Introduction
Cervical cancer is the fourth most frequent cancer
in women globally with ~530,000 new cases in 2012, accounting for
7.5% of all female cancer-associated mortalities (1). A major cause of cervical cancer is
persistent infection with high-risk human papillomavirus (HR-HPV)
(1). HPV subtypes 16 and 18 cause
~70% of all cases of HPV (1,2). At present, >170 HPV types have been
identified (3). Infection with 15
subtypes of HPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59,
68, 73 and 82) may lead to cancer, which is why these 15 types are
known as carcinogenic or high-risk types (4). The genome of human papillomaviruses
consists of ~8,000 base pairs and contains six early genes (E6, E7,
E1, E2, E4 and E5) and two late genes (L1 and L2) (5). Upon replication of the viral gene E6, E6
oncoprotein is expressed, which alters the cell cycle (6). E6 oncoprotein and E6-associated protein
(E6-AP) form a complex that binds to p53 and causes its proteolytic
degradation (7).
The tumour suppressor protein p53 (p53) signalling
pathways leads to cell cycle arrest or apoptosis in case of DNA
damage (8). As E6 oncoprotein induces
the degradation of p53, the function of this important cell cycle
protein is disturbed following HPV infection (9). In addition, the cell cycle regulation
protein p16 is expressed at high levels in HPV-infected epithelial
cells, and thus acts as a marker for the diagnosis of
HPV-associated carcinoma (9,10). In non-carcinoma tissues p53 is
regulated by MDM2 proto-oncogene (MDM2) through a negative feedback
mechanism. MDM2 promotes the ubiquitination and
proteasome-dependent degradation of p53 (11). There is also an association between
MDM2, p53 polymorphism and the progression of cervical carcinoma
(12).
A protein previously demonstrated to be associated
with cervical cancer is galectin-3 (gal-3) (5). Galectins are defined as lectins with a
galactose-binding ability and a characteristic amino-acid sequence
(13). Galectin is a name proposed by
Hirabayashi and Kasai (14) for a
family of animal lectins. Galectins are typically soluble and
metal-independent in their activity (15). They have similar features to
cytoplasmic proteins, including no disulfide bridges, no sugar
chains, no signal sequences and, in most cases, their N-terminal
amino acids are acetylated (16). It
is possible to classify galectins into the following three types on
the basis of their structural architecture: Proto, chimera and
tandem-repeat types. Gal-3 is a chimera-type galectin (17).
Gal-3 may increase the invasiveness of cervical
cancer by activating vascular endothelial growth factor receptor-3
(5). Therefore, the aim of the
present study was to systematically analyse the expression and
interactions of E6, p53, p16, MDM2 and gal-3 in cervical cancer
specimens.
Materials and methods
Ethical approval
The present study was approved by the local Ethics
Committee of the Ludwig-Maximilians-University of Munich (approval
no. 259-16; Munich, Germany), and was performed in compliance with
the guidelines of the Helsinki Declaration. Patient data were fully
anonymised.
Specimens
Archived formalin-fixed paraffin-embedded (FFPE)
sections from 250 cases of cervical cancer were used in the present
study; it was possible to analyse 248 cases as there was no tumour
tissue present on two sections (Table
I). Cervical dysplasia [cervical intra-epithelial neoplasia
(CIN) stage III] (18) and
non-dysplastic cervical tissue (3 sections of each) was used for
the E6 immunohistochemical staining, and breast cancer tissue was
used for the mutated p53 immunohistochemistry. Specimens were
obtained from the Department of Obstetrics and Gynecology of
Ludwig-Maximilians-University of Munich, and were obtained from
patients undergoing surgery there between 1993 and 2002. Follow-up
data were received from the Munich Cancer Registry (Munich Tumour
Centre, Munich, Germany).
 | Table I.Clinical parameters of the patients
included in the present study. |
Table I.
Clinical parameters of the patients
included in the present study.
| Clinical
parameter | No./total no. | % |
|---|
| Age (years) |
|
|
|
≤50 | 143/248 | 58 |
|
>50 | 105/248 | 42 |
| No. of metastasis
positive lymph nodes |
|
|
| 0 | 149/248 | 60 |
|
1–4 | 97/248 | 39 |
| NA | 2/248 | 1 |
| Tumour size
(cm) |
|
|
|
<2 | 111/248 | 45 |
|
2–4 | 128/248 | 52 |
|
>4 | 9/248 | 3 |
| Tumour grade |
|
|
| I | 20/248 | 8 |
| II | 141/248 | 57 |
|
III | 78/248 | 31 |
| NA | 9/248 | 4 |
| Tumour subtype |
|
|
|
Squamous | 199/248 | 80 |
|
Adenocarcinoma | 49/248 | 20 |
| Progression (over
236 months) |
|
|
|
None | 190/248 | 77 |
| ≥1 | 58/248 | 23 |
| Survival (over 236
months) |
|
|
| Right
censured | 210/248 | 85 |
|
Succumbed | 38/248 | 15 |
Immunohistochemistry
The FFPE sections (3-µm-thick) were dewaxed in
xylol, endogenous peroxidase was inhibited with 3%
methanol/H2O2 and sections were rehydrated in
a descending ethanol gradient. To stain for mutated p53, wild-type
p53, E6, gal-3 and MDM2, the slides were pre-treated in citrate
buffer (100°C; pH 6.0) for antigen retrieval. Following this,
non-specific binding of the primary antibodies was blocked, and
incubation with the primary antibodies followed (Tables II and III). Incubation with the secondary
antibodies and the following steps of the detection system and
colour development are illustrated in Tables II and III. For p16 detection, the specimens were
automatically stained using the Ventana BenchMark XT Stainer
(Ventana Medical Systems, Inc., Oro Valley, AZ, USA) and the CINtec
Histology kit (cat. no. 9517; Roche Applied Science, Mannheim,
Germany) according to the manufacturer's instructions, while all
other antibodies were stained for manually. For wild-type p53, the
slides were washed in PBS/0.05% Tween-20. All other slides were
washed in PBS only. Finally, the slides were counterstained with
hemalaun (Waldeck GmbH, Münster, Germany) for 2 min at room
temperature, dehydrated in an ascending series of ethanol and
stored.
| Table II.Procedures for gal-3 and MDM2
staining. |
Table II.
Procedures for gal-3 and MDM2
staining.
| Protocol | Gal-3 | MDM2 |
|---|
| Blocking
method | Horse
seruma, 20 min, RT | Goat
seruma, 20 min, RT |
| Primary antibody,
dilution, incubation duration, incubation temperature, cat.
no. | Anti-galectin-3,
1:1,000 in PBS, 16 h, 4°C; NCL-GAL3b | Anti-MDM2, 1:100 in
PBS, 16 h, 4°C, NCL-MDM2b |
| Secondary antibody,
dilution, incubation duration, incubation temperature, cat.
no. | Biotynilated
anti-mouse IgGa, 30 min,
RT; PK-6100 | Biotinylated goat
anti-mouse IgM, 30 min, RT ZMB2020c |
| Detection of
secondary antibody |
ABC-complexa, 30 min |
ABC-complexa, 30 min |
| Chromogen | 1 mg/ml
DABd, 5 min | 1 mg/ml
DABd, 1 min |
| Table III.Procedures for mutated p53, wild-type
p53 and E6 staining. |
Table III.
