Introduction
Breast cancer (BC) is one of the most common female
malignant tumors in the world, with increasing incidence (1). As increasing attention has been paid to
early detection in previous years, numerous precancerous diseases,
including atypical ductal hyperplasia, ductal carcinoma in
situ and atypical lobular hyperplasia, may be treated prior to
malignant transformation (2).
However, with the development and combination of traditional
therapy methods, including surgery, chemotherapy and radiotherapy,
molecular target therapy and endocrine therapy have also
contributed to a breakthrough in cancer therapy, and may ameliorate
prognosis significantly (3–7). However, at present, there remains
~500,000 BC-associated mortalities worldwide every year, which is
increasing (8). Therefore, it is
necessary to identify more effective molecular targets for the
diagnosis and treatment of BC.
Tumor necrosis factor receptor 2 (TNFR2) is a member
of the tumor necrosis factor receptor family (9). TNFR2 is composed of membrane binding
TNFR2 and soluble TNFR2 (sTNFR2). It was initially identified in
hematopoietic cells and endothelial cells, and is involved in
anti-inflammation, immune regulation, the repair of lung injury
induced by lipopolysaccharide and the healing of bone fracture
(10–12). The high expression of TNFR2 and its
pro-progression roles have been previously reported in various
types of tumor, including skin tumors, cholangiocarcinoma, myeloma,
colorectal cancer and non-Hodgkin lymphoma (13–17).
However, in BC, clinical studies about TNFR2 were mainly focused on
sTNFR2 in the blood, and the clinical implication of TNFR2 in BC
tissue remains limited (18,19). To the best of our knowledge, the
association between TNFR2 in BC tissue with clinical parameters and
prognosis has not yet been reported.
In the present study, TNFR2 expression was detected
in BC tissue using immunohistochemistry (IHC) and, to the best of
our knowledge, the results showed for the first time that patients
with high TNFR2 were characterized by increased tumor size,
advanced clinical stage, higher pathological grade and poorer
overall survival (OS) rate and disease-free survival (DFS) rate. In
addition, univariate and multivariate Cox regression analysis
detected the impacts of clinical parameters on OS and DFS rate.
Materials and methods
Patient selection
Following approval by the review board and ethics
committee of Weifang People's Hospital (Weifang, China), 125
primary BC specimens were selected from patients who underwent
surgical resection between January 2005 and December 2010 at
Weifang People's Hospital. No patients received chemotherapy,
radiotherapy, immunomodulatory therapy or hormonal therapy prior to
surgery, or by the time of follow-up. Follow-up data was summarized
on December 31th, 2015. The information of patients is shown in
Table I.
 | Table I.Association between tumor necrosis
factor receptor 2 and clinical parameters of patients with breast
cancer. |
Table I.
Association between tumor necrosis
factor receptor 2 and clinical parameters of patients with breast
cancer.
|
|
| TNFR2 expression,
n |
|
|---|
|
|
|
|
|
|---|
| Clinical
parameters | Cases, n | Low | High | P-value |
|---|
| Total | 125 | 71 | 54 |
|
| Age |
|
|
| 0.788 |
| <35
years | 40 | 22 | 18 |
|
| ≥35
years | 85 | 49 | 36 |
|
| Menopausal
status |
|
|
| 0.156 |
| No | 49 | 24 | 25 |
|
| Yes | 76 | 47 | 29 |
|
| Family history |
|
|
| 0.245 |
| No | 105 | 62 | 43 |
|
| Yes | 20 | 9 | 11 |
|
| Tumor size |
|
|
| 0.006a |
| <5
cm | 109 | 67 | 42 |
|
| ≥5
cm | 16 | 4 | 12 |
|
| Lymph node
involvement |
|
|
| 0.188 |
| No | 61 | 31 | 30 |
|
| Yes | 64 | 40 | 24 |
|
| Clinical stage |
|
|
| 0.011a |
| I/II | 93 | 59 | 34 |
|
| III | 32 | 12 | 20 |
|
| Pathological
grade |
|
|
| 0.004a |
|
G1/G2 | 106 | 66 | 40 |
|
| G3 | 19 | 5 | 14 |
|
| Pathological
type |
|
|
| 0.379 |
| Ductal
invasive | 84 | 50 | 34 |
|
|
Others | 41 | 21 | 20 |
|
| ER, PR and HER2
status |
|
|
| 0.607 |
|
Triple-negative | 33 | 20 | 13 |
|
|
Non-triple-negative | 92 | 51 | 41 |
|
IHC
Sections were cut into 3-µm slices and incubated
with primary antibodies for TNFR2 (rabbit anti-human; dilution,
1:300; cat. no. 3727; Cell Signaling Technology, Inc., Danvers, MA,
USA) at 4°C overnight. Normal rabbit immunoglobulin G (IgG),
instead of antibodies, was used as the negative control. The
sections were then incubated with horseradish peroxidase goat
anti-rabbit IgG polymer (ready-to-use dilution; cat. no. 9902;
Maixin Biotechnology Development Co., Ltd., Fuzhou, China) and
stained with 3,3′-diaminobenzidine (cat. no. ZLI-9017; ZSGB-BIO,
Beijing, China); cell nuclei were stained using hematoxylin (cat.
