Introduction
Anatomical irregularities of the female genital
tract resulting from abnormalities of the embryogenesis of the
Müllerian duct system are relatively common. Between 1 in 200 and 1
in 600 fertile women are reported to be affected by congenital
uterine anomalies, however, among these cases, rudimentary horns
are rare (1 in 100,000) (1).
Rudimentary horns can be subclassified into either the
communicating or non-communicating type according to whether or not
there is a cavity between the uterine cavity and the horn. The
majority of rudimentary horns are of the non-communicating type
(72–85%) (2). The majority of uterine
rudimentary horns coexist with a homolateral genitourinary tract
malformation and are asymptomatic. However, certain rudimentary
horns cause infertility, hematometra, dysmenorrhea or endometriosis
as gynecological consequences (3).
Pregnancy in such a rudimentary horn is uncommon. The present study
therefore describes an unexpected horn pregnancy with an invasive
mole, which is an extremely rare presentation. The final diagnosis
of a non-communicating rudimentary horn with pregnancy was found
intraoperatively and the presence of the invasive mole was
confirmed by histopathology.
Case report
A 29-year-old gravidity-3, parity-1, abortion-1,
live-1 female patient during a 7-week period of amenorrhea was
referred to the Department of Gynecology of Qilu Hospital of
Shandong University (Shandong, China) in March 2015, as the patient
was found to possess a uterine deformity and the presence of a
hydatidiform mole was suspected 3 days earlier. The patient
exhibited a normal menstrual cycle prior to this and the uterine
aberration had not been identified until the patient underwent a
cesarean in October 2011. A positive pregnancy test was shown 1
year prior when the patient exhibited amenorrhea for 36 days. The
