Introduction
Bladder cancer is the most frequent malignancy of
urinary tract and the 11th most common cancer with an incidence of
5.3 cases per 100,000 worldwide (1).
Compared with developing countries, bladder cancer poses an
increased risk to health due to its higher incidence in developed
countries (2). Bladder cancer is the
fifth most common type of cancer in Europe with 116,000 new cases
per year (3).
There are various histological types of bladder
cancer, including urothelial bladder cancer, squamous carcinoma and
adenocarcinoma, of which urothelial bladder cancer is the most
frequent type, accounting for >90% of cases (4). Clinically, bladder cancer can be divided
into non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive
bladder cancer (MIBC), with different treatments and outcome
(4). NMIBC accounts for ~75–85% of
all bladder cancers, with relatively higher overall survival rates
compared with MIBC (5).
At diagnosis, 15–25% of patients with bladder cancer
have muscle-invasion. Although there have been advances in radical
cystectomy and systemic therapy, ~50% of these patients with
muscle-invasion succumb from metastatic disease (6,7). Overall,
~50–80% of all treated patients with transurethral resection have
tumor relapse within a period of 2 years and 10–25% of cases may
present with a high grade tumor (8).
Discovery of novel effective prognostic or predictive biomarkers
may enable the development of therapeutics. Therefore, it is
urgently required to search for novel effective and promising
biomarkers, which may decrease relapse rate and improve overall
survival rate.
Tumor necrosis factor (TNF) receptor-associated
factor 6 (TRAF6) is a member of a new family of signaling proteins
with a conserved TRAF domain of ~230 amino acids in the C-terminal
and zinc finger motifs in the N-terminal (9) TRAF6 may function as an important
molecule in activating nuclear factor-κB (NF-κB) by mediating
interactions to NF-κB (10).
Inhibition of TRAF6 by short interfering RNA has been demonstrated
in in vitro experiments to impair interleukin-1
(IL-1)-induced NF-κB and c-Jun/activator protein 1 activation. This
leads to the inhibition of proliferation and promotion of apoptosis
in myeloma cells (11,12). Furthermore, TRAF6 is an E3 ubiquitin
ligase, which mediates the synthesis of
Lysine-63-linked-polyubiquitin chains conjugated to proteins,
including IκB kinase subunit γ (IKBKG), interleukin 1 receptor
associated kinase 1 (IRAK1), AKT1, AKT2, ubiquitin conjugating
enzyme E2 N and ubiquitin conjugating enzyme E2 V1 (13). Previously, TRAF6 has been demonstrated
to promote oncogenesis by inhibiting apoptosis and stimulating
proliferation and invasion as an E3 ubiquitin ligase (14,15).
Additionally, overexpression of TRAF6 was observed in a number of
types of malignancies, including glioma, pancreatic cancer and
non-small cell lung cancer (16–18).
However, the clinical significance and biological effects of TRAF6
remain to be elucidated in bladder cancer.
In the present study, the expression of TRAF6 was
detected in 126 cases of urothelial bladder cancer and the cohort
was divided according to TRAF6 expression into low and high
expression groups. The associations between TRAF6 and
clinicopathological factors were analyzed using χ2 test.
Furthermore, the effects of TRAF6 expression on tumor recurrence
were analyzed in univariate and multivariate analyses. In addition,
we evaluated the associations between TRAF6 expression and other
clinicopathological factors.
Patients and methods
Patients and sample collection
Between January, 2005 to December, 2012, a total of
329 patients were diagnosed as bladder cancer and underwent
surgical resection (transurethral tumor resection or radical total
bladder cystectomy) at the Yidu Central Hospital of Weifang
(Weifang, China), which were considered as the primary cohort of
the present study.
A total of 126 patients with MIBC and NMIBC were
selected for the validation cohort if the following criteria were
fulfilled: i) The histological type is urothelial bladder cancer,
ii) the patient had follow-ups following surgery, and
paraffin-embedded samples were available, and iii) no history of
other tumors and no neoadjuvant chemotherapy. The validation cohort
consisted of 97 patients with tumor stage Ta-T according to the
American Joint Committee on Cancer/Union for International Cancer
Control staging system (19), who
underwent transurethral tumor resection and 29 patients with tumor
stage T2-T4, who underwent radical total bladder cystectomy. All
126 paraffin-embedded samples were obtained from the Pathological
Department at the Yidu Central Hospital of Weifang as part of
routine examination, with prior informed consent of all patients
and prior approval of the Ethics Committee of Yidu Central Hospital
of Weifang and Shandong Cancer Hospital and Institute.
The parameters used to evaluate the clinical
significance of TRAF6 expression in the present study are overall
survival rate and recurrence-free survival rate. Recurrence was
defined as any new bladder cancer lesion detected following
surgery, and the time of recurrence was defined from time of
surgery to diagnosis of new tumors.
