Introduction
Spontaneous rupture of hepatocellular carcinoma
(SRHCC) is a rare but fatal complication observed in patients with
hepatocellular carcinoma (HCC). The incidence of SRHCC in patients
with HCC is between 3 and 15%, and such patients exhibit a poor
therapeutic outcome. In addition, the mortality rate of patients
with SRHCC is currently between 50 and 80% (1,2). A
previous study of 12 patients with SRHCC who received a
hepatectomy, observed that 1 patient (8.3%) with Child-Pugh class B
survived for only 4 days and succumbed to liver failure [the
diagnosis of liver failure was according to the American
Association for the Study of Liver Diseases (3)]; the remaining 11 patients (91.7%) had a
median survival time of 16.5 months (4). Hepatectomy for patients with SRHCC
prolongs their mean survival time; however, there have been
instances of post-operative liver failure leading to mortality.
Potential reasons for this may be: First, patients with SRHCC
experience various extents of blood loss prior to surgery, which
may result in hemodynamic changes or even decreased hepatic blood
supply; secondly, liver ischemia/reperfusion as a result of surgery
and portal triad clamping may further aggravate liver injury; and
lastly, concomitant hepatic cirrhosis also predicts a poor
prognosis (5). The prognosis of
patients with SRHCC may therefore be improved if liver injury is
attenuated and the risk of liver failure following surgery is
minimized. Between January 1970 and February 2010, a total of 38
patients with SRHCC received a hepatectomy at Xiangya Hospital and
Xiangya Third Hospital (Changsha, China), and 18 patients received
a hepatectomy without portal triad clamping which resulted in
attenuation of liver injury and decreased short-term mortality.
Patients and methods
Patients
A total of 38 patients with SRHCC underwent a
hepatectomy at Xiangya Hospital and Xiangya Third Hospital between
January 1970 and February 2010. The present study was approved by
the Ethics Committee of Xiangya Third Hospital and informed written
consent was obtained from each patient. Patients that were treated
with sorafenib, transcatheter arterial embolization (TAE) or
transcatheter arterial chemoembolization (TACE) were excluded. The
sample comprised 31 male and 7 female patients ranging between 22
and 68 years of age. Non-coagulable blood was observed following
abdominal paracentesis, and postoperative pathology revealed HCC,
confirming the diagnosis of SRHCC. The following criteria were used
for the selection of patients with SRHCC for emergency hepatectomy:
i) Patients were in a good general condition of health prior to
SRHCC; ii) shock [systolic blood pressure ≤70 mmHg or systolic
blood pressure between 71 and 90 mmHg with heart rate ≥108 beats
per min (6)] was rapidly controlled
shortly following admission; iii) hepatic cirrhosis was mild during
the surgery; iv) cancer was confined to a single lobe and
clinicians had no difficulty in performing the hepatectomy; and v)
there were no metastatic foci.
Grouping
In the present retrospective study, patients were
divided into two groups on the basis of hepatic portal triad
clamping during surgery (the clamping group and non-clamping
group).
The portal triad clamping maneuver was routinely
used with cycles of clamp/unclamp times of 15/5 min. There were 20
patients in the clamping group including 16 males and 4 females.
The median age was 51 years (range, 22–60 years). A total of 14
patients in this group (70%) had a history of hepatitis B and 2
patients had a concomitant Schistosoma infection. All 20
patients exhibited abdominal pain, 14 patients (70%) had
generalized peritonitis and 7 patients (35%) had shock. Notably, 16
patients (80%) had serum AFP >200 U/l. All 20 patients underwent
ultrasonography and 11 patients received computed tomography scans.
The two procedures revealed space-occupying lesions in the liver.
Concomitant hepatic cirrhosis was noted in 14 patients (70%),
Child-Pugh class A in 16 patients (80%) and Child-Pugh class B in 4
patients (20%) according to the Child-Pugh classification (7). A total of 19 patients (95%) exhibited a
single cancer and 1 patient (5%) exhibited multiple foci in the
liver. The diameter of tumors ranged between 6.0 and 10.5 cm (mean,
8 cm).
