite the lack of
evidence regarding its efficacy from prospective studies (31–33). In
France, reimbursement for nab-paclitaxel is not yet available, thus
limiting its prescription. Bertocchi et al (44), Portal et al (45) and Palacio et al (46) recently reported the results of a
GemBrax regimen for second-line therapy following a gemcitabine- or
pyrimidine-based treatment (including folfirinox). However,
definitive conclusions could not be drawn due to the retrospective
design of the studies and the lack of a control arm. New drug
combinations with gemcitabine are currently under study in phase II
trials as mentioned in https://clinicaltrials.gov/, but the choice of the
control arm in future phase III studies remains open. Furthermore,
second-line chemotherapy may have a significant effect on the OS
results in phase III trials. Therefore, it appears to be essential
to report these second-line treatments in phase III trials that
evaluate first-line therapies in order to analyze any differences
in the OS results.
In conclusion, the use of gemcitabine as a
second-line treatment is well tolerated in PDAC patients, and may
offer a small benefit to their OS (median, 3.6 months; 95% CI,
2.1–5.1), particularly in patients whose disease progressed during
first-line folfirinox treatment. The management of metastatic PDAC
patients has recently evolved, as the results of new chemotherapy
regimens (folfirinox and GemBrax) have shown significant benefits
over gemcitabine alone for first-line treatments (4,19). These
therapeutic advances provide an opportunity for clinicians to
explore new strategic approaches. Therefore, second-line treatments
must be prospectively evaluated in order to draw formal conclusions
about their efficacy.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Burris H and Storniolo AM: Assessing
clinical benefit in the treatment of pancreas cancer: Gemcitabine
compared to 5-fluorouracil. Eur J Cancer. 33 Suppl 1:S18–S22. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Burris HA III, Moore MJ, Andersen J, Green
MR, Rothenberg ML, Modiano MR, Cripps MC, Portenoy RK, Storniolo
AM, Tarassoff P, et al: Improvements in survival and clinical
benefit with gemcitabine as first-line therapy for patients with
advanced pancreas cancer: A randomized trial. J Clin Oncol.
15:2403–2413. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Conroy T, Desseigne F, Ychou M, Bouché O,
Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de
la Fouchardière C, et al: FOLFIRINOX versus gemcitabine for
metastatic pancreatic cancer. N Engl J Med. 364:1817–1825. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
von Hoff DD, Ervin T, Arena FP, Chiorean
EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, et
al: Increased survival in pancreatic cancer with nab-paclitaxel
plus gemcitabine. N Engl J Med. 369:1691–1703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pelzer U, Schwaner I, Stieler J, Adler M,
Seraphin J, Dörken B, Riess H and Oettle H: Best supportive care
(BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF)
plus BSC in patients for second-line advanced pancreatic cancer: A
phase III-study from the German CONKO-study group. Eur J Cancer.
47:1676–1681. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tsavaris N, Kosmas C, Skopelitis H,
Gouveris P, Kopterides P, Loukeris D, Sigala F, Zorbala-Sypsa A,
Felekouras E and Papalambros E: Second-line treatment with
oxaliplatin, leucovorin and 5-fluorouracil in
gemcitabine-pretreated advanced pancreatic cancer: A phase II
study. Invest New Drugs. 23:369–375. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cantore M, Rabbi C, Fiorentini G, Oliani
C, Zamagni D, Iacono C, Mambrini A, Del Freo A and Manni A:
Combined irinotecan and oxaliplatin in patients with advanced
pre-treated pancreatic cancer. Oncology. 67:93–97. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Demols A, Peeters M, Polus M, Marechal R,
Gay F, Monsaert E, Hendlisz A and Van Laethem JL: Gemcitabine and
oxaliplatin (GEMOX) in gemcitabine refractory advanced pancreatic
adenocarcinoma: A phase II study. Br J Cancer. 94:481–485. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bauer TM, El-Rayes BF, Li X, Hammad N,
Philip PA, Shields AF, Zalupski MM and Bekaii-Saab T: Carbohydrate
antigen 19–9 is a prognostic and predictive biomarker in patients
with advanced pancreatic cancer who receive gemcitabine-containing
chemotherapy: A pooled analysis of 6 prospective trials. Cancer.