Immunohistochemical (IHC)
staining
The tissue samples were deparaffinized for 20 min
and rehydrated in graded ethanol according to previous studies
(20–22). The samples were subsequently incubated
in 0.01 M citric acid (pH 6.0) and heated in a microwave for 30 min
for antigen retrieval. Endogenous peroxidase activity was blocked
by incubating the samples in 0.3% hydrogen peroxide at room
temperature for 10 mins. The slides were incubated in diluted
anti-TRAF6 primary antibody (1:50; cat. no. sc-8409, Santa Cruz
Biotechnology, Inc., Dallas, TX, USA) at 4°C overnight, followed by
primary antibody retrieval and washed with phosphate buffered
saline (PBS). The slides were incubated in horseradish
peroxidase-labeled anti-mouse secondary antibody at dilution
1:1,000 (cat. no. A0216, Beyotime Institute of Biotechnology,
Haimen, China) at 37°C for 2 h. Subsequently, the slides were
incubated with 3,3′-diaminobenzidine for visualization, and the
slides were counterstained with hematoxylin at room temperature for
5 min.
Staining was scored by two senior pathologists, who
were unaware of the clinical information of the patients. The
samples were scored according to staining intensity and the
percentage of positively stained cells, which has been described
previously (23,24). The staining intensity was scored as
weak (score 1), medium (score 2) or high (score 3). The scores for
positively stained cells were determined as follows: 25% (score 1),
25–75% (score 2) and 75% (score 3). The final IHC score was
calculated as the intensity score multiplied by the score for
positively stained cells, which ranged from 1 to 9 (25). Samples with final scores of ≥4 were
defined as high TRAF6 expression and final scores of <4 as low
TRAF6 expression.
Statistical analysis
The software SPSS 17.0 (SPSS, Inc., Chicago, IL,