There were 18 patients in the non-clamping group,
including 15 males and 3 females. The median age was 56 years
(range, 26–68 years). A total of 15 patients (83.3%) had a history
of hepatitis B (HBV) and 1 patient had a concomitant
Schistosoma infection. All 18 patients exhibited abdominal
pain, 13 patients (72.2%) exhibited signs of generalized
peritonitis and 7 patients (38.9%) had shock. Notably, 15 patients
(83.3%) had serum AFP >200 U/l. A total of 11 patients underwent
ultrasonography and 16 patients received computed tomography scans.
The two procedures revealed space-occupying lesions in the liver
and ascites. Concomitant hepatic cirrhosis was noted in 14 patients
(77.8%), Child-Pugh class A in 12 patients (66.7%) and Child-Pugh
class B in 6 patients (33.3%). A total of 16 patients (88.9%) had a
single cancer, whereas 2 patients (11.1%) had multiple foci in the
liver. The diameter of tumors ranged between 7.0 and 12.5 cm (mean,
9 cm). There were no marked differences in clinical
characteristics, Child-Pugh classification or cancer diameter
between the two groups (Table I).
 | Table I.Preoperative data for patients
undergoing hepatectomy with or without portal triad clamping. |
Table I.
Preoperative data for patients
undergoing hepatectomy with or without portal triad clamping.
| Parameter | Clamping group
n=20 | Non-clamping group
n=18 | P-value |
|---|
| Mean age (range),
years | 51 (22–60) | 56 (26–68) | NS |
| Sex |
|
| NS |
| Male | 16 | 15 |
|
|
Female | 4 | 3 |
|
| Mean tumor size
(range), cm | 8 (6–10.5) | 9 (7–12.5) | NS |
| Number of tumors |
|
| NS |
|
Single | 19 | 16 |
|
|
Multiple | 1 | 2 |
|
| Hemoglobin, g/l | 83.4±8.4 | 78.3±7.7 | NS |
| Platelet count,
×109/l | 109.7±9.3 | 89.2±10.5 | NS |
| Child-Pugh class |
|
| NS |
| A | 16 | 12 |
|
| B | 4 | 6 |
|
| With liver
cirrhosis | 14 | 14 | NS |
| HBsAg-positive | 14 | 15 | NS |
Therapeutic protocol
Clamping group
The hepatic portal triad was clamped at room
temperature for a mean of 9 min (range, 2–22 min). Of the 20
patients, 19 received an emergency hepatectomy and peritoneal
lavage. Of the patients who received an emergency hepatectomy, 8
patients received a left lateral lobectomy, 2 patients received a
left inner lobectomy and 1 patient received a left hepatectomy. A
total of 3 patients received a regional HCC resection and 5
patients received a partial right hepatectomy. All 20 patients had
hemostasis with gauzes and peritoneal lavage due to lack of a blood
source, with a second left hepatectomy performed 36 h later.
Intra-operative pathology revealed that the surgical margin was
negative in patients who received regional HCC resections. Oxygen
inhalation, fluid supplementation and administration of albumin and
broad-spectrum antibiotics were performed post-operatively.
Patients treated later than the year 2000 received oral lamivudine
(100 mg per day) following surgery when HBV DNA levels were >500
copies/ml.
Non-clamping group
Hepatectomy was performed without portal triad
clamping. All 18 patients received an emergency hepatectomy and
peritoneal lavage. A total of 6 patients received a left lateral
lobectomy, 2 patients received a left inner lobectomy and 2
patients received a left hepatectomy. A total of 4 patients
received a regional HCC resection and 4 patients received a partial
right hepatectomy. Intra-operative pathology revealed that the
surgical margin was negative in patients who received regional
hepatectomy. Intra-operative peritoneal lavage and other
post-operative therapies were identical with those in the clamping
group.
Observations and clinical evaluations
The intra-operative blood loss, volume of blood
transfusion, surgical time, incidence of post-operative
complications and mortality were compared between the two
groups.
