Introduction
Urothelial carcinoma of the bladder is the second
most common malignancy of the genitourinary tract, the ninth most
common cancer and the fourteenth leading cause of mortality due to
cancer in the world (1).
Approximately 70% of all bladder cancers are non-muscle invasive
bladder cancer (NMIBC) (2). Long-term
follow-up of low-grade Ta tumors shows a progression rate of ~6%,
whereas high-grade T1 tumors exhibit a greater rate of progression,
namely ~17% (3,4). Disease progression frequently results in
an unfavorable clinical outcome following progression to
muscle-invasive tumor or development of distant metastases
(3,4).
Conventional clinicopathological factors predicting disease
progression include number of tumors, tumor diameter, stage,
concomitant carcinoma in situ and tumor grade (2). However, the prediction of progression
remains difficult based on conventional parameters, and to date, no
useful biomarkers have been established for follow-up in routine
practice (5).
DNA copy number variations (CNVs) involve gains or
losses of several to hundreds kb of genomic DNA among
phenotypically normal individuals, and ≥291,801 CNV regions have
been identified to date (6). Recent
studies have described germline CNVs as potential susceptibility
loci for a range of diseases, including infectious, autoimmune and
neuropsychiatric diseases (7–10). Concerning malignancies, CNVs have
recently been reported as markers predisposing individuals to
neuroblastoma, prostate cancer, pancreatic cancer, colorectal
cancer, ovarian cancer and breast cancer risk (11–16).
However, the significance of CNVs in NMIBC remains unclear.
Therefore, the present study investigated the association between
CNVs and disease progression in NMIBC. To the best of our
knowledge, the present report is the first to confirm CNV as a
potential biomarker for assessing disease progression in NMBC.
Materials and methods
Patients
The study group comprised 189 patients who underwent
transurethral resection of bladder tumor (TURBT) and were
histopathologically diagnosed with pTa and pT1 (N0M0) urothelial
carcinoma of the bladder based on the tumor-node-metastasis
classification of the International Union Against Cancer (2002) at
the first documented diagnosis (17).
The patients were followed up from April 2004 to December 2012 at
Yamaguchi University Hospital (Ube, Japan). Written informed
consent was obtained from each patient. The present study was
performed according to the Declaration of Helsinki, and the
procedures were approved by the Ethics Committee of Yamaguchi
University.
Venous blood samples were collected from each
patient, and the original medical records were retrospectively
reviewed for collecting data. Tumor grade was classified according
to the World Health Organization classification system (1973)
(18). The patients' characteristics
are summarized in Table I. Patients
who underwent TURBT were followed up every 3 months by cystoscopic
examination and urine cytology, whereas those with high-risk NMIBC
were followed up by computerized tomography scan every year, with a
median follow-up period of 81.4 months (range, 1.7–301.9 months).
Disease progression was defined when either the recurrent tumor had
progressed to muscle-invasive tumor or when development of distant
metastases had occurred.
 | Table I.Patients' demographics and
pathological background. |
Table I.
Patients' demographics and
pathological background.
| Factor | No. (%) |
|---|
| Sex |
|
| Male | 160 (84.7) |
|
Female | 29 (15.3) |
| Tumor grade |
|
| 1 | 17 (9.0) |
| 2 | 67 (35.4) |
| 3 | 105 (55.6) |
| pT stage |
|
|
pTa | 84 (44.4) |
|
pT1 | 105 (55.6) |
| Concurrent CIS |
|
| No | 122 (64.5) |
|
Yes | 67 (35.5) |
| Cytology |
|
|
Negative | 79 (41.8) |
|
Positive | 110 (58.2) |
| Recurrence |
|
| No | 88 (46.6) |
|
Yes | 101 (53.4) |
| Disease
progression |
|
| No | 157 (83.1) |
|
Yes | 32 (16.9) |
|
Local | 9 (4.8) |
|
Distant | 23 (12.2) |
Array comparative genomic
hybridization (GCH) assay and data analysis
A total of 67 DNA samples were obtained from the
peripheral blood of individuals without a history of human
malignancies, including bladder cancer (healthy controls), and 18
DNA samples were obtained from the peripheral blood of patients
with a history of NMIBC (6 pTa and 12 pT1). The pathological grades
were 1, 2 and 3 for 3, 5 and 10 tumors, respectively. A pool of
blood-derived DNA from 30 healthy individuals was used as a
reference sample for all the hybridizations performed. The mean age
and sex ratio were almost identical in the control and NMIBC
patient groups. Assessment of CNVs in the human genome by
oligonucleotide array CGH assay (NimbleGen Human CGH 2.1M
Whole-Genome Tiling v2.0D Array; Roche Diagnostics, Indianapolis,
IN, USA) was performed according to the manufacturer's standard
protocol. Array image analysis and data normalization were
performed with NimbleScan version 2.5 software (Roche Diagnostics).