USA) was used to analyze all the data and generate the P-values.
The associations between TRAF6 expression and clinicopathological
features were evaluated by χ2 test. Kaplan-Meier
analysis and log-rank test were performed for analysis of
recurrence-free survival and overall survival curves and to
evaluate statistical difference. In multivariate analysis, the
Cox-regression proportional hazards model was used to identify the
independent factors. In all tests, P<0.05 was considered to
indicate a statistically significant difference.
Results
Expression of TRAF6 in bladder cancer
tissues
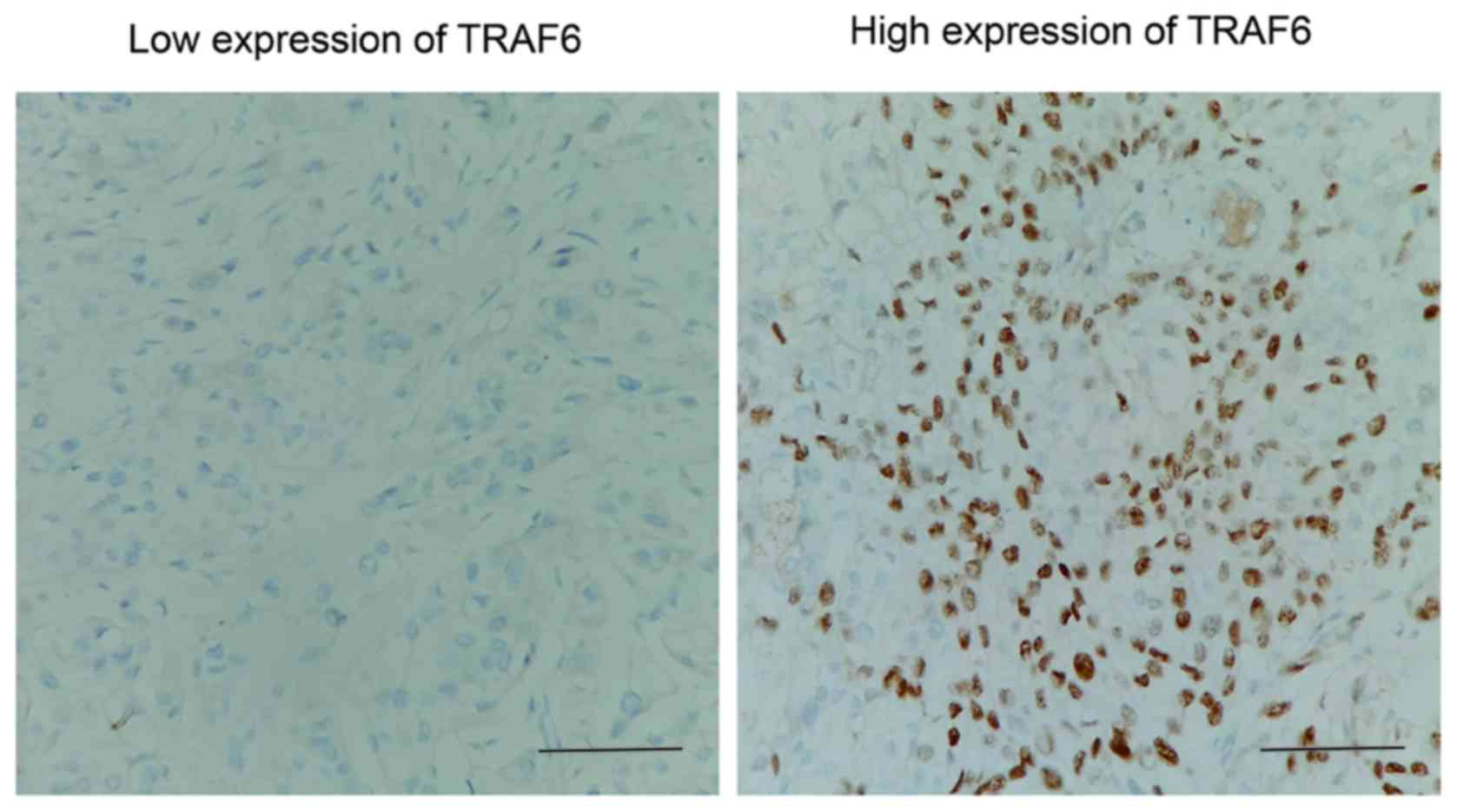
Expression of TRAF6 was initially detected by IHC.
As a signal mediator of members of the TNF receptor superfamily and
members of the Toll/interleukin (IL)-1 family, TRAF6 was primarily
expressed in the cytoplasm of bladder cancer cells. IHC results
were evaluated by calculating the total IHC score, which was the
product of staining intensity and the percentage of positively
stained cells as described previously in the Patients and materials
section. The validation cohort was further divided according to the
level of TRAF6 expression (low and high expression groups),
according to the IHC score (Fig. 1).
In the present cohort, the rates of low and high TRAF6 expression
were 38.10% (48/126) and 61.90% (78/126), respectively.
Association between TRAF6 expression
and clinicopathological factors
χ2 test was used to evaluate the
association between TRAF6 expression and clinicopathological
factors, including sex, age, tumor diameter, tumor number, tumor
stage, tumor grade and metastasis (Table
I). Notably, TRAF6 high expression was observed to be
significantly associated with metastasis (P=0.001), indicating that
high TRAF6 may promote the bladder cancer progression and
metastasis. However, no significant associations between TRAF6 and