Fresh liver specimens were obtained during surgery
and examined immediately by pathologists with hematoxylin and eosin
(HE) staining. Hemoglobin (Hb), platelets (PLT), alanine
aminotransferase (ALT), aspartate aminotransferase (AST), total
bilirubin (TBil), fibrinogen (FBI) and α-fetoprotein (AFP) levels
were determined, and prothrombin (PT) and kaolin partial
thromboplastin (KPTT) times were recorded prior to, and at 1 week
and 2 weeks after, hepatectomy. Ultrasonography and/or computed
tomography scans were used for imaging the liver prior to, and at 2
weeks after, hepatectomy. The liver tissue samples collected during
surgery were processed for pathological examination.
Follow-up
All the patients received follow-up examinations.
The disease-free and overall survival times were determined.
Statistical analysis
Quantitative data are shown as the mean ± standard
deviation. Quantitative data obtained were compared among the
groups by one-way analysis of variance followed by Tukey's post-hoc
test. Qualitative data were analyzed using a χ2 test and
survival analysis was calculated using the Kaplan-Meier estimator
method with a log-rank test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Evaluation of intra-operative blood
loss, blood transfused, surgery time, mortality and incidence of
post-operative complications
In the clamping group, intra-operative blood loss
was between 50 and 3,625 ml, the volume of blood transfused was
between 100 and 4,200 ml, and the operative time was between 90 and
280 min. Surgical complications observed among the clamping group
included acute liver failure (5 patients), gastrointestinal
bleeding (1 patient), lung infection (3 patients) and wound
infection (4 patients). In the clamping group, 1 patient succumbed
to acute liver failure 4 days after surgery (mortality rate of 5%).
In the non-clamping group, the intra-operative blood loss was
between 100 and 2,900 ml, volume of blood transfused was between 0
and 3,000 ml, and the operative time was between 90 and 320 min.
Surgical complications in this group included lung infection (1
patient) and wound infection (2 patients). All these patients
recovered following non-surgical therapies and acute liver failure;
gastrointestinal bleeding and mortality were not observed (Table II). The non-clamping group exhibited
a significantly lower incidence of acute liver failure compared
with the clamping group (P<0.05), but no significant differences
in blood loss, volume of blood transfused, operative time or
mortality rate between the two groups were identified (all
P>0.05).
| Table II.Operative data for undergoing
hepatectomy with or without portal triad clamping. |
Table II.
Operative data for undergoing
hepatectomy with or without portal triad clamping.
| Parameter | Clamping group
n=20 | Non-clamping group
n=18 | P-value |
|---|
| Mean operative time
(range), min | 189.5 (90–280) | 194.4 (90–320) | NS |
| Mean blood loss
(range), ml | 989.8
(50–3,625) | 1061.0
(100–2,900) | NS |
| Mean blood
transfusion (range), ml | 921.0
(100–4,200) | 895.0
(0–3,000) | NS |
| Treatment |
|
|
|
|
Emergency hepatectomy | 19 | 18 | NS |
| Staged
hepatectomy | 1 | 0 | NS |
| Type of
resection |
|
|
|
| Left
lateral lobectomy | 8 | 6 | NS |
| Left
lobe resection | 2 | 2 | NS |
| Left
liver resection | 2 | 2 | NS |
|
Limited | 3 | 4 | NS |
| Partial
right hepatectomy | 5 | 4 | NS |
| Complication |
|
|
|
|
Total | 13 | 3 | 0.0026 |
|
Gastrointestinal bleeding | 1 | 0 | NS |
|
Pulmonary infection | 3 | 1 | NS |
| Acute
liver failure | 5 | 0 | 0.0228 |
| Wound
infection | 4 | 2 | NS |
Blood levels of Hb, PLT, ALT, AST,
TBil, PT, KPTT, FBI and AFP
No significant differences were observed in Hb, PLT,
ALT, AST, TBil, PT, KPTT, FBI or AFP between the two groups prior
to surgery (all P>0.05). Serum ALT, AST and TBil levels in the
non-clamping group were significantly decreased at 1 week and 2
weeks after surgery compared with the clamping group (all
P<0.05), but no significant differences in Hb, PLT, PT, KPTT,
PFIB or AFP levels between the two groups were observed (all
P>0.05; Fig. 1).
 | Figure 1.Levels of (A) Hb, (B) PLT, (C) ALT,
(D) AST, (E) TBil, (F) PT, (G) KPTT, (H) FBI and (I) AFP prior to,
and 7 and 14 days after, clamping or non-clamping hepatectomy (mean
± standard deviation). At 1 week and 2 weeks after surgery, the
non-clamping group exhibited significantly lower serum levels of
ALT, AST and TBil compared with the clamping group (all P<0.05).