The normalized data were then processed using Nexus Copy Number
version 5.0 software (BioDiscovery, Inc., El Segundo, CA, USA) as
previously described (16).
Quantitative polymerase chain reaction
(qPCR) and data analysis
qPCR was performed using predesigned
TaqMan® Copy Number Assays (Applied Biosystems; Thermo
Fisher Scientific, Inc., Waltham, MA, USA) containing a primer pair
and a fluorescein amidite dye-labeled minor groove binder probe was
performed to detect the copy number of the genomic sequence. Copy
number assay identity is described in Table II. For the internal control, a
predesigned TaqMan® Copy Number Reference Assay RNase P
(Applied Biosystems; Thermo Fisher Scientific, Inc.), was used. A
total of 189 DNA samples were obtained from the peripheral blood of
patients with a history of NMIBC. The calibrator sample for qPCR
was the DNA pooled from the 30 healthy volunteers, which was also
used as the reference in the array CGH assay, and the copy number
of the calibrator sample was assumed to be 2. The 7900HT Fast
Real-Time PCR System (Applied Biosystems; Thermo Fisher Scientific,
Inc.) and the StepOnePlus Real-Time PCR System (Applied Biosystems;
Thermo Fisher Scientific, Inc.) were used for qPCR analysis. The
PCRs were carried out according to the manufacturer's standard
protocol using the comparative 2−ΔΔCq method, as
previously described (16).
| Table II.CNV markers associated with bladder
cancer risk. |
Table II.
CNV markers associated with bladder
cancer risk.
| Location
(GRCh37/hg19) | Cytoband | Gene | CNV assay ID | CNV |
P-valuea | Bonferroni |
|---|
|
chr2:72,218,053–72,222,026 | p13.3 | CYP26B1 | Hs05873524_cn | Gain | <0.0001 | 0.0149 |
|
chr2:101,678,677–101,683,846 | q11.2 | MAP4K4 | Hs02074840_cn | Loss | <0.0001 | 0.0040 |
|
chr7:1,237,863–1,240,528 | p22.3 | UNCX | Hs03622829_cn | Loss | <0.0001 | 0.0384 |
|
chr8:61,752,169–61,756,537 | q12.2 | CHD7 | Hs02866323_cn | Loss | <0.0001 | 0.0149 |
|
chr10:64,949,973–64,952,473 | q21.3 | REEP3 | Hs00735097_cn | Loss | <0.0001 | 0.0002 |
|
chr11:256,350–257,345 | p15.5 | Non-coding region
of the genome | Hs03791448_cn | Loss | <0.0001 | 0.0331 |
|
chr14:50,365,069–50,365,879 | q22.1 | NIN | Hs07054232_cn | Loss | <0.0001 | <0.0001 |
|
chr15:57,515,723–57,519,569 | q22.2 | FAM81A | Hs59732286_cn | Loss | <0.0001 | 0.0012 |
|
chr15:99,843,944–99,844,859 | q26.3 | PCSK6 | Hs03899300_cn | Loss | <0.0001 | 0.0040 |
|
chr16:45,732,422–45,736,896 | q12.1 | NETO2 | Hs02817425_cn | Loss | <0.0001 | 0.0012 |
|
chr19:35,123,405–35,132,171 | q12 | C19orf2 | Hs07125447_cn | Loss | <0.0001 | <0.0001 |
Statistical analysis
Statistical analysis was performed using JMP
(version 13) statistical software (SAS Institute, Inc., Cary, NC,
USA). The Fisher's exact test (Tables
II and III) and an unpaired
t-test (Fig. 1) were applied to
compare variables. CNV markers detected by array CGH assay were
calculated using Fisher's exact test and the Bonferroni correction.