other clinicopathological factors were observed.
 | Table I.Associations between TRAF6 expression
and clinicopathological factors in urothelial bladder cancer. |
Table I.
Associations between TRAF6 expression
and clinicopathological factors in urothelial bladder cancer.
|
|
| TRAF6 expression |
|
|---|
|
|
|
|
|
|---|
| Parameters | n | Low | High | P-valuea |
|---|
| Sex |
|
|
| 0.229 |
| Male | 99 | 35 | 64 |
|
|
Female | 27 | 13 | 14 |
|
| Age |
|
|
| 0.246 |
|
<60 | 43 | 13 | 30 |
|
| ≥60 | 63 | 15 | 48 |
|
| Tumor diameter,
cm |
|
|
| 0.856 |
| ≤3 | 64 | 25 | 39 |
|
|
>3 | 62 | 23 | 39 |
|
| Tumor number |
|
|
| 0.218 |
|
Single | 105 | 43 | 62 |
|
|
Multiple | 21 | 5 | 16 |
|
| Metastasis
status |
|
|
| 0.001 |
|
Negative | 116 | 48 | 68 |
|
|
Positive | 10 | 0 | 10 |
|
| Tumor stage |
|
|
| 0.828 |
|
Ta-T1 | 97 | 38 | 59 |
|
|
T2-T4 | 29 | 10 | 19 |
|
| Tumor
gradeb |
|
|
| 0.196 |
|
Low | 51 | 23 | 28 |
|
|
High | 75 | 25 | 50 |
|
Correlation between TRAF6 and
recurrence rate
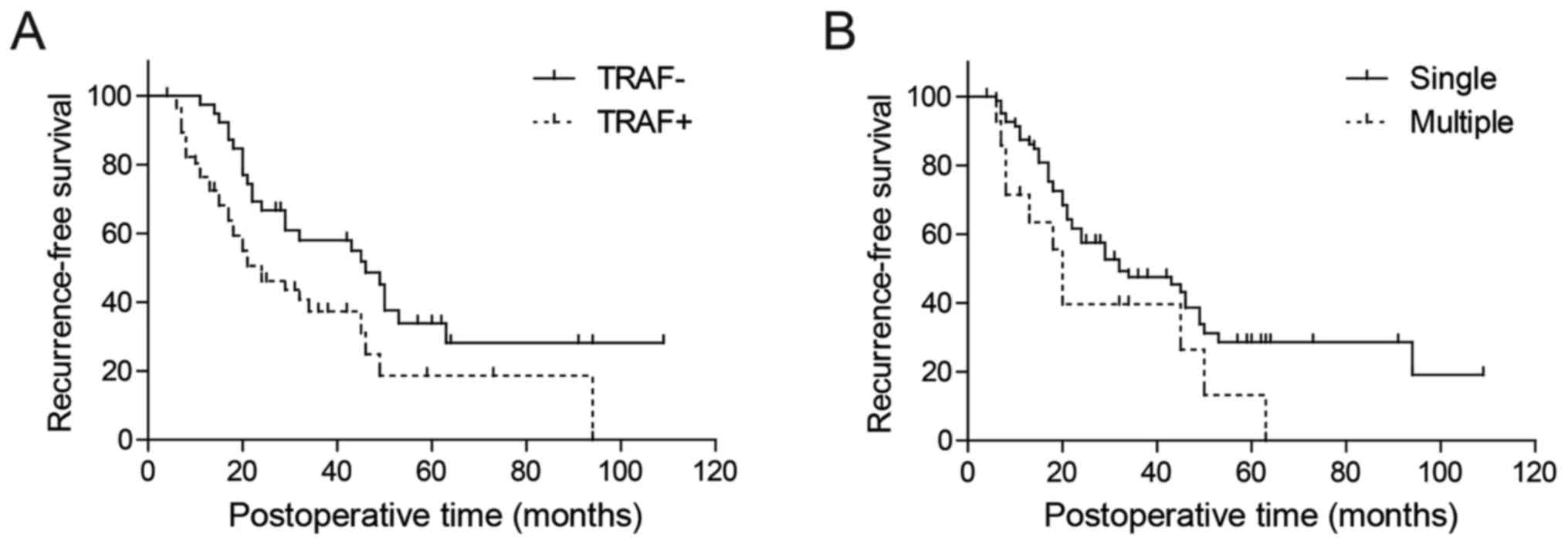
The correlation between TRAF6 and recurrence-free
survival rate was first analyzed by Kaplan-Meier analysis (Table II). Only patients with tumor stage
Ta-T1 (n=97) were selected for analysis of rate of recurrence-free
survival. In univariate analysis, recurrence-free survival rate was
demonstrated to be significantly associated with tumor number and
TRAF6 expression (P=0.042 and 0.016, respectively; Fig. 2; Table
II). Using the Cox-regression model in multivariate analysis,
tumor number, tumor grade and TRAF6 expression were identified as
independent predictive parameters of bladder cancer recurrence
(P=0.008, 0.029 and 0.011, respectively; Table II).
| Table II.Univariate and multivariate analyses
of association between clinicopathological factors and
progression-free survival in patients with non-muscle-invasive
