Introduction
Nuclear medicine consists of using two major classes
of isotopes for therapeutic purposes: Stable ones, not undergoing
radioactive decay in time and unstable ones. Stable isotopes are
mainly used as tracers in pharmacokinetic studies, in order to
investigate biochemical pathways in humans. Stable isotopes already
play an important role in current medical research, with great
future research applications, since the customised synthesis of
novel carbon-13, nitrogen-15 and oxygen-18 radiolabelled compounds,
as well as noble gas isotopes are actively expanding (1). Unstable isotopes have an excess of
neutrons that interact with the protons in the nucleus, which
explains not only their capacity to emit ionizing radiation, but
also their decay, measured through their half-life (1). The stability of radioisotope nuclei is
typically achieved by an α and/or an electron or positron emission,
accompanied by energy emission materialised as gamma-rays
(electromagnetic radiation).
The present study is a review of radionuclide
therapy in oncology, highlighting the new trends in this field.
Approximately 3,800 radiation emitting isotopes can be produced
artificially through neutron activation in a nuclear reactor, or by
other nuclear reaction in a cyclotron or linear accelerator
(2); about 200 radioisotopes have
been investigated for potential medical applications and less than
50 are used clinically on a regular basis (3). Globally, there is high prevalence of
radioisotope use for diagnostic purposes (ca. 90%), common practice
in more than 10,000 hospitals. More specifically, in 26% of the
world's population, representing the total approximate number of
inhabitants of developed countries, diagnostic nuclear medicine
procedures are used with a 1.9% frequency per year, of which
radioisotope therapy represents more or less one tenth. Over 20
million nuclear medicine procedures in 311 million individuals are
carried out in the US per year, whereas about 10 million are
performed in Europe in 500 million individuals (4,5). Australia
is the top country using nuclear medicine for therapeutic purposes
(it is estimated that half the current population will be exposed
to nuclear radiation for different disease therapies) (6).
Radionuclide therapy for different types of
cancer
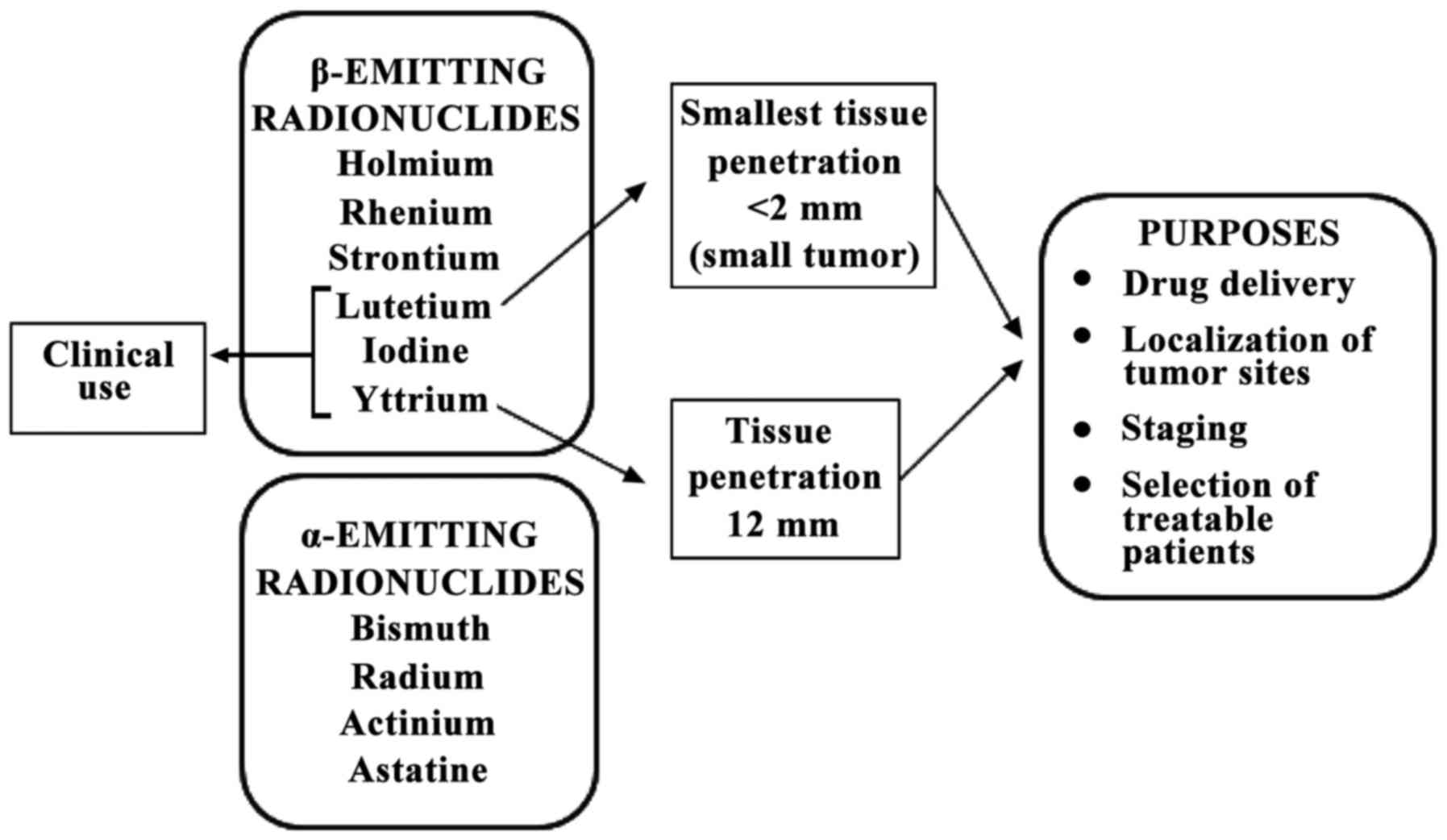
Current clinical and preclinical research targeting
internal radiotherapy for oncology purposes involves at least 13
β-emitting radionuclides (177Lutetium,
166Holmium, 186Rhenium,
188Rhenium, 67Copper,
149Promethium, 199Gold, 77Bromine,
153Samarium, 105Rhodium,
89Strontium, 90Yttrium and
131Iodine) and four α-emitting radionuclides
(213Bismuth, 223Radium,
225Actinium and 211Astatine) (7–9),
characterised by different ranges, distance of effectiveness and
relative biologic efficacy (RBE). Notwithstanding this number, the
full implementation of targeted radiopharmaceutical therapeutics
still suffers from a shortage of radionuclides for research and
clinical trials, the more so as of the above radionuclides, only