patient was then diagnosed with an ectopic pregnancy and was
treated with methotrexate (MTX 50 mg intramuscularly, every other
day, 3 times daily) in The Second Hospital of Shandong University
(Shandong, China), followed by being discharged with a decreased
level (57.70 mIU/ml) of β-human chorionic gonadotropin (β-HCG) 2
weeks later (compared to 634.94 mIU/ml at the point of
admission).
The patient was asymptomatic until amenorrhea
occurred for 47 days, and a uterine anomaly and right ovarian cyst
was revealed by gynecological ultrasound in The Second Hospital of
Shandong University (Shandong, China). Another gynecological
ultrasound revealed a high possibility of a rudimentary horn of the
uterus, with a solid mass cyst and bilateral ovarian cysts. In
addition, the serum β-HCG level was >200,000 mIU/ml (normal
range, 0–10 mIU/ml), without pelvic pain or abnormal vaginal
bleeding. The patient was then admitted to Qilu Hospital of
Shandong University with a pregnancy in the rudimentary horn of the
uterus. Upon general examination, the blood pressure was 113/66
mmHg (normal range, 90/60-120/90 mmHg), with a pulse rate of 89
beats per min (normal range, 60–100 beats per min). The result of
the vaginal examination revealed normal external genitalia, and a
vagina and single cervix that appeared normal. The size of the
uterine body appeared to be that of a 2-month pregnancy. In
addition, a mass of ~5×4 cm, with mild tenderness, was palpated on
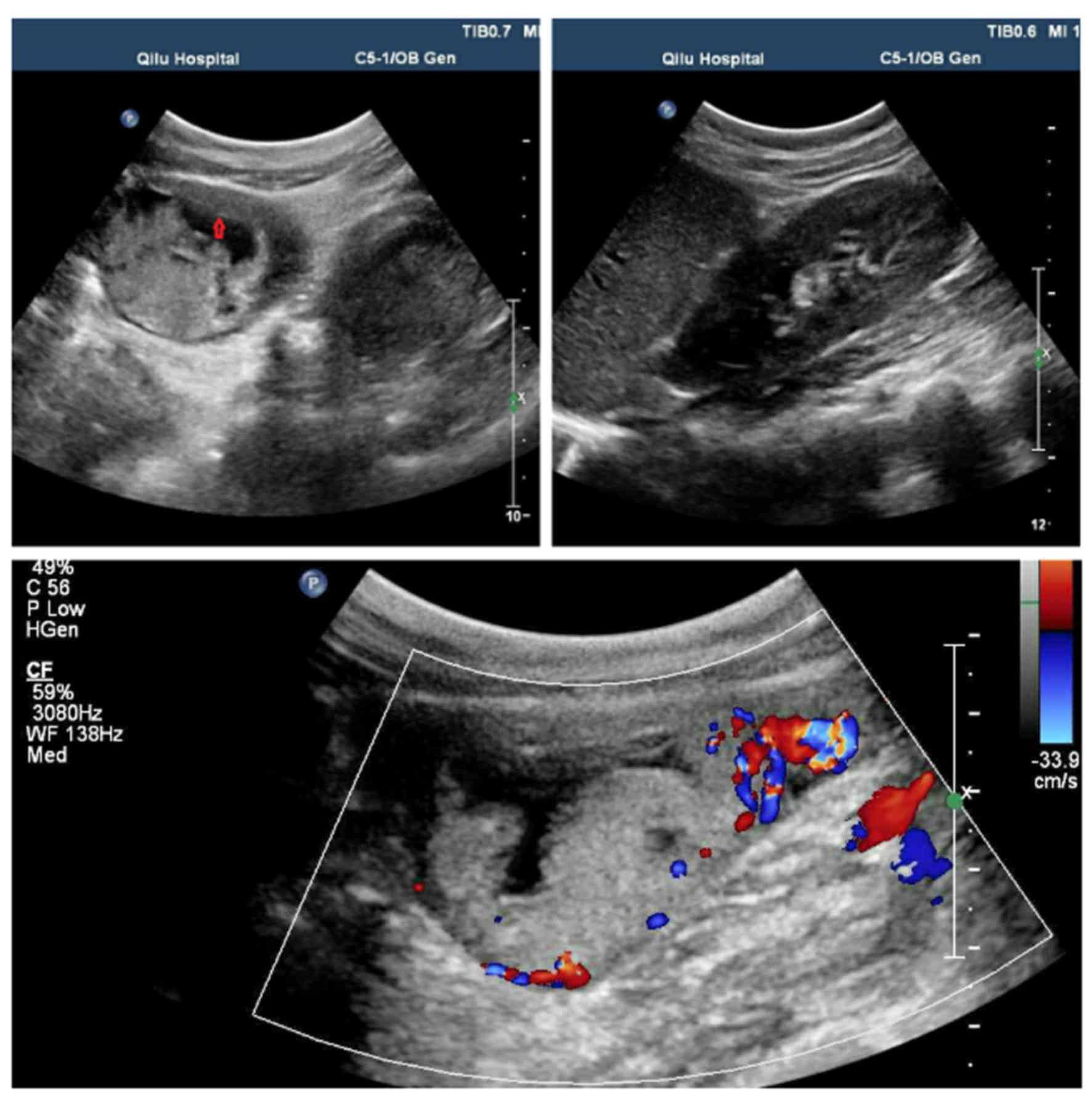
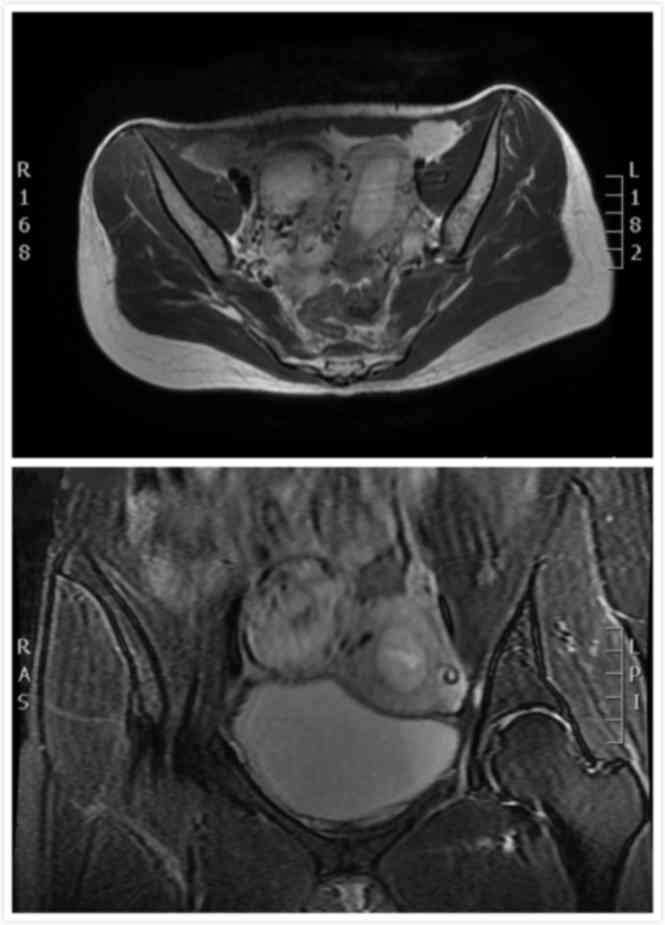
the right side of the uterus. The results of the gynecological
ultrasound and the pelvic magnetic resonance imaging (MRI) scan are
reported in Figs. 1 and 2. The ultrasound illustrates a suspicious
gestational trophoblastic disease in the rudimentary uterine horn,
with a rich blood flow signal at the right side of the uterus.