119:285–292. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nagrial A, Chin VT, Sjoquist K, Chantrill
LA and Yip D: Survival benefit of second-line chemotherapy in
advanced pancreatic adenocarcinoma: A systematic review of the
literature. J Clin Oncol. 32:2962014. View Article : Google Scholar
|
|
13
|
Rahma OE, Duffy A, Liewehr DJ, Steinberg
SM and Greten TF: Second-line treatment in advanced pancreatic
cancer: A comprehensive analysis of published clinical trials. Ann
Oncol. 24:1972–1979. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Boeck S, Weigang-Köhler K, Fuchs M,
Kettner E, Quietzsch D, Trojan J, Stötzer O, Zeuzem S, Lordick F,
Köhne CH, et al: Second-line chemotherapy with pemetrexed after
gemcitabine failure in patients with advanced pancreatic cancer: A
multicenter phase II trial. Ann Oncol. 18:745–751. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kulke MH, Blaszkowsky LS, Ryan DP, Clark
JW, Meyerhardt JA, Zhu AX, Enzinger PC, Kwak EL, Muzikansky A,
Lawrence C and Fuchs CS: Capecitabine plus erlotinib in
gemcitabine-refractory advanced pancreatic cancer. J Clin Oncol.
25:4787–4792. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Boeck S and Heinemann V: Second-line
therapy in gemcitabine-pretreated patients with advanced pancreatic
cancer. J Clin Oncol. 26:1178–1179. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
International Union Against Cancer (UICC),
. TNM Classification of Malignant Tumours. Sobin LH, Gospodarowicz
M and Wittekind C: 7th. John Wiley & Sons, Ltd.; Chichester,
West Sussex: 2009
|
|
18
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
organization for research and treatment of cancer, national cancer
institute of the United States, national cancer institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar
|
|
19
|
Goldstein D, El-Maraghi RH, Hammel P,
Heinemann V, Kunzmann V, Sastre J, Scheithauer W, Siena S,
Tabernero J, Teixeira L, et al: nab-Paclitaxel plus gemcitabine for
metastatic pancreatic cancer: Long-term survival from a phase III
trial. J Natl Cancer Inst. 107:pii: dju413. 2015. View Article : Google Scholar
|
|
20
|
Gresham GK, Wells GA, Gill S, Cameron C
and Jonker DJ: Chemotherapy regimens for advanced pancreatic
cancer: A systematic review and network meta-analysis. BMC Cancer.
14:4712014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kaddis N and Saif MW: Second-line
treatment for pancreatic cancer. JOP. 15:344–347. 2014.PubMed/NCBI
|
|
22
|
Xiong HQ, Varadhachary GR, Blais JC, Hess
KR, Abbruzzese JL and Wolff RA: Phase 2 trial of oxaliplatin plus
capecitabine (XELOX) as second-line therapy for patients with
advanced pancreatic cancer. Cancer. 113:2046–2052. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Reni M, Cereda S, Mazza E, Passoni P,
Nicoletti R, Balzano G, Zerbi A, Arcidiacono PG, Staudacher C and
Di Carlo V: PEFG (cisplatin, epirubicin, 5-fluorouracil,
gemcitabine) regimen as second-line therapy in patients with
progressive or recurrent pancreatic cancer after
gemcitabine-containing chemotherapy. Am J Clin Oncol. 31:145–150.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Boeck S, Wilkowski R, Bruns CJ, Issels RD,
Schulz C, Moosmann N, Laessig D, Haas M, Golf A and Heinemann V:
Oral capecitabine in gemcitabine-pretreated patients with advanced
pancreatic cancer. Oncology. 73:221–227. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Reni M, Pasetto L, Aprile G, Cordio S,
Bonetto E, Dell'Oro S, Passoni P, Piemonti L, Fugazza C, Luppi G,
et al: Raltitrexed-eloxatin salvage chemotherapy in
gemcitabine-resistant metastatic pancreatic cancer. Br J Cancer.
