Introduction
Lung cancer remains the leading cause of
malignancy-associated mortality worldwide (1). Non-small cell lung cancer (NSCLC)
comprises ~80% of all cases, and the majority of patients present
with locally advanced or metastatic disease (2). Systemic chemotherapy (with or without
bevacizumab) or tyrosine kinase inhibitor (TKI) therapy currently
represent the primary treatment options for prolonging a patient's
survival rate and improving their quality of life (3–6). At
present, the standard first-line chemotherapy for unselected
advanced NSCLC is platinum doublet regimens using a
third-generation anti-cancer agent (7,8).
Erlotinib, a small molecule inhibitor of the
intracellular tyrosine kinase of epidermal growth factor receptor
(EGFR), has been approved as second-line therapy for
patients with advanced NSCLC in numerous countries. A phase III
trial (the BR.21 trial) demonstrated that unselected patients with
advanced NSCLC, progressing subsequent to first-line chemotherapy,
gained a survival benefit when treated with erlotinib compared with
best supportive care (9). At the
start of BR.21, EGFR mutations in NSCLC had not yet been
identified; therefore, the study included molecularly unselected
patients. The discovery and characterization of EGFR
mutations in 2004 was a key example of oncogene addiction,
associated with a high efficacy of biomarker-driven treatment
(10–12). As a result, EGFR TKIs are
currently the treatment of choice for patients with EGFR
mutations. Several phase III studies have demonstrated that
erlotinib and gefitinib are superior to chemotherapy in first-line
treatment, but only in EGFR-mutated patients (5,13–15). The value of erlotinib as a second-line
and third-line treatment of patients with wild type or unknown
EGFR mutation status remains controversial.
In previous years, the Tarceva Italian Lung
Optimization (TAILOR) phase III trial demonstrated that
chemotherapy was more effective compared with erlotinib for
second-line treatment for previously treated patients with NSCLC
who possess wild type EGFR tumors (16). The present study was undertaken to
evaluate the efficacy of erlotinib in second-line or more advanced
NSCLC, in particular for patients with EGFR wild type status
and who received pretreatment with gefitinib.
Patients and methods
Patients
A total of 222 patients with NSCLC received
erlotinib treatment as a first-line or further chemotherapy at the
National Kyushu Cancer Center (Fukuoka, Japan) between July 2007
and the end of February 2013. Erlotinib therapy was applied for
patients who satisfied all the following requirements: Age ≥20
years; pathologically or cytologically diagnosed as exhibiting
NSCLC; clinical stage III or IV disease (including IIIA,
non-applicable for radical radiotherapy) according to the seventh
edition of the ‘tumor, node, metastasis’ classification of lung
cancer (17); presenting evaluable
lesions (cases without measurable lesions were acceptable); freedom
from severe disorders in major organs (bone marrow, heart, lungs,
liver and kidneys); without interstitial lung disease (ILD); and
laboratory test data at the commencement of treatment indicating a
neutrophil count ≥2,000 cells/mm3 (normal range,
3,300–8,600 cells/mm3), a hemoglobin level ≥9.0 g/dl
(normal range, 13.7–16.8 g/dl), a platelet count
≥10.0×104 cells/mm3 (normal range,
15.8–34.8×104 cells/mm3), aspartate
aminotransferase [normal range 13–30 international units (IU)/l]
and alanine aminotransferase (normal range 10–42 IU/l) levels ≤100
IU/l, a total bilirubin level ≤1.5 mg/dl (normal range, 0.4–1.5
mg/dl), a serum creatinine level ≤1.2 mg/dl (normal range,
0.65–1.07 mg/dl) and a peripheral O2 saturation level of
≥90% (normal range, ≥90%). Treatment was provided subsequent to
each patient providing written consent on the basis of receiving
sufficient information regarding the treatment plan. All patients
signed a consent form prior to entry to the study. The present
study was approved by the National Kyushu Cancer Center Local
Research Ethics Committee.
Treatment and study design
Eligible patients received oral erlotinib at a dose
of 150 mg/day until disease progression (PD) or unacceptable
toxicity. Dose reductions (in 50-mg decrements) were permitted to
manage adverse events associated with erlotinib treatment. If a
patient had a confirmed diagnosis of ILD, erlotinib was
discontinued immediately.