Hb, hemoglobin; PLT, platelets; ALT, alanine aminotransferase; AST,
aspartate aminotransferase; TBil, total bilirubin; PT, prothrombin
time; KPTT, kaolin partial thromboplastin time; FBI, fibrinogen;
AFP, α-fetoprotein. |
Liver imaging examinations
Prior to surgery, computed tomography scans of the
liver in the two groups revealed space-occupying lesions surrounded
by multiple high-intensity hematomas and hemoperitoneum (Fig. 2A). At 2 weeks after surgery, computed
tomography scans of the liver revealed no space-occupying lesions
in the liver and surrounding hematomas, and hemoperitoneum were not
observed (Fig. 2B).
Pathological examination
Pathological examination of specimens from the two
groups revealed HCC with hemorrhagic necrosis and hematoma
(Fig. 3A), as well as venous rupture
and thrombi at the site of rupture (Fig.
3B).
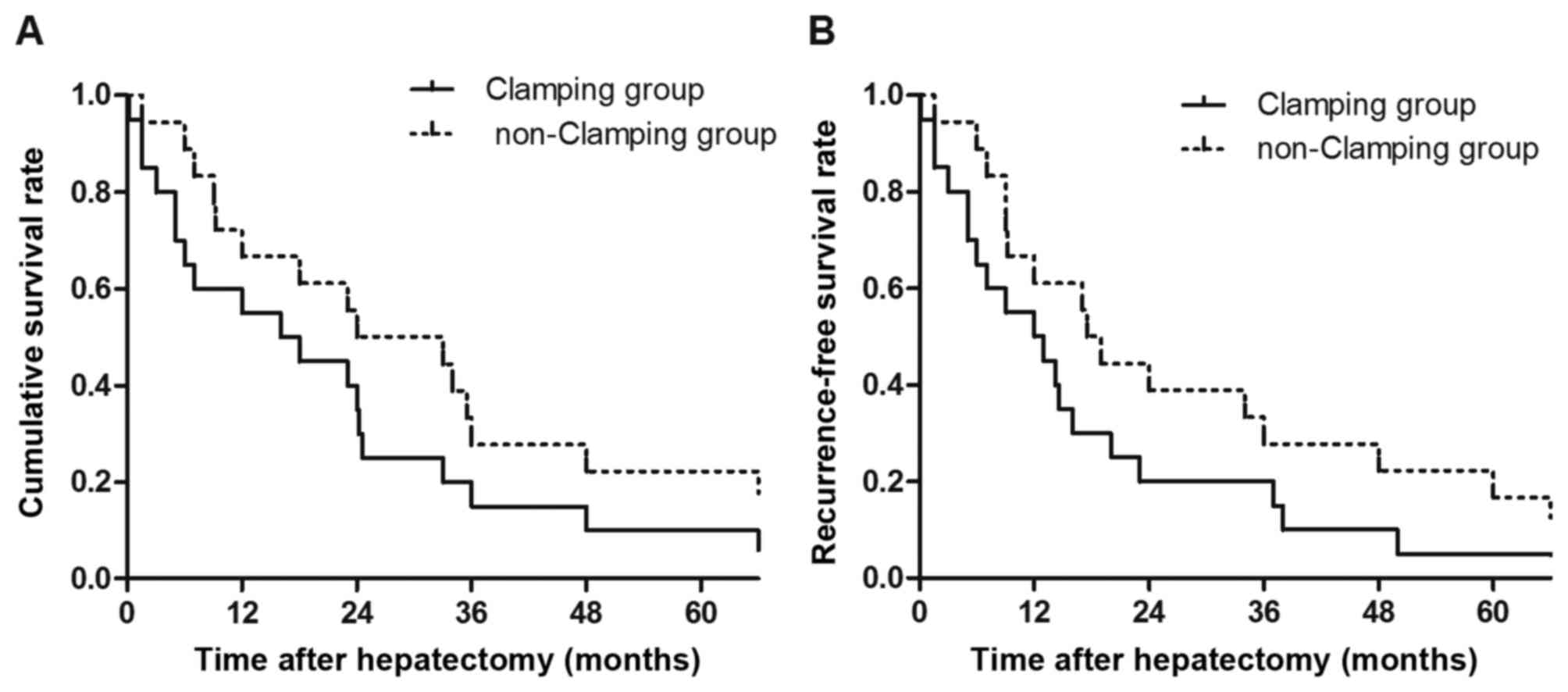
Disease-free survival and overall
survival
Of the 38 patients with SRHCC (97.4%), 37 received
an emergency hepatectomy, these patients did not exhibit
intra-operative peritoneal dissemination. The 1-, 3- and 5-year
survival rates were 67.6 (25/37), 24.3 (9/37) and 16.2% (6/37),
respectively. In addition, 2.6% (1/38) of the patients with SRHCC
received a two-stage liver resection and exhibited no
intra-operative peritoneal dissemination. However, these patients
succumbed to peritoneal dissemination of liver cancer 9 months
later (Fig. 4A).