no. ZLI-9609; ZSGB-BIO). The scores were evaluated a CX31
microscope (Olympus corporation, Tokyo, Japan) by two pathologists
(magnification, ×400). The proportion of stained cells was recorded
in at least 5 random fields. The proportion score represented the
fraction of positively stained tumor cells 0, <10%; 1, 10–25%;
2, 26–75%; 3, >75%). The intensity score represented the average
staining intensity 0, none; 1, weak; 2, intermediate; 3, strong).
The expression score of TNFR2 was calculated as the product of the
proportion and intensity scores. Scores ≥4 were classified as high
expression, while scores <4 were classified as low
expression.
Statistical analysis
SPSS 11.0 software (SPSS, Inc., Chicago, IL, USA)
was used for statistical analysis. The association between the
expression of TNFR2 and clinical parameters was analyzed using the
χ2 test. Survival curves were drawn using the Kaplan-Meier method
and compared using the log-rank test. Cox's proportional hazards
regression model was performed to identify factors affecting the OS
and DFS rate of BC. P<0.05 was considered to indicate a
statistically significant difference.
Results
TNFR2 was positively associated with
increased tumor size, advanced clinical stage and higher
pathological grade
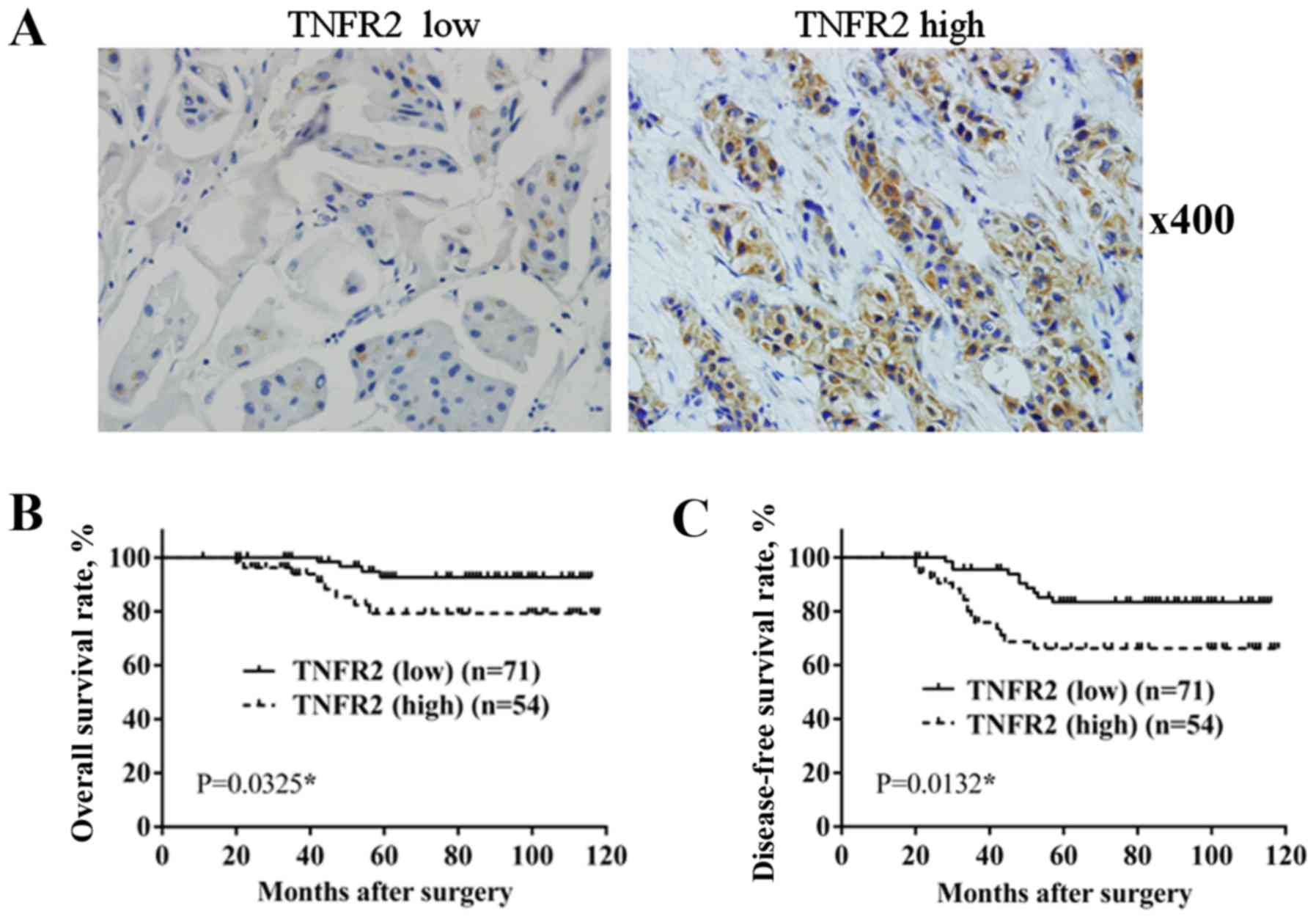
A total of 125 BC specimens were divided into 2
groups, according to TNFR2 expression, resulting in 71 cases with
low expression and 54 cases with high expression (Fig. 1). As shown in Table I, only 4 out of 71 cases in the low
TNFR2 group had a tumor size >5 cm, whereas in the high TNFR2