Procedures for mutated p53, wild-type
p53 and E6 staining.
| Protocol | Mutated p53 | p53 wild-type | E6 |
|---|
| Blocking
method | Reagent
1a; 5 min, RT | Reagent
1a; 5 min, RT | Reagent
1a; 5 min, RT |
| Primary antibody,
dilution, incubation duration, incubation temperature, cat.
no. | Anti-p53, 1:100 in
PBS, 16 h, 4°C, ab32049b | Anti-p53, 1:200 in
PBS, 16 h, 4°C, ab26b | Anti-E6, 1:150 in
PBS, 1 h, RT, ab70b |
| Post blocking
method | Reagent
2a; 20 min, RT | Reagent
2a; 20 min, RT | Reagent
2a; 20 min, RT |
| Secondary antibody,
dilution, incubation duration, incubation temperature, cat.
no. | HRP-Polymer Reagent
3a, 30 min, RT
POLHRP-100 | HRP-Polymer Reagent
3a, 30 min, RT
POLHRP-100 | HRP-Polymer Reagent
3a; 30 min, RT
POLHRP-100 |
| Chromogen | 1 mg/ml
DABc, 1 min | 1 mg/ml
DABc, 1 min | 1 mg/ml
DABc, 1 min |
Slides were examined with a Zeiss Axiophot light
photomicroscope (Zeiss GmbH, Jena, Germany). Digital images were
obtained with a digital-camera system (CF20DXC; KAPPA Messtechnik,
Gleichen, Germany). All specimens were evaluated by a pathologist.
The intensity and distribution patterns of the staining reaction
was evaluated by two blinded, independent observers, including the
gynecological pathologist, using the semi-quantitative
immunoreactive (IRS)-score, as previously described (19), to asses steroid receptors (20) and cathepsin D (21) expression. The IRS score was calculated
by multiplication of optical staining intensity (graded as 0, no
staining; 1, weak staining; 2, moderate staining; and 3, strong
staining) and the percentage of positive stained cells (0, no
staining; 1, ≤10% of the cells, 2, 11–50% of the cells, 3=51–80% of
the cells and 4, ≥81% of the cells) and without knowing the
pathological evaluation, the diagnosis or the standard performed
hematoxylin reaction for 2 min at room temperature for each
specimen.
Statistical analysis
Data were analysed using SPSS software (version
19.0; IBM SPSS, Armonk, NY, USA) for Microsoft Windows and
visualised using Microsoft Office 7 (Microsoft Corporation,
Redmond, WA, USA). Spearman coefficients were calculated to assess
correlations, while the Mann-Whitney U test was applied to examine
differences between groups. Differences in survival were assessed
using the log-rank test and survival curves were plotted in
accordance with Kaplan-Meier estimator. P<0.05 was considered to
indicate a statistically significant difference and data were
expressed as the mean ± standard error. Cox regression analysis was
used to compare the risk of mortality in patients with and without
gal-3 expression when the effects of further factors were accounted
for. Independent variables included in the Cox regression model
were gal-3 expression, age at the time of surgery, histological
subtype, tumour size, lymph node status (pN), metastasis, tumour
grade, International Federation of Gynecology and Obstetrics (FIGO)
stage (22,23), and E6, mutated p53 and MDM2 expression
status.
Results
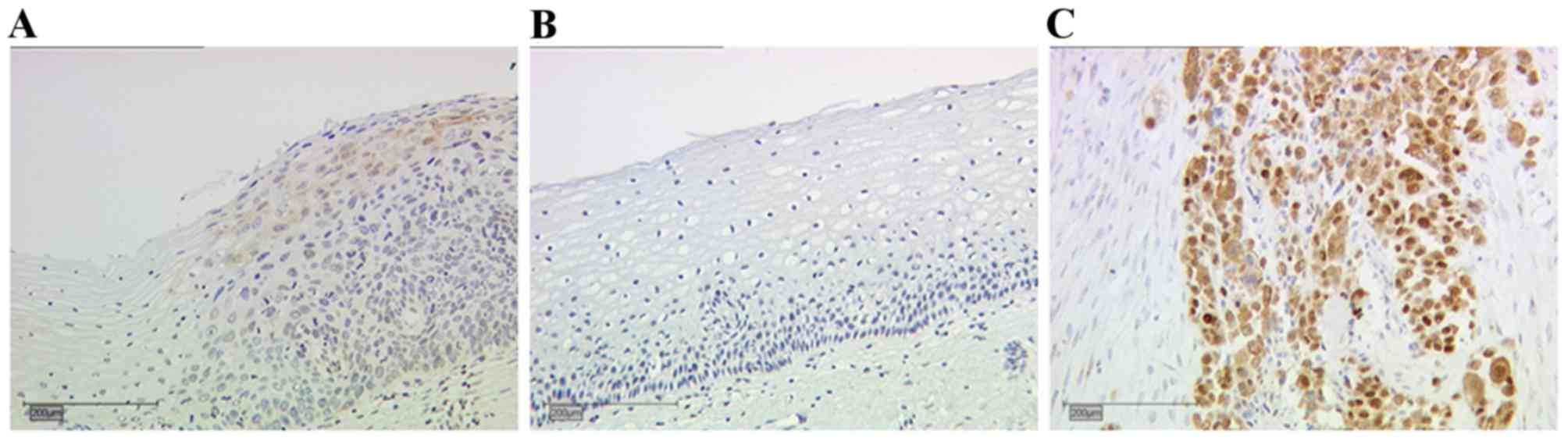
Evaluation of E6 oncoprotein
immunohistochemistry and the detection of mutated p53 on control
slides
CIN III tissue slides were used for the evaluation
of E6 oncoprotein staining. Moderate expression levels of E6 were
observed in the CIN III sections (Fig.
1A). There was no expression of the E6 oncoprotein, and
therefore no staining observed, in the non-dysplastic cervical
tissue (Fig. 1B). Breast cancer
tissue was used to evaluate the staining of mutated p53 (Fig. 1C), which exhibited nuclear and
cytoplasmic staining.
E6 oncoprotein staining
A total of 81% of all cervical cancer tissue
examined expressed E6 oncoprotein (data not shown). Cervical cancer
specimens demonstrated significantly increased staining with a
higher T stage (according to the Tumor-Node-Metastasis
classification system) (24). T1
stage carcinomas (Fig. 2A)
demonstrated E6 staining with a median IRS of 2, while T2 (Fig. 2B) and T3 (Fig. 2C) stage carcinoma tissues had a
significantly higher median E6 expression of IRS 3 (P=0.017;
Fig. 2D).