The probability of survival was calculated by the Kaplan-Meier
estimator method, and statistical differences were evaluated by the
log-rank test. Categorical variables influencing progression-free
survival were compared using Cox proportional hazards regression
models. Variables with P<0.05 in univariate analysis were also
assessed for their association with progression-free survival in
multivariate analysis. For all of the statistical tests, P<0.05
was considered to indicate a statistically significant
difference.
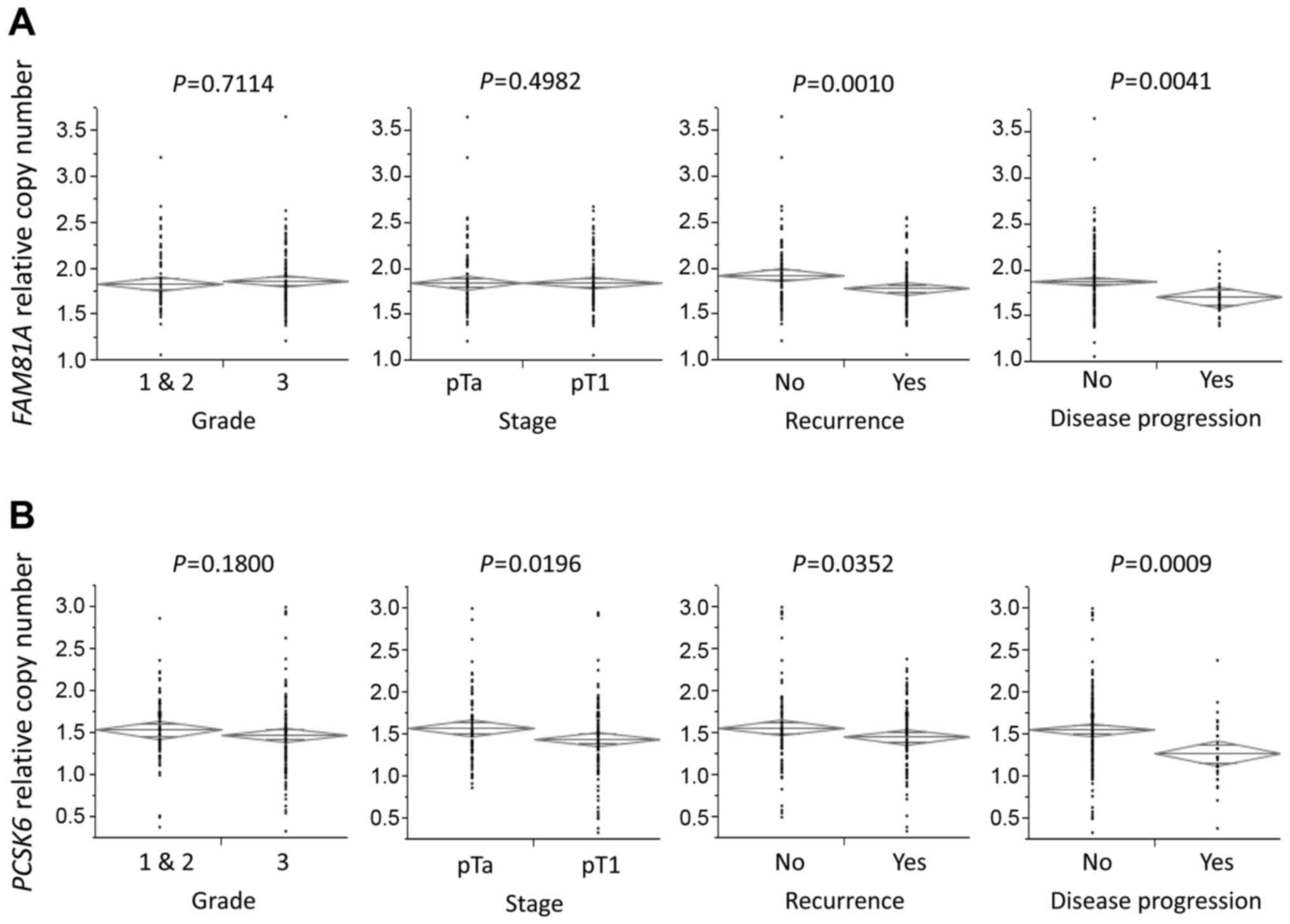 | Figure 1.Association of tumor grade, stage,
recurrence, disease progression and serum sodium levels with
FAM81A or PCSK6 relative copy numbers. (A) Patients
with recurrence and disease progression had significantly lower
FAM81A relative copy number than those without recurrence
and disease progression (P=0.0010 and P=0.0041, respectively). (B)
Patients with pT1 stage, recurrence and disease progression had
significantly lower PCSK6 relative copy number than those
without pT1 stage, recurrence and disease progression (P=0.0196,
P=0.0352 and P=0.0009, respectively). The diamonds show the mean
(long horizontal line) and 95% confidence interval of the relative
copy number. (C) Patients with lower PCSK6 copy number had
significantly higher sodium levels in blood than those with higher
PCSK6 copy number (P=0.0165). (D) A positive correlation
between PCSK6 relative copy number and serum sodium levels
was identified in linear regression analysis (P=0.0162).