group, a increased number of cases had a tumor size >5 cm (12/54
cases; P=0.006). In total, 12 out of 71 cases in the low TNFR2
group were at stage III, which was significantly less than the 20
out of 54 cases in the high TNFR2 group (P=0.011). A total of 5 out
of 71 cases in the low TNFR2 group were pathological grade III,
which was significantly less than the 14 out of 54 cases in the
high TNFR2 group (P=0.004). The differences between the two groups
in age, menopausal status, family history, lymph node involvement,
pathological type, estrogen receptor (ER) or progesterone receptor
(PR) status and human epidermal growth factor receptor 2 (HER2)
status were not significant. This confirmed the positive
association of TNFR2 with larger tumor size, advanced clinical
stage and higher pathological grade.
TNFR2 is positively associated with
poor prognosis
During the follow-up period, there were 4
mortalities out of the 71 cases in TNFR2 low expression group, with
an OS rate of 94.36%; however, in the TNFR2 high expression group,
there were 8 mortalities out of the 54 cases, with an OS rate of
85.18%. In addition, 10 cases of recurrence or metastasis occurred
in the TNFR2 low expression group, with a DFS rate of 85.91%, while
in the TNFR2 high expression group, 16 cases of recurrence or
metastasis occurred, with a DFS rate of 70.37%. Survival rate was
estimated using the Kaplan-Meier method and differences were
compared using the log-rank test. The differences in OS rate
(P=0.0325; Fig. 1B) and DFS rate
(P=0.0132; Fig. 1C) between the two
groups were revealed to be significantly different.