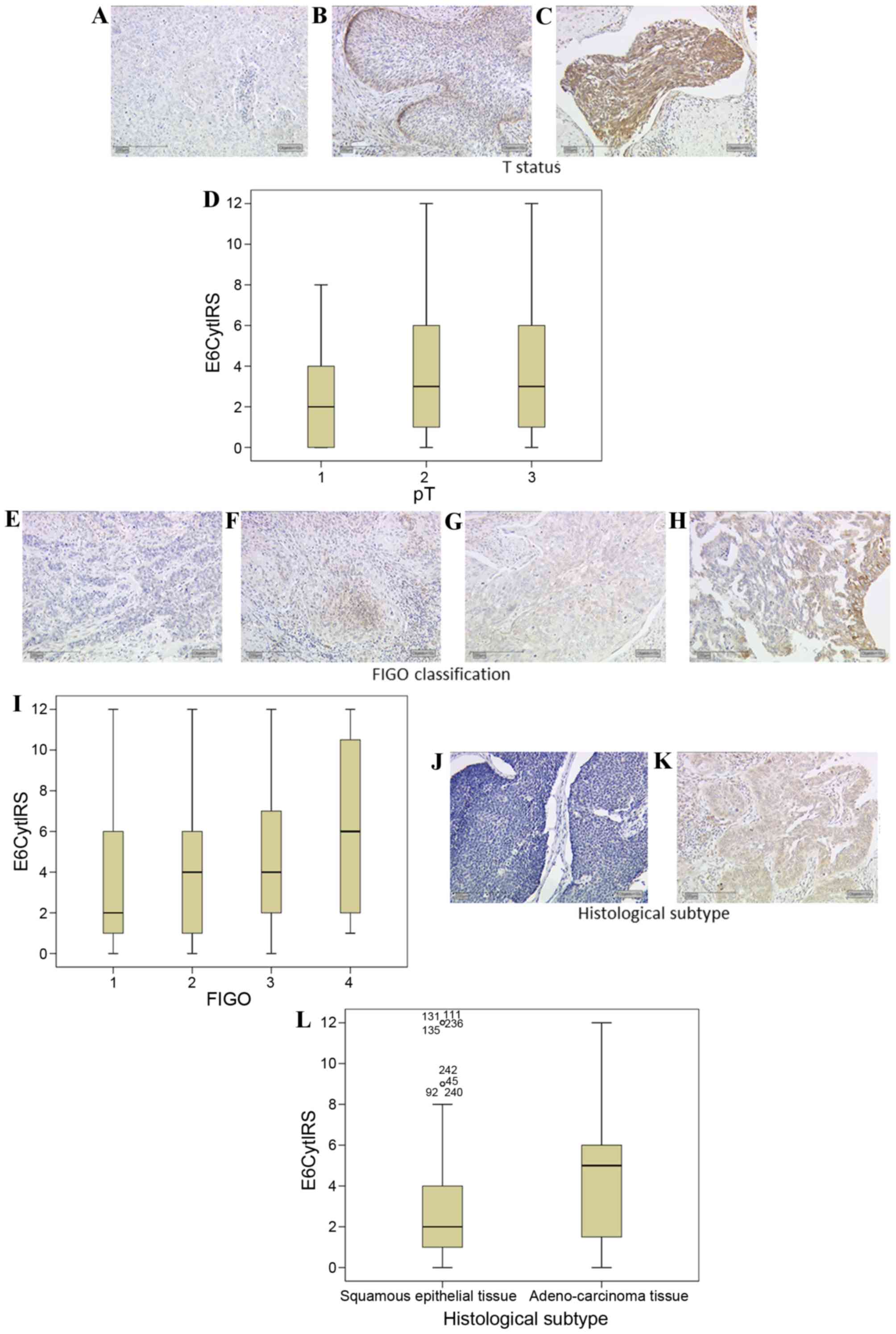 | Figure 2.E6 expression is enhanced with
cervical cancer tumour staging. (A) Low intensity E6 expression was
observed in T1 tumours, whereas (B) T2 and (C) T3 staged tumours
demonstrated increased expression of E6. (D) Box plot summary of
the IRS for each tumour stage (P=0.017, FIGO 1 vs. 3). E6
expression was positively correlated with FIGO classification, with
(E) FIGO 1 classified tissue demonstrating low expression of E6
while (F) FIGO 2 and (G) FIGO 3 classified tissue demonstrated
increased expression levels, and (H) FIGO 4 tissue further
increased expression levels. (I) Box plot summary of the IRS for
each FIGO stage (P<0.001, FIGO 1 vs. 4). (J) Squamous epithelial
tissue demonstrated lower levels of E6 staining than (K)
adenocarcinoma tissue. (L) Box plot summary of the IRS for each
histological subtype. Scale bar, 200 µm. FIGO, International
Federation of Gynecology and Obstetrics; IRS, immunoreactive score;
E6Cyt, E6 cytoplasmic; pT, pathological tumour stage. |
FIGO 1 carcinoma tissues had a median E6 expression
of IRS 2 (Fig. 2E). FIGO 2 (Fig. 2F) and FIGO 3 (Fig. 2G) carcinoma tissues had a median IRS
of 4. FIGO 4-classified cervical cancer tissue had a median E6 IRS
score of 6 (Fig. 2H). E6 demonstrated
a significant positive correlation with the FIGO classification
(R=0.277, P<0.001; Fig. 2I).
E6 demonstrated significantly different expression
levels in cervical cancer tissue dependent on the histological
subtype. Squamous epithelial carcinomas (Fig. 2J) had a median expression of IRS 2.
Adenocarcinoma tissue (Fig. 2K) had
significantly increased staining with a median of IRS 5 (P=0.015
vs. squamous epithelial carcinoma; Fig.
2L).
Wild-type and mutated p53
expression
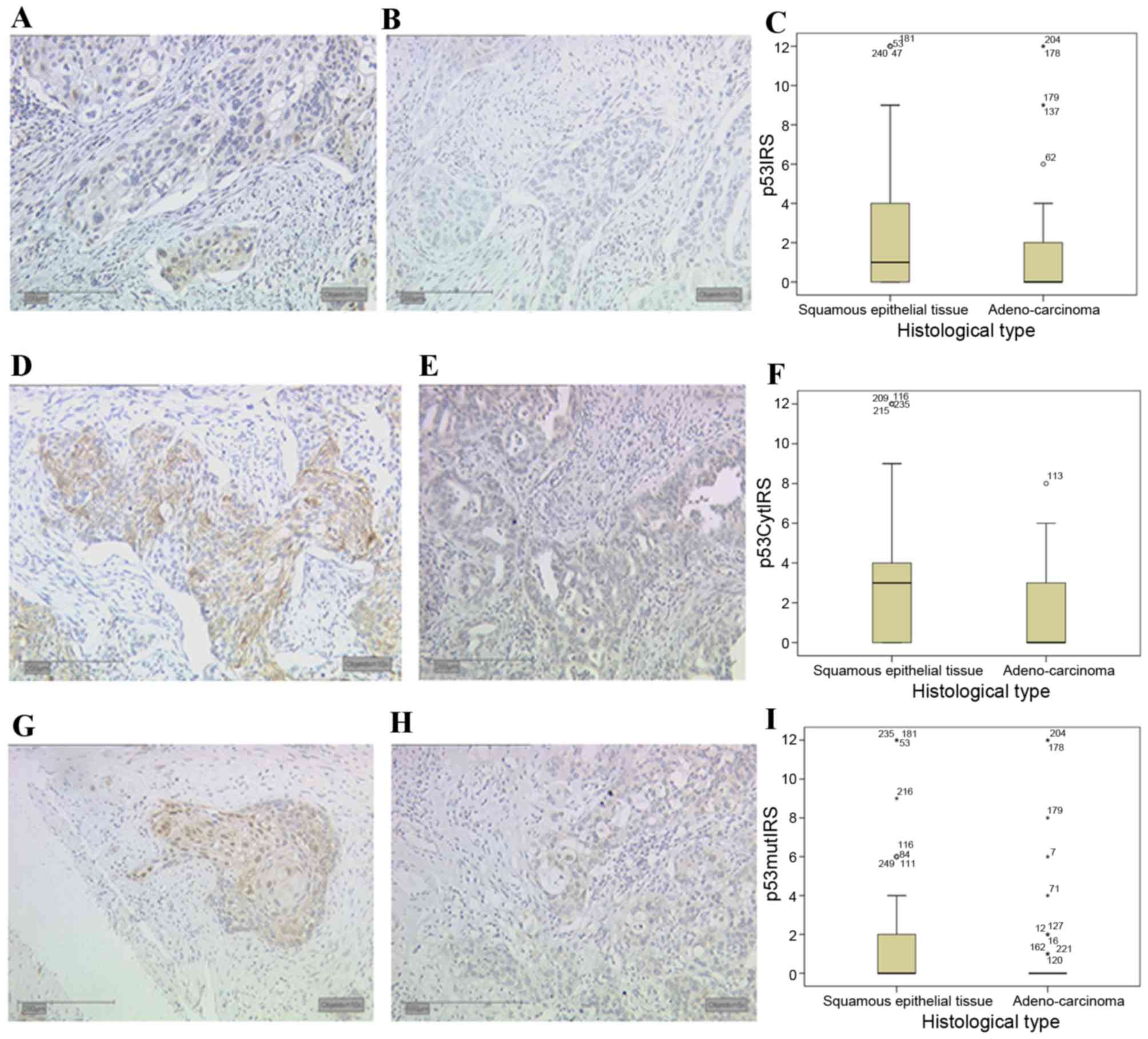
Expression of wild-type p53 was observed in the
nucleus and cytoplasm of 60 and 66% of all cervical cancer
specimens, respectively. Significantly different expression levels
in cervical cancer tissue in different histological subtypes were
also observed for p53 expression. Wild-type p53 demonstrated a
median nuclear expression (Fig. 3A)
of IRS 1 in squamous epithelial tissue, whereas in adenocarcinoma
tissue (Fig. 3B) the median nuclear
expression was significantly decreased in comparison (IRS 0,
P=0.024; Fig. 3C).