90Y and 131I are readily available in a form
suitable for clinical trial use. These are used in association with
monoclonal antibodies in the treatment of non-Hodgkin's lymphoma,
whereas samarium-153-EDTMP and strontium-89-chloride are included
in the palliation of bone metastases. 177Lutetium is the
radionuclide with the most attractive physical properties for
oncology due to its emission characteristics (0.5 MeV maximum
energy β emission and <2 mm tissue penetration) permit the
energy to focus on the tumour rather than on the surrounding
healthy tissue. In comparison to 90Y, whose particle
range is 12 mm, this is more suitable for small tumours (Fig. 1).
Current clinical practice is characterised by the
immediate and sharp need for α-emitting therapeutic radionuclides,
featuring higher (ca. 100 keV/µm) linear energy transfer (LET) and
shorter action range, able to yield much more selective and
localised cytotoxicity. In addition to α-emitters, the variety of
available theranostics (isotope compounds allowing for both imaging
and therapy) needs to include β-emitters for improved determination
of the radiation dose (10).
As far as therapy is concerned, the suitability of a
particular radionuclide primarily relies on radionuclide
properties, both physical and chemical, on manufacturing methods,
as well as on biological behaviour (the more so if in vivo
dissociation from the carrier molecule is involved); however, other
additional aspects, such as specific activity, radionuclide purity,
target nuclide occurrence in the environment, feasibility and ease
of radionuclide production in a suitable form for application
should not be overlooked either (11). In addition, the efficacy of
radionuclide therapies could be further enhanced by implementing
fractionated dose radiotherapy schemes, combining
radiopharmaceutical with radio-sensitizing medication, or adopting
pre-targeting radionuclide strategies (pRIT). Molecular imaging
probes function by the delivery of radionuclides to tumour tissue
directed to antibodies or peptides, targeting specific
malignancy-related biochemical pathways enabling non-invasive
imaging at molecular level. Since biochemical alterations occur at
an earlier stage compared to the detection of anatomical
abnormalities, molecular imaging probes allow the efficient
early-stage localization of tumour sites, accurate disease staging
and restaging, tracking of drug effectiveness, systemic treatment
of all disease sites, monitoring of treatment response and the
selection of patients suitable for radionuclide-based therapies,
facilitating personalised diagnostic and treatment strategies
(12). In systemic radiotherapy,
radiolabelled molecular probes targeting the same biochemical
processes deliver in situ high destructive capacity of β-
and α-emitting radionuclides, which destroy cancer cells by
damaging their DNA. This has been proven to be effective for the
treatment of several malignancies, enabling the eradication of
disseminated tumour cells and small metastases (13).