Regression analysis of factors
affecting OS and DFS rate
To confirm factors that affect the prognosis of
patients with BC, Cox regression analysis was performed. Firstly,
univariate Cox regression analysis revealed that TNFR2 expression
(P=0.045), tumor size (P<0.0001), clinical stage (P<0.0001),
pathological grade (P=0.002), ER, PR and HER2 triple-status
(P=0.001) all impacted the OS rate of patients with BC
significantly. In addition, TNFR2 expression (P=0.017), age
(P=0.011), menopausal status (P<0.0001), tumor size (P=0.016),
clinical stage (P=0.005), pathological grade (P=0.002), ER, PR and
HER2 triple-status (P=0.008) all had an impact on the DFS rate of
patients with BC (Table II).
| Table II.Univariate analysis and multivariate
analysis identifies factors affecting overall survival of patients
with breast cancer. |
Table II.
Univariate analysis and multivariate
analysis identifies factors affecting overall survival of patients
with breast cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| TNFR2 | 3.428 | 1.03–11.404 | 0.045a | 3.36 | 0.624–18.107 | 0.158 |
| Age | 1.012 | 0.273–3.755 | 0.986 | 1.962 | 0.373–10.303 | 0.426 |
| Menopausal
status | 0.374 | 0.119–1.172 | 0.091 | 1.073 | 0.126–9.125 | 0.948 |
| Family history | 0.672 | 0.182–2.483 | 0.551 | 2.315 | 0.398–13.472 | 0.35 |
| Tumor size | 16.156 | 4.821–54.138 |
<0.0001a | 0.256 | 0.047–1.407 | 0.117 |
| Lymph
involvement | 2.493 | 0.674–9.215 | 0.171 | 0.425 | 0.065–2.79 | 0.373 |
| Clinical stage | 11.743 | 3.147–43.823 |
<0.0001a | 0.071 | 0.007–0.703 | 0.024a |
| Pathological
grade | 6.48 | 2.04–20.584 | 0.002a | 0.371 | 0.057–2.395 | 0.297 |
| Histological
type | 1.347 | 0.427–4.245 | 0.611 | 0.132 | 0.014–1.271 | 0.08 |
| ER, PR and
HER2 | 7.448 | 2.236–24.804 | 0.001a | 0.077 | 0.011–0.53 | 0.009a |
To ascertain the factors effecting prognosis,
multivariate Cox regression analysis showed that only clinical
stage (P=0.024) and ER, PR and HER2 triple-status (P=0.009) showed
a significant impact on the OS rate of patients with BC. In
addition, only TNFR2 expression (P=0.043) and menopausal status
(P=0.033) showed a significant impact on the DFS rate of patients
with BC (Table III).
| Table III.Univariate analysis and multivariate
analysis identifies factors affecting disease-free survival of
patients with breast cancer. |
Table III.
Univariate analysis and multivariate
analysis identifies factors affecting disease-free survival of
patients with breast cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| TNFR2 | 2.616 | 1.185–5.775 | 0.017a | 2.622 | 1.031–6.668 | 0.043a |
| Age | 2.723 | 1.258–5.895 | 0.011a | 2.033 | 0.797–5.19 | 0.138 |
| Menopausal
status | 4.324 | 1.916–9.759 |
<0.0001a | 3.41 | 1.103–10.544 | 0.033a |
| Family history | 0.875 | 0.301–2.541 | 0.806 | 1.232 | 0.374–4.054 | 0.732 |
| Tumor size | 0.344 | 0.144–0.82 | 0.016a | 0.847 | 0.28–2.561 | 0.769 |
| Lymph
involvement | 1.351 | 0.625–2.921 | 0.444 | 0.73 | 0.26–2.054 | 0.551 |
| Clinical stage | 0.328 | 0.15–0.714 | 0.005a | 0.442 | 0.158–1.241 | 0.121 |
| Pathological
grade | 0.257 | 0.111–0.595 | 0.002a | 0.596 | 0.225–1.574 | 0.296 |
| Histological
type | 1.407 | 0.466–2.349 | 0.912 | 0.949 | 0.393–2.291 | 0.908 |
| ER, PR and
HER2 | 2.856 | 1.318–6.187 | 0.008a | 0.615 | 0.238–1.588 | 0.315 |
Discussion
TNFR2 is encoded by the tumor necrosis factor
receptor superfamily 1B (TNFRSF1B) gene (20). In previous years, it was reported that
TNFR2 has important roles in the occurrence and progression of
various types of tumor, including skin tumors, cholangiocarcinoma,
myeloma, colorectal cancer and non-Hodgkin lymphoma (13–17).