Pelvic MRI shows the endometrial thickening and gestational
trophoblastic disease in the rudimentary uterine horn. The chest
X-ray was negative.
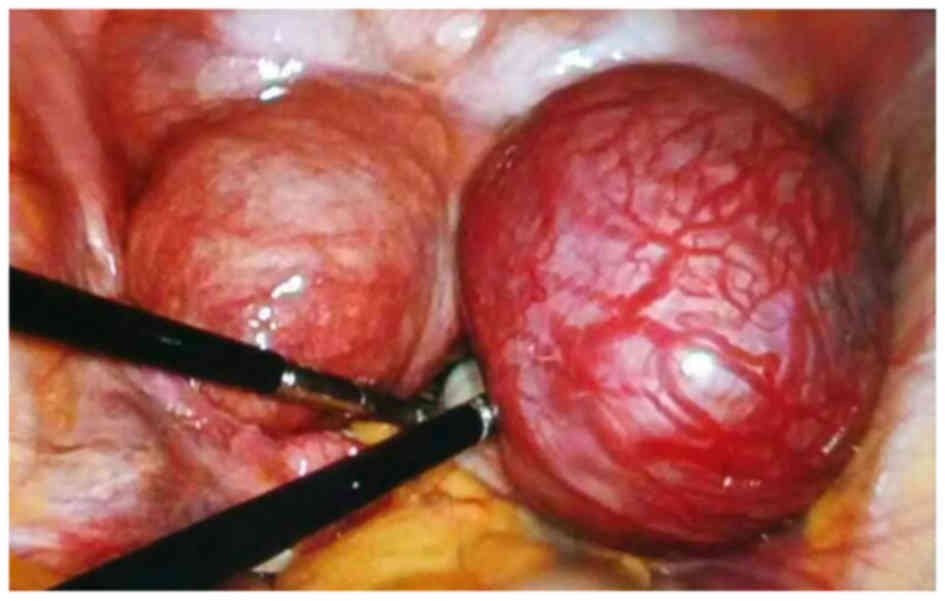
A combined hysteroscopy and laparoscopy was
performed 6 days subsequent to admission. The intraoperative
findings are shown in Fig. 3. The
uterus was increased in size, as is normal for a pregnancy at 2
months, and a normal ovary and fallopian tube was identified on the
left side. A rudimentary horn covered with tortuous and expansive
blood vessels, measuring 8×6×5 cm, was identified on the right side
of the uterus, with a normal ovary and fallopian tube attached. The