Accounting for 15% of all malignancies typically
diagnosed in males (14), prostate
cancer ranks the most frequent cancer affecing males worldwide,
resulting in significant morbidity and mortality. Although usually
presenting in early stages, the number of patients with metastases
at diagnosis is important. Radical prostatectomy and external beam
radiotherapy are used for treatment of local disease, whereas
androgen deprivation therapy or chemotherapy are the available
choices for metastatic stages (15).
Prostate specific membrane antigen (PSMA) is a type
II transmembrane protein on the surface of neoplastic prostate
cells, which currently is the most promising target for both
imaging and treatment, since it is upregulated in the majority of
cases of prostate cancer, regardless of disease stage. Furthermore,
PSMA is internalised following antibody binding, while is not
released into the blood stream. PSMA may be encountered in normal
tissues as the lacrimal glands, the salivary glands or the small
intestine; however, in normal prostatic tissue, PSMA is expressed
only in the apical epithelium of secretory ducts at low levels. In
recent years, positron emitting compounds that target PSMA have
shown great potential for the accurate detection of all disease
sites, regardless of the levels of prostate-specific antigen (PSA).
In addition, PSMA peptides and antibodies can be conjugated with
131I, 90Y or 177Lu for the
treatment of metastatic, castrate-resistant prostate cancer.
However, for the treatment of advanced prostate cancer, the FDA,
for instance, has approved no PSMA targeting radionuclide therapy.
This type of peptide most often described in the literature is
PSMA-DKFZ-617. Apart from being easily conjugated with peptides,
177Lu has the advantage of a long half-life. Therefore,
it irradiates on a very small area, but for a long period of time.
In most reported trials, 177Lu is administered at 6-week
intervals or longer (16).
A multicentre German trial enrolling 145 patients
analysed the efficacy of 177Lu as a therapeutic agent in
patients with advanced stage prostate cancer. The patients were
exposed to a maximum of 4 cycles of radioisotope therapy, with a
total dosage of 8 GBq. The study primary endpoint was the
biochemical response, the level of PSA being determined for 16
weeks after treatment, but toxicity was also reported. During
treatment or follow-up, 19 patients died, 18 had grade 3 or 4
toxicities reported, among which xerostomia was the most frequent.
By the end of follow-up time (16 weeks), 45% of the patients
exhibited a decrease of ≥50% in PSA levels. The response was early
in over 40% of the patients, usually after the first course
(17).
A different trial enrolling 82 patients reported
similar response rates to only one administration of isotope-based
therapy. The biochemical response rate (defined as an >50%
decrease in PSA levels) was 31%. Furthermore, 47% displayed a
25–50% decrease in PSA levels and in another 23% of patients, PSA
levels increased by <25% (18).
Thus, radiolabelled PSMA ligands hold promise for
the management of patients with metastatic prostate cancer,
enabling accurate imaging, disease staging, restaging and therapy,
facilitating personalised treatment strategies.
Radionuclide therapy has also been employed in the
management of patients diagnosed with neuroendocrine tumours
(NETs). Localised NETs are treated with surgical excision. However,
>40% of patients with NETs present with metastatic disease on
diagnosis, requiring the application of systemic treatment
strategies. Gastrointestinal NETs have been investigated with
177Lu-DOTATATE scintigraphy for some time now, enabling
the detection of metastatic sites that were not visible by means of
anatomical imaging techniques. Furthermore, this investigation
informs on the tumour affinity for this isotope, revealing patients
with a high likelihood to respond positively. The phase III,
randomised NETTER-1 trial revealed remarkable tolerability and
efficiency for 177Lu-DOTATATE. The study enrolled 230
patients with midgut, metastatic NETs already receiving long acting
release-LAR octreotide (19).