FAM81A, family with sequence similarity 81 member A;
PCSK6, proprotein convertase subtilisin/kexin type 6. |
| Table III.Correlation of several variables with
FAM81A or PCSK6 CNV. |
Table III.
Correlation of several variables with
FAM81A or PCSK6 CNV.
|
| FAM81A
CNV |
| PCSK6
CNV |
|
|---|
|
|
|
|
|
|
|---|
| Factor | <1.77 | ≥1.77a | P-value | <1.33 |
>1.33a | P-value |
|---|
| Tumor grade |
|
|
|
|
|
|
| 1 &
2 | 41 | 32 | 0.1380 | 19 | 54 | 0.0606 |
| 3 | 52 | 64 |
| 46 | 70 |
|
| pT stage |
|
|
|
|
|
|
|
pTa | 46 | 38 | 0.1896 | 22 | 62 | 0.0449 |
|
pT1 | 47 | 58 |
| 43 | 62 |
|
| Recurrence |
|
|
|
|
|
|
| No | 37 | 51 | 0.0803 | 26 | 62 | 0.2206 |
|
Yes | 56 | 45 |
| 39 | 62 |
|
| Disease
progression |
|
|
|
|
|
|
| No | 70 | 87 | 0.0062 | 45 | 112 | 0.0004 |
|
Yes | 23 | 9 |
| 20 | 12 |
|
Results
CNV markers are associated with
bladder cancer risk
Using array CGH assay, 11 CNV regions with
significant differences in the frequency of copy number changes
between the NMIBC patient group and the control group were
identified. The CNV regions reached significance by Bonferroni
correction. Therefore, it can be speculated that these regions may
involve candidate genes associated with NMIBC risk (Table II).
Association of CNVs with several
variables
A case-case study was carried out by qPCR to
evaluate the association of the above 11 CNVs with recurrence and
disease progression in the present 189 NMIBC cases. Notably, family
with sequence similarity 81 member A (FAM81A) and proprotein
convertase subtilisin/kexin type 6 (PCSK6) copy numbers,
according to these 11 CNVs, exhibited a significant association
with recurrence and disease progression in NMIBC (Fig. 1). Another CNV lesion (CYP26B1,
MAP4K4, UNCX, CHD7, REEP3, NIN, NETO2 and C19orf2)
exhibited a non-significant association with recurrence and disease
progression. Therefore, the association between FAM81A and
PCSK6 copy numbers and clinicopathological parameters was
reviewed. No significant differences were observed in FAM81A copy
number between patients with pT1 stage and those with pTa
(P=0.4982; Fig. 1A); however,
patients with pT1 stage had a significantly lower PCSK6
relative copy number than those with pTa (P=0.0196; Fig. 1B).
The threshold values of CNVs were set based on the
area under the curve (AUC) from the receiver operating
characteristic curve for disease progression. The AUC of
FAM81A and PCSK6 copy numbers at 1.77 and 1.33
threshold values was 0.65 and 0.70, respectively, with a
sensitivity of 71.9 and 65.6%, and a specificity of 55.4 and 73.9%,
respectively. In those copy number thresholds, the FAM81A
and PCSK6 copy numbers were significantly associated with
disease progression (P=0.0062 and P=0.0004, respectively; Table III). PCSK6 copy number was
also significantly associated with pT stage (P=0.0449; Table III).