In the clamping group, the survival time ranged from
4 days to 309 months (median, 17.0 months) and the mean
disease-free survival time was 12.5 months. The 1-, 3- and 5-year
survival rates were 65.5 (13/20), 25.0 (5/20) and 15.0% (3/20),
respectively. In the non-clamping group, the median survival time
was 28.5 months (range, 1.5–294 months) and the mean disease-free
survival time was 18.25 months. The 1-, 3- and 5-year survival
rates were 6.7 (12/18), 22.2 (4/18) and 16.7% (3/18), respectively.
There were no significant differences in disease-free or overall
survival rates between the two groups (P>0.05; Fig. 4B).
Discussion
Surgical therapy of SRHCC remains contentious and
certain clinicians recommend non-surgical therapy including TAE and
TACE. The hemostasis rate of TAE was as high as 97% (32/33) and the
therapeutic efficacy of TAE suggests that it may be an emergent
strategy for hemostasis. However, patients receiving TAE have a
median survival time of 9 weeks (8).
TACE has been demonstrated to effectively inhibit the growth of HCC
cells and decrease tumor size; the hemostasis rate was as high as
100% in the short term (24/24) and patients receiving TACE may
survive for longer than 110 days (9).
Although TAE and TACE are minimally invasive and exhibit a high
hemostasis rate, the survival time of patients receiving TAE or
TACE was decreased when compared with patients receiving
hepatectomy. The presence of SRHCC does not reflect that the cancer
is in an advanced stage and HCC not progressing into the advanced
stage is associated with the risk of spontaneous rupture (5). Additionally, since a number of clinical
studies have suggested that hepatectomy for SRHCC may prolong the
survival time, certain clinicians preferentially perform a
hepatectomy to treat patients with SRHCC (10–14).
When to surgically intervene in SRHCC treatment
remains controversial and it remains unclear whether emergency
hepatectomy has an improved outcome compared with TAE followed by
two-stage hepatectomy. Clinicians who support TAE followed by
hepatectomy propose that TAE is effective for hemostasis in the
acute stage of SRHCC and may subsequently allow more time for
evaluation of HCC, and improvement of hepatic functional
reservation before two-stage hepatectomy (15,16). A
previous study revealed that patients receiving TAE for hemostasis
and subsequent two-stage hepatectomy exhibited 1-, 3- and 5-year
survival rates of 88.5, 64.4 and 55.2%, respectively (17). Clinicians supporting emergency
hepatectomy suggested that SRHCC may cause abdominal dissemination
of HCC cells due to bleeding (18).