The enrolled patients were randomly assigned to
receive 177Lu-DOTATATE combined with LAR octreotide or
LAR octreotide alone. The final results have not yet been
published, but intermediate analysis of the data shows a clear
advantage for isotope therapy in progression-free survival (PFS).
The LAR octreotide arm has reached this endpoint, with an 8.4
months PFS. The fact that such PFS is rarely achieved in cancer
holds great promise for the role of PRRT (peptide receptor
radionuclide therapy) in (neo)adjuvant management of patients with
NETs (19).
As previously mentioned (3), 90Y is another option for
isotope-based treatments. Not only does it emit the highest levels
of β energy with a maximum of 2.28 MeV, but it also has important
tissue penetration: 12 mm, which is why it should be administered
locally.
SIR-spheres, the radioactive units that can be used
for selective internal radiation therapy in hepatic metastases or
primary tumours, contain 90Y. For colorectal cancer
(CRC) with liver metastases, they have been tested alone, in
comparison to chemoembolisation, or together with systemic therapy
(20).
The efficacy and toxicity profiles of the combined
approach are just beginning to be studied. The SIRFLOX study
enrolled 530 patients with CRC and unresectable liver metastases.
They were randomised to first-line treatment with FOLFOX VI
(bevacizumab at investigator's discretion) alone or with
SIR-spheres. The median PFS was 10.7 months in the SIR-spheres arm
vs. 10.2 in the standard of care arm. There was a significantly
longer median duration of liver PFS in a completing risk analysis
(20.5 vs. 12.6 months; HR, 0.69; 95% CI, 0.55–0.90). There was no
significant improvement in the rate of subsequent liver resection
in the SIR group. Worse toxicities more common with SIR-spheres
were neutropenia (41% as compared to 29%), febrile neutropenia (6%
as compared to 2%), thrombocytopenia (10% as compared to 3%),
gastric or duodenal ulcer (4% as compared to 0%), and ascites (23%
as compared to 0%). One also has to take into account that that
team needed for SIR-spheres administration consists in a wide
variety of medical specialties and the procedure itself is
expensive and long-lasting. Therefore, until further research is
undertaken, radioembolisation is not a standard first line-therapy,
but can be taken into account for later lines of therapy (20).
As opposed to conventional chemotherapy,
radioimmunotherapy enables specific targeting of malignant cells
and delivery of monoclonal antibodies. This strategy has been
proven to be efficient in the treatment of low-grade B-cell
non-Hodgkin lymphoma, by using 90Y or 131I
marked monoclonal antibodies: 90Y-ibritumomab tiuxetane
and 131I tositumomab. Tositumomab has high affinity for
the CD20 receptor on the B lymphocyte surface, either malignant or
normal. When both these agents reach their target, they not only
have the classical monoclonal antibody effect, but also deliver
ionizing radiation to the cell (21,22).
The same strategy was used for pancreatic cancer.
90Y-clivatuzumab is a complex targeting the hPAM4
antigen that resides on pancreatic ductal malignant cells only.
This complex was administered together with gemcitabine in a small
dosage in 38 patients with locally-advanced and metastatic
pancreatic cancer enrolled in a phase II clinical trial.
Gemcitabine was administered for 4 weeks at a dosage of 200
mg/m2. The isotope-antibody complex had three
administrations, in weeks 2, 3 and 4. In 28 patients, grade 3 or 4
thrombocytopenia was reported, although it is thought that
fractionation contributed to a lower toxicity profile. Six patients
displayed partial response and stable disease was reported in 16,
with 7.7 months PFS, demonstrating the efficacy of this option
(23).
One of the first radionuclide therapy alternatives
ever used was in cases of papillary or follicular thyroid cancer.
The medullary type, lymphoma or anaplastic types do not have the
tumour biology necessary to take up the isotope, therefore in these
cases such treatment has no purpose. 131I is both a
local treatment, providing the ablation of the remaining
post-operative tissue and a treatment of the possibly existing
metastases. It was repeatedly proven that it prolongs PFS and
overall survival, being a highly active treatment (24).
Radioiodine has dose dependent toxicity. A higher
incidence of leukaemia and solid malignancies has been reported in
the treated population, compared to general one. Due to the
relatively low dose delivered to other tissues, only patients
exposed to high cumulative 131I activities (>600 mCi)
are considered at risk. However, in the case of a patient with
functioning thyroid metastases, these doses can be necessary
(25). This is why the need to
separate responders from non-responders to radioiodine is a pending
issue. A mathematical model has recently been established for
treatment individualisation. A clinical trial with this purpose
enrolled 50 patients initially treated with total thyroidectomy
associated with lymph node dissection and subsequent radiation
therapy. The criteria for patient classification as responders or
non-responders were decrease of number of RAI-avid foci and the
absence of new lesions on post-therapy body scan and, most
importantly, decrease in stimulating thyroglobulin (Tg) over time.
