Introduction
Myeloid sarcoma (MS) is a rare solid neoplasm
composed of primitive myeloid cells, which may occur in any organ
and most frequently involves the soft tissue and musculoskeletal
system. MS is most commonly detected in association with acute
myeloblastic leukemia (AML), myelodysplastic syndrome or
myeloproliferative disorders and typically occurs during the course
of active leukemia or following remission (1–4). However,
MS may occasionally occur de novo without any evidence of
concomitant hematological disease (5,6). MS most
frequently affects the bone, periosteum, lymph nodes and skin, but
unusual presentations of MS in the breast, ovary, rectum, pancreas
and urinary bladder have also been reported in previous studies
(7–9).
Central nervous system involvement of MS (CNS-MS) is very rare,
with a reported incidence of 3.25% in patients with MS (10). The presence of this tumor without
hematological disorders has been described in a small number of
isolated case reports (5,6,11).
The present study describes 4 cases of primary
CNS-MS, in which the results of hematological examinations during
hospitalization were all normal. To the best of our knowledge, this
is the largest number of cases of this disease reported in a single
study. Radiological findings, histopathological characteristics,
clinical presentation and disease management were analyzed in the
present study.
Materials and methods
The present study was approved by the Ethics Board
of Capital Medical University (Beijing, China). Informed consent
was obtained from the patients or their guardians in the case of
the patient being <18 or unable to make informed medical
decisions. The study included 3 males and 1 female who were
admitted to Beijing Tiantan Hospital (Beijing, China) between
January 2013 and December 2015, with a mean age of 28.5 years
(range, 6–54).
All patients underwent surgical treatment, and
CNS-MS diagnosis was based on pathological and immunohistochemical
staining. The resected specimens were fixed in 10% buffered
formalin and embedded in paraffin. The slides were dried at 60°C
for 1 h followed by deparaffinization in xylene (slides were
immersed in xylene for 10 min and subsequently immersed in fresh
xylene for 10 min), rehydration using graded ethanol (100% ethanol
for 3 min, 95% ethanol for 3 min, 80% ethanol for 3 min and 70%
ethanol for 3 min) and washing in distilled water for 5 min.
Sections (thickness, 5 µm) were cut for hematoxylin-eosin staining
and immunohistochemistry. Hematoxylin-eosin staining was performed
at room temperature according to the following protocol: i)
Staining in hematoxylin solution for 8 min; ii) washing with
H2O for 5 min; iii) differentiation in 1% acid ethanol
for 30 sec; iv) washing with H2O for 1 min; v) bluing in
0.2% ammonia water for 40 sec; vi) washing with H2O for
5 min; vii) counterstaining in 1% eosin solution for 5 min; viii)
washing with H2O for 2 min; ix) dehydration in
increasing concentrations of ethanol and clearing in xylene; and x)
mounting with xylene-based mounting medium. Immunohistochemical
staining was performed using monoclonal antibodies (Sigma-Aldrich;
Merck KGaA, Darmstadt, Germany) directed against myeloperoxidase
(MPO; dilution, 1:1,000; cat. no., HPA021147), glial fibrillary
acidic protein (GFAP; dilution, 1:1,000; cat. no., HPA056030),
synaptophysin (SYN; dilution, 1:200; cat. no., SAB5500180),
neurofilament protein (NF; dilution, 1:1,000; cat. no.,
SAB4700772), epithelial membrane antigen (EMA; dilution, 1:200;
cat. no., HPA004179), leukocyte common antigen [LCA/cluster of
differentiation (CD) 45; dilution, 1:50; cat. no., SAB1306481],
lysozyme (dilution, 1:500; cat. no., HPA039179), CD3 (dilution,
1:150; cat. no., SAB5500057), CD10 (dilution, 1:100; cat. no.,
SAB5500035), CD20 (dilution, 1:100; cat. no., SAB5500049), CD33
(dilution, 1:200; cat. no., HPA035832), CD34 (dilution, 1:200; cat.
no., HPA036722), CD38 (dilution, 1:100; cat. no., SAB5500063), CD56
(dilution, 1:200; cat. no., HPA039835), CD68 (dilution, 1:100; cat.
no., SAB5500070), CD99 (dilution, 1:200; cat. no., HPA035304),
CD117 (dilution, 1:200; cat. no., SAB4700750), S-100
calcium-binding protein (S-100; dilution, 1:100; cat. no.,
SAB4200671), and proliferation marker protein Ki-67 (Ki-67;
dilution, 1:200; cat. no., SAB5500134) (12). The antibodies were diluted in 5%
bovine serum albumin (Sigma-Aldrich; Merck KGaA), and the tissues
were incubated overnight at 4°C. Following use of the color
developing reagent (3,3′-diaminobenzidine; Sigma-Aldrich; Merck
KGaA) to reveal the staining, the slides were analyzed using an
Olympus BX51 microscope equipped with an Olympus DP71 digital
camera (Olympus Corporation, Tokyo, Japan).
The laboratory data were collected, including
complete blood counts, serum biochemical parameters and hepatorenal
functions. Magnetic resonance imaging (MRI) scans were performed
using a 3.0T scanner (Signa Excite 3.0T; GE Healthcare
Bio-Sciences, Pittsburgh, PA, USA), including routine T1-weighted
(TE/TR=10–20/500-700 ms), T2-weighted (TE/TR=100–120/2700-3700 ms)
and gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA)
contrasted T1-weighted (TE/TR=10–20/400-800 ms) sequences.