bladder cancer. |
Table II.
Univariate and multivariate analyses
of association between clinicopathological factors and
progression-free survival in patients with non-muscle-invasive
bladder cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Parameters | 5-year
recurrence-free rate, % |
P-valuea | HR | 95% CI |
P-valueb |
|---|
| Sex |
| 0.926 |
|
| 0.498 |
|
Male | 26.4 |
| 1 |
|
|
|
Female | 26.6 |
| 1.24 | 0.67–2.30 |
|
| Age |
| 0.313 |
|
| 0.168 |
|
<60 | 40.8 |
| 1 |
|
|
|
≥60 | 20.6 |
| 1.51 | 0.84–2.69 |
|
| Tumor diameter,
cm |
| 0.359 |
|
| 0.114 |
| ≤3 | 28.8 |
| 1 |
|
|
|
>3 | 25.5 |
| 1.55 | 0.90–2.66 |
|
| Tumor number |
| 0.042 |
|
| 0.008 |
|
Single | 34.9 |
| 1 |
|
|
|
Multiple | 14.6 |
| 2.12 | 1.22–3.68 |
|
| Tumor grade |
| 0.080 |
|
| 0.029 |
| Low
grade | 28.6 |
| 1 |
|
|
| High
grade | 13.2 |
| 2.15 | 1.08–4.29 |
|
| TRAF6
expression |
| 0.016 |
|
| 0.011 |
|
Low | 33.9 |
| 1 |
|
|
|
High | 18.7 |
| 2.04 | 1.18–3.53 |
|
Effects of TRAF6 expression on patient
outcome
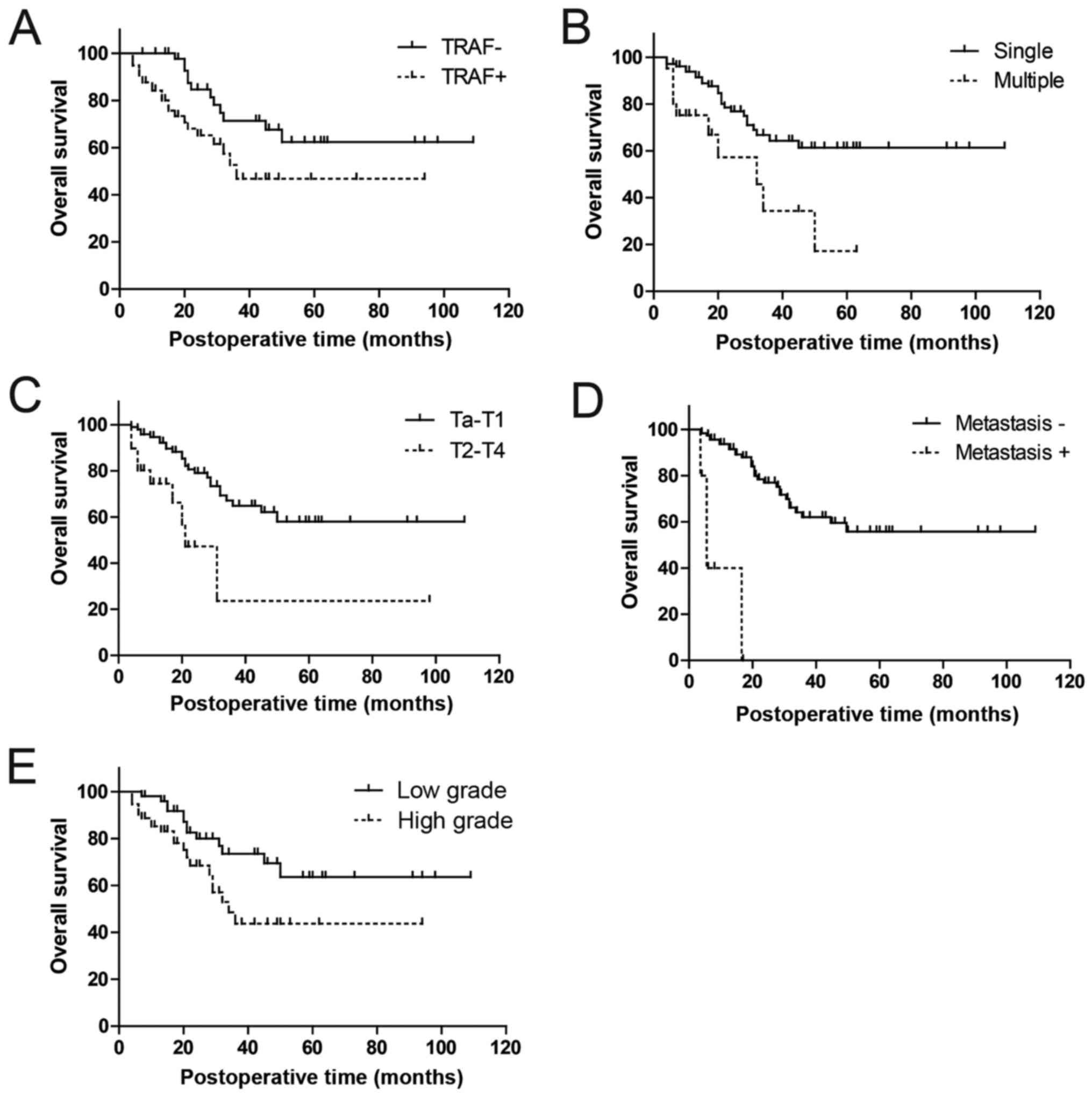
The effects of TRAF6 expression on prognosis was
subsequently evaluated by analyzing the correlation between TRAF6
expression and 5-year overall survival rates using Kaplan-Meier
analysis (Table III). High TRAF6
expression was demonstrated to be significantly associated with
poorer prognosis in patients with urothelial bladder cancer
compared with low TRAF6 expression (univariate analysis, P=0.016,
61.0 vs. 47.8%; Fig. 3A). Apart from
TRAF6 expression, tumor number, metastasis status, tumor stage and
tumor grade were also identified as prognostic factors in
univariate analysis (P=0.003, P<0.001, P=0.001 and P=0.023,
respectively; Fig. 3B-E).
| Table III.Associations between
clinicopathological factors and prognosis in urothelial bladder
cancer. |
Table III.