Evaluation of the response and
statistical analysis
Prior to the start of erlotinib therapy, diagnostic
imaging with computed tomography scanning was performed to yield
baseline information. Tumor response evaluation was scheduled every
6 weeks. Responses to treatment were evaluated using the Response
Evaluation Criteria in Solid Tumors (RECIST) version 1.1 (18). The progression free survival (PFS) was
defined as the time from the start of treatment to PD or mortality.
The overall survival (OS) was defined as the time from the start of
treatment to mortality. The follow-up period concluded on May 31,
2013 for patients either still receiving treatment or beginning to
receive the next treatment.
Statistical analysis
Survival curves were produced using the Kaplan-Meier
method. Data were expressed as means ± standard deviation.
Univariate analysis was initially undertaken, followed by Cox's
multivariate analysis that included all variables with a
significance level of P<0.05, to identify variables associated
with a risk of mortality. Analysis of linear correlation was used
to evaluate the correlation between two variables; analysis of
variance with Dixon's Q-test was used to compare multiple
variables. Two-sided P<0.05 was considered to indicate a
statistically significant difference. Statistics were produced
using StatView version 5.0 (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
Table I summarizes the
background variables of the 222 patients who received erlotinib in
the present study. There were 119 males and 103 females, with a
median age of 63 years (range, 33–95 years). The Eastern
Cooperative Oncology Group (19)
performance status (PS) was 0–1, 2 and 3–4 in 181, 21 and 20 cases,
respectively. The histological types were adenocarcinoma, squamous
cell carcinoma, large cell carcinoma and NSCLC (NOS; not otherwise
specified) in 191, 10, 5 and 16 cases, respectively. The clinical
stage was IIIA, IIIB and IV in 1, 15 and 206 cases, respectively.
The EGFR mutation status was positive in 95 patients [exon
18 (G719A or G719S) in 3 cases, exon 19 deletion in 47 cases (with
T790M in 3 cases), exon 21 (L858R or L861Q) in 43 cases (with T790M
in 5 cases) and NOS in 2 cases], wild type in 52 cases and unknown
in 75 cases, respectively. A total of 92/222 patients received
gefitinib prior to erlotinib treatment. The median follow-up time
for the 222 patients who received erlotinib therapy was 858 days
(range, 27–4543 days).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Clinical
features | All patients
(n=222) | EGFR wild type
(n=52) | EGFR mutated
(n=95) | EGFR status unknown
(n=75) |
|---|
| Gender |
|
|
|
|
|
Male/female |
119/103 |
33/19 |
33/62 |
37/38 |
| Age |
|
|
|
|
| Median
(range) | 63
(33–95) | 64
(36–85) | 63
(37–95) | 61
(33–83) |
| ECOG performance
status |
|
|
|
|
|
0/1/2/3/4 | 63/118/21/15/5 | 17/28/3/3/1 | 38/35/10/8/4 |
8/55/8/4/0 |
| Smoking
history |
|
|
|
|
|
Never |
122 | 13 | 55 | 32 |
|
Current/former |
100 |
23/16 |
15/25 |
20/23 |
| Histological
type |
|
|
|
|
|
Adenocarcinoma |
191 | 43 | 88 | 60 |
| Large
cell carcinoma |
5 |
3 |
1 |
1 |
|
Squamous cell carcinoma | 10 |
3 |
1 |
6 |
| NSCLC
(NOS) | 16 |
3 |
5 |
8 |
| Stage |
|
|
|
|
|
IIIA/IIIB/IV | 1a/15/206 | 0/7/45 | 1/2/92 | 0/5/70 |
| Prior gefitinib
treatment |
|
|
|
|
|
Yes/no |
91/131 |
9/43 |
50/45 |
32/43 |
| Prior regimens |
|
|
|
|
| 0/1/2/3
or more | 3/55/107 | 0/6/30 | 3/20/32 | 0/9/21/45 |
Response and survival analysis of all
patients
The efficacy was evaluated by each attending
physician in accordance with the RECIST criteria, version 1.1.