Additionally, diffusion-weighted imaging (TE/TR=90/6700 ms) was
performed in 1 patient (case two); computed tomography (CT) scans
were performed for 2 patients (cases two and four) using a
64-detector CT scanner (LightSpeed VCT, GE Healthcare
Bio-Sciences). Follow-up data was collected for all patients. The
clinical and radiological profiles of these patients are summarized
in Table I.
 | Table I.Clinicoradiological profiles of
patients with primary myeloid sarcoma. |
Table I.
Clinicoradiological profiles of
patients with primary myeloid sarcoma.
|
|
|
|
|
| MRI findings |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Case no. | Age, years, and
gender | Site of tumor | Symptoms | Duration of
symptoms | T1WI | T2WI | Gd-DTPA
contrasted | DWI | Tumor appearance | CT findings | Hematological
disorders | Treatment | Outcomea | Follow-up
durationb |
|---|
| 1 | 27, M | T12-S1 | Lower extremities
numbness and weakness; sciatica | 5 months | Iso | Iso | Homogeneous | N/A | Multiple | N/A | None | T12-L: GTR L5-S1: PR
+ chemo | Improved | 9 months |
| 2 | 27, M | CPA | Right tinnitus and
hearing loss | 6 months | Iso | Iso | Homogeneous | Restricted
diffusion | Solitary | Hyperdense | AML (21 days
following surgery) | STR | Posterior fossa
recurrence; succumbed | 27 days |
| 3 | 54, M | L1, L3, S1-2: | Sacrococcygeal pain
and numbness | 3 months | Iso | Iso | Homogeneous | N/A | Multiple | N/A | None | L1: Conservative L3:
GTR | In situ
recurrence | 13 months |
|
|
| Recurrence in L1,
S1-2 | Left lower extremity
weakness and numbness; sphincter disturbances | 3 months | Iso | Iso | Homogeneous | N/A | Multiple | N/A | None | L1: Conservative
S1-2: PR + chemo | Improved | 22 months |
| 4 | 6, F | Parietal lobe, left
orbit, sphenoid sinus | Headache | 10 months | Iso | Iso | Homogeneous | H/A | Multiple | Hyperdense | None | Parietal lobe lesion:
STR orbital lesion, sphenoid sinus lesion: Conservative | Improved | 29 months |
Case reports
Case one
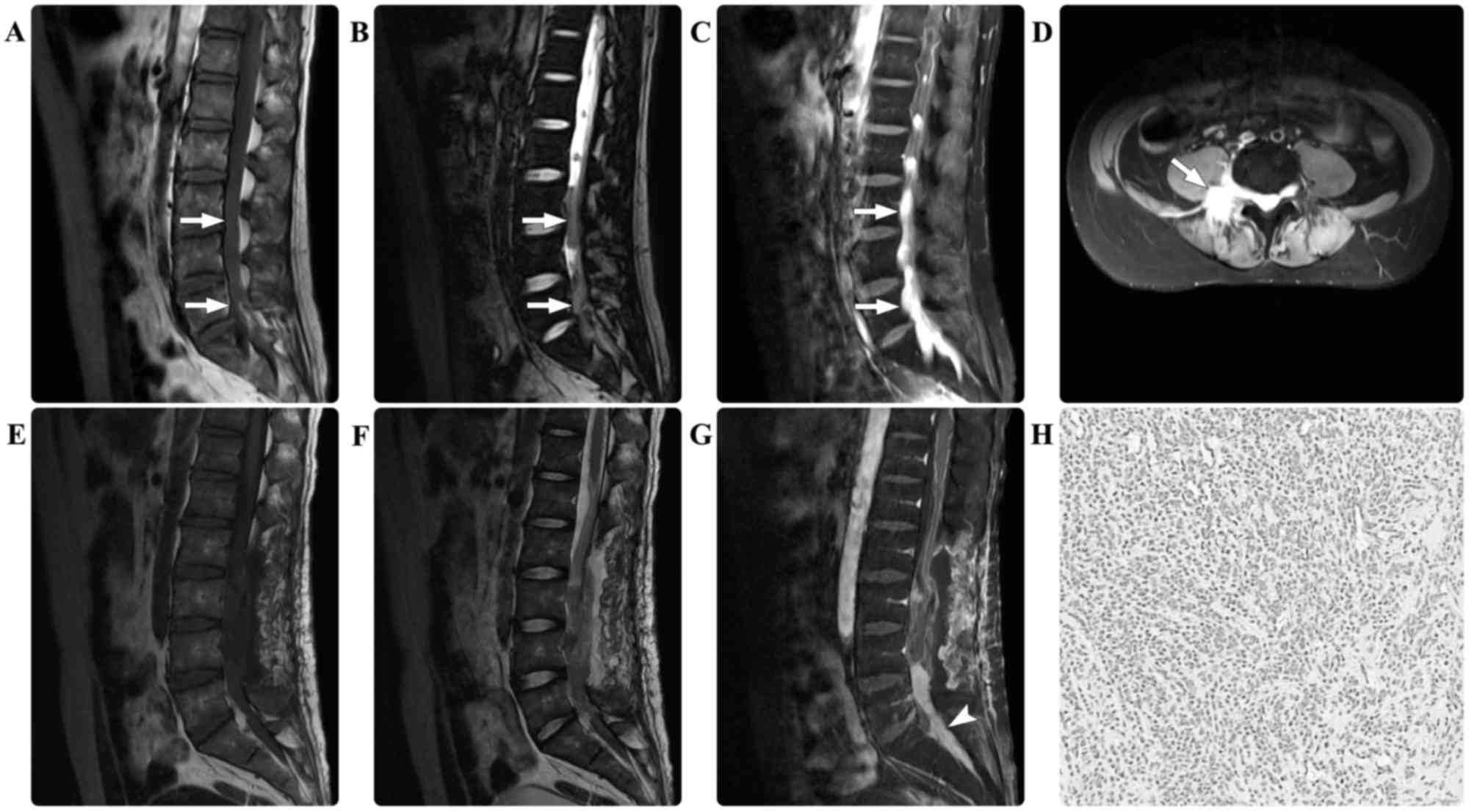
A 27-year-old male presented with a 5-month history
of numbness and weakness in the lower extremities accompanied by
sciatica. The baseline laboratory examinations of the peripheral
blood and the bone marrow at admission were all normal.