Associations between
clinicopathological factors and prognosis in urothelial bladder
cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Parameters | 5-year survival
rate, % |
P-valuea | HR | 95% CI |
P-valueb |
|---|
| Sex |
| 0.669 |
|
| 0.336 |
|
Male | 53.9 |
| 1 |
|
|
|
Female | 48.6 |
| 1.47 | 0.67–3.24 |
|
| Age |
| 0.804 |
|
| 0.629 |
|
<60 | 57.4 |
| 1 |
|
|
|
≥60 | 41.7 |
| 0.83 | 0.38–1.78 |
|
| Tumor diameter,
cm |
| 0.436 |
|
| 0.188 |
| ≤3 | 54.7 |
| 1 |
|
|
|
>3 | 54.4 |
| 1.61 | 0.79–3.25 |
|
| Tumor number |
| 0.003 |
|
| 0.022 |
|
Single | 61.4 |
| 1 |
|
|
|
Multiple | 17.2 |
| 2.47 | 0.96–6.35 |
|
| Metastasis
status |
| <0.001 |
|
|
|
|
Negative | 55.8 |
| – |
|
|
|
Positive |
0.0 |
| – | – | – |
| Tumor stage |
| 0.001 |
|
| 0.013 |
|
Ta-T1 | 58.0 |
| 1 |
|
|
|
T2-T4 | 23.6 |
| 4.05 | 1.35–12.17 |
|
| Tumor grade |
| 0.023 |
|
| 0.030 |
| Low
grade | 63.6 |
| 1 |
|
|
| High
grade | 43.7 |
| 2.33 | 1.09–4.99 |
|
| TRAF6
expression |
| 0.016 |
|
| 0.037 |
|
Low | 61.0 |
| 1 |
|
|
|
High | 47.8 |
| 2.04 | 0.92–4.49 |
|
Metastasis status was excluded from multivariate
analysis, because it was indicated to be associated with TRAF6
expression using the χ2 test in univariate analysis
(Table I). In multivariate analysis,
TRAF6 expression was identified as an independent prognostic factor
in urothelial bladder cancer (hazard ratio, 2.04; 95% confidence
interval, 0.92–4.49; P=0.037; Table
III). Furthermore, additional three factors, including tumor
number, stage and grade, were also identified to be independent
prognostic factors (P=0.022, 0.013 and 0.030, respectively;
Table III).
Discussion
Bladder cancer was the most common malignancy of the
urinary tract worldwide in 2014 and is also prominent for its high
recurrence rate in all treated patients (26). Investigating potential biomarkers may
bring about new breakthroughs in strategies on reducing recurrence
and survival rate, similar to the discovery of trastuzumab
following studies on the human epidermal growth factor receptor-2
(HER2) studies.
Recently, important progress has been made in the
biomarker field particularly in new detection techniques in
genomics and proteomics (27,28). In bladder cancer, a number of
accomplishments were achieved, including the identification of the
gene signatures, which associate with bladder cancer progression
(29). However, basic science
research is not sufficient for breakthroughs in bladder cancer
treatment. Translational studies, including the study of potential
biomarkers, also have an important role in advancing progress in
treatment.
The identification of prognostic and predictive
markers is of great importance to improve the management of
patients and to decrease the rate of mortality. Promising
biomarkers may lead to effective therapeutic drug targets and
drugs.
TRAF6 has been demonstrated to mediate signal
transduction from the TNF receptor superfamily and receptors,
including cluster of differentiation 40, tumor necrosis factor
superfamily member 11 and IL-1 (10).
These receptors are involved in numerous signaling pathways and
tumor processes. Furthermore, ectopic TRAF6 expression was observed
in a number of types of cancer, including glioma, pancreas cancer
(9,16). However, the underlying molecular
mechanisms in these types of cancer remain to be elucidated.
In bladder cancer, no previous study on TRAF6
function was reported to the best of our knowledge. However, in a
large screen of effective genetic variants in microRNAs (miRNAs) in
bladder cancer, TRAF6 was hypothesized as an effector molecule of
miR-146a. miR-146a has an notable role in predicting the risk and
recurrence of bladder cancer (30).
This supported the results in the present study, which indicated
that TRAF6 expression may be a prognostic factor in urothelial
bladder cancer.
There are two main intracellular protein degradation
pathways in eukaryotic cells: Ubiquitination and autophagy
(31). Ubiquitination is an important
post-translational modification that involves the multi-stage
stepwise conjugation of proteins to ubiquitin monomers by the
ubiquitinating enzymes E1, E2, and E3 (32). In this process, TRAF6 acts as an E3
ubiquitin ligase, which mediates the conjugation of
lysine-63(K63)-linked polyubiquitin chains to targeted proteins,
which is responsible for substrate specificity (10). The substrates of TRAF6-mediated
ubiquitination include: IKBKG, IRAK1, AKT1 and AKT2 (33). In breast cancer, TRAF6 was
demonstrated to ubiquitinate the proform of asparaginyl
endopeptidase through K63-linked polyubiquitin therefore promoting
invasion and metastasis in breast cancer (34). However, whether TRAF6 functions as an
oncogenic factor in bladder cancer by facilitating the
ubiquitination of a downstream key molecule remain unknown. The
authors of the present study.