In addition to nuclear expression, wild-type
cytosolic p53 expression also demonstrated significant differences
associated with the histological subtype. In squamous epithelial
tissue (Fig. 3D) a median expression
of IRS 3 was observed, whereas in comparison the median cytosolic
expression of p53 was significantly decreased in adenocarcinoma
tissue (Fig. 3E) to IRS 0
(P<0.001; Fig. 3F).
The monoclonal antibody that recognises a previously
described mutated form of p53, (25)
also revealed significant staining differences associated with the
histological subtype of cervical cancer. In addition, 42% of all
cervical cancer tissue slides demonstrated nuclear expression of
mutated p53, and 67% of all cases demonstrated mutated p53
expression in the cytoplasm. Although the median expression of
mutated p53 in squamous epithelial tissue (Fig. 3G) and adenocarcinoma tissue (Fig. 3H) was 0, differences between the
subtypes were significant (P=0.011; Fig.
3I).
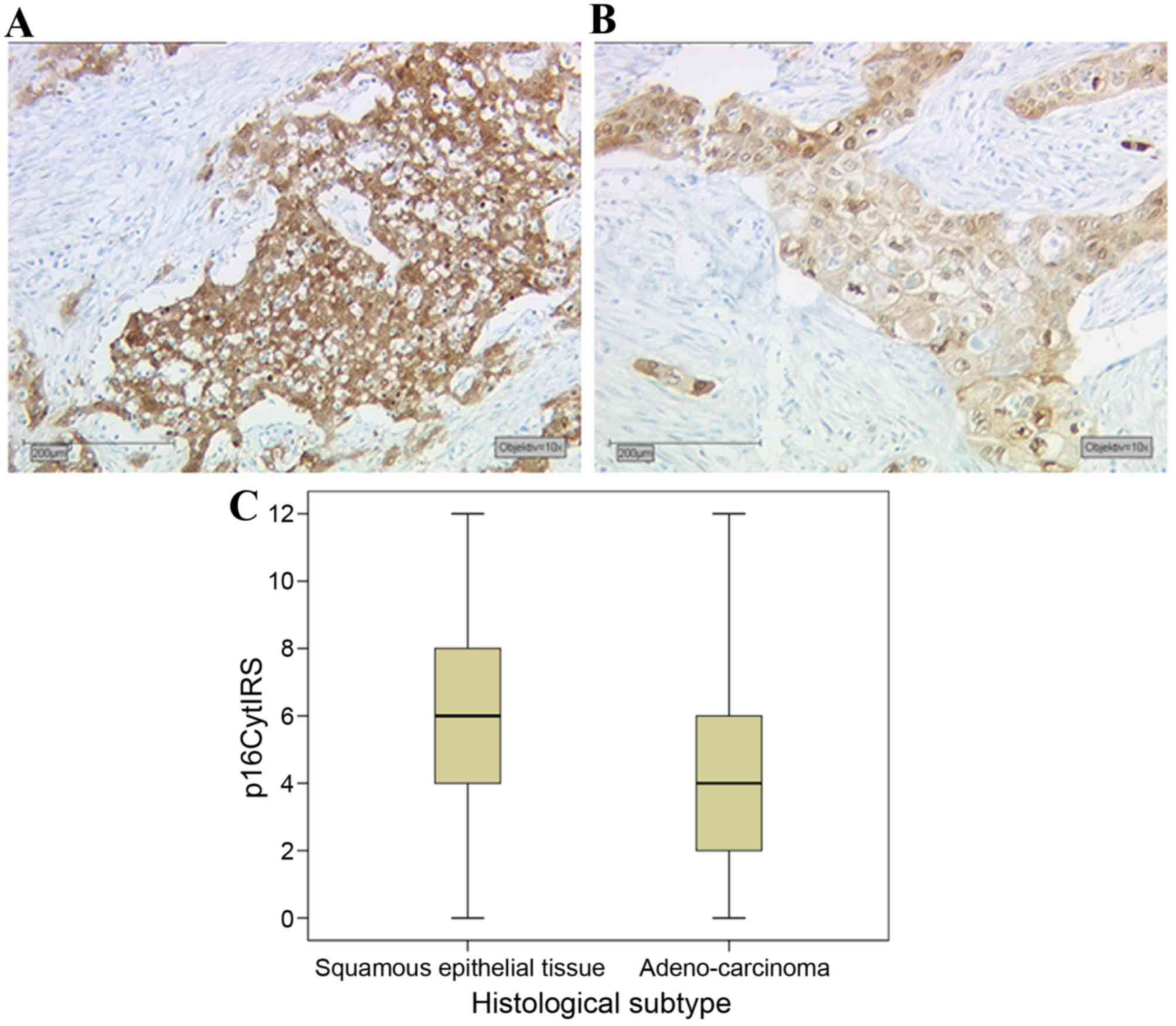
Expression of p16 oncoprotein in
cervical cancer tissue
p16 overexpression is routinely used in the
Pathology Department of the Ludwig-Maximilians-University of Munich
as a marker for HPV-associated head and neck squamous carcinoma
(11). A total of 94% of cervical
carcinoma cases tested demonstrated p16 expression, and 61% of
these cases were p16-overexpressing according to pathological
evaluation. The cell cycle protein p16 demonstrated significant
differences in expression between different histological subtypes
of cervical cancer. Squamous epithelial tissue (Fig. 4A) had a median expression of IRS 6,
while adenocarcinoma tissue (Fig. 4B)
had a significantly lower expression in comparison, with an IRS of
4 (P<0.001; Fig. 4C). Notably, p16
demonstrated no significant correlation with E6 oncoprotein
expression (data not shown).