Neurological examination revealed a loss of sensation below the
lumbar (L)1 dermatome and grade 1/5 bilateral weakness of the lower
extremities. Spinal MRI scans detected multiple masses in the
spinal canal in the thoracic (T)12-sacral (S)1 region and the
sacral giant cell mass extended out from the spinal canal into the
paraspinal region. The masses were isointense on the T1- and
T2-weighted MRI scans. Following contrast agent administration, the
masses demonstrated marked homogeneous enhancement (Fig. 1). Gross total resection of the masses
in the T12-L3 region was performed, whereas the mass at the L5-S1
level was partially resected for decompression. Intraoperatively,
the lesions were intradural and highly attached to the cauda
equina. Immunohistological examination revealed the presence of
myeloid sarcoma, with positive staining for MPO, LCA, lysozyme, and
CD10, 56, 68, 99 and 117, but negative staining results for GFAP,
SYN, NF, EMA, CD20 and S-100. The marker of proliferation Ki-67
labeling index (12) was ~60%.
Repeated examinations of the peripheral blood and the bone marrow
revealed no abnormalities. Considering the potential leukemic risk,
an aggressive induction chemotherapy regime for leukemia was
administered. The patient's postoperative course was without
adverse events and the sciatica was completely relieved. During the
follow-up period of 9 months, the patient's neurological functions
improved.
Case two
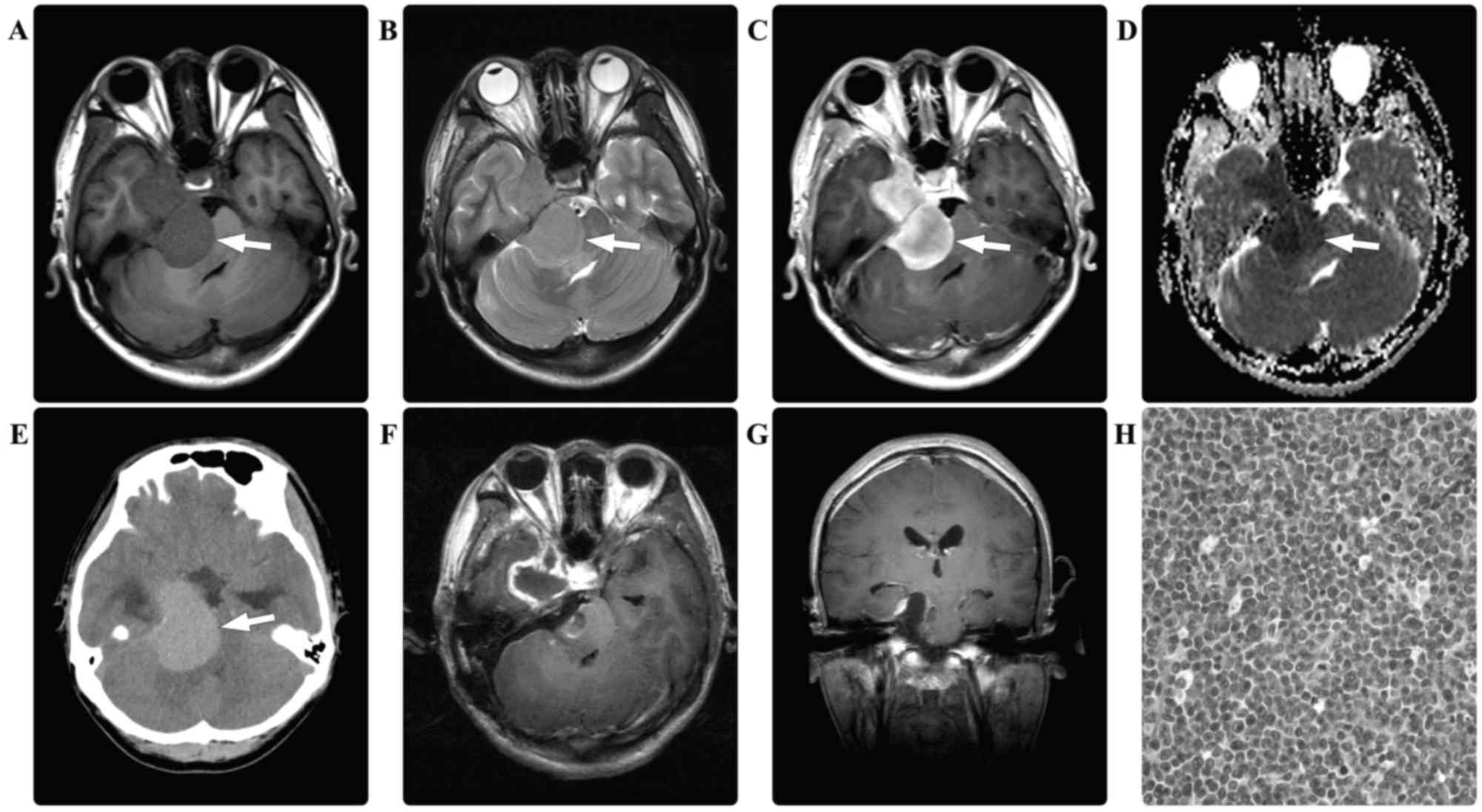
A 27-year-old male presented with a 6-month history
of right tinnitus and hearing loss. Three months prior to hospital
admission, the patient developed right-sided facial pain. There
were no relevant findings in the patient's prior medical history.