94:785–791. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Burris HA III, Rivkin S, Reynolds R,
Harris J, Wax A, Gerstein H, Mettinger KL and Staddon A: Phase II
trial of oral rubitecan in previously treated pancreatic cancer
patients. Oncologist. 10:183–190. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jacobs AD, Burris HA, Rivkin S, Ritch PS,
Eisenberg PD and Mettinger KL: A randomized phase III study of
rubitecan (ORA) vs. best choice (BC) in 409 patients with
refractory pancreatic cancer report from a North-American
multi-center study. J Clin Oncol. 22:4013. 2004. View Article : Google Scholar
|
|
28
|
Ulrich-Pur H, Raderer M, Kornek G Verena,
Schüll B, Schmid K, Haider K, Kwasny W, Depisch D, Schneeweiss B,
Lang F and Scheithauer W: Irinotecan plus raltitrexed vs
raltitrexed alone in patients with gemcitabine-pretreated advanced
pancreatic adenocarcinoma. Br J Cancer. 88:1180–1184. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kozuch P, Grossbard ML, Barzdins A, Araneo
M, Robin A, Frager D, Homel P, Marino J, DeGregorio P and Bruckner
HW: Irinotecan combined with gemcitabine, 5-fluorouracil,
leucovorin, and cisplatin (G-FLIP) is an effective and
noncrossresistant treatment for chemotherapy refractory metastatic
pancreatic cancer. Oncologist. 6:488–495. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Altwegg R, Ychou M, Guillaumon V, Thezenas
S, Senesse P, Flori N, Mazard T, Caillo L, Faure S, Samalin E and
Assenat E: Second-line therapy for gemcitabine-pretreated advanced
or metastatic pancreatic cancer. World J Gastroenterol.
18:1357–1364. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang-Gillam A, Li CP, Bodoky G, Dean A,
Shan YS, Jameson G, Macarulla T, Lee KH, Cunningham D, Blanc JF, et
al: Nanoliposomal irinotecan with fluorouracil and folinic acid in
metastatic pancreatic cancer after previous gemcitabine-based
therapy (NAPOLI-1): A global, randomised, open-label, phase 3
trial. Lancet. 387:545–557. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Proctor MJ, Horgan PG, Talwar D, Fletcher
CD, Morrison DS and McMillan DC: Optimization of the systemic
inflammation-based Glasgow prognostic score: A Glasgow Inflammation
Outcome Study. Cancer. 119:2325–2332. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Glen P, Jamieson NB, McMillan DC, Carter
R, Imrie CW and McKay CJ: Evaluation of an inflammation-based
prognostic score in patients with inoperable pancreatic cancer.
Pancreatology. 6:450–453. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
La Torre M, Nigri G, Cavallini M,
Mercantini P, Ziparo V and Ramacciato G: The Glasgow prognostic
score as a predictor of survival in patients with potentially
resectable pancreatic adenocarcinoma. Ann Surg Oncol. 19:2917–2923.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Shimoda M, Katoh M, Kita J, Sawada T and
Kubota K: The Glasgow prognostic score is a good predictor of
treatment outcome in patients with unresectable pancreatic cancer.