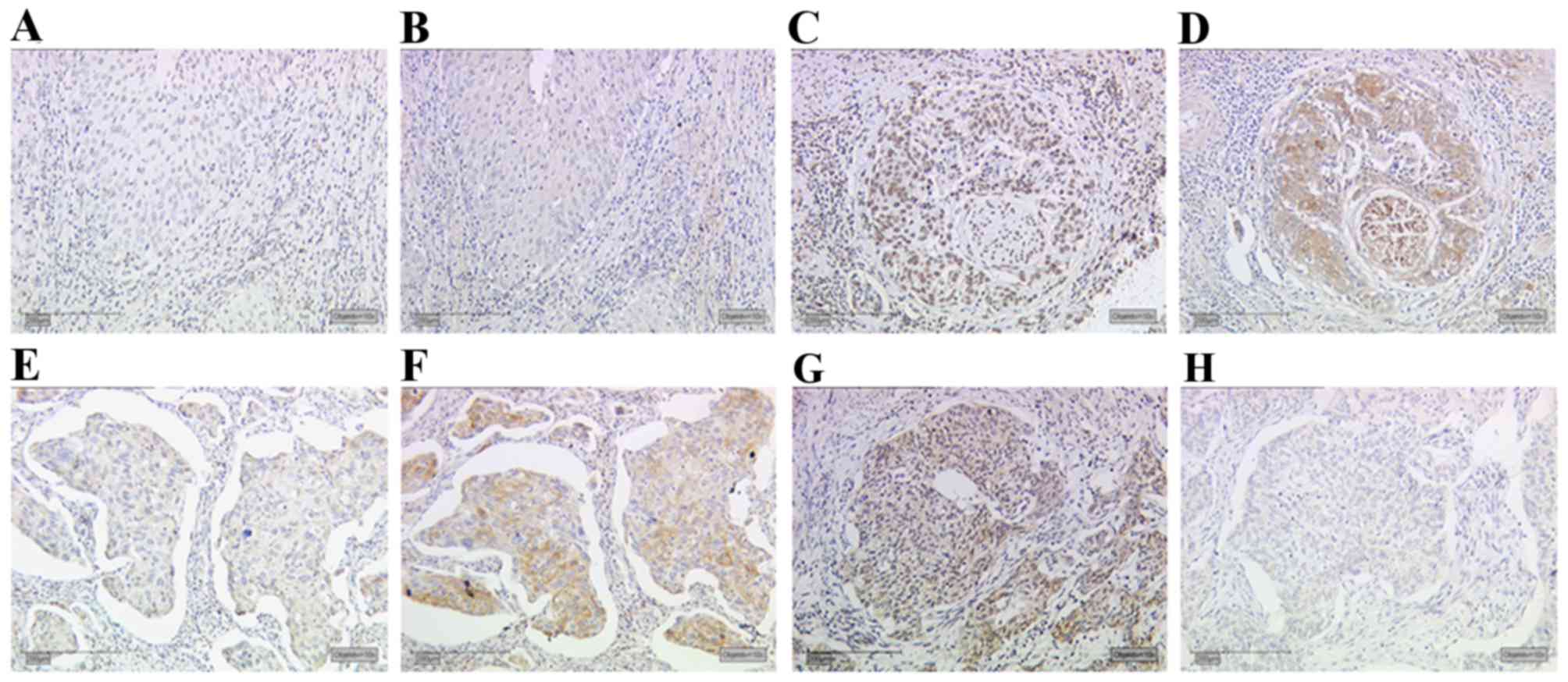
Correlation analysis
A significant correlation was identified between
MDM2 and gal-3 expression in cervical cancer tissue (R=0.181,
P=0.005; data not shown). Cases of cervical cancer with low MDM2
expression (Fig. 5A) also
demonstrated low gal-3 expression (Fig.
5B). Likewise, a case with high MDM2 expression (Fig. 5C) demonstrated high gal-3 expression
(Fig. 5D). Cases of cervical cancer
with low E6 oncoprotein expression (Fig.
5E) demonstrated enhanced staining of the mutated form of p53
in the same area of the tumour (Fig.
5F). However, cases with high expression of E6 (Fig. 5G) revealed low expression of mutated
p53 (Fig. 5H). The statistical
evaluation confirmed these results of serial section staining
(R=−0.140, P=0.028; Table IV). A
significant correlation was also identified between the expression
of MDM2 and mutated p53 in cervical cancer tissue (R=0.144,
P=0.025; Table IV). The correlation
analyses and clinical parameters are summarised in Table IV.
| Table IV.Correlation analyses of clinical
parameters and immunohistochemical staining parameters. |
Table IV.
Correlation analyses of clinical
parameters and immunohistochemical staining parameters.
| Clinical
parameter | Statistic | Age | Histology | pT | pN | pM | Grade | FIGO | E6 | p53-mutated | MDM2 | Galectin-3 |
|---|
| Age (years) | Correlation
coefficient | −.019 | .004 | −.115 | −.065 | −.140* | .354b | .133a | .169b | .107 | .026 | .050 |
|
| Sig.
(2-tailed) | .766 | .945 | .070 | .307 | .028 | .000 | .037 | .008 | .095 | .686 | .438 |
|
| N | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 | 246 | 241 | 240 |
| Histology | Correlation
coefficient | .028 | 1.000 | .000 | −.073 | −.108 | −.084 | .045 | .156a | −.162a | .075 | .029 |
|
| Sig.
(2-tailed) | .664 | . | .994 | .249 | .089 | .185 | .477 | .015 | .010 | .242 | .652 |
|
| N | 245 | 249 | 249 | 249 | 249 | 249 | 249 | 245 | 249 | 244 | 243 |
| pT | Correlation
coefficient | .276b | .000 | 1.000 | .359b | −.202b | .182b | .380b | .174b | .055 | −.019 | −.039 |
|
| Sig.
(2-tailed) | .000 | .994 | . | .000 | .001 | .004 | .000 | .006 | .384 | .762 | .540 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| pN | Correlation
coefficient | .037 | −.073 | .359b | 1.000 | −.172b | .212b | .240b | .033 | −.050 | −.058 | −.033 |
|
| Sig.
(2-tailed) | .559 | .249 | .000 | . | .007 | .001 | .000 | .610 | .435 | .370 | .608 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| pM | Correlation
coefficient | −.081 | −.108 | −.202b | −.172b | 1.000 | −.146* | −.150a | −.037 | .004 | .032 | −.074 |
|
| Sig.
(2-tailed) | .206 | .089 | .001 | .007 | . | .021 | .018 | .560 | .951 | .619 | .252 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| Grade | Correlation
coefficient | −.081 | −.084 | .182b | .212b | −.146a | 1.000 | .093 | .084 | −.065 | −.175b | −.047 |
|
| Sig.
(2-tailed) | .203 | .185 | .004 | .001 | .021 | . | .142 | .191 | .302 | .006 | .461 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| FIGO | Correlation
coefficient | .076 | .045 | .380b | .240b | −.150a | .093 | 1.000 | .227b | −.099 | .021 | .067 |
|
| Sig.
(2-tailed) | .233 | .477 | .000 | .000 | .018 | .142 | . | .000 | .120 | .748 | .296 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| E6 | Correlation
coefficient | .088 | .156a | .174b | .033 | −.037 | .084 | .227b | 1.000 | .093 | .001 | .009 |
|
| Sig.
(2-tailed) | .173 | .015 | .006 | .610 | .560 | .191 | .000 | . | .147 | .986 | .893 |
|
| N | 242 | 245 | 246 | 246 | 246 | 246 | 246 | 246 | 246 | 244 | 243 |
| p53-mutated | Correlation
coefficient | .092 | −.290b | .016 | −.019 | .004 | −.115 | −.065 | −.140a | 1.000 | .133a | .169b |
|
| Sig.