SRHCC has been revealed to cause abdominal metastasis (19–21) and
multiple metastatic foci have been observed 3 months after SRHCC
(22). However, intra-operative
peritoneal lavage may effectively prevent abdominal metastasis of
HCC, delay the recurrence of HCC following surgery and improve the
survival rate (23). In addition, the
progression of HCC may cause metastasis due to a long interval
between TAE and hepatectomy, and the untreated hemoperitoneum may
increase the risk of ankylenteron and sepsis. It has been reported
that 10% of patients with SRHCC receiving two-stage hepatectomy
developed intra-operative abdominal dissemination and 33.3%
developed recurrence during the postoperative follow-up. However,
no abdominal dissemination was observed in patients with SRHCC
receiving emergency hepatectomy and 20% of these patients exhibited
recurrence during the postoperative follow-up. Investigating
clinicians therefore recommended that hepatectomy and peritoneal
lavage be performed as early as possible to decrease the incidence
of abdominal dissemination (24). In
the present study, 97.4% of patients received emergency
hepatectomy, intra-operative peritoneal lavage and negative
surgical margins confirmed by intra-operative pathological
examination. Intra-operative peritoneal dissemination was not
noted, and the 1-, 3- and 5-year survival rates were 67.6 (25/37),
24.3 (9/37) and 16.2 % (6/37), respectively. The survival rates in
these patients were consistent with those of previous studies
(1,23). Emergency hepatectomy may achieve
definite hemostasis, treat HCC and decrease abdominal
dissemination. Emergency hepatectomy, subsequent peritoneal lavage
and negative surgical margins, confirmed by intra-operative
pathological examination, may therefore be effective therapeutic
strategies for SRHCC and for decreasing abdominal
dissemination.
During hepatectomy, hepatic portal triad clamping is
usually used to completely or partially block blood supply to the
liver at room temperature, aiming to decrease blood loss during
surgery and increase safety (25).
However, hepatic portal triad clamping has been revealed to cause
liver ischemia/reperfusion injury which may induce postoperative
liver failure or even mortality (26). In certain patients, HCC is derived
from chronic hepatic fibrosis and hepatic cirrhosis (27). In the present study, 73.7% (28/38) of
patients with SRHCC had concomitant hepatic cirrhosis. However, the
cirrhotic liver is susceptible to transient ischemia and patients
with SRHCC and hepatic cirrhosis exhibited bleeding and ischemic
injury before hepatectomy. The use of hepatic portal triad clamping
for hepatectomy therefore comes with a risk of severe complications
including liver failure and infection. Additionally, postoperative
recovery is often unstable and patients are at risk of mortality
after surgery. Attenuating postoperative liver injury and liver
failure in patients with SRHCC and hepatic cirrhosis is of pivotal
clinical importance. Although there is evidence demonstrating that
hepatectomy without portal triad clamping may attenuate
postoperative liver injury and decrease the incidence of liver
failure (28), to the best of our
knowledge, there are no clinical trial data in patients with SRHCC
to confirm this. Patients with SRHCC usually have a poor prognosis
and those who decline surgery often succumbed within 1 month
(29). Hepatectomy in patients with
SRHCC may significantly prolong survival time. A study evaluating
60 patients with SRHCC who received hepatectomy revealed that the
1-, 3- and 5-year survival rates were 54.2, 35.0 and 21.1%,
respectively. These data indicated that the prognosis of these
patients was comparable with that of patients with HCC without
SRHCC (72.1, 47.3 and 33.3%, respectively) (1). However, this therapy possesses risks of
postoperative liver failure and mortality following surgery.
Attenuation of liver failure and decrease postoperative mortality
has been a challenge in patients with SRHCC receiving hepatectomy,
with portal triad clamping having been used to attenuate liver
injury in patients with HCC. Clinical trials exploring the use of
hepatectomy without portal triad clamping have not been reported in
patients with HCC with SRHCC, a life-threatening complication of
HCC.
The aim of the present study was to decrease liver
injury and postoperative mortality in 18 patients with SRHCC by
treating them with hepatectomy without portal triad clamping. The
results of the present study demonstrate that the incidence of
acute liver failure and postoperative recovery of liver function in
the non-clamping group was superior to that in the clamping group,
although there was no marked difference in survival time. Portal
triad clamping aggravates liver injury and increases the incidence
of acute liver failure. Hepatectomy without portal triad clamping
attenuates liver injury and decreases the incidence of acute liver
failure. The results of the present study suggest that hepatectomy
without portal triad clamping is the preferred strategy to treat
patients with SRHCC.
In summary, hepatectomy without portal triad
clamping attenuated liver injury and decreased the incidence of
acute liver failure in patients with SRHCC with hepatic cirrhosis;
intra-operative peritoneal lavage and negative surgical margins
confirmed by intra-operative pathological examination may increase
the survival rate of patients with SRHCC.