horn was connected to the right wall of the uterus above the
internal orifice of the uterus via a thin fibrous band. The
hysteroscopy revealed that the cervix and uterine cavity were
normal and that the left tubal opening was clear. However, the
right tubal opening could not be observed. The endometrium was
thick, presenting as an Arias-Stella reaction. As a result, the
rudimentary horn was dissected and diagnostic curettage was
performed by combined hysteroscopy and laparoscopy. The ipsilateral
adnexa was conserved as it appeared to be normal. The dissected
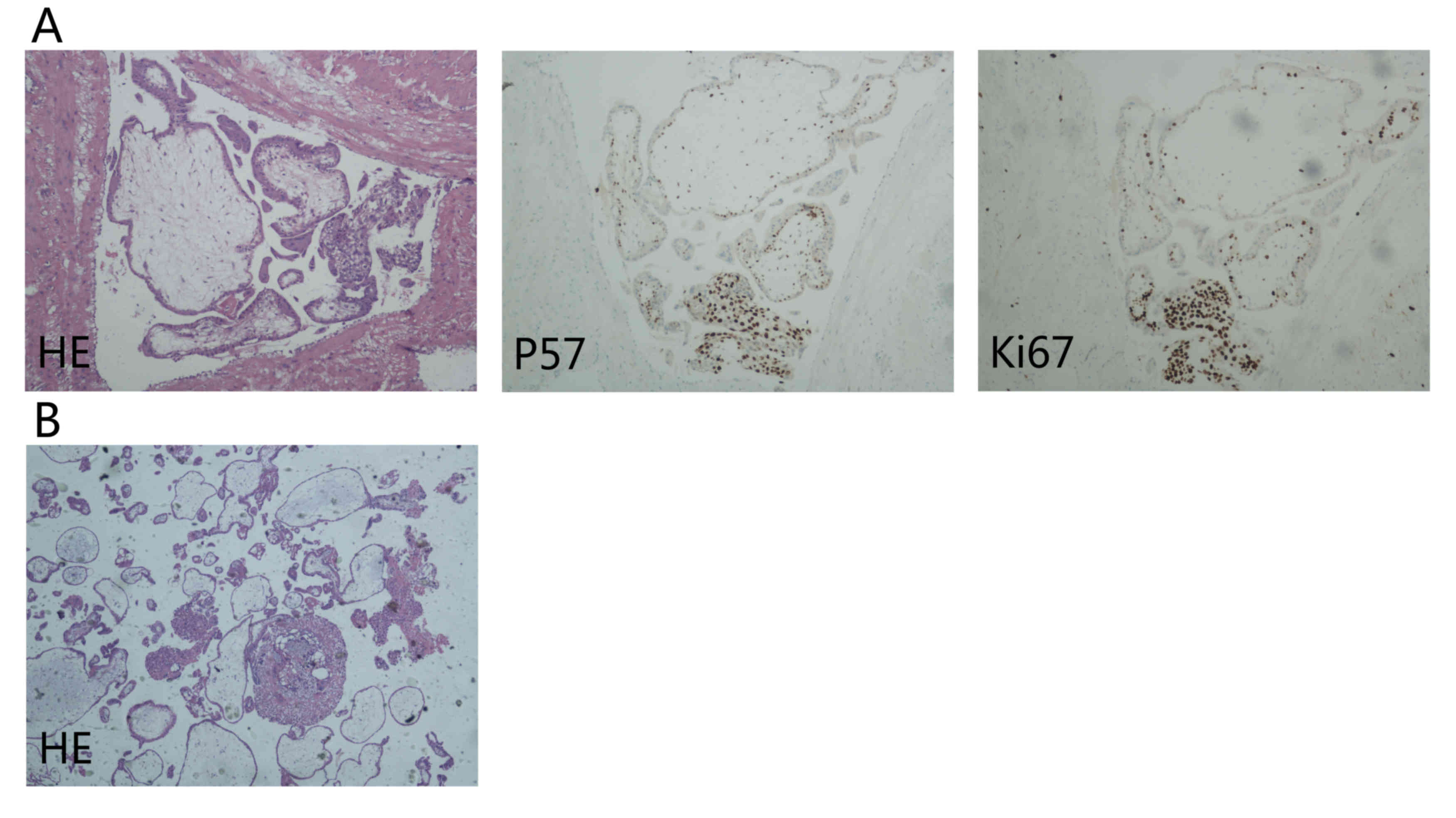
tissues were sent for routine pathological tests (Fig. 4).