Tumour doubling time (Td) was an additional important
parameter. This study shows usefulness of mathematical modelling in
clinical decision-making and delivery of personalised care
(26,27).
Head and neck cancers can also benefit from
radionuclide-related procedures, both diagnostic and therapeutic.
One example is passive nanotargeting delivery of radionuclides for
tumour radiotherapy. This concept was first used for tumour
imaging. Radiolabelled pegylated liposomes used to target solid
tumours also proved useful for delivery of β-emitting
radionuclides, especially in head and neck patients (28).
However, several new detection methods have been
imagined for cancer detection in the early stages. Colorimetric,
narrow band imaging, video contact endoscopy and SPIES software
filters represent a category of so-called optical biopsy that help
the surgeon to early detect and define the tumour margins for free
disease resection margin (29–33). ELISA
and flow cytometric analysis allow the evaluation of tumour cells,
which can influence the prognosis (34).
Scattered, painful bone metastases often bring about
poor quality of life in breast cancer patients. The only option in
most cases is energetic, however for the price of toxicity and
dependence. Radiopharmaceuticals, such as
186Re-hydroxyethylidene diphosphonate (HEDP) are an
attractive alternative. The overall response rate to this compound
is >70%. Given its short half-life, bone marrow toxicity is low
in this case. Choosing a more aggressive, longer half-life compound
could generate bone marrow suppression in a heavily pre-treated
patient. An additional advantage is its easy, safe administration
that does not require specialised personnel; therefore, this option
should be taken into account whenever the clinical situation
permits (35).
Conclusions
In conclusion, 131I is no longer the only
efficient radionuclide therapy in oncology and a new, promising era
of novel malignancy specific radiopharmaceuticals is actively
emerging potentially improving the management and outcomes for
oncologic patients. Highly specific and more sophisticated
strategies such as radioimmunotherapy increase the treatment
arsenal, paving the way towards individualised medicine. However,
the full potential of this field is far from being completely
exploited. Randomised double-blinded multicentre prospective
studies are needed in order to elucidate potential contribution to
therapeutic efficacy of radionuclide therapies in comparison to
conventional therapeutic schemes.
References
|
1
|
Stable isotopes, . http://chemistry.tutorvista.com/inorganic-chemistry/stable-and-unstable-isotopes.htmlApril
16–2017
|
|
2
|
Nuclear Medicine: Medical isotopes:
General concepts. https://www.radiochemistry.org/nuclearmedicine/radioisotopes/01_isotopes.shtml#topApril
16–2017
|
|
3
|
American Nuclear Society: Medical use of
radioisotopes. 2014, http://www.nuclearconnect.org
|
|
4
|
Australian Nuclear Science Technology
Organisation: What are radioisotopes? http://www.ansto.gov.au/NuclearFacts/AboutNuclearScience/RadioisotopesApril
16–2017
|
|
5
|
World Nuclear Association: Radioisotopes
in medicine. http://www.world-nuclear.org/information-library/non-power-nuclear-applications/radioisotopes-research/radioisotopes-in-medicine.aspx(Updated
December 2016). April. 2017
|
|
6
|
Zalutsky MR: Radionuclide therapyHandbook
of Nuclear Chemistry: Radiochemistry and Radiopharmaceutical
Chemistry in Life Sciences. Roesch F: 4. Kluwer Academic;
Dordrecht: pp. 315–348. 2003
|
|
7
|
Harris TJR, Kalen JD and Hall J: Report of
meeting held to discuss existing and future radionuclide
requirements for the national cancer institute. https://www.isotopes.gov/outreach/reports/Radionuclide_Report.pdf
|
|
8
|
Nordberg E, Orlova A, Friedman M,
Tolmachev V, Ståhl S, Nilsson FY, Glimelius B and Carlsson J: In
vivo and in vitro uptake of 111In, delivered
with the affibody molecule (ZEGFR:955)2, in
EGFR expressing tumour cells. Oncol Rep. 19:853–857.