Among the 222 patients who received erlotinib therapy, the best
overall response was a partial response (PR) in 31 patients, stable
disease (SD) in 101 patients and progressive disease (PD) in 90
patients. The best response rate (RR) of all patients was 14% [95%
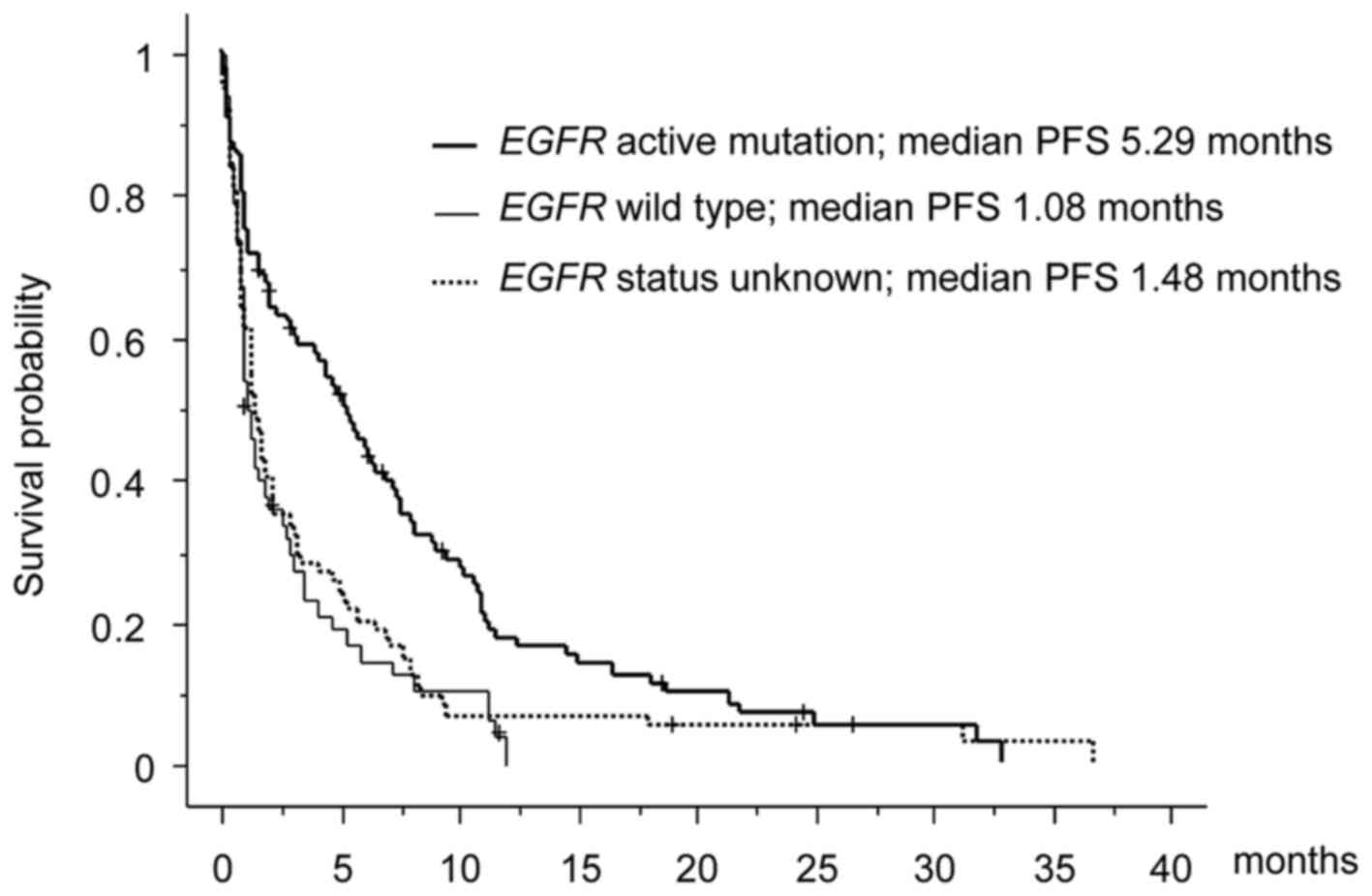
confidence interval (CI), 10.0–19.1%]. The median PFS and OS were
2.14 months (95% CI, 2.09–2.16 months) and 8.87 months (95% CI,
8.65–9.61 months), respectively. In a subset analysis, the PFS of
EGFR wild type and unknown status were 1.08 months and 1.48 months,
respectively, whereas the PFS of EGFR active mutation was
5.29 months (Fig. 1).
Analysis of the RR according to the
EGFR mutation status
According to the RECIST criteria, the RR of 95
patients with an EGFR mutation was 25% (24/43/28, PR/SD/PD;
95% CI, 15–34%). Conversely, the RR of 52 EGFR wild type and
75 unknown patients were 6% (3/25/24, PR/SD/PD; 95% CI, 1.3–15%)
and 5% (4/33/38, PR/SD/PD; 95% CI, 2.1–13%), respectively (Table II).
| Table II.Subset analysis of the EGFR mutation
status. |
Table II.