PCSK6 has been reported to regulate sodium
homeostasis (19). Therefore, the
present study investigated the association between PSCK6 and
sodium concentration. Patients with lower PCSK6 copy number
had significantly higher serum sodium levels than those with higher
PCSK6 copy number (P=0.0330; Fig.
1C). A positive correlation between PCSK6 copy number
and serum sodium concentration was identified in linear regression
analysis (P=0.0162; Fig. 1D).
Univariate and multivariate analyses
of disease progression
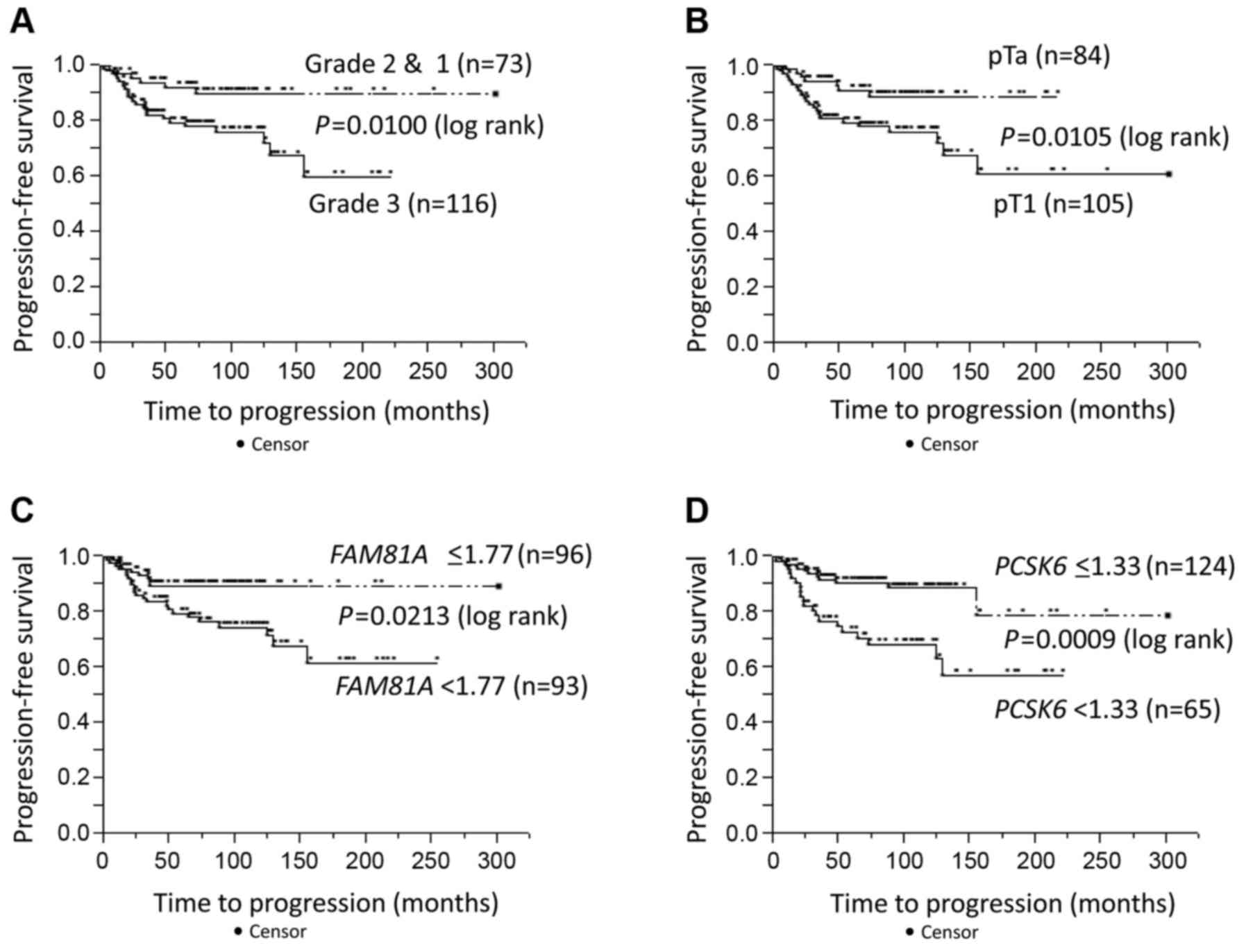
Progression-free survival was evaluated in the
context of pathological data and CNVs. Univariate Cox proportional
hazards regression analysis revealed that tumor grade (P=0.0067),
pT stage (P=0.0079), urine cytology (P=0.0041), and FAM81A
(P=0.0190) and PCSK6 (P=0.0013) copy numbers had a
significant effect on progression-free survival (Table IV). Progression-free survival rates
were plotted using Kaplan-Meier survival curves (Fig. 2). Tumor grade and stage, and
FAM81A and PCSK6 copy numbers were significant
prognostic factors for disease-specific survival (P=0.0100,
P=0.0105, P=0.0213 and P=0.0009, respectively; log-rank test;
Fig. 2A-D). In multivariate analyses,
PCSK6 copy number was an independent prognostic factor for
progression-free survival (P=0.0456; risk ratio, 2.17; 95%
confidence interval, 1.02–4.82; Table
IV).