Jöhrer et al reported that high expression of TNFR2 promoted
the metastasis of myeloma cells (15). Tanimura et al identified that
TNFR2 facilitated invasion of cholangiocarcinoma cells through
regulating matrix metalloproteinase 9 secretion (14). A previous study by Mizoguchi et
al reported that TNFR2 promoted hyperplasia of mouse colon
epithelium and induced carcinomatosis (21). However, clinical studies investigating
TNFR2 in BC are limited. In 1997, Jablonska reported that soluble
TNF receptors in patients prior to treatment were higher than in
the control, and decreased following the surgery treatment
(18). In 2000, Tesarová et al
reported that plasma levels of soluble TNF receptors may act as a
non-specific marker of the untreated BC (19). Xu et al (2014) reported that
TNFR2 gene polymorphism in the peripheral blood was associated with
risk of BC (20). However, these
studies were limited to sTNFR2 in BC, but did not investigate
TNFR2. In 2005, a study by Mestiri et al demonstrated that
the 196R-TNFRII allele showed a significant association with
increased OS and DFS in patients with BC (22). This previous study focused on genetic
variation in TNFR2, but not TNFR2 itself. In 2006, García-Tuñón
et al reported that TNFR2 was higher in in situ
carcinoma than in benign breast diseases, and even higher in
infiltrating tumors, but no further analysis was performed
(23). In the present study, TNFR2
expression was detected in BC tissue using IHC and, to the best of
our knowledge, its association with clinical parameters and
prognosis was analyzed for the first time. TNFR2 was revealed to be
positively associated with increased tumor size, advanced clinical
stage and higher pathological grade. This is consistent with the
effects of TNFR2 on malignant behaviors of tumor cells reported
previously, including proliferation, migration and invasion
(14,24).
In addition, survival analysis confirmed that TNFR2
was positively associated with poor OS and DFS rates, in accordance
with prognostic effects of the 196R-TNFRII allele. This indicated
that TNFR2 has an independent role in predicting the prognosis of
BC. During the follow-up period, almost all patients accepted
different types of adjuvant therapies, including chemotherapy,
radiotherapy, immunomodulatory therapy and even Chinese herbal
therapy. According to ER, PR and HER2 status and economical
capability, patients accepted hormonal therapy or molecular target
therapy to a different degree. All the treatments may play a role
in prognosis. However, the present study aimed to analyze the roles
of TNFR2 in prognosis. Therefore, the association of all the
adjuvant therapies with prognosis was not investigated.
BC is a complicated disease and its prognosis may be
effected by different factors, including age, menopausal status,
clinical stage, pathological grade and receptors on the tumor cell
surface (25–27). Tumor cells at an advanced stage
usually possess higher malignant behaviors, including
proliferation, migration, invasion and drug resistance, and lose
surgery opportunity, resulting in poor prognosis (28,29).
Triple negative BC (TNBC) is a distinct subgroup of BC that has
been shown to exhibit negative ER, PR and HER2 expression, and was
characterized by more aggressive behavior compared with non-TNBC
(30). In addition, patients lacking
expression of ER, PR and HER2 cannot benefit from endocrine therapy
and molecular targeted treatments for HER2, which is effective for
ameliorating prognosis (6,7,31). In the
present study, univariate and multivariate Cox regression showed
that clinical stage and ER, PR and HER2 triple-status may
significantly impact the OS rate of patients with BC. Univariate
and multivariate Cox regression showed also that TNFR2 expression
and menopausal status may significantly impact the DFS rate of
patients with BC. This can be explained by the important role of
estrogen in BC occurrence and the impact of TNFR2 on malignant
behaviors of tumor cells.
However, the present study had certain deficiencies.
Since all the samples were from local patients, data evidently had
regional limitation and the results could not embody the
implication of TNFR2 universally. Furthermore, only 125 BC samples
were involved, and the limited number of cases also restricted the
reliability of the present study. In addition, establishment of a
validation cohort may make the results more convincing.
In conclusion, the present study verified the
important roles of TNFR2 in progression and prognosis of BC and
enriched the understanding of the roles of TNFR2 as an effective
target for BC therapy.