Subset analysis of the EGFR mutation
status.
|
|
| Response (%) |
|---|
|
|
|
|
|---|
| EGFR mutation
status | Gefitinib treatment
status | n=222 | CR | PR | SD | PD | RR | 95% CI (%) |
|---|
| Mutated | Total (Prior
gefitinib treatment) | 95 | 0 | 24 | 43 | 28 | 25 | 15–34 |
|
|
Yes | 50 | 0 | 7 | 29 | 14 | 14 | 7–26 |
|
| No | 45 | 0 | 17 | 14 | 14 | 38 | 25–52 |
| Wild type | Total (Prior
gefitinib treatment) | 52 | 0 | 3 | 25 | 24 | 6 | 1.3–15 |
|
|
Yes | 10 | 0 | 0 | 7 | 3 | 0 | – |
|
| No | 42 | 0 | 3 | 17 | 22 | 7 | 2–19 |
| Unknown | Total (Prior
gefitinib treatment) | 75 | 0 | 4 | 33 | 38 | 5 | 2.1–13 |
|
|
Yes | 32 | 0 | 2 | 18 | 12 | 6 | 2–20 |
|
| No | 43 | 0 | 2 | 15 | 26 | 5 | 1–15 |
Univariate and multivariate survival
analyses
To rule out potential cofounding interaction between
efficacy and other factors, the present study performed univariate
and multivariate analyses of the PFS. Kaplan-Meier analyses
compared by the log-rank test were used to calculate the effect of
the clinicopathological factors on the PFS (Table III). A univariate analysis
demonstrated that male gender [hazard ratio (HR) 1.63; P<0.001],
poor PS (PS 3 or 4; HR 1.75; P=0.028), current or former smoking
history (HR 1.64; P<0.001), prior regimens (2 or more) (HR 1.44;
P=0.036) and EGFR wild type or unknown (HR 2.09; P<0.001)
status significantly predicted a decreased PFS. Furthermore, a
multivariate analysis identified only EGFR mutation (HR
1.89; P<0.001) to be an independent prognostic factor for
PFS.
| Table III.Univariate and multivariate analyses
of factors associated with the progression-free survival (all
patients). |
Table III.
Univariate and multivariate analyses
of factors associated with the progression-free survival (all
patients).
| Variable | No. of
patients | Univariate hazard
ratio (95% CI) | P-value | Multivariate hazard
ratio (95% CI) | P-value |
|---|
| Gender |
|
| 0.0009 |
| 0.164 |
|
Male | 119 | 1.626
(1.219–2.169) |
| 1.333
(0.889–2.004) |
|
|
Female | 103 | 1 |
| 1 |
|
| ECOG performance
status |
|
| 0.0278 |
| 0.629 |
|
3–4 | 20 | 1.754