2008.PubMed/NCBI
|
|
9
|
Sabongi JG, Gonçalves MC, Alves CD, Alves
J, Scapulatempo-Neto C and Moriguchi SM: Lutetium 177-DOTA-TATE
therapy for esthesioneuroblastoma: A case report. Exp Ther Med.
12:3078–3082. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bobeica M, Niculae D, Balabanski D,
Filipescu D, Gheorghe I, Ghita DG and Luo W: Radioisotope
production for medical applications at ELI-NP. Rom Rep Phys. 68
Suppl:847–83. 2016.
|
|
11
|
Cutler CS, Chanda N, Shukla R, Sisay N,
Cantorias M, Zambre A, McLaughlin M, Kelsey J, Upenandran A,
Robertson D, et al: Nanoparticles and phage display selected
peptides for imaging and therapy of cancer. In: Theranostics,
Gallium-68 and Other RadionuclidesRecent Results in Cancer
Research. 194. Baum RP and Rosch F: Springer; Heidelberg: pp.
133–147. 2013, View Article : Google Scholar : PubMed/NCBI
|
|
12
|
National Research Council (US) and
Institute of Medicine (US) Committee on State of the Science of
Nuclear Medicine: Advancing nuclear medicine through innovation.
National Academies Press; Washington, DC: 2007
|
|
13
|
Kwekkeboom DJ, Mueller-Brand J, Paganelli
G, Anthony LB, Pauwels S, Kvols LK, O'dorisio TM, Valkema R, Bodei
L, Chinol M, et al: Overview of results of peptide receptor
radionuclide therapy with 3 radiolabeled somatostatin analogs. J
Nucl Med. 46 Suppl 1:62–66. 2005.
|
|
14
|
Emmet L, Willowson K, Violet J, Shin J,
Blanksby A and Lee J: Lutetium177 PSMA radionuclide therapy for men
with prostate cancer: A review of the current literature and
discussion of practical aspects of therapy. J Med Radiat Sci.
64:52–60. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Weill Cornell Medicine: Using radiation,
radioimmunotherapy and radioactive isotopes such as lutetium 177 to
treat prostate cancer. https://weillcornellgucancer.org/2017/01/12/using-radiation-radioimmunotherapy-and-radioactive-isotopes-such-as-lutetium-177-to-treat-prostate-cancerApril
16–2017
|
|
16
|
Ahmadzadehfar H, Rahbar K, Kürpig S,
Bögemann M, Claesener M, Eppard E, Gärtner F, Rogenhofer S,
Schäfers M and Essler M: Early side effects and first results of
radioligand therapy with (177)Lu-DKFZ-617 PSMA of
castrate-resistant metastatic prostate cancer: a two-centre study.
EJNMMI Res. 5:1142015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rahbar K, Ahmadzadehfar H, Kratochwil C,
Haberkorn U, Schäfers M, Essler M, Baum RP, Kulkarni HR, Schmidt M,
Drzezga A, et al: German multicenter study investigating
177Lu-PSMA-617 radioligand therapy in advanced prostate
cancer patients. J Nucl Med. 58:85–90. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rahbar K, Schmidt M, Heinzel A, Eppard E,
Bode A, Yordanova A, Claesener M and Ahmadzadehfar H: Response and
tolerability of a single dose of 177Lu-PSMA-617 in
patients with metastatic castration-resistant prostate cancer: A
multicenter retrospective analysis. J Nucl Med. 57:1334–1338. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Strosberg J, El-Haddad G, Wolin E,
Hendifar A, Yao J, Chasen B, Mittra E, Kunz PL, Kulke MH, Jacene H,
et al: NETTER-1 Trial Investigators: Phase 3 trial of
177Lu-Dotatate for midgut neuroendocrine tumors. N Engl
J Med. 376:125–135. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
van Hazel GA, Heinemann V, Sharma NK,
Findlay MP, Ricke J, Peeters M, Perez D, Robinson BA, Strickland
AH, Ferguson T, et al: SIRFLOX: Randomized phase III trial
comparing first-line mFOLFOX6 (plus or minus bevacizumab) versus
mFOLFOX6 (plus or minus bevacizumab) plus selective internal
radiation therapy in patients with metastatic colorectal cancer. J
Clin Oncol. 34:1723–1731. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Weigert O, Illidge T, Hiddemann W and