Laboratory data were all within normal limits, and no hematological
abnormalities were noted. A CT scan of the brain revealed a
hyperdense mass in the right cerebellopontine angle. A further MRI
scan of the brain revealed a dumbbell-shaped mass that appeared
isointense on the T1- and T2-weighted images, with marked
homogeneous enhancement. Diffusion-weighted imaging demonstrated
restricted diffusion of the mass (Fig.
2). A presumptive diagnosis of schwannoma and secondary
trigeminal neuralgia was made. Intraoperatively, the right
trigeminal, oculomotor and trochlear nerves were observed to be
enveloped and infiltrated by the intradural tumor. The tumor was
subtotally resected in a piecemeal manner. Immunohistological
examination revealed myeloid sarcoma, with positive staining for
MPO, LCA, lysozyme, and CD10, 33, 38, 45, 56, 68, 99 and 117, but
no staining for SYN, GFAP, NF, EMA, CD20 or S-100. The Ki-67
labeling index was ~80%. The patient's postoperative course was
without adverse events, laboratory indices were normal and he was
discharged 1 week following surgery. At 3 weeks post-surgery, the
patient was re-admitted due to vomiting, dysphagia and paraplegia.
An MRI scan of the brain revealed multiple masses with an
isointense appearance on T1- and T2-weighted images, and
homogeneous enhancement in the posterior fossa, which was presumed
to indicate the recurrence of MS. Hematological examinations
revealed AML. Due to the disease progression and a poor Karnofsky
performance scoring 20 points, no further surgical intervention was
considered. Supportive treatment (including oxygen and assisted
ventilation, monitoring, fluid and nutrition) and an AML-specific
induction chemotherapy regimen (including idarubicin at 45
mg/m2/day for 3 days and cytarabine at 100
mg/m2/day for 5 days) were scheduled. However, the
patient succumbed to the disease 6 days following his
re-admission.
Case three
A 54-year-old male presented with a 3-month history
of pain and numbness in the sacrococcygeal region. There were no
relevant findings in the patient's prior medical history. The
results of routine laboratory examinations were all normal and no
hematological abnormalities were noted. Physical examination
detected no sensorimotor disturbances. An MRI scan of the spine
revealed multiple masses in the spinal canal in the L1, L3 and
S1-S2 regions, and a giant cell sacral mass extended from the
spinal canal into the paraspinal region. The masses were isointense
on T1- and T2-weighted images. Following contrast agent
administration, the masses underwent marked homogeneous enhancement
(Fig. 3). A diagnosis of multiple
schwannomas was suspected. Gross total resection was performed on
the tumor in the L3 region; however, the tumor at the S1-S2 levels
was partially resected due to its diffuse paraspinal infiltration.
Intraoperatively, the lesions were epidural and highly attached to
the nerve roots. Immunohistological examination revealed myeloid
sarcoma, with positive staining for MPO, LCA, lysozyme, and CD3,
10, 33, 34, 38, 45, 56, 68, 99 and 117, but negative staining
results for SYN, GFAP, NF, EMA, CD20 and S-100. The Ki-67 labeling
index was ~20%. The patient's postoperative course was without
adverse events and standard laboratory test results were all
normal. Twelve months following surgery, the patient was readmitted
to hospital with a 3-month history of left lower extremity weakness
and numbness, and sphincter disturbances. Physical examination
revealed a loss of sensation below the S1 dermatome and grade 3/5
decreased muscle strength in the left lower extremity. Repeated
spinal MRI scans detected an in situ progression of the
sacral residual tumor. A second surgical resection of this tumor
was performed; however, a complete resection was unable to be
achieved. A comprehensive hematological evaluation, including
cytological examinations and chromosome analysis, was performed,
but no abnormalities were identified. Due to the potential presence
of a myeloblastic disorder and the poor prognosis, an anti-leukemia
chemotherapy regimen composed of dasatinib (100 mg/day) and Gleevec
(400 mg/day) was recommended. The patient underwent this
chemotherapy for 3 consecutive months and subsequently stopped due
to financial reasons. During the follow-up period, the patient's
neurological functions improved gradually. At a total of 22 months
following the second surgery, the patient was neurologically
asymptomatic.