(1.063–2.894) |
| 1.635
(0.974–2.746) |
|
|
0–2 | 202 | 1 |
| 1 |
|
| Smoking
history |
|
| 0.0009 |
| 0.534 |
| Current
or former | 100 | 1.639
(1.225–2.192) |
| 1.142
(0.752–1.730) |
|
|
Never | 122 | 1 |
| 1 |
|
| Histological
type |
|
| 0.1370 |
|
|
|
Non-adenocarcinoma | 31 | 1.371
(0.904–2.079) |
|
|
|
|
Adenocarcinoma | 191 | 1 |
|
|
|
| Prior gefitinib
treatment |
|
| 0.3890 |
|
|
| No | 131 | 1.135
(0.851–1.515) |
|
|
|
|
Yes | 91 | 1 |
|
|
|
| Prior regimens |
|
| 0.0364 |
| 0.867 |
|
>2 | 164 | 1.438
(1.023–2.020) |
| 1.034
(0.701–1.529) |
|
|
0–1 | 58 | 1 |
| 1 |
|
| EGFR status |
|
| <0.0001 |
| <0.001 |
| Wild
type or unknown | 170 | 2.087
(1.548–2.814) |
| 1.892
(1.346–2.662) |
|
|
Mutation | 52 | 1 |
| 1 |
|
Association between the PFS and prior
gefitinib therapy
Of the 222 patients treated with erlotinib, 91
patients previously received gefitinib. To evaluate the potential
cofounding interaction between erlotinib and previous gefitinib
therapy, the present study performed univariate and multivariate
analyses of the PFS (Table III). A
univariate analysis demonstrated that non-adenocarcinoma (HR 4.78;
P=0.035) and poor response of gefitinib (HR 2.27; P=0.014)
significantly predicted a decreased PFS. However, the multivariate
analysis identified no association between the characteristics and
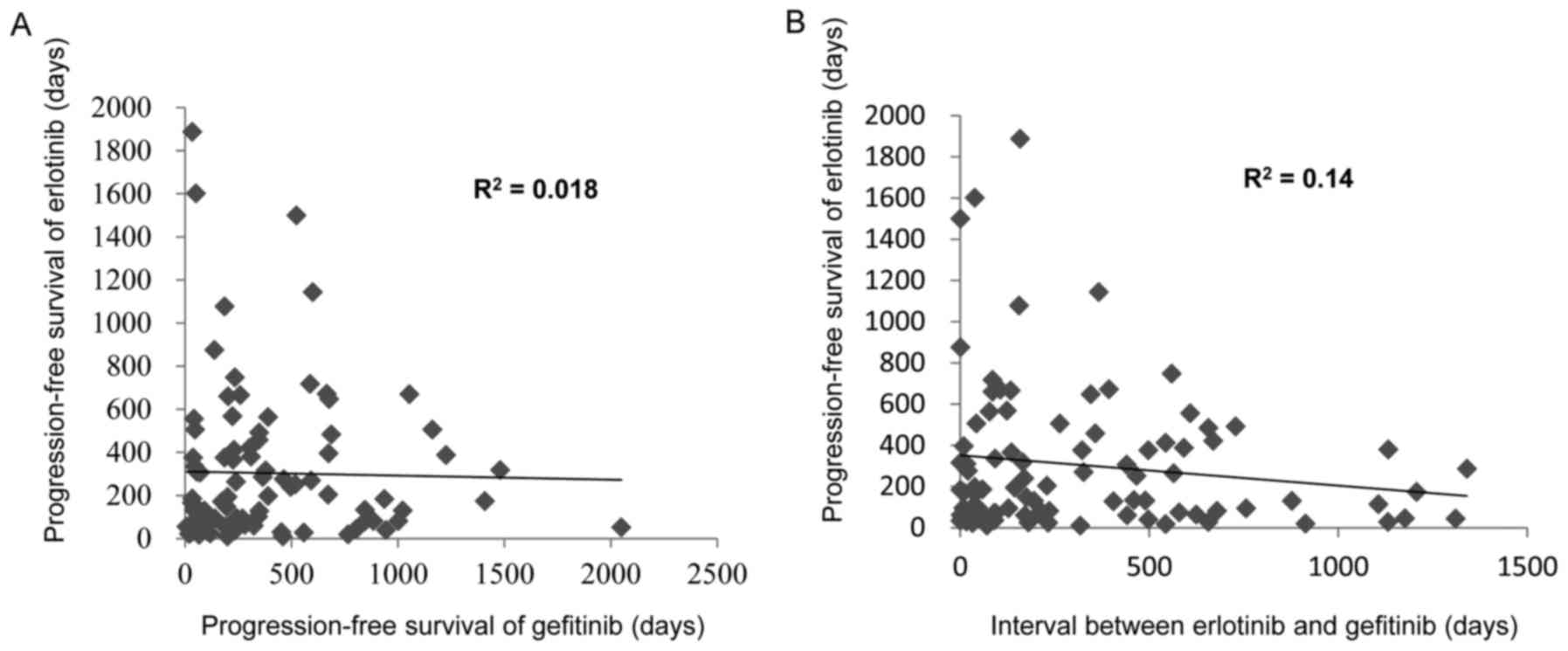
the PFS of erlotinib. Furthermore, as it was speculated that a
response to erlotinib treatment may be associated with a long
interval of a previous gefitinib therapy or a long duration from
erlotinib to gefitinib therapy, the present study investigated the
impact of a long disease control interval on the survival outcome
among patients treated with gefitinib who achieved ≥12 months PFS
(Table IV). However, no significant
correlation was detected between previous gefitinib therapy and the
PFS of erlotinib therapy (Fig.
2).
| Table IV.Univariate and multivariate analyses
of factors associated with the progression-free survival (patients
who received previous gefitinib treatment). |
Table IV.