Chemotherapy. 56:501–506. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Johansen JS, Vibat CRT, Hancock S, Chen I,
Hassaine L, Samuelsz E, Collisson EA, Jensen VB, Lu T, Melnikova V
and Erlander MG: Prognostic value of plasma circulating tumor (ct)
DNA KRAS mutations and serum CA19-9 in unresectable pancreatic
cancer (PC) patients. ASCO Meeting Abstracts. 33:pp. 40222015;
|
|
37
|
Wei CH, Gorgan TR, Elashoff DA, Hines OJ,
Farrell JJ and Donahue TR: A meta-analysis of gemcitabine
biomarkers in patients with pancreaticobiliary cancers. Pancreas.
42:1303–1310. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Farrell JJ, Elsaleh H, Garcia M, Lai R,
Ammar A, Regine WF, Abrams R, Benson AB, Macdonald J, Cass CE, et
al: Human equilibrative nucleoside transporter 1 levels predict
response to gemcitabine in patients with pancreatic cancer.
Gastroenterology. 136:187–195. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Maréchal R, Bachet JB, Mackey JR, Dalban
C, Demetter P, Graham K, Couvelard A, Svrcek M, Bardier-Dupas A,
Hammel P, et al: Levels of gemcitabine transport and metabolism
proteins predict survival times of patients treated with
gemcitabine for pancreatic adenocarcinoma. Gastroenterology.
143:664–674.e1-e6. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Greenhalf W, Ghaneh P, Neoptolemos JP,
Palmer DH, Cox TF, Lamb RF, Garner E, Campbell F, Mackey JR,
Costello E, et al: Pancreatic Cancer hENT1 expression and survival
from gemcitabine in patients from the ESPAC-3 trial. J Natl Cancer
Inst. 106:djt3472014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sinn M, Riess H, Sinn BV, Stieler JM,
Pelzer U, Striefler JK, Oettle H, Bahra M, Denkert C, Bläker H and
Lohneis P: Human equilibrative nucleoside transporter 1 expression
analysed by the clone SP 120 rabbit antibody is not predictive in
patients with pancreatic cancer treated with adjuvant
gemcitabine-Results from the CONKO-001 trial. Eur J Cancer.
51:1546–1554. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ormanns S, Heinemann V, Raponi M, Isaacson
J, Laubender RP, Haas M, Kruger S, Kleespies A, Mann E,
Bartosiewicz M, et al: Human equilibrative nucleoside transporter 1
is not predictive for gemcitabine efficacy in advanced pancreatic
cancer: Translational results from the AIO-PK0104 phase III study
with the clone SP120 rabbit antibody. Eur J Cancer. 50:1891–1899.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Poplin E, Wasan H, Rolfe L, Raponi M,
Ikdahl T, Bondarenko I, Davidenko I, Bondar V, Garin A, Boeck S, et
al: Randomized, multicenter, phase II study of CO-101 versus
gemcitabine in patients with metastatic pancreatic ductal
adenocarcinoma: Including a prospective evaluation of the role of
hENT1 in gemcitabine or CO-101 sensitivity. J Clin Oncol.
31:4453–4461. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Bertocchi P, Abeni C, Meriggi F, Rota L,
Rizzi A, Di Biasi B, Aroldi F, Ogliosi C, Savelli G, Rosso E and
Zaniboni A: Gemcitabine plus nab-paclitaxel as second-line and
beyond treatment for metastatic pancreatic cancer: A single
institution retrospective analysis. Rev Recent Clin Trials.
10:142–145. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Portal A, Pernot S, Tougeron D, Arbaud C,
Bidault AT, de la Fouchardière C, Hammel P, Lecomte T, Dréanic J,
Coriat R, et al: Nab paclitaxel plus gemcitabine for metastatic
pancreatic adenocarcinoma after Folfirinox failure: Results of an
AGEO multicenter prospective cohort. Br J Cancer. 113:989–995.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Palacio S, Akunyili II, Ernani V, et al:
Gemcitabine (Gem) and nab-paclitaxel (nab-P) in patients (pts) with
refractory advanced pancreatic cancer. Am Soc Clin Oncol. (Suppl
3): S4132015. View Article : Google Scholar
|