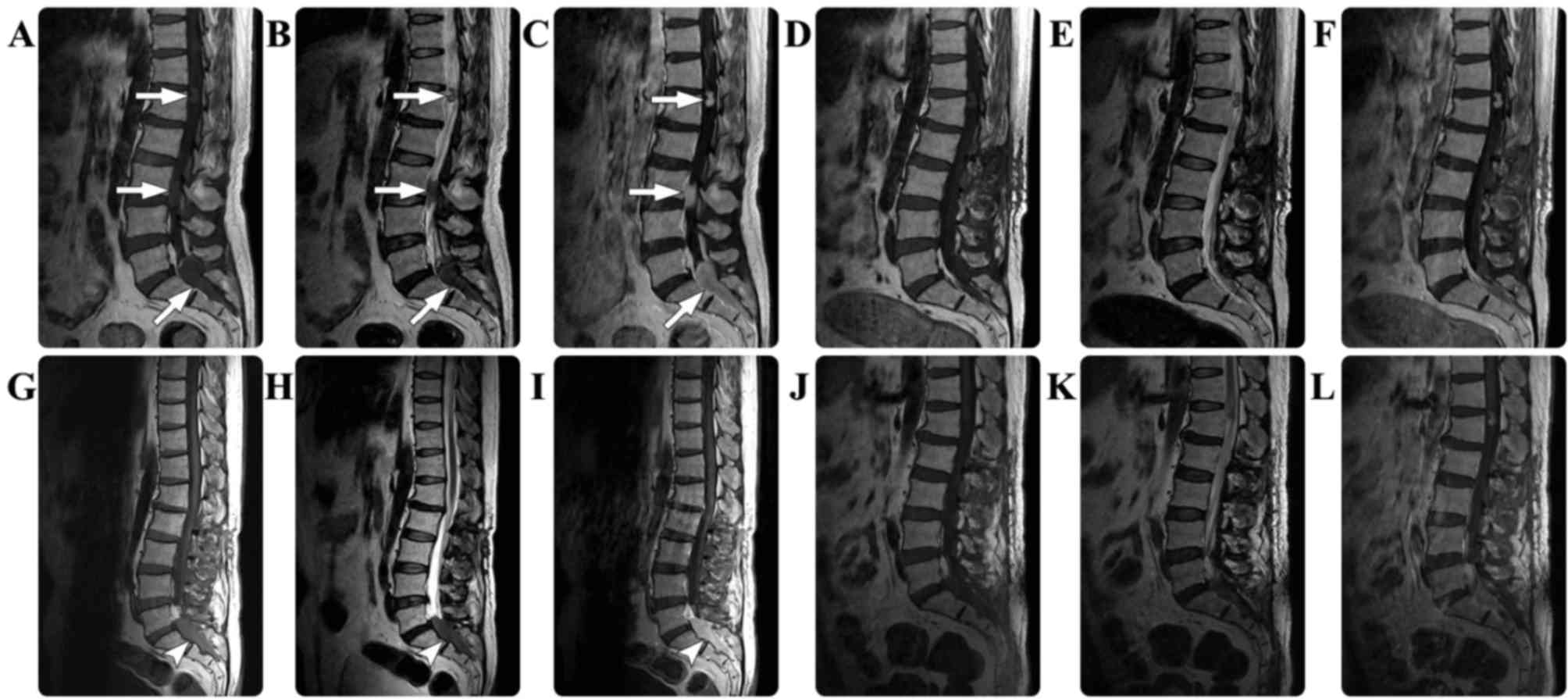 | Figure 3.In case three, the preoperative spinal
MRI scan revealed multiple masses (arrows) in the spinal canal in
the L1, L3 and S1-S2 regions, which appeared isointense on the (A)
T1-weighted and (B) T2-weighted images, with (C) marked homogeneous
enhancement. The postoperative (D) T1-weighted, (E) T2-weighted and
(F) contrasted T1-weighted images demonstrated that the mass at in
the S1-S2 region had been partially resected. Twelve months
following surgery, a repeated spinal MRI revealed in situ
progression (arrowheads) of the sacral residual tumor in the (G)
T1-weighted, (H) T2-weighted and (I) contrasted T1-weighted images.