References
|
1
|
Riaz SK, Saeed M and Malik MF: Clinical
and therapeutic implications of histone acetylation in breast
cancer. West Indian Med J. May 6–2015.(Epub ahead of print).
View Article : Google Scholar
|
|
2
|
Strasser-Weippl K, Horick N, Smith IE,
O'Shaughnessy J, Ejlertsen B, Boyle F, Buzdar AU, Fumoleau P,
Gradishar W, Martin M, et al: Identification of early breast cancer
patient cohorts who may benefit from lapatinib therapy. Eur J
Cancer. 56:85–92. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sage EK, Schmid TE, Sedelmayr M, Gehrmann
M, Geinitz H, Duma MN, Combs SE and Multhoff G: Comparative
analysis of the effects of radiotherapy versus radiotherapy after
adjuvant chemotherapy on the composition of lymphocyte
subpopulations in breast cancer patients. Radiother Oncol.
118:176–180. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Smoot B, Paul SM, Aouizerat BE, Dunn L,
Elboim C, Schmidt B, Hamolsky D, Levine JD, Abrams G, Mastick J, et
al: Predictors of altered upper extremity function during the first
year after breast cancer treatment. Am J Phys Med Rehabil.
95:639–655. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Partridge AH: Chemotherapy in
premenopausal breast cancer patients. Breast Care (Basel).
10:307–310. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhu YY, Si W, Ji TF, Guo XQ, Hu Y and Yang
JL: The variation and clinical significance of hormone receptors
and Her-2 status from primary to metastatic lesions in breast
cancer patients. Tumour Biol. 37:7675–7684. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lin PL, Hao Y, Xie J, Li N, Zhong Y, Zhou
Z, Signorovitch JE and Wu EQ: Physician experiences and preferences
in the treatment of HR+/HER2- metastatic breast cancer in the
United States: A physician survey. Cancer Med. 5:209–220. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rossi L and Pagani O: The modern landscape
of endocrine therapy for premenopausal women with breast cancer.
Breast Care (Basel). 10:312–315. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hosono K, Yamada E, Endo H, Takahashi H,
Inamori M, Hippo Y, Nakagama H and Nakajima A: Increased tumor
necrosis factor receptor 1 expression in human colorectal adenomas.
World J Gastroenterol. 18:5360–5368. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tang W, Lu Y, Tian QY, Zhang Y, Guo FJ,
Liu GY, Syed NM, Lai Y, Lin EA, Kong L, et al: The growth factor
progranulin binds to TNF receptors and is therapeutic against
inflammatory arthritis in mice. Science. 332:478–484. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Guo Z, Li Q, Han Y, Liang Y, Xu Z and Ren
T: Prevention of LPS-induced acute lung injury in mice by
progranulin. Mediators Inflamm. 2012:5407942012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhao YP, Tian Q, Frenkel S and Liu CJ: The
promotion of bone healing by progranulin, a downstream molecule of
BMP-2, through interacting with TNF/TNFR signaling. Biomaterials.
34:6412–6421. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Arnott CH, Scott KA, Moore RJ, Robinson
SC, Thompson RG and Balkwill FR: Expression of both TNF-alpha
receptor subtypes is essential for optimal skin tumour development.
Oncogene. 23:1902–1910. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tanimura Y, Kokuryo T, Tsunoda N, Yamazaki
Y, Oda K, Nimura Y, Mon N Naing, Huang P, Nakanuma Y, Chen MF, et
al: Tumor necrosis factor alpha promotes invasiveness of
cholangiocarcinoma cells via its receptor, TNFR2. Cancer Lett.
219:205–213. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jöhrer K, Janke K, Krugmann J, Fiegl M and
Greil R: Transendothelial migration of myeloma cells is increased
by tumor necrosis factor (TNF)-alpha via TNF receptor 2 and
autocrine up-regulation of MCP-1. Clin Cancer Res. 10:1901–1910.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Grotowski M and Wojtuń S: CEA, CA-19-9 and
il-8, sTNFRII and sil-2R in persons at high risk of colorectal
cancer. Pol Merkur Lekarski. 14:327–330. 2003.(In Polish).