| Table IV.Cox proportional hazard model for
progression-free survival in non-muscle invasive bladder
cancer. |
Table IV.
Cox proportional hazard model for
progression-free survival in non-muscle invasive bladder
cancer.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Factor | Category | Risk ratio (95%
CI) | P-value | Risk ratio (95%
CI) | P-value |
|---|
| Tumor grade | Grade 3 vs. 1 &
2 | 3.04
(1.34–8.16) | 0.0067 | 1.62
(0.56–5.33) | 0.3866 |
| pT stage | pT1 vs.
pTa | 2.85
(1.30–7.14) | 0.0079 | 1.67
(0.63–5.09) | 0.3168 |
| Concurrent CIS | Yes vs.
no | 1.51
(0.74–3.03) | 0.2489 |
|
|
| Cytology |
Negative vs. positive | 3.22
(1.42–8.65) | 0.0041 | 2.05
(0.85–5.77) | 0.1126 |
| FAM81A
CNV |
<1.77 vs. ≥1.77 | 2.42
(1.15–5.53) | 0.0190 | 1.93
(0.86–4.66) | 0.1110 |
| PCSK6
CNV |
<1.33 vs. ≥1.33 | 3.15
(1.56–6.64) | 0.0013 | 2.17
(1.02–4.82) | 0.0456 |
Discussion
Since treatment modalities for NMIBC patients vary
from simple transurethral resection in low-risk NMIBC patients to
recommendation of radical cystectomy in high-risk NMIBC patients,
the prediction of biological characteristics of disease progression
in individual patients, including invasiveness and metastatic
potential, are markedly important for selecting the most
appropriate treatment (5). Due to the
limited prediction abilities of conventional markers such as tumor
grade or stage (2,5), the identification of reliable genetic
markers predicting disease progression in NMIBC is urgently
required.
Previous reports demonstrated the association
between CNVs and the risk of several human malignancies (11–16).
PCSK6 is a member of the protease family of proprotein
convertases, which activate precursor proteins by cleaving at the
specific recognition sequence RXK/RR (20). PCSK6 is important for
maintaining sodium homeostasis and normal blood pressure (19). Although PCSK6 has been reported
to regulate cell proliferation and tumor progression in breast and
prostate cancer (21–23), the exact association between
PCSK6 expression and carcinogenesis is controversial. In an
experimental model, the overexpression of PCSK6 in
immortalized non-tumorigenic or papilloma-derived keratinocytes
increased their invasiveness (24),
whereas absent or reduced PCSK6 expression was linked to
ovarian cancer (25). Reduced
germline copy number of PCSK6 was also reported to be
associated with breast cancer risk (16). These reports may support the present
data that reduced copy number of germline PCSK6 may confer
tumor aggressiveness, thus leading to poor disease progression in
NMIBC. In addition, a significant reverse correlation between
PCSK6 copy number and serum sodium levels was identified in
the present study. Since PCSK6 regulates sodium homeostasis,
this correlation implies a functional relevance due to gene dosage.