Subsequently, a second surgical resection of this tumor was
performed, and postoperative MRI scans revealed residual tumor in
the (J) T1-weighted, (K) T2-weighted and (L) contrasted T1-weighted
images. MRI, magnetic resonance imaging; S, sacral; L, lumbar. |
Case four
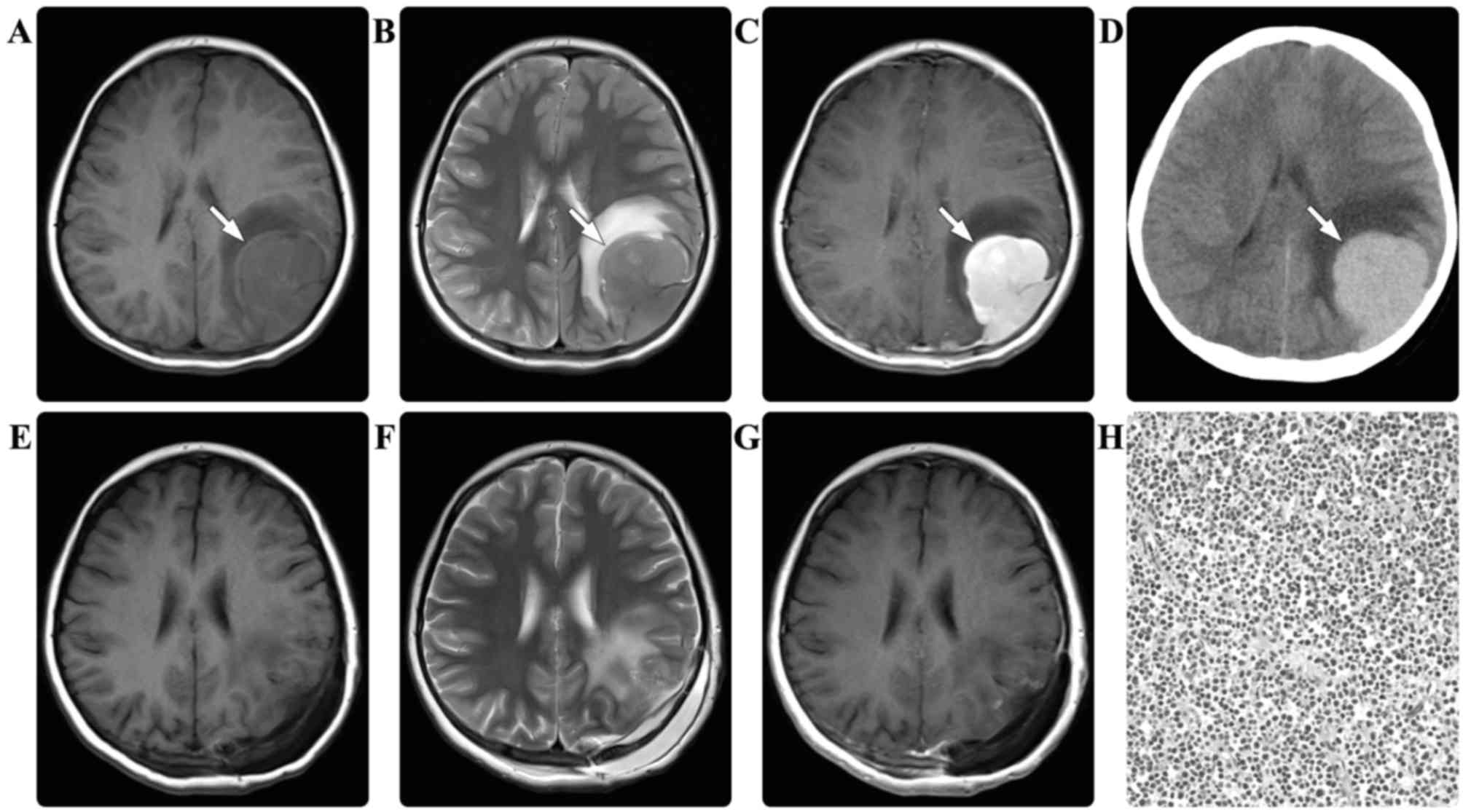
A 6-year-old female presented with a recurrent
headache for 10 days. There were no relevant findings in the
patient's prior medical history. The baseline laboratory
examination results were all normal. A CT scan of the brain
revealed multiple intracranial hyperdense masses. An MRI scan of
the brain subsequently identified a mass in the parietal lobe, the
left orbit and the sphenoid sinus. The masses were all isointense
on the T1- and T2-weighted images, with marked homogeneous
enhancement (Fig. 4). A diagnosis of
multiple schwannoma or Rosai-Dorfman disease was suspected. Due to
the symptom of left frontoparietal headache, a surgical resection
of the parietal tumor was scheduled. Intraoperatively, the dura
mater and local skull were observed to be infiltrated by the tumor.
Subtotal resection of the tumor was performed in a piecemeal manner
and the peripherally infiltrated dura mater was fulgurated.
Immunohistological examination revealed myeloid sarcoma, with
positive staining for MPO, LCA, lysozyme, and CD10, 33, 34, 45, 68,
99 and 117, but no staining for SYN, GFAP, NF, EMA, CD20, vimentin
or S-100. The Ki-67 labeling index was ~16%. The patient's
postoperative course was without adverse events and the headache
was relieved. The results of repeated laboratory examinations were
all normal. No adjuvant radiotherapy or chemotherapy was performed
due to the parents' refusal. During the follow-up period of 29
months, no disease progression was detected.