(2-tailed) | .148 | .000 | .796 | .766 | .945 | .070 | .307 | .028 | . | .037 | .008 |
|
| N | 246 | 249 | 250 | 250 | 250 | 250 | 250 | 246 | 250 | 245 | 244 |
| MDM2 | Correlation
coefficient | .026 | .075 | −.019 | −.058 | .032 | −.175b | .021 | .001 | −.042 | 1.000 | .181b |
|
| Sig.
(2-tailed) | .686 | .242 | .762 | .370 | .619 | .006 | .748 | .986 | .511 | . | .005 |
|
| N | 241 | 244 | 245 | 245 | 245 | 245 | 245 | 244 | 245 | 245 | 243 |
| Galectin-3 | Correlation
coefficient | .050 | .029 | −.039 | −.033 | −.074 | −.047 | .067 | .009 | −.020 | .181b | 1.000 |
|
| Sig.
(2-tailed) | .438 | .652 | .540 | .608 | .252 | .461 | .296 | .893 | .760 | .005 | . |
|
| N | 240 | 243 | 244 | 244 | 244 | 244 | 244 | 243 | 244 | 243 | 244 |
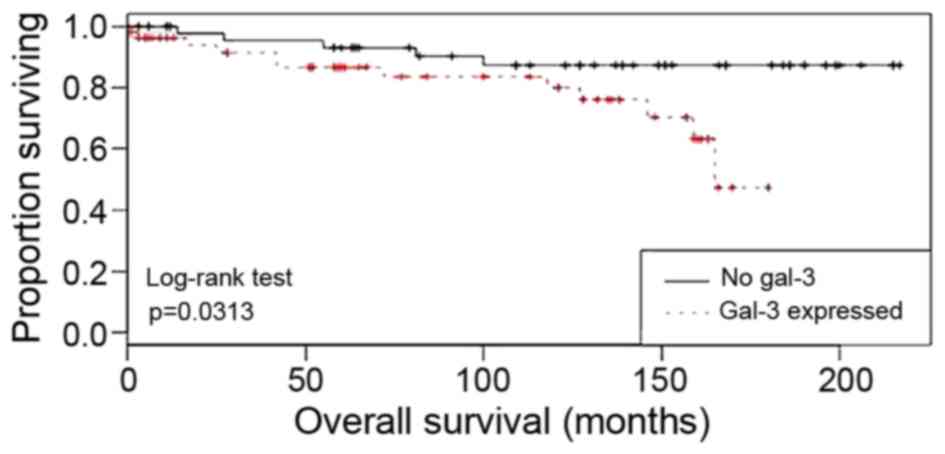
Gal-3 is a negative prognosticator in
p16-negative patients with cervical cancer
In patients with cervical cancer with no or very low
p16 expression, gal-3 expression was correlated with a poor
prognosis in overall survival analyses (P=0.0313; Fig. 6). Multivariate Cox regression analysis
was performed to test which histopathological variables were
independent prognosticators for survival rate in the tested breast
cancer collective. It was demonstrated that the histological
subtype (P=0.02), tumour size (P=0.011) and pN (P=0.045) were
independent prognosticators for overall survival (Table V). No significant effect was
demonstrated for the other histopathological variables.
| Table V.Cox regression of overall survival on
cervical cancer variables. |
Table V.
Cox regression of overall survival on
cervical cancer variables.
|
|
|
| 95.0% CI |
|---|
|
|
|
|
|
|---|
| Parameters | P-value | Hazard ratio | Lower | Upper |
|---|
| Age (years) | 0.071 | 1.029 | 0.997 | 1.062 |
| Histology | 0.002 | 3.576 | 1.586 | 8.063 |
| pT | 0.011 | 1.270 | 1.057 | 1.525 |
| pN | 0.045 | 2.113 | 1.016 | 4.395 |
| pM | 0.702 | 1.305 | 0.335 | 5.085 |
| Tumour grade | 0.065 | 1.717 | 0.968 | 3.048 |
| FIGO | 0.875 | 0.994 | 0.926 | 1.068 |
| E6CytIRS | 0.475 | 0.961 | 0.863 | 1.071 |
| p16CytIRS | 0.696 | 1.026 | 0.903 | 1.165 |
| p53IRS | 0.267 | 0.892 | 0.729 | 1.092 |
| p53mutIRS | 0.975 | 0.996 | 0.765 | 1.296 |
| MDM2IRS | 0.460 | 1.050 | 0.922 | 1.196 |
| Gal-3 IRS
score | 0.452 | 0.937 | 0.792 | 1.109 |
Discussion
Within the present study, immunohistochemical
evaluation of E6 oncoprotein expression was conducted. In addition,
E6 expression levels were demonstrated to be associated with the
histological subtype. The expression of wild-type p53 and a mutated
form of p53 were identified in the cervical cancer specimens
tested. Finally, correlation analyses revealed a combined positive
expression pattern for galectin-3 and MDM2, and a negative
correlation between E6 and mutated p53 expression.
Although the early era of HPV research identified
that ≤99.5% of cervical cancer cases are HPV-associated (26), it remains controversial in the
literature whether viral load and disease severity are positively
correlated (12). Therefore, the
present study investigated a number of markers that are associated
with HPV-driven changes in cell cycle proteins. Using these markers
permitted a comparative analysis of the influence of HPV on the
progression of cervical cancer for >10 years following
surgery.
The replication of the viral genes E6 and E7 results
in the cellular expression of E6 and E7 oncoproteins, which
interfere with the cell cycle (6). E6
oncoprotein binds to E6-AP, forming a complex that selectively
binds to p53 and leads to its ubiquitin-dependent proteolytic
degradation (7). The present study
demonstrated that E6 immunohistochemistry was a fast and simple
method for the detection of the HPV-associated oncoprotein E6 in
cervical cancer tissues. As a routine practice, E6 and E7 are
detected using either in situ hybridisation (11) or polymerase chain reaction (27) methodology due to the non-specific
immunohistochemical staining results of antibodies used in former
studies (28).
In the present study a well-tested antibody, and
specific antigen retrieval and staining protocol was used,
resulting in the establishment of a useful immunohistochemical
evaluation protocol for the detection of the HPV E6 oncoprotein.
The optimal results were obtained with the E6 antibody supplied by
Abcam (Cambridge, UK). The advantage of immunohistochemical
evaluation is that it is easier to apply and less expensive
compared with mRNA in situ hybridisation. mRNA in
situ hybridisation may be the optimal way to detect HPV;
however, this method is more complicated for routine detection
compared with immunohistochemistry (26). Evaluation of E6 immunohistochemical
staining in cervical cancer tissue has previously revealed positive
correlations with advanced T staging and FIGO classification
(22). Although specific studies have
indicated correlations between E6/E7 gene expression and the
clinicopathological parameters of cervical cancer (26), such a correlation was not demonstrated
in the present study.
An additional finding of the present study is the
negative correlation between E6 and mutated p53 expression.
Mutations of the gene encoding p53 (TP53) are the most
frequent alterations in multiple human malignancies (29–31). In
total, >50% of human tumours contain a mutation/deletion of
TP53, ranging from 5–80% depending on the type, stage and
etiology of the tumours (32). A
number of previous studies have investigated a potential genetic
link between these variations and cancer susceptibility, but the
results have been controversial. A previous meta-analysis study
from 49 pooled studies failed to demonstrate a link between a
common TP53 mutation (25) and
cervical cancer susceptibility (33).