Paraffin-embedded, 4-µm thick tissue sections from
the dissected tissues were stained with p57 and Ki-67 antibodies
for immunohistological analysis. All tissue sections were de-waxed,
rehydrated and incubated in 3% hydrogen peroxide for 10 min at room
temperature to halt endogenous peroxidase activity, then incubated
for 30–60 min with an anti-p57 antibody (Mouse Monoclonal Antibody;
ready-to-use dilution; cat. no., ZM-0252; ZSGB-BIO, Beijing, China)
and anti-Ki67 antibody (Rabbit Monoclonal Primary Antibody;
ready-to-use dilution, 2 ug/ml; cat. no., 790-4286; Roche
Diagnostics Shanghai Ltd., Shanghai, China) at room temperature.
Then the sections were incubated with a HRP-labeled staining
reagent (Universal Immuno-peroxidase Polymer Anti-Mouse/Rabbit
Immunohistochemical Staining reagent; ready-to-use dilution; cat.
no., PV-8000; ZSGB-BIO) at room temperature for 20 min. Sections
were developed with a DAB kit (ZSGB-BIO) used according to the
manufacturer's protocol. The tissue sections were washed 3 times
with phosphate-buffered saline (ZSGB-BIO) between each step.
Following staining, the tissue sections were counterstained using
hematoxylin (ZSGB-BIO), and subsequently dehydrated using ethanol
and xylene. Permount TM Mounting Medium (ZSGB-BIO) was then applied
to the coverslips. An ECLIPSE 80i research microscope (Nikon
Corporation, Tokyo, Japan) was used to observe the
immunohistological staining results at a magnification of
×40-x100.
Histological sections of the right rudimentary horn
revealed the myometrial invasion of massive placental villi and
metatypical trophoblastic cells (Fig.
4A). Immunohistological staining demonstrated positive
expression of p57, and a high Ki-67 proliferation index (Fig. 4A). Diagnostic curettage sections
showed the decidualized endometrium (Fig.
4B). Based on the high serum β-HCG level, imageological results
and the final pathology, the patient was diagnosed as follows:
invasive hydatidiform mole, rudimentary uterine horn and scarred
uterus. Post-operative care and follow-up were performed. Following
the surgery, the serum β-HCG level decreased from 182,232 mIU/ml to
26,086 mIU/ml. Concurrently, the patient was reluctant to undergo
chemotherapy and chose to close follow-up. The patient was
monitored with monthly serum β-HCG level examinations for the first
6 months following the operation, and then every 2 months for the
subsequent 6 months. Physical examinations and necessary imaging
examination was performed at intervals of 6–12 months. At present,
the patient has a good condition.
Discussion
Uterine rudimentary horns occur following the
partial non-development of one Müllerian duct and incomplete fusion
with the contralateral side (4). The
majority of rudimentary horns are non-communicating with the
uterine cavity, and may connect to the lower uterine segment via a
thin fibrous band. According to the American Fertility Society
classification of Müllerian anomalies (5), the patient in the present study
exhibited a non-communicating rudimentary horn of the II-b
variety.
Rudimentary horn pregnancy (RHP) is rare clinical
condition and represents a form of ectopic gestation, estimated to
occur in 1 in 100,000 to 140,000 pregnancies (6). As reported in the study by Pal et
al, Mauriceau and Vassal first described pregnancy in a
rudimentary horn in 1669 (7). Tsafrir
et al outlined the criteria for sonographic diagnoses of RHP
(8). As Siwatch et al
reported, the sensitivity of ultrasound with respect to the
diagnosis of rudimentary horn pregnancies ranges between 29 and 33%
only (9). However, MRI has a major
role with respect to the diagnosis of RHP and should be considered
when the condition is suspected (8).
Due to the maldevelopment of the musculature and
poor distensibility of the wall of the rudimentary horn, the
prognosis of RHP is often poor. The condition generally presents as
a rupture of the uterine wall between 10 and 15 gestational weeks
(10), manifesting as a
life-threatening condition of high risk, involving acute abdominal
pain with heavy intraperitoneal hemorrhage. Therefore, timely
diagnosis and management is required. However, there are certain
patients that reach a near term pregnancy (11).