The finding in the present study that TRAF6
overexpression is associated with the higher recurrence and poorer
prognosis may trigger further interests in researching the
underlying function of TRAF6 in bladder cancer and further
investigation into potential chemotherapeutics for the treatment of
bladder cancer.
In conclusion, TRAF6 expression was detected in 126
urothelial bladder cancer samples, and the clinical significance of
TRAF6 expression was analyzed. It was demonstrated that TRAF6
expression was significantly associated with metastasis status,
indicating that TRAF6 may promote the tumor invasion. In univariate
and multivariate analysis, it was indicated that.
TRAF6 expression was an independent factor, which
may predict bladder cancer recurrence and prognosis.
Acknowledgements
The present study was supported by Science and
Technology Project of Yantai City (grant nos. 2015WS018 and
2016WS006), Youth Research Initiation Foundation of Yuhuangding
Hospital (grant no. 201511) and Shandong Province Medical Science
and Technology development project (grant no. 2016WS0706).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dy GW, Gore JL, Forouzanfar MH, Naghavi M
and Fitzmaurice C: Global burden of urologic cancers, 1990–2013.
Eur Urol. 71:437–446. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
La Vecchia C, Bosetti C, Lucchini F,
Bertuccio P, Negri E, Boyle P and Levi F: Cancer mortality in
Europe, 2000–2004, and an overview of trends since 1975. Ann Oncol.
21:1323–1360. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jiang X, Du L, Wang L, Li J, Liu Y, Zheng
G, Qu A, Zhang X, Pan H, Yang Y and Wang C: Serum microRNA
expression signatures identified from genome-wide microRNA
profiling serve as novel noninvasive biomarkers for diagnosis and
recurrence of bladder cancer. Int J Cancer. 136:854–862. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Babjuk M, Oosterlinck W, Sylvester R,
Kaasinen E, Böhle A, Palou-Redorta J and Rouprêt M; European
Association of Urology (EAU), : EAU guidelines on
non-muscle-invasive urothelial carcinoma of the bladder, the 2011
update. Eur Urol. 59:997–1008. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wu XR: Urothelial tumorigenesis: A tale of
divergent pathways. Nat Rev Cancer. 5:713–725. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Black PC, Brown GA and Dinney CP:
Molecular markers of urothelial cancer and their use in the
monitoring of superficial urothelial cancer. J Clin Oncol.
24:5528–5535. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cheng L, Zhang S, MacLennan GT, Williamson
SR, Lopez-Beltran A and Montironi R: Bladder cancer: Translating
molecular genetic insights into clinical practice. Hum Pathol.
42:455–481. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chiu HW, Lin SW, Lin LC, Hsu YH, Lin YF,
Ho SY, Wu YH and Wang YJ: Synergistic antitumor effects of
radiation and proteasome inhibitor treatment in pancreatic cancer
through the induction of autophagy and the downregulation of TRAF6.
Cancer Lett. 365:229–239. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Deng L, Wang C, Spencer E, Yang L, Braun
A, You J, Slaughter C, Pickart C and Chen ZJ: Activation of the
IkappaB kinase complex by TRAF6 requires a dimeric
ubiquitin-conjugating enzyme complex and a unique polyubiquitin
chain. Cell. 103:351–361. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen H, Li M, Campbell RA, Burkhardt K,
Zhu D, Li SG, Lee HJ, Wang C, Zeng Z, Gordon MS, et al:
Interference with nuclear factor kappa B and c-Jun NH2-terminal
kinase signaling by TRAF6C small interfering RNA inhibits myeloma
cell proliferation and enhances apoptosis. Oncogene. 25:6520–6527.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang KZ, Galson DL and Auron PE: TRAF6 is
autoinhibited by an intramolecular interaction which is
counteracted by trans-ubiquitination. J Cell Biochem. 110:763–771.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lamothe B, Besse A, Campos AD, Webster WK,
Wu H and Darnay BG: Site-specific Lys-63-linked tumor necrosis
factor receptor-associated factor 6 auto-ubiquitination is a
critical determinant of I kappa B kinase activation. J Biol Chem.
282:4102–4112. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Choi YB and Harhaj EW: HTLV-1 tax
stabilizes MCL-1 via TRAF6-dependent K63-linked polyubiquitination
to promote cell survival and transformation. PLoS Pathog.
10:e10044582014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chaudhry SI, Hooper S, Nye E, Williamson
P, Harrington K and Sahai E: Autocrine IL-1β-TRAF6 signalling
promotes squamous cell carcinoma invasion through paracrine TNFα
signalling to carcinoma-associated fibroblasts. Oncogene.