Discussion
MS has previously been termed chloroma,
extramedullary myeloid tumor or granulocytic sarcoma (13). The term chloroma is derived from the
Greek word chloros (green), as the appearance of the lesion is
typically green due to high levels of myeloperoxidase expression;
however, this is not always applicable as the color may rapidly
fade upon oxygen exposure (14). The
2008 World Health Organization classification adopted the term
‘myeloid sarcomas’ as a subgroup of ‘acute myeloid leukemias, not
otherwise categorized’ (15). This
type of malignancy frequently occurs during the course of active
hematological disease, including acute or chronic leukemia and
myeloproliferative disorder, or occurs during remission from
leukemia (1–4). CNS-MS is uncommon, and it has been
suggested that it may occur when leukemic cells pass from the bone
marrow of the skull to the dura, subarachnoid space and
Virchow-Robin spaces, resulting in invasion of the brain surface
(16). However, there remains a
highly rare variant, primary CNS-MS, presenting as isolated solid
neoplasms in the brain or spinal cord and occurring de novo
with no apparent signs or symptoms of concomitant hematological
disease (5,6,11).
According to the classification proposed by Audouin
et al (17), there are four
varied patterns of MS: i) MS that develops during the active phase
of leukemia; ii) MS that develops alongside known chronic
myeloproliferative disorders; iii) MS that manifests as a relapse
months or years following clinical remission from AML, particularly
following bone marrow transplantation; and iv) MS preceding AML
diagnosis, which may be detected in previously healthy individuals
with no blast cell infiltration into the bone marrow and a normal
peripheral blood cell count. As described by Krause (18), patients with MS without leukemic
evidence accounted for 0.6% of all MS cases. The pathogenesis of
isolated CNS-MS without bone marrow involvement remains to be
elucidated; however, relevant clinical profiles suggest that CNS-MS
may portend a potential or delayed leukemia (19–21).
According to a previous study, the majority of patients with
isolated CNS-MS may progress to myeloid leukemia with blast cell
infiltration at an average of 10.5 months following the
pathological diagnosis of MS (3).
Clinical manifestations of CNS-MS are nonspecific
and are associated with increased intracranial pressure or
space-occupying effects (6,11). The radiological features of CNS-MS are
typically characterized by the presence of an isodense or
hyperdense mass on CT scan images, with marked homogeneous
enhancement following contrast agent administration (22). The appearance of CNS-MS via MRI is
typically hypointense to isointense on T1- and T2-weighted images,
with marked enhancement following the administration of a contrast
agent (23,24). Radiological differential diagnoses may
include meningioma, lymphoma and schwannoma. Obtaining a
preoperative diagnosis is challenging and isointense signal
characteristics may be suggestive of CNS-MS.
The definitive diagnosis of CNS-MS may depend upon
pathological and immunohistochemical evidence. MPO is a specific
antigen marker for MS (25). In the
present study, the tumor specimens from all patients were positive
for MPO, CD68 and CD45, which is consistent with data from a
previous study (26). Histological
differential diagnoses comprise various small cell tumors,
including Burkitt's lymphoma, embryonal rhabdomyosarcoma and
Ewing's sarcoma.
The optimal treatment for CNS-MS remains the subject
of debate. The typical therapeutic option is a combination of local
surgical resection and chemotherapy (1–4,11,26).
However, there are several challenges to treatment that arise as a
result of isolated CNS-MS. Complete surgical resection is
challenging due to the extensive infiltration of MS into the
surrounding tissues and, in the majority of cases, only subtotal or
partial resection is achieved. In the present study, an in
situ progression of the residual tumor was observed in case
three. In this case, complete surgical resection was difficult and
not enforced in the second surgical procedure, with adjuvant
chemotherapy aiding long-term tumor remission. Additionally, the
administration of chemotherapy remains problematic for cases of
primary CNS-MS without leukemic evidence. In the present study,
case one was managed using an aggressive induction chemotherapy
regime for leukemia; the clinical improvement and event-free
follow-up in this patient supports the decision to perform an
aggressive treatment. In case two, chemotherapy was not
administrated in a timely manner and upon the detection of leukemia
the condition was not manageable. In case four, 1 tumor was
subtotally resected and the remaining 2 tumors were conservatively
observed. Although no chemotherapy was administered, the disease
did not progress during the 29-month follow-up period. The low
Ki-67 index may provide an explanation for the indolent disease
course in this patient. Considering the risk of progression to
leukemia, the results of the present study indicate that systematic
chemotherapy be included in the treatment for all CNS-MS cases.
In conclusion, primary CNS-MS without leukemic
evidence is highly rare and has distinctive radiological
characteristics. Due to its diffuse tissue infiltration, completely
surgical resection of this type of tumor is challenging. It is
important for clinicians to be aware of potential hematological
disorders in patients with CNS-MS. A combined surgical and
chemotherapeutic strategy may facilitate long-term remission in
this group.
References
|
1
|
Collins C and Knoderer H: Central nervous
system involvement at the time of presentation in acute
promyelocytic leukemia. Pediatr Blood Cancer. 54:603–605.
2010.PubMed/NCBI
|
|
2
|
Colović N, Colović M, Cemerikić V, Terzić
T, Ivanović S, Skender M and Bosković D: Granulocytic sarcoma of
the brain in a patient with acute myeloid leukemia. Acta Chir
Iugosl. 51:129–131. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cervantes GM and Cayci Z: Intracranial CNS
manifestations of myeloid sarcoma in patients with acute myeloid
leukemia: Review of the literature and three case reports from the
author's institution. J Clin Med. 4:1102–1112. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cho SF, Liu TC and Chang CS: Isolated
central nervous system relapse presenting as myeloid sarcoma of
acute myeloid leukemia after allogeneic peripheral blood stem cell
transplantation. Ann Hematol. 92:133–135. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Piñán MA, Ardanaz MT, Guinea JM and
García-Ruiz JC: Myeloid sarcoma preceding an acute promyelocytic
leukaemia with neuromeningeal infiltration. Ann Hematol.