Gestational trophoblastic neoplasia (GTN)
encompasses a group of pregnancy-associated disorders, including
invasive hydatidiform moles (IHMs), choriocarcinoma, placental-site
trophoblastic tumors and epithelioid trophoblastic tumors. IHM is a
benign tumor that occurs following the myometrial invasion of a
hydatidiform mole via direct extension through the tissue or venous
channels to other areas of the body subsequent to conception. While
for the majority of patients IHM commonly occurs less than half a
year after the evacuation of a molar pregnancy, the condition may
also develop subsequent to any gestation (12). The majority of affected patients
present with either vaginal bleeding subsequent to the evacuation
of a molar pregnancy, abortion, term delivery or ectopic pregnancy,
or with subinvolution of the uterus, abdominal pain or false
pregnancy symptoms. The prognosis is good, as IHM mainly causes
local invasion of myometrial invasion. A total of 10–17% of
hydatidiform moles will result in invasive moles, of which ~15%
metastasize to the lungs or the vagina (13).
Invasive moles are mostly diagnosed clinically
rather than pathologically, based on persistently elevated levels
of β-HCG subsequent to molar evacuation (14). Close monitoring of the serum β-HCG
level and imageological changes are key for the effective diagnosis
and management of GTN. The symptoms required to diagnose post-molar
GTN include at least 1 of the following (15): Levels of β-HCG that have plateaued for
4 consecutive values over 3 weeks; a β-HCG level that has risen 10%
across 3 values over 2 weeks; persistent β-HCG levels 6 months
subsequent to molar evacuation; a histopathological diagnosis of
choriocarcinoma; or the presence of metastatic disease (16). Characteristic ultrasonographic scans
of an invasive mole reveal a hyperechoic mass in the myometrium,
with an ill-defined boundary, accompanied by theca lutein ovarian
cysts. A color Doppler ultrasound will typically reveal abundant
blood flow signals in the presence of GTN (17). A chest X-ray is performed for the
diagnosis of lung metastases. If lesions are exhibited on the chest
radiograph, brain MRI and whole-body computed tomography (CT) are
recommended to exclude the possibility of a more widespread
disease. The utility of the new imaging modality of positron
emission tomography/CT scans should also be investigated.
The incidence of invasive hydatidiform moles in
rudimentary horns is extremely rare. Due to the atypical
characteristics of the condition, it is difficult to definitively
diagnose it prior to surgery (18).
IHM in a rudimentary horn is uncommon. As the number
of gestational weeks increases, the markedly enlarged rudimentary
horn can occur adjacent to the normal uterus body, easily leading
to misdiagnosis as an intrauterine pregnancy. An early diagnosis of
IHM, of which imaging examination is foremost, is essential for the
successful management of the condition in order to prevent maternal
morbidity and mortality. However, the condition is usually
diagnosed subsequent to laparoscopy or laparotomy for an acute
abdomen (7).
The excision of the rudimentary horn and an
ipsilateral salpingectomy, preferably preserving the ovary, is the
recommended treatment for patients hoping to preserve fertility
potential, thus preventing uterine rupture, future ectopic
pregnancies and dysmenorrhea (1).
Although laparotomy has traditionally been performed, with the
availability of improved laparoscopic equipment and techniques,
laparoscopic surgery has more recently been used to successfully
treat several patients (19). The
present study described the laparoscopic removal of a rudimentary
horn with IHM. In such cases, a harmonic scalpel can be utilized to
effectively amputate the uterine horn, whilst ensuring the surgical
field is relatively bloodless, thus reducing the length of the
surgery and the recovery of the patient. The rudimentary horn of
the uterus can be removed via a morcellator or a fetch bag via a
minilaparotomy. A round ligament should be fixed in the ipsilateral
cornu of the normal section of the uterus in case of uterine
torsion.