Univariate and multivariate analyses
of factors associated with the progression-free survival (patients
who received previous gefitinib treatment).
| Variable | No. of
patients | Univariate hazard
ratio (95% CI) | P-value | Multivariate hazard
ratio (95% CI) | P-value |
|---|
| Gender |
|
| 0.235 |
|
|
|
Male | 24 | 1.342
(0.825–2.183) |
|
|
|
|
Female | 67 | 1 |
|
|
|
| ECOG performance
status |
|
| 0.587 |
|
|
|
3–4 | 9 | 1.226
(0.588–2.556) |
|
|
|
|
0–2 | 82 | 1 |
|
|
|
| Smoking
history |
|
| 0.615 |
|
|
| Current
or former | 31 | 1.123
(0.714–1.766) |
|
|
|
|
Never | 60 | 1 |
|
|
|
| Histological
type |
|
| 0.035 |
| 0.809 |
|
Non-adenocarcinoma | 2 | 4.784
(1.116–20.408) |
| 3.74
(0.850–16.393) |
|
|
Adenocarcinoma | 89 | 1 |
|
|
|
| Prior regimens |
|
| 0.125 |
|
|
|
>2 | 77 | 1.690
(0.864–3.303) |
|
|
|
|
0–1 | 14 | 1 |
|
|
|
| EGFR status |
|
| 0.388 |
|
|
| Wild
type or unknown | 41 | 1.210
(0.784–1.865) |
|
|
|
|
Mutation | 50 | 1 |
|
|
|
| Response of
gefitinib |
|
| 0.0139 |
| 0.249 |
| PD | 12 | 2.271
(1.181–4.365) |
| 2.141
(1.101–4.164) |
|
|
CR-SD | 79 | 1 |
|
|
|
| Duration of
gefitinib treatment |
|
| 0.6125 |
|
|
|
<12 | 58 | 1.122
(0.718–1.754) |
|
|
|
|
>12 | 33 | 1 |
|
|
|
| Interval between
gefitinib and erlotinib treatment |
|
| 0.429 |
|
|
|
<12 | 57 | 1.197
(0.766–1.871) |
|
|
|
|
>12 | 34 | 1 |
|
|
|
Discussion
At present, several EGFR TKIs are
commercially available for patients with EGFR mutations:
Gefitinib, erlotinib and afatinib (20). Erlotinib, an orally available EGFR
TKI, has proven to be effective as a second- or third-line
treatment for patients with NSCLC, regardless of the EGFR
mutation status (9). Additionally,
maintenance therapy with erlotinib for patients with NSCLC is
well-tolerated and significantly prolongs the PFS compared with
placebo (21). In these trials,
subgroup analyses of the PFS according to the clinical
characteristics also suggested an improved PFS with erlotinib
treatment compared with the placebo; this benefit was observed
irrespective of histology and EGFR mutation status. However,
erlotinib was compared with BCS or placebo for unselected patients
with NSCLC, which included patients with wild type EGFR in
the BR.21 and Sequential Tarceva in Unresectable NSCLC trials
(9,21).
As the benefit of EGFR TKIs varies widely between
patients with EGFR mutations and those with wild type
EGFR, it is crucial to establish which second- or third-line
treatment is preferable, particularly for patients with wild type
EGFR (22). The TAILOR phase
III trial, conducted to compare erlotinib with docetaxel in
patients who failed first-line platinum-based chemotherapy and who
had EGFR wild type, demonstrated that chemotherapy was more
effective compared with erlotinib for the second-line treatment for
previously treated patients with NSCLC with EGFR wild type
(16). Erlotinib had low efficacy for
patients with wild type EGFR compared with patients who had
EGFR active mutations. In addition, the effectiveness of
erlotinib subsequent to gefitinib therapy remains
controversial.
The present study analyzed the characteristics of
222 patients according to the response to erlotinib. The
multivariate analysis revealed that the EGFR mutation status
(with active mutation) was only associated with a longer PFS and
good response to erlotinib treatment. Patients with wild type
EGFR or unknown status had a poor PFS (1.1 and 1.5 months,
respectively) and RR (6 and 5%, respectively). Similarly, the
TAILOR phase III trial, which compared erlotinib with standard
chemotherapy in patients with wild type EGFR as second-line
chemotherapy, demonstrated that the RR of erlotinib in wild type
EGFR patients was 3–5.6%, whereas that of standard
chemotherapy was 10.3–20% (16). In
addition, a randomized phase III trial (Docetaxel and Erlotinib
Lung cancer trial) of erlotinib vs. docetaxel in Japanese patients
with advanced NSCLC who had an EGFR wild type status
demonstrated the poor effectiveness of erlotinib as a second or
third-line therapy. The RR of chemotherapy for patients with NSCLC
as a second-line therapy was 7.1–22.7% (23–25). The
present study therefore considered erlotinib to be invalid for
patients with NSCLC with wild type EGFR as a second or
third-line therapy.