Acknowledgements
The present study was supported by the Key
Development Program of Hunan Province of China (grant no.
2015JC3003, to FQ).
Glossary
Abbreviations
Abbreviations:
|
SRHCC
|
spontaneous rupture of hepatocellular
carcinoma
|
|
HCC
|
hepatocellular carcinoma
|
|
ALT
|
alanine aminotransferase
|
|
AST
|
aspartate aminotransferase
|
|
TBil
|
total bilirubin
|
|
Hb
|
hemoglobin
|
|
PT
|
prothrombin time
|
|
KPTT
|
kaolin partial thromboplastin time
|
|
AFP
|
α-fetoprotein
|
|
PLT
|
platelets
|
|
FBI
|
fibrinogen
|
|
TAE
|
transcatheter arterial
embolization
|
|
TACE
|
transcatheter arterial
chemoembolization
|
References
|
1
|
Yeh CN, Lee WC, Jeng LB, Chen MF and Yu
MC: Spontaneous tumour rupture and prognosis in patients with
hepatocellular carcinoma. Br J Surg. 89:1125–1129. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kim PT, Su JC, Buczkowski AK, Schaeffer
DF, Chung SW, Scudamore CH and Ho SG: Computed tomography and
angiographic interventional features of ruptured hepatocellular
carcinoma: Pictorial essay. Can Assoc Radiol J. 57:159–168.
2006.PubMed/NCBI
|
|
3
|
Lee WM, Stravitz RT and Larson AM:
Introduction to the revised American association for the study of
liver diseases position paper on acute liver failure, 2011.
Hepatology. 55:965–967. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lü XS, Zheng YS and Fan QQ: Liver
resection for spontaneous rupture of primary hepatocellular
carcinoma. The Chinese-German Journal of Clinical Oncology.
2:23–24. 2003. View Article : Google Scholar
|
|
5
|
Battula N, Madanur M, Priest O, Srinivasan
P, O'Grady J, Heneghan MA, Bowles M, Muiesan P, Heaton N and Rela
M: Spontaneous rupture of hepatocellular carcinoma: A western
experience. Am J Surg. 197:164–167. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bulger EM, May S, Kerby JD, Emerson S,
Stiell IG, Schreiber MA, Brasel KJ, Tisherman SA, Coimbra R, Rizoli
S, et al: Out-of-hospital hypertonic resuscitation after traumatic
hypovolemic shock: A randomized, placebo controlled trial. Ann
Surg. 253:431–441. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang J, Ye L, Zhang J, Lin M, He S, Mao
X, Zhou X and Zhi F: MELD scores and Child-Pugh classifications
predict the outcomes of ERCP in cirrhotic patients with
choledocholithiasis: A retrospective cohort study. Medicine
(Baltimore). 94:e4332015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ngan H, Tso WK, Lai CL and Fan ST: The
role of hepatic arterial embolization in the treatment of
spontaneous rupture of hepatocellular carcinoma. Clin Radiol.
53:338–341. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim JY, Lee JS, Oh DH, Yim YH and Lee HK:
Transcatheter arterial chemoembolization confers survival benefit
in patients with a spontaneously ruptured hepatocellular carcinoma.
Eur J Gastroenterol Hepatol. 24:640–645. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hsueh KC, Fan HL, Chen TW, Chan DC, Yu JC,
Tsou SS, Chang TM and Hsieh CB: Management of spontaneously
ruptured hepatocellular carcinoma and hemoperitoneum manifested as
acute abdomen in the emergency room. World J Surg. 36:2670–2676.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Andersson R, Tranberg KG and Bengmark S:
Hemoperitoneum after spontaneous rupture of liver tumor: Results of
surgical treatment. HPB Surg. 1:81–83. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shirabe K, Kitamura M, Tsutsui S, Maeda T,
Matsumata T and Sugimachi K: A long-term survivor of ruptured
hepatocellular carcinoma after hepatic resection. J Gastroenterol
Hepatol. 10:351–354. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen ZY, Qi QH and Dong ZL: Etiology and
management of hemorrhage in spontaneous liver rupture: A report of
70 cases. World J Gastroenterol. 8:1063–1066. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Marini P, Vilgrain V and Belghiti J:
Management of spontaneous rupture of liver tumours. Dig Surg.