The function of a reduced copy number of PCSK6 in normal
human cells has not been investigated yet. PCSK6 affects
sodium homeostasis; however, this mechanism may be different from
tumor progression through PCSK6. The function of
FAM81A remains unknown, and there are no reports about
FAM81A CNVs. Further studies may be required on the function
and significance of PCSK6 and FAM81A CNVs in human
malignancies.
In the present study, FAM81A and PCSK6
copy numbers in NMIBC were lower than those in healthy human
volunteers, as shown by qPCR (Fig.
1). These data support and validate the data detected by array
CGH. Our hypothesis proposed that several candidate genes linked to
bladder cancer risk may also affect tumor aggressiveness, thus
leading to tumor progression. The present study aimed to determine
the prognostic value of CNVs for NMIBC rather than to detect CNVs
associated with bladder cancer susceptibility. However, further
studies on the association between FAM81A and PCSK6
copy numbers with NMIBC risk may be required to compare a larger
sample size of NMIBC cases with healthy volunteers in order to
determine CNVs associated with bladder cancer susceptibility.
The present study is constrained by several
limitations. First, it is a retrospective study with a limited
number of patients. Second, the patients in the present study
underwent TURBT by several surgeons over a long time period. Thus,
prospective studies including a larger sample size are required to
confirm the predictive significance of CNVs in NMIBC. Third, there
is a possibility of false positive results in array CGH analysis.
CNVs detected by array CGH assay harbor false positives due to a
poor signal-to-noise ratio of hybridizations, which leads to
considerable variation in the reported CGH ratio (16). Therefore, qPCR with a larger cohort
should be carried out to confirm the CNVs that appeared to be
associated with bladder cancer susceptibility.
In conclusion, PCSK6 copy number is an
independent predictor of progression-free survival in NMIBC.
PCSK6 copy number may have significant potential as a
biomarker for estimating disease progression in NMIBC patients
treated by TURBT, and may help to select patients with NMIBC who
may benefit from more aggressive treatment, including radical
cystectomy.
Acknowledgements
The authors thank Mrs. Kiyomi Fujita (Department of
Urology, Graduate School of Medicine, Yamaguchi University) for her
technical assistance.
References
|
1
|
Mahdavifar N, Ghoncheh M, Pakzad R,
Momenimovahed Z and Salehiniya H: Epidemiology, incidence and
mortality of bladder cancer and their relationship with the
development index in the world. Asian Pac J Cancer Prev.
17:381–386. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van Rhijn BW, Burger M, Lotan Y, Solsona
E, Stief CG, Sylvester RJ, Witjes JA and Zlotta AR: Recurrence and
progression of disease in non-muscle-invasive bladder cancer: From
epidemiology to treatment strategy. Eur Urol. 56:430–442. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Leblanc B, Duclos AJ, Bénard F, Côté J,
Valiquette L, Paquin JM, Mauffette F, Faucher R and Perreault JP:
Long-term followup of initial Ta grade 1 transitional cell
carcinoma of the bladder. J Urol. 162:1946–1950. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Palou J, Sylvester RJ, Faba OR, Parada R,
Peña JA, Algaba F and Villavicencio H: Female gender and carcinoma
in situ in the prostatic urethra are prognostic factors for
recurrence, progression, and disease-specific mortality in T1G3
bladder cancer patients treated with bacillus Calmette-Guerin. Eur
Urol. 62:118–125. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Babjuk M, Böhle A, Burger M, Capoun O,
Cohen D, Compérat EM, Hernández V, Kaasinen E, Palou J, Rouprêt M,
et al: EAU guidelines on non-muscle-invasive urothelial carcinoma
of the bladder: Update 2016. Eur Uro. 71:447–461. 2017. View Article : Google Scholar
|
|
6
|
Suehiro Y, Furuya T, Sasaki K and Hinota
Y: DNA polymorphisms. Rinsho Byori. 61:1001–1007. 2013.(In
Japanese). PubMed/NCBI
|
|
7
|
Shlien A and Malkin D: Copy number
variations and cancer. Genome Med. 1:622009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wain LV, Armour JA and Tobin MD: Genomic
copy number variation, human health, and disease. Lancet.