The prognosis for IHM is excellent due to its
inherent sensitivity to chemotherapy. With the adoption of the
novel International Federation of Gynecology and Obstetrics
stage-risk scoring system (15), a
score of 0–6 indicates a low risk of metastasis and a score of ≥7
suggests a high risk. Patients with low-risk metastatic GTN should
be treated with single-agent MTX or actinomycin-D chemotherapy,
with resulting survival rates approaching 100% (20). At present, an etoposide, MTX,
actinomycin D, cyclophosphamide and vincristine/oncovine
chemotherapy regimen is widely used for patients at high risk of
developing a GTN, which has resulted in improved remission and
survival rates (21). Nevertheless,
the point at which to stop chemotherapy that results in highest
efficacy and low toxic effects should be better defined. There is
no consensus with respect to the proper time point at which to stop
chemotherapy subsequent to biochemical remission (12). Generally, chemotherapy should continue
at least until the attainment of biochemical remission, and two
additional courses should be administered following the
confirmation of normal weekly serum β-HCG levels. Medical treatment
with MTX or feticide, and posterior pregnancy rudimentary horn
excision by laparoscopy has been proposed by Cutner et al
(19), with the aim of shrinking the
horn and thus facilitating a less invasive surgery.
Close follow-up should be insisted upon subsequent
to the return of the β-HCG level to normal and the completion of
chemotherapy. Patients are monitored with monthly serum β-HCG level
examinations for the first 6 months after the completion of
chemotherapy and then every 2 months for the subsequent 6 months.
Physical examinations should be performed at intervals of 6–12
months and other diagnostic techniques such as ultrasonographic
scans or X-rays are necessary. In addition, the use of
contraception is recommended for 12 months subsequent to the
completion of chemotherapy to allow for uninterrupted β-HCG
follow-up and to reduce the potential teratogenicity associated
with a subsequent pregnancy (22).
In conclusion, IHM in a rudimentary horn is rare,
and diagnosis is challenging. In view of the life-threatening
condition that follows rupture, Muram et al (23) suggested that when a rudimentary horn
of the uterus is identified prior to conception, it should be
resected prophylactically. Maintaining vigilant care and obstetric
expertise is required to prevent the morbidity associated with this
devastating condition. The removal of the uterine rudimentary horn
is essential to reduce future risk. However, excision of the
ipsilateral adnexa is controversial. In the present study, the
ipsilateral adnexa was conserved since it appeared to be normal.
Despite the removal of the RHP, the patient should be advised to
undergo chemotherapy for a better prognosis, with a close
follow-up. The present study highlights the requirement for high
clinical suspicion of this rare condition.
Glossary
Abbreviations
Abbreviations:
|
β-HCG
|
β-human chorionic gonadotropin
|
|
MTX
|
methotrexate
|
|
RHP
|
rudimentary horn pregnancy
|
|
MRI
|
magnetic resonance imaging
|
|
GTD
|
gestational trophoblastic disease
|
|
GTN
|
gestational trophoblastic
neoplasia
|
|
IHM
|
invasive hydatidiform mole
|
|
CT
|
computed tomography
|
References
|
1
|
Chopra S, Keepanasseril A, Rohilla M,
Bagga R, Kalra J and Jain V: Obstetric morbidity and the diagnostic
dilemma in pregnancy in rudimentary horn: Retrospective analysis.
Arch Gynecol Obstet. 280:907–910. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sevtap HK, Aral AM and Sertac B: An early
diagnosis and successful local medical treatment of a rudimentary
uterine horn pregnancy: A case report. Arch Gynecol Obstet.
275:297–298. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lankford J.C..Mancuso P..Appel R.:
Congenital Reproductive Abnormalities. J Midwifery Womens Health.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gonçalves E, Prata JP, Ferreira S, Abreu
R, Mesquita J, Carvalho A and Pinheiro P: An unexpected near term
pregnancy in a rudimentary uterine horn. Case Rep Obstet Gynecol.
2013:3078282013.PubMed/NCBI
|
|
5
|
The American Fertility Society
classifications of adnexal adhesions, distal tubal occlusion, tubal
occlusion secondary to tubal ligation, tubal pregnancies, mullerian
anomalies and intrauterine adhesions. Fertil Steril. 49:944–955.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pal SK, Purkait D, Modak G and Dawn CS:
Pregnancy in rudimentary horn. J Indian Med Assoc.