The current study analyzed the characteristics of 95
patients according to the response and interval time on erlotinib
subsequent to gefitinib failure. In these patients, a significantly
altered response following erlotinib therapy was observed in
patients who had exhibited SD for a long period of time during
gefitinib treatment. Thus, it appeared that erlotinib is a
potential therapeutic option for the treatment of patients with
advanced NSCLC with wild type EGFR who had SD while
receiving gefitinib, as previously suggested (26). However, there was no association
between the erlotinib and gefitinib treatments. The predictive
factor of erlotinib subsequent to gefitinib therapy was associated
with the EGFR mutation status alone.
Although the PFS was markedly improved with EGFR TKI
treatment compared with chemotherapy in such EGFR mutated
patients, patients who had initially responded to EGFR TKI
treatment eventually relapsed (27).
This acquired resistance to EGFR TKI treatment may be linked to a
number of molecular mechanisms, including secondary mutations in
the EGFR gene coding for the intracellular kinase domain of
this receptor, a T790M mutation and other factors, including
MET amplification and hepatocyte growth factor
overexpression (28–30). Thus, oncologists may consider a repeat
biopsy prior to retreatment with EGFR TKI subsequent to the initial
EGFR TKI failure.
In conclusion, the efficacy of erlotinib therapy was
closely associated with the EGFR mutation status. Erlotinib
treatment is therefore considered to be limited for patients with
NSCLC with EGFR mutations, at least as a second or
third-line therapy.
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J,
Murray T and Thun MJ: Cancer statistics, 2008. CA Cancer J Clin.
58:71–96. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Potosky AL, Saxman S, Wallace RB and Lynch
CF: Population variations in the initial treatment of
non-small-cell lung cancer. J Clin Oncol. 22:3261–3268. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ramalingam S and Belani C: Systemic
chemotherapy for advanced non-small cell lung cancer: Recent
advances and future directions. Oncologist. 13 Suppl 1:S5–S13.
2008. View Article : Google Scholar
|
|
4
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rosell R, Carcereny E, Gervais R, Gervais
R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, et al: Erlotinib versus standard chemotherapy as
first-line treatment for European patients with advanced EGFR
mutation-positive non-small-cell lung cancer (EURTAC): A
multicentre, open-label, randomised phase 3 trial. Lancet Oncol.
13:239–246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sandler A, Gray R, Perry MC, Brahmer J,
Schiller JH, Dowlati A, Lilenbaum R and Johnson DH:
Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med. 355:2542–2550. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH; Eastern
Cooperative Oncology Group, : Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ohe Y, Ohashi Y, Kubota K, Tamura T,
Nakagawa K, Negoro S, Nishiwaki Y, Saijo N, Ariyoshi Y, Fukuoka M,
et al: Randomized phase III study of cisplatin plus irinotecan
versus carboplatin plus paclitaxel, cisplatin plus gemcitabine, and
cisplatin plus vinorelbine for advanced non-small-cell lung cancer:
Four-Arm Cooperative Study in Japan. Ann Oncol. 18:317–323. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shepherd FA, Pereira J Rodrigues, Ciuleanu
T, Tan EH, Hirsh V, Thongprasert S, Campos D, Maoleekoonpiroj S,
Smylie M, Martins R, et al: Erlotinib in previously treated
non-small-cell lung cancer. N Engl J Med. 353:123–132. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pao W, Miller V, Zakowski M, Doherty J,
Politi K, Sarkaria I, Singh B, Heelan R, Rusch V, Fulton L, et al:
EGF receptor gene mutations are common in lung cancers from ‘never
smokers’ and are associated with sensitivity of tumors to gefitinib
and erlotinib. Proc Natl Acad Sci USA. 101:pp. 13306–13311. 2004;
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Paez JG, Jänne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Garassino MC, Martelli O, Broggini M,
Farina G, Veronese S, Rulli E, Bianchi F, Bettini A, Longo F,
Moscetti L, et al: Erlotinib versus docetaxel as second-line
treatment of patients with advanced non-small-cell lung cancer and
wild-type EGFR tumours (TAILOR): A randomised controlled trial.