93:339–340. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Widhalm G, Dietrich W, Müllauer L,
Streubel B, Rabitsch W, Kotter MR, Knosp E and Roessler K: Myeloid
sarcoma with multiple lesions of the central nervous system in a
patient without leukemia. Case report. J Neurosurg. 105:916–919.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Breccia M, D'Andrea M, Mengarelli A,
Morano SG, D'Elia GM and Alimena G: Granulocytic sarcoma of the
pancreas successfully treated with intensive chemotherapy and stem
cell transplantation. Eur J Haematol. 70:190–192. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fitoz S, Atasoy C, Yavuz K, Gozdasoglu S,
Erden I and Akyar S: Granulocytic sarcoma. Cranial and breast
involvement. Clin Imaging. 26:166–169. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aki H, Baslar Z, Uygun N, Ozguroglu M and
Tuzuner N: Primary granulocytic sarcoma of the urinary bladder:
Case report and review of the literature. Urology. 60:3452002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pileri SA, Ascani S, Cox MC, Campidelli C,
Bacci F, Piccioli M, Piccaluga PP, Agostinelli C, Asioli S, Novero
D, et al: Myeloid sarcoma: Clinico-pathologic, phenotypic and
cytogenetic analysis of 92 adult patients. Leukemia. 21:340–350.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang C, Liu Y, Li G, Bai J, Qian J and Xu
Y: Multifocal myeloid sarcoma in the central nervous system without
leukemia. Clin Neurol Neurosurg. 120:99–102. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Karamitopoulou E, Perentes E, Diamantis I
and Maraziotis T: Ki-67 immunoreactivity in human central nervous
system tumors: A study with MIB 1 monoclonal antibody on archival
material. Acta Neuropathol. 87:47–54. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Campidelli C, Agostinelli C, Stitson R and
Pileri SA: Myeloid sarcoma: Extramedullary manifestation of myeloid
disorders. Am J Clin Pathol. 132:426–437. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cho WH, Choi YJ, Choi BK and Cha SH:
Isolated recurrence of intracranial granulocytic sarcoma mimicking
a falx meningioma in acute myeloblastic leukemia. J Korean
Neurosurg Soc. 47:385–388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vardiman JW, Thiele J, Arber DA, Brunning
RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM,
Hellström-Lindberg E, Tefferi A and Bloomfield CD: The 2008
revision of the World Health Organization (WHO) classification of
myeloid neoplasms and acute leukemia: Rationale and important
changes. Blood. 114:937–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Azzarelli V and Roessmann U: Pathogenesis
of central nervous system infiltration in acute leukemia. Arch
Pathol Lab Med. 101:203–205. 1977.PubMed/NCBI
|
|
17
|
Audouin J, Comperat E, Le Tourneau A,
Camilleri-Broët S, Adida C, Molina T and Diebold J: Myeloid
sarcoma: Clinical and morphologic criteria useful for diagnosis.
Int J Surg Pathol. 11:271–282. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Krause JR: Granulocytic sarcoma preceding
acute leukemia: A report of six cases. Cancer. 44:1017–1021. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hurwitz BS, Sutherland JC and Walker MD:
Central nervous system chloromas preceding acute leukemia by one
year. Neurology. 20:771–775. 1970. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Llena JF, Kawamoto K, Hirano A and Feiring
EH: Granulocytic sarcoma of the central nervous system: Inital
presentation of leukemia. Acta Neuropathol. 42:145–147. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Piñán MA, Ardanaz MT, Guinea JM and
García-Ruiz JC: Myeloid sarcoma preceding an acute promyelocytic
leukaemia with neuromeningeal infiltration. Annals Hematol.
93:339–340. 2014. View Article : Google Scholar
|
|
22
|
Sowers JJ, Moody DM, Naidich TP, Ball MR,
Laster DW and Leeds NE: Radiographic features of granulocytic
sarcoma (chloroma). J Comput Assist Tomogr. 3:226–233. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chaudhry AA, Gul M, Chaudhry AA and Dunkin
J: Qualitative assessment of diffusion weighted imaging and
susceptibility weighted imaging of myeloid sarcoma involving the
brain. J Comput Assist Tomogr. 40:61–66. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pui MH, Fletcher BD and Langston JW:
Granulocytic sarcoma in childhood leukemia: Imaging features.
Radiology. 190:698–702. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pinkus GS and Pinkus JL: Myeloperoxidase:
A specific marker for myeloid cells in paraffin sections. Mod
Pathol. 4:733–741. 1991.PubMed/NCBI
|
|
26
|
Qian J, Cui QU, Liu Y, Li X, Sun X, Zhu H
and Wang C: Isolated primary intracranial myeloid sarcoma with
neuromeningeal infiltration: A case report. Oncol Lett.
9:1647–1650. 2015.PubMed/NCBI
|