19:109–113. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Leung CS, Tang CN, Fung KH and Li MK: A
retrospective review of transcatheter hepatic arterial embolisation
for ruptured hepatocellular carcinoma. J R Coll Surg Edinb.
47:685–688. 2002.PubMed/NCBI
|
|
16
|
Tanaka A, Takeda R, Mukaihara S, Hayakawa
K, Shibata T, Itoh K, Nishida N, Nakao K, Fukuda Y, Chiba T and
Yamaoka Y: Treatment of ruptured hepatocellular carcinoma. Int J
Clin Oncol. 6:291–295. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee HS, Choi GH, Kang DR, Han KH, Ahn SH,
Kim DY, Park JY, Kim SU and Choi JS: Impact of spontaneous
hepatocellular carcinoma rupture on recurrence pattern and
long-term surgical outcomes after partial hepatectomy. World J
Surg. 38:2070–2078. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sonoda T, Kanematsu T, Takenaka K and
Sugimachi K: Ruptured hepatocellular carcinoma evokes risk of
implanted metastases. J Surg Oncol. 41:183–186. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Okano J, Shiota G, Horie Y, Mitsuda A,
Suou T, Kawasaki H and Oofuji S: Rupture of metastatic nodule on
the peritoneal surface secondary to hepatocellular carcinoma.
Intern Med. 35:783–784. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yunoki Y, Takeuchi H, Makino Y, Murakami
I, Yasui Y, Tanakaya K, Kawaguchi K and Konaga E: Intraperitoneal
seeding of ruptured hepatocellular carcinoma: Case report. Abdom
Imaging. 24:398–400. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Eriguchi N, Aoyagi S, Okuda K, Tamae T,
Fukuda S, Kanazawa N, Hamada S, Kawabata M, Nishimura K and Kodama
T: Successful surgical treatment for implanted intraperitoneal
metastases of hepatocellular carcinoma. J Hepatobiliary Pancreat
Surg. 7:520–523. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lin CC, Chen CH, Tsang YM, Jan IS and Sheu
JC: Diffuse intraperitoneal metastasis after spontaneous rupture of
hepatocellular carcinoma. J Formos Med Assoc. 105:577–582. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chang YM, Hsu KF, Yu JC, Chan DC, Chen CJ,
Chen TW, Hsieh CB and Hsieh HF: Distilled water peritoneal lavage
in patients with rupture hepatocellular carcinoma.
Hepatogastroenterology. 60:140–143. 2013.PubMed/NCBI
|
|
24
|
Yang T, Sun YF, Zhang J, Lau WY, Lai EC,
Lu JH, Shen F and Wu MC: Partial hepatectomy for ruptured
hepatocellular carcinoma. Br J Surg. 100:1071–1079. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Qian NS, Liao YH, Cai SW, Raut V and Dong
JH: Comprehensive application of modern technologies in precise
liver resection. Hepatobiliary Pancreat Dis Int. 12:244–250. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tashiro H, Kuroda S, Mikuriya Y and Ohdan
H: Ischemia-reperfusion injury in patients with fatty liver and the
clinical impact of steatotic liver on hepatic surgery. Surg Today.
44:1611–1625. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ramakrishna G, Rastogi A, Trehanpati N,
Sen B, Khosla R and Sarin SK: From cirrhosis to hepatocellular
carcinoma: New molecular insights on inflammation and cellular
senescence. Liver Cancer. 2:367–383. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wrightson WR, Edwards MJ and McMasters KM:
The role of the ultrasonically activated shears and vascular
cutting stapler in hepatic resection. Am Surg. 66:1037–1040.
2000.PubMed/NCBI
|
|
29
|
Zhu Q, Li J, Yan JJ, Huang L, Wu MC and
Yan YQ: Predictors and clinical outcomes for spontaneous rupture of
hepatocellular carcinoma. World J Gastroenterol. 18:7302–7307.
2012. View Article : Google Scholar : PubMed/NCBI
|