Lancet Oncol. 14:981–988. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Postmus PE, Brambilla E, Chansky K,
Crowley J, Goldstraw P, Patz EF Jr and Yokomise H: International
Association for the Study of Lung Cancer International Staging
Committee; Cancer Research and Biostatistics; Observers to the
Committee; Participating Institutions: The IASLC lung cancer
staging project: Proposals for revision of the M descriptors in the
forthcoming (seventh) edition of the TNM classification of lung
cancer. J Thorac Oncol. 2:686–693. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zubrod CG, Ipsen J, Frei E, Lc, Lipsett
Mb, Gehan E Lasagna and Escher Gc: Newer techniques and some
problems in cooperative group studies. Natl Cancer Inst Monogr.
3:277–292. 1960.PubMed/NCBI
|
|
20
|
Lee CK, Brown C, Gralla RJ, Hirsh V,
Thongprasert S, Tsai CM, Tan EH, Ho JC, Chu da T, Zaatar A, et al:
Impact of EGFR inhibitor in non-small cell lung cancer on
progression-free and overall survival: A meta-analysis. J Natl
Cancer Inst. 105:595–605. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cappuzzo F, Ciuleanu T, Stelmakh L,
Cicenas S, Szczésna A, Juhász E, Esteban E, Molinier O, Brugger W,
Melezínek I, et al: Erlotinib as maintenance treatment in advanced
non-small-cell lung cancer: A multicentre, randomised,
placebo-controlled phase 3 study. Lancet Oncol. 11:521–529. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Laurie SA and Goss GD: Role of epidermal
growth factor receptor inhibitors in epidermal growth factor
receptor wild-type non-small-cell lung cancer. J Clin Oncol.
31:1061–1069. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shepherd FA, Dancey J, Ramlau R, Mattson
K, Gralla R, O'Rourke M, Levitan N, Gressot L, Vincent M, Burkes R,
et al: Prospective randomized trial of docetaxel versus best
supportive care in patients with non-small-cell lung cancer
previously treated with platinum-based chemotherapy. J Clin Oncol.
18:2095–2103. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fossella FV, DeVore R, Kerr RN, Crawford
J, Natale RR, Dunphy F, Kalman L, Miller V, Lee JS, Moore M, et al:
Randomized phase III trial of docetaxel versus vinorelbine or
ifosfamide in patients with advanced non-small-cell lung cancer
previously treated with platinum-containing chemotherapy regimens.
The TAX 320 non-small cell lung cancer study group. J Clin Oncol.
18:2354–2362. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kudoh S, Takeda K, Nakagawa K, Takada M,
Katakami N, Matsui K, Shinkai T, Sawa T, Goto I, Semba H, et al:
Phase III study of docetaxel compared with vinorelbine in elderly
patients with advanced non-small-cell lung cancer: Results of the
West Japan Thoracic Oncology Group Trial (WJTOG 9904). J Clin
Oncol. 24:3657–3663. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cho BC, Im CK, Park MS, Kim SK, Chang J,
Park JP, Choi HJ, Kim YJ, Shin SJ, Sohn JH, et al: Phase II study
of erlotinib in advanced non-small-cell lung cancer after failure
of gefitinib. J Clin Oncol. 25:2528–2533. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Remon J, Morán T, Majem M, Reguart N,
Dalmau E, Márquez-Medina D and Lianes P: Acquired resistance to
epidermal growth factor receptor tyrosine kinase inhibitors in
EGFR-mutant non-small cell lung cancer: A new era begins. Cancer
Treat Rev. 40:93–101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yun CH, Mengwasser KE, Toms AV, Woo MS,
Greulich H, Wong KK, Meyerson M and Eck MJ: The T790M mutation in
EGFR kinase causes drug resistance by increasing the affinity for
ATP. Proc Natl Acad Sci USA. 105:pp. 2070–2075. 2008; View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bean J, Brennan C, Shih JY, Riely G, Viale
A, Wang L, Chitale D, Motoi N, Szoke J, Broderick S, et al: MET
amplification occurs with or without T790M mutations in EGFR mutant
lung tumors with acquired resistance to gefitinib or erlotinib.
Proc Natl Acad Sci USA. 104:pp. 20932–20937. 2007; View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yano S, Wang W, Li Q, Matsumoto K,
Sakurama H, Nakamura T, Ogino H, Kakiuchi S, Hanibuchi M, Nishioka
Y, et al: Hepatocyte growth factor induces gefitinib resistance of
lung adenocarcinoma with epidermal growth factor
receptor-activating mutations. Cancer Res. 68:9479–9487. 2008.
View Article : Google Scholar : PubMed/NCBI
|