Later on, the same mutation was revealed to be associated with
higher pancreatic cancer risk among males; however, results also
indicated that it may protect Arab women against the development of
breast cancer (34,35). Multiple other mutations of TP53
have since been described. Mutations that deactivate p53 in cancer
are primarily located in the central DNA binding domain. These
mutations typically ablate the ability of the protein to bind to
its target DNA sequences, prevent the transcriptional activation of
p53 target genes. In total, ~80% of the most common p53 mutants
demonstrate the capacity to exert dominant-negative effects over
wild-type p53 and thus prevent the activation of transcription. In
contrast, only 45% of the less frequent mutants studied have this
capacity (36).
The mutation detected by the antibody used in the
present study is an mutation at position 20 (serine to aspartic
acid), which abolishes the phosphorylation site on p53. The
phosphorylation of this serine when DNA damage is detected weakens
the interaction between p53 and MDM2, thereby stabilising p53
(37–39). Thus, this mutation maintains increased
protein levels of p53 following DNA damage. The analysis of the
immunohistochemical detection of mutated p53 revealed that cervical
cancer specimens derived from squamous epithelial tissue
demonstrated significantly higher expression levels compared with
adenocarcinoma tissue. In addition, a positive correlation between
the expression of mutated p53 and MDM2, and a negative correlation
between the expression of mutated p53 and E6, were identified.
Therefore, it is possible to speculate that E6 also degrades the
mutated form of p53. In a previously published study, this mutation
was demonstrated to be associated with the improved survival of
patients with cervical cancer (25).
Finally, a positive correlation between MDM2 and
gal-3 expression was demonstrated in cervical cancer tissue. Little
information concerning the involvement of galectins in cervical
cancer exists at present. Research has primarily focused on gal-1
(40,41), gal-7 (42,43) and
gal-9 (44). A previous publication
described the influence of gal-3 on vascular endothelial growth
factor C expression and its influence on the enhancement of
cervical cancer cell invasiveness (5). The present study demonstrated that gal-3
was a negative independent prognosticator for the overall survival
of patients with p16-negative cervical cancer. In this group of
patients, gal-3 may be responsible for the aggressiveness of
cervical cancer, whereas in p16-positive carcinomas different
factors/signal transduction pathways may be responsible.
In the present study, a total of 250 cervical cancer
cases were systematically analysed for the expression and
interaction of E6, p53, p16, MDM2 and gal-3 in FFPE tumour tissue.
Significantly increased levels of E6 staining were correlated with
an advanced T stage and FIGO classification. Furthermore, MDM2 and
gal-3 expression levels were positively correlated in cervical
cancer. In addition, gal-3 expression levels were negatively
correlated with prognosis in p16-negative cases. As gal-3 is
overexpressed in the cervical cancer tissue of patients with a
worse prognosis, the investigation of gal-3 inhibiting compounds is
an additional task for the development of alternative treatments
for this tumour type. In addition, a negative correlation between
E6 and a mutated form of p53 in cervical cancer was identified. In
conclusion, the results of the present study indicate that
immunohistochemical staining may be a useful method for the
detection the HPV E6 oncoprotein.
Acknowledgements
The present study was supported by the German
Research Foundation. The authors would like to thank Professor
Jutta Engel and Mr. Max Wiedemann (The Munich Cancer Registry,
Munich Tumour Centre, Munich, Germany) for providing the follow-up
data.
References
|
1
|
Munoz N, Bosch FX, Castellsagué X, Díaz M,
de Sanjose S, Hammouda D, Shah KV and Meijer CJ: Against which
human papillomavirus types shall we vaccinate and screen? The
international perspective. Int J Cancer. 111:278–285. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schiffman M, Castle PE, Jeronimo J,
Rodriguez AC and Wacholder S: Human papillomavirus and cervical
cancer. Lancet. 370:890–907. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wittekindt C, Wagner S, Mayer CS and
Klussmann JP: Basics of tumor development and importance of human
papilloma virus (HPV) for head and neck cancer.
Laryngorhinootologie. 91 (Suppl 1):S1–S26. 2012.(In German).
PubMed/NCBI
|
|
4
|
Muñoz N, Bosch FX, de Sanjosé S, Herrero
R, Castellsagué X, Shah KV, Snijders PJ and Meijer CJ:
International Agency for Research on Cancer Multicenter Cervical
Cancer Study Group: Epidemiologic classification of human
papillomavirus types associated with cervical cancer. N Engl J Med.
348:518–527. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zengel P, Assmann G, Mollenhauer M, Jung
A, Sotlar K, Kirchner T and Ihrler S: Cancer of unknown primary
originating from oropharyngeal carcinomas are strongly correlated
to HPV positivity. Virchows Archiv. 461:283–290. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gupta S, Takhar PP, Degenkolbe R, Koh CH,
Zimmermann H, Yang CM, Sim Guan K, Hsu SI and Bernard HU: The human
papillomavirus type 11 and 16 E6 proteins modulate the cell-cycle
regulator and transcription cofactor TRIP-Br1. Virology.
317:155–164. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Scheffner M, Huibregtse JM, Vierstra RD
and Howley PM: The HPV-16 E6 and E6-AP complex functions as a
ubiquitin-protein ligase in the ubiquitination of p53. Cell.
75:495–505. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tang D, Wu D, Hirao A, Lahti JM, Liu L,
Mazza B, Kidd VJ, Mak TW and Ingram AJ: ERK activation mediates
cell cycle arrest and apoptosis after DNA damage independently of
p53. J Biol Chem. 277:12710–12717. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mao C, Balasubramanian A, Yu M, Kiviat N,
Ridder R, Reichert A, Herkert M, von Knebel Doeberitz M and Koutsky
LA: Evaluation of a new p16(INK4A) ELISA test and a high-risk HPV
DNA test for cervical cancer screening: Results from
proof-of-concept study. Int J Cancer. 120:2435–2438. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Melkane AE, Mirghani H, Aupérin A,
Saulnier P, Lacroix L, Vielh P, Casiraghi O, Griscelli F and Temam
S: HPV-related oropharyngeal squamous cell carcinomas: A comparison
between three diagnostic approaches. Am J Otolaryngol. 35:25–32.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Assmann G and Sotlar K: HPV-associated
squamous cell carcinogenesis. Pathologe. 32:391–398. 2011.(In
German). View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Adams AK, Wise-Draper TM and Wells SI:
Human papillomavirus induced transformation in cervical and head
and neck cancers. Cancers (Basel). 6:1793–1820. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Barondes SH, Castronovo V, Cooper DN,
Cummings RD, Drickamer K, Feizi T, Gitt MA, Hirabayashi J, Hughes
C, Kasai K, et al: Galectins: A family of animal
beta-galactoside-binding lectins. Cell. 76:597–598. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hirabayashi J and Kasai KI: Evolution of
animal lectins. Prog Mol Subcell Biol. 19:45–88. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Barondes SH, Cooper DN, Gitt MA and
Leffler H: Galectins. Structure and function of a large family of
animal lectins. J Biol Chem. 269:20807–20810. 1994.PubMed/NCBI
|
|
16
|
Kasai K and Hirabayashi J: Galectins: A
family of animal lectins that decipher glycocodes. J Biochem.
119:1–8. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hirabayashi J, Hashidate T, Arata Y, Nishi
N, Nakamura T, Hirashima M, Urashima T, Oka T, Futai M, Muller WE,
et al: Oligosaccharide specificity of galectins: A search by
frontal affinity chromatography. Biochim Biophys Acta.