32:747–758. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liu J, Xu J, Li H, Sun C, Yu L, Li Y, Shi
C, Zhou X, Bian X, Ping Y, et al: miR-146b-5p functions as a tumor
suppressor by targeting TRAF6 and predicts the prognosis of human
gliomas. Oncotarget. 6:29129–29142. 2015.PubMed/NCBI
|
|
17
|
Rong Y, Wang D, Wu W, Jin D, Kuang T, Ni
X, Zhang L and Lou W: TRAF6 is over-expressed in pancreatic cancer
and promotes the tumorigenicity of pancreatic cancer cells. Med
Oncol. 31:2602014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu H, Zhang T, Ye J, Li H, Huang J, Li X,
Wu B, Huang X and Hou J: TNF receptor-associated factor 6 in
advanced non-small cell lung cancer: Clinical and prognostic
implications. J Cancer Res Clin Oncol. 138:1853–1863. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sanli O, Dobruch J, Knowles MA, Burger M,
Alemozaffar M, Nielsen ME and Lotan Y: Bladder cancer. Nat Rev Dis
Primers. 3:170222017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liu H, Xu Y, Zhang Q, Yang H, Shi W, Liu
Z, Li K, Gong Z, Ning S, Li S and Chen Y: Prognostic significance
of TBL1XR1 in predicting liver metastasis for early stage
colorectal cancer. Surg Oncol. 26:13–20. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu YF, Yang XQ, Lu XF, Guo S, Liu Y, Iqbal
M, Ning SL, Yang H, Suo N and Chen YX: Fibroblast growth factor
receptor 4 promotes progression and correlates to poor prognosis in
cholangiocarcinoma. Biochem Biophys Res Commun. 446:54–60. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Xu Y, Yang X, Li Z, Li S, Guo S, Ismail S,
Liu H, Huang Z, Zhang Z, Chen Y and Sun Q: Sprouty2 correlates with
favorable prognosis of gastric adenocarcinoma via suppressing
FGFR2-induced ERK phosphorylation and cancer progression.
Oncotarget. 8:4888–4900. 2017.PubMed/NCBI
|
|
23
|
Hemdan T, Lindén M, Lind SB, Namuduri AV,
Sjöstedt E, de Ståhl TD, Asplund A, Malmström PU and Segersten U:
The prognostic value and therapeutic target role of stathmin-1 in
urinary bladder cancer. Br J Cancer. 111:1180–1187. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yang XQ, Xu YF, Guo S, Liu Y, Ning SL, Lu
XF, Yang H and Chen YX: Clinical significance of nerve growth
factor and tropomyosin-receptor-kinase signaling pathway in
intrahepatic cholangiocarcinoma. World J Gastroenterol.
20:4076–4084. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu H, Xu Y, Zhang Q, Li K, Wang D, Li S,
Ning S, Yang H, Shi W, Liu Z and Chen Y: Correlations between
TBL1XR1 and recurrence of colorectal cancer. Sci Rep. 7:442752017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Solomon JP and Hansel DE: Prognostic
factors in urothelial carcinoma of the bladder: Histologic and
molecular correlates. Adv Anat Pathol. 22:102–112. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gogalic S, Sauer U, Doppler S and
Preininger C: Bladder cancer biomarker array to detect aberrant
levels of proteins in urine. Analyst. 140:724–735. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chan EC, Pasikanti KK, Hong Y, Ho PC,
Mahendran R, Nee Mani L Raman, Chiong E and Esuvaranathan K:
Metabonomic profiling of bladder cancer. J Proteome Res.
14:587–602. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mitra AP, Bartsch CC and Cote RJ:
Strategies for molecular expression profiling in bladder cancer.
Cancer Metastasis Rev. 28:317–326. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang M, Chu H, Li P, Yuan L, Fu G, Ma L,
Shi D, Zhong D, Tong N, Qin C, et al: Genetic variants in miRNAs
predict bladder cancer risk and recurrence. Cancer Res.
72:6173–6182. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shaid S, Brandts CH, Serve H and Dikic I:
Ubiquitination and selective autophagy. Cell Death Differ.
20:21–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pickart CM: Ubiquitin enters the new
millennium. Mol Cell. 8:499–504. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yang WL, Wang J, Chan CH, Lee SW, Campos
AD, Lamothe B, Hur L, Grabiner BC, Lin X, Darnay BG and Lin HK: The
E3 ligase TRAF6 regulates Akt ubiquitination and activation.
Science. 325:1134–1138. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lin Y, Qiu Y, Xu C, Liu Q, Peng B,
Kaufmann GF, Chen X, Lan B, Wei C, Lu D, et al: Functional role of
asparaginyl endopeptidase ubiquitination by TRAF6 in tumor invasion
and metastasis. J Natl Cancer Inst. 106:dju0122014. View Article : Google Scholar : PubMed/NCBI
|