Dreyling M: Recommendations for the use of yttrium-90 ibritumomab
tiuxetan in malignant lymphoma. Cancer. 107:686–695. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kaminski MS, Tuck M, Estes J, Kolstad A,
Ross CW, Zasadny K, Regan D, Kison P, Fisher S, Kroll S and Wahl
RL: 131I-tositumomab therapy as initial treatment for
follicular lymphoma. N Engl J Med. 352:441–449. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ocean AJ, Pennington KL, Guarino MJ,
Sheikh A, Bekaii-Saab T, Serafini AN, Lee D, Sung MW, Gulec SA,
Goldsmith SJ, et al: Fractionated radioimmunotherapy with (90)
Y-clivatuzumab tetraxetan and low-dose gemcitabine is active in
advanced pancreatic cancer: A phase 1 trial. Cancer. 118:5497–5506.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tuttle RM: Differentiated thyroid cancer:
Radioiodine treatment. Ross DS and Mulder JE: https://www.uptodate.com/contents/differentiated-thyroid-cancer-radioiodine-treatment?source=see_linkApril
18–2017 View Article : Google Scholar
|
|
25
|
Nixon IJ, Ganly I, Patel SG, Palmer FL, Di
Lorenzo MM, Grewal RK, Larson SM, Tuttle RM, Shaha A and Shah JP:
The results of selective use of radioactive iodine on survival and
on recurrence in the management of papillary thyroid cancer, based
on Memorial Sloan-Kettering Cancer Center risk group
stratification. Thyroid. 23:683–694. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer, . Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,
Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, et
al: Revised American Thyroid Association management guidelines for
patients with thyroid nodules and differentiated thyroid cancer.
Thyroid. 19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Barbolosi D, Summer I, Meille C, Serre R,
Kelly A, Zerdoud S, Bournaud C, Schvartz C, Toubeau M, Toubert ME,
et al: Modeling therapeutic response to radioiodine in metastatic
thyroid cancer: A proof-of-concept study for individualized
medicine. Oncotarget. 8:39167–39176. 2017.PubMed/NCBI
|
|
28
|
Harrington KJ, Mohammadtaghi S, Uster PS,
Glass D, Peters AM, Vile RG and Stewart JS: Effective targeting of
solid tumors in patients with locally advanced cancers by
radiolabeled pegylated liposomes. Clin Cancer Res. 7:243–254.
2001.PubMed/NCBI
|
|
29
|
Stefanescu DC, Ceachir O, Zainea V,
Hainarosie M, Pietrosanu C, Ionita IG and Hainarosie R: Methilene
blue video contact endoscopy enhancing methods. Rev Chim.
67:1558–1559. 2016.
|
|
30
|
Hainarosie R, Ceachir O, Zainea V,
Hainarosie M, Pietrosanu C, Zamfir C and Stefanescu DC: The test of
lugol iodine solution associated with NBI examination in early
diagnostic of tongue carcinoma. Rev Chim. 68:226–227. 2017.
|
|
31
|
Stefanescu DC, Ceachir O, Zainea V,
Hainarosie M, Pietrosanu C, Ionita IG and Hainarosie R: The use
ofmethylene blue in assessing disease free margins during
CO2 LASER assisted direct laryngoscopy for glottis
cancer. Rev Chim. 67:1327–1328. 2016.
|
|
32
|
Hainarosie R, Zainea V, Ceachir O,
Hainarosie M, Pietrosanu C and Stefanescu DC: The use of methylene
blue in early detection of the vocal fold cancer. Rev Chim.
68:16–17. 2017.
|
|
33
|
Stefanescu DC, Ceachir O, Zainea V,
Hainarosie M, Pietrosanu C, Ionita IG and Hainarosie R: The value
of toluidine blue staining test in assessing disease free margins
of oral cavity carcinomas. Rev Chim. 67:1255–1256. 2016.
|
|
34
|
Petrică-Matei GG, Iordache F, Hainăroşie R
and Bostan M: Characterization of the tumor cells from human head
and neck cancer. Rom J Morphol Embryol. 57 Suppl:791–799.
2016.PubMed/NCBI
|
|
35
|
Lam MG, de Klerk JM and van Rijk PP:
186Re-HEDP for metastatic bone pain in breast cancer
patients. Eur J Nucl Med Mol Imaging. 31 Suppl 1:162–170. 2004.
View Article : Google Scholar : PubMed/NCBI
|