1572:232–254. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Boonlikit S and Srisantiroj N: Is there
any clinical advantage in separating CIN 2 from CIN 3 in the
current two-tiered cytological classification? Asian Pac J Cancer
Prev. 10:115–118. 2009.PubMed/NCBI
|
|
19
|
Remmele W, Hildebrand U, Hienz HA, Klein
PJ, Vierbuchen M, Behnken LJ, Heicke B and Scheidt E: Comparative
histological, histochemical, immunohistochemical and biochemical
studies on oestrogen receptors, lectin receptors, and Barr bodies
in human breast cancer. Virchows Arch A Pathol Anat Histopathol.
409:127–147. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mylonas I, Speer R, Makovitzky J, Richter
DU, Briese V, Jeschke U and Friese K: Immunohistochemical analysis
of steroid receptors and glycodelin A (PP14) in isolated glandular
epithelial cells of normal human endometrium. Histochem Cell Biol.
114:405–411. 2000.PubMed/NCBI
|
|
21
|
Mylonas I, Makovitzky J, Richter DU,
Jeschke U, Briese V and Friese K: Cathepsin D expression in normal,
hyperplastic and malignant endometrial tissue: An
immunohistochemical analysis. Acta Histochem. 105:245–252. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kraljevic Z, Visković K, Ledinsky M,
Zadravec D, Grbavac I, Bilandzija M, Soljacić-Vranes H, Kuna K,
Klasnić K and Krolo I: Primary uterine cervical cancer: Correlation
of preoperative magnetic resonance imaging and clinical staging
(FIGO) with histopathology findings. Coll Antropol. 37:561–568.
2013.PubMed/NCBI
|
|
23
|
Ozsarlak O, Tjalma W, Schepens E,
Corthouts B, de Beeck Op B, Van Marck E, Parizel PM and De Schepper
AM: The correlation of preoperative CT, MR imaging, and clinical
staging (FIGO) with histopathology findings in primary cervical
carcinoma. Eur Radiol. 13:2338–2345. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Horn LC, Schierle K, Schmidt D, Ulrich U,
Liebmann A and Wittekind C: Current TNM/FIGO classification for
cervical and endometrial cancer as well as malignant mixed
mullerian tumors. Facts and background. Pathologe. 32:239–243.
2011.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Freier CP, Stiasny A, Kuhn C, Mayr D,
Alexiou C, Janko C, Wiest I, Jeschke U and Kost B:
Immunohistochemical evaluation of the role of p53 mutation in
cervical cancer: Ser-20 p53-Mutant correlates with better
prognosis. Anticancer Res. 36:3131–3137. 2016.PubMed/NCBI
|
|
26
|
zur Hausen H: Papillomaviruses causing
cancer: Evasion from host-cell control in early events in
carcinogenesis. J Natl Cancer Inst. 92:690–698. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hafner N, Gajda M, Altgassen C, Hertel H,
Greinke C, Hillemanns P, Schneider A and Dürst M: HPV16-E6 mRNA is
superior to cytokeratin 19 mRNA as a molecular marker for the
detection of disseminated tumour cells in sentinel lymph nodes of
patients with cervical cancer by quantitative reverse-transcription
PCR. Int J Cancer. 120:1842–1846. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hoffmann M, Tribius S, Quabius ES, Henry
H, Pfannenschmidt S, Burkhardt C, Görögh T, Halec G, Hoffmann AS,
Kahn T, et al HPV DNA: E6*I-mRNA expression and p16INK4A
immunohistochemistry in head and neck cancer-how valid is p16INK4A
as surrogate marker? Cancer Lett. 323:88–96. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nigro JM, Baker SJ, Preisinger AC, Jessup
JM, Hostetter R, Cleary K, Bigner SH, Davidson N, Baylin S, Devilee
P, et al: Mutations in the p53 gene occur in diverse human tumour
types. Nature. 342:705–708. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Petitjean A, Achatz MI, Borresen-Dale AL,
Hainaut P and Olivier M: TP53 mutations in human cancers:
Functional selection and impact on cancer prognosis and outcomes.
Oncogene. 26:2157–2165. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Vogelstein B, Lane D and Levine AJ:
Surfing the p53 network. Nature. 408:307–310. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hainaut P and Hollstein M: p53 and human
cancer: The first ten thousand mutations. Adv Cancer Res.
77:81–137. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Klug SJ, Ressing M, Koenig J, Abba MC,
Agorastos T, Brenna SM, Ciotti M, Das BR, Del Mistro A, Dybikowska
A, et al: TP53 codon 72 polymorphism and cervical cancer: A pooled
analysis of individual data from 49 studies. Lancet Oncol.
10:772–784. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sonoyama T, Sakai A, Mita Y, Yasuda Y,
Kawamoto H, Yagi T, Yoshioka M, Mimura T, Nakachi K, Ouchida M, et
al: TP53 codon 72 polymorphism is associated with pancreatic cancer
risk in males, smokers and drinkers. Mol Med Rep. 4:489–495.
2011.PubMed/NCBI
|
|
35
|
Alawadi S, Ghabreau L, Alsaleh M,
Abdulaziz Z, Rafeek M, Akil N and Alkhalaf M: P53 gene
polymorphisms and breast cancer risk in Arab women. Med Oncol.
28:709–715. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Petitjean A, Mathe E, Kato S, Ishioka C,
Tavtigian SV, Hainaut P and Olivier M: Impact of mutant p53
functional properties on TP53 mutation patterns and tumor
phenotype: Lessons from recent developments in the IARC TP53
database. Hum Mutat. 28:622–629. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bode AM and Dong Z: Post-translational
modification of p53 in tumorigenesis. Nat Rev Cancer. 4:793–805.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chehab NH, Malikzay A, Stavridi ES and
Halazonetis TD: Phosphorylation of Ser-20 mediates stabilization of
human p53 in response to DNA damage. Proc Natl Acad Sci USA.
96:13777–13782. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wade M, Wong ET, Tang M, Stommel JM and
Wahl GM: Hdmx modulates the outcome of p53 activation in human
tumor cells. J Biol Chem. 281:33036–33044. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kim HJ, Do IG, Jeon HK, Cho YJ, Park YA,
Choi JJ, Sung CO, Lee YY, Choi CH, Kim TJ, et al: Galectin 1
expression is associated with tumor invasion and metastasis in
stage IB to IIA cervical cancer. Hum Pathol. 44:62–68. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Huang EY, Chen YF, Chen YM, Lin IH, Wang
CC, Su WH, Chuang PC and Yang KD: A novel radioresistant mechanism
of galectin-1 mediated by H-Ras-dependent pathways in cervical
cancer cells. Cell Death Dis. 3:e2512012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Matsui Y, Ueda S, Watanabe J, Kuwabara I,
Ogawa O and Nishiyama H: Sensitizing effect of galectin-7 in
urothelial cancer to cisplatin through the accumulation of
intracellular reactive oxygen species. Cancer Res. 67:1212–1220.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Tsai CJ, Sulman EP, Eifel PJ, Jhingran A,
Allen PK, Deavers MT and Klopp AH: Galectin-7 levels predict
radiation response in squamous cell carcinoma of the cervix.
Gynecol Oncol. 131:645–649. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Liang MY, Lu YM, Zhang Y and Zhang SL:
Serum galectin-9 in cervical cancer. Zhonghua Yi Xue Za Zhi.
88:2783–2785. 2008.(In Chinese). PubMed/NCBI
|