374:340–350. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang F, Gu W, Hurles ME and Lupski JR:
Copy number variation in human health, disease, and evolution. Annu
Rev Genomics Hum Genet. 10:451–481. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fanciulli M, Petretto E and Aitman TJ:
Gene copy number variation and common human disease. Clin Genet.
77:201–213. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Diskin SJ, Hou C, Glessner JT, Attiyeh EF,
Laudenslager M, Bosse K, Cole K, Mossé YP, Wood A, Lynch JE, et al:
Copy number variation at 1q21.1 associated with neuroblastoma.
Nature. 459:987–991. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu W, Sun J, Li G, Zhu Y, Zhang S, Kim
ST, Sun J, Wiklund F, Wiley K, Isaacs SD, et al: Association of a
germ-line copy number variation at 2p24.3 and risk for aggressive
prostate cancer. Cancer Res. 69:2176–2179. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lucito R, Suresh S, Walter K, Pandey A,
Lakshmi B, Krasnitz A, Sebat J, Wigler M, Klein AP, Brune K, et al:
Copy-number variants in patients with a strong family history of
pancreatic cancer. Cancer Biol Ther. 6:1592–1599. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Thean LF, Loi C, Ho KS, Koh PK, Eu KW and
Cheah PY: Genome-wide scan identifies a copy number variable region
at 3q26 that regulates PPM1L in APC mutation-negative familial
colorectal cancer patients. Genes Chromosomes Cancer. 49:99–106.
2010.PubMed/NCBI
|
|
15
|
Yoshihara K, Tajima A, Adachi S, Quan J,
Sekine M, Kase H, Yahata T, Inoue I and Tanaka K: Germline copy
number variations in BRCA1-associated ovarian cancer patients.
Genes Chromosomes Cancer. 50:167–177. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Suehiro Y, Okada T, Shikamoto N, Zhan Y,
Sakai K, Okayama N, Nishioka M, Furuya T, Oga A, Kawauchi S, et al:
Germline copy number variations associated with breast cancer
susceptibility in a Japanese population. Tumour Biol. 34:947–952.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sobin LH, Gospodarowicz M and Wittekind C:
TNM classification of malignant tumors. 7th. UICC International
Union Against Cancer; pp. 262–265. 2009
|
|
18
|
Mostofi FK, Sobin LH and Torloni H:
Histologic typing of urinary bladder tumorsInternational
Histological Classification of Tumors. No. 10. World Health
Organization; Geneva: 1973
|
|
19
|
Chen S, Cao P, Dong N, Peng J, Zhang C,
Wang H, Zhou T, Yang J, Zhang Y, Martelli EE, et al: PCSK6-mediated
corin activation is essential for normal blood pressure. Nat Med.
21:1048–1053. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Molloy SS, Anderson ED, Jean F and Thomas
G: Bi-cycling the furin pathway: From TGN localization to pathogen
activation and embryogenesis. Trends Cell Biol. 9:28–35. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lapierre M, Siegfried G, Scamuffa N,
Bontemps Y, Calvo F, Seidah NG and Khatib AM: Opposing function of
the proprotein convertases furin and PACE4 on breast cancer cells'
malignant phenotypes: Role of tissue inhibitors of
metalloproteinase-1. Cancer Res. 67:9030–9034. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang F, Wang L and Pan J: PACE4 regulates
proliferation, migration and invasion in human breast cancer
MDA-MB-231 cells. Mol Med Rep. 11:698–704. 2015.PubMed/NCBI
|
|
23
|
Kang S, Zhao Y, Hu K, Xu C, Wang L, Liu J,
Yao A, Zhang H and Cao F: miR-124 exhibits antiproliferative and
antiaggressive effects on prostate cancer cells through PACE4
pathway. Prostate. 74:1095–1106. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mahloogi H, Bassi DE and Klein-Szanto AJ:
Malignant conversion of non-tumorigenic murine skin keratinocytes
overexpressing PACE4. Carcinogenesis. 23:565–572. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fu Y, Campbell EJ, Shepherd TG and
Nachtigal MW: Epigenetic regulation of proprotein convertase PACE4
gene expression in human ovarian cancer cells. Mol Cancer Res.
1:569–576. 2003.PubMed/NCBI
|