81:961983.PubMed/NCBI
|
|
7
|
Pal K, Majumdar S and Mukhopadhyay S:
Rupture of rudimentary uterine horn pregnancy at 37 weeks gestation
with fetal survival. Arch Gynecol Obstet. 274:325–326. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tsafrir A, Rojansky N, Sela HY, Gomori JM
and Nadjari M: Rudimentary horn pregnancy: First-trimester
prerupture sonographic diagnosis and confirmation by magnetic
resonance imaging. J Ultrasound Med. 24:219–223. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Siwatch S, Mehra R, Pandher DK and Huria
A: Rudimentary horn pregnancy: A 10-year experience and review of
literature. Arch Gynecol Obstet. 287:687–695. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nahum GG: Rudimentary uterine horn
pregnancy. The 20th-century worldwide experience of 588 cases. J
Reprod Med. 47:151–163. 2002.PubMed/NCBI
|
|
11
|
Cheng C, Tang W, Zhang L, Luo M, Huang M,
Wu X and Wan G: Unruptured pregnancy in a noncommunicating
rudimentary horn at 37 weeks with a live fetus: A case report. J
Biomed Res. 29:83–86. 2015.PubMed/NCBI
|
|
12
|
Ng TY and Wong LC: Diagnosis and
management of gestational trophoblastic neoplasia. Best Pract Res
Clin Obstet Gynaecol. 17:893–903. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lurain JR: Gestational trophoblastic
disease I: Epidemiology, pathology, clinical presentation and
diagnosis of gestational trophoblastic disease and, management of
hydatidiform mole. Am J Obstet Gynecol. 203:531–539. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lurain JR and Brewer JI: Invasive mole.
Semin Oncol. 9:174–180. 1982.PubMed/NCBI
|
|
15
|
Ngan HY, Bender H, Benedet JL, Jones H,
Montruccoli GC and Pecorelli S: FIGO Committee on Gynecologic
Oncology: Gestational trophoblastic neoplasia, FIGO staging and
classification. Int J Gynaecol Obstet. 83 Suppl 1:S175–S177. 2003.
View Article : Google Scholar
|
|
16
|
Lurain JR: Gestational trophoblastic
disease II: Classification and management of gestational
trophoblastic neoplasia. Am J Obstet Gynecol. 204:11–18. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nair K and Al-Khawari H: Invasive mole of
the uterus-a rare case diagnosed by ultrasound: A case report. Med
Ultrason. 16:175–178. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
van Esch EM, Lashley EE, Berning B and de
Kroon CD: The value of hysteroscopy in the diagnostic approach to a
rudimentary horn pregnancy. BMJ Case Rep. 2010(pii):
bcr08201032292010.PubMed/NCBI
|
|
19
|
Cutner A, Saridogan E, Hart R, Pandya P
and Creighton S: Laparoscopic management of pregnancies occurring
in non-communicating accessory uterine horns. Eur J Obstet Gynecol
Reprod Biol. 113:106–109. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Alazzam M, Tidy J, Hancock BW and Osborne
R: First line chemotherapy in low risk gestational trophoblastic
neoplasia. Cochrane Database Syst Rev. 21:CD0071022009.
|
|
21
|
Newlands ES, Mulholland PJ, Holden L,
Seckl MJ and Rustin GJ: Etoposide and cisplatin/etoposide,
methotrexate, and actinomycin D (EMA) chemotherapy for patients
with high-risk gestational trophoblastic tumors refractory to
EMA/cyclophosphamide and vincristine chemotherapy and patients
presenting with metastatic placental site trophoblastic tumors. J
Clin Oncol. 18:854–859. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Garrett LA, Garner EI, Feltmate CM,
Goldstein DP and Berkowitz RS: Subsequent pregnancy outcomes in
patients with molar pregnancy and persistent gestational
trophoblastic neoplasia. J Reprod Med. 53:481–486. 2008.PubMed/NCBI
|
|
23
|
Muram D, McAlister MS, Winer-Muram HT and
Smith WC: Asymptomatic rupture of a rudimentary uterine horn.
Obstet Gynecol. 69:486–487. 1987.PubMed/NCBI
|