PubMed/NCBI
|
|
17
|
Heemann C, Kreuz M, Stoller I, Schoof N,
von Bonin F, Ziepert M, Löffler M, Jung W, Pfreundschuh M, Trümper
L and Kube D: Circulating levels of TNF receptor II are prognostic
for patients with peripheral T-cell non-Hodgkin lymphoma. Clin
Cancer Res. 18:3637–3647. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jablonska E: Release of soluble IL-6
receptor (IL-6sR) in comparison with release of soluble TNF
receptors (sTNF-Rs) by PMNs and WBC derived from breast cancer
patients. Cancer Lett. 119:79–85. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tesarová P, Kvasnicka J, Umlaufová A,
Homolková H, Jirsa M and Tesar V: Soluble TNF and IL-2 receptors in
patients with breast cancer. Med Sci Monit. 6:661–667.
2000.PubMed/NCBI
|
|
20
|
Xu F, Zhou G, Han S, Yuan W, Chen S, Fu Z,
Li D, Zhang H, Li D and Pang D: Association of TNF-α, TNFRSF1A and
TNFRSF1B gene polymorphisms with the risk of sporadic breast cancer
in northeast Chinese Han women. PLoS One. 9:e1011382014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mizoguchi E, Mizoguchi A, Takedatsu H,
Cario E, de Jong YP, Ooi CJ, Xavier RJ, Terhorst C, Podolsky DK and
Bhan AK: Role of tumor necrosis factor receptor 2 (TNFR2) in
colonic epithelial hyperplasia and chronic intestinal inflammation
in mice. Gastroenterology. 122:134–144. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mestiri S, Bouaouina N, Ben Ahmed S and
Chouchane L: A functional polymorphism of the tumor necrosis factor
receptor-II gene associated with the survival and relapse
prediction of breast carcinoma. Cytokine. 30:182–187. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
García-Tuñón I, Ricote M, Ruiz A, Fraile
B, Paniagua R and Royuela M: Role of tumor necrosis factor-alpha
and its receptors in human benign breast lesions and tumors (in
situ and infiltrative). Cancer Sci. 97:1044–1049. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yang D, Wang LL, Dong TT, Shen YH, Guo XS,
Liu CY, Liu J, Zhang P, Li J and Sun YP: Progranulin promotes
colorectal cancer proliferation and angiogenesis through TNFR2/Akt
and ERK signaling pathways. Am J Cancer Res. 5:3085–3097.
2015.PubMed/NCBI
|
|
25
|
Mouttet D, Laé M, Caly M, Gentien D,
Carpentier S, Peyro-Saint-Paul H, Vincent-Salomon A, Rouzier R,
Sigal-Zafrani B, Sastre-Garau X and Reyal F: Estrogen-receptor,
progesterone-receptor and HER2 status determination in invasive
breast cancer. Concordance between immuno-histochemistry and
MapQuant microarray based assay. PLoS One. 11:e01464742016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pizot C, Boniol M, Mullie P, Koechlin A,
Boniol M, Boyle P and Autier P: Physical activity, hormone
replacement therapy and breast cancer risk: A meta-analysis of
prospective studies. Eur J Cancer. 52:138–154. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chai P, Tian J, Zhao D, Zhang H, Cui J,
Ding K and Liu B: GSE1 negative regulation by miR-489-5p promotes
breast cancer cell proliferation and invasion. Biochem Biophys Res
Commun. 471:123–128. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Richards P, Ward S, Morgan J, Lagord C,
Reed M, Collins K and Wyld L: The use of surgery in the treatment
of ER+ early stage breast cancer in England: Variation by time, age
and patient characteristics. Eur J Surg Oncol. 42:489–496. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Qiu J, Xue X, Hu C, Xu H, Kou D, Li R and
Li M: Comparison of clinicopathological features and prognosis in
triple-negative and non-triple negative breast cancer. J Cancer.
7:167–173. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ingthorsson S, Andersen K, Hilmarsdottir
B, Maelandsmo GM, Magnusson MK and Gudjonsson T: HER2 induced EMT
and tumorigenicity in breast epithelial progenitor cells is
inhibited by coexpression of EGFR. Oncogene. 35:4244–4255. 2016.
View Article : Google Scholar : PubMed/NCBI
|