Introduction
Lung cancer involves malignant tumors with highest
morbidity and mortality rates thought the world. Further, rising
levels of environmental pollution and the effects of smog on
respiratory system could not be underestimated, especially in China
(1,2).
The incidence of lung cancer in the next few decades is expected to
further rise (3). According to
pathological classification, lung cancer could be divided into
small cell lung cancer and non-small cell lung cancer (NSCLC).
NSCLC accounts for more than 80% of cases. Also, more than 2/3 of
NSCLC patients are diagnosed at advanced stage. So, the diagnostics
are poor and the 5-year survival rate of this disease is extremely
low (4).
Previous studies have confirmed that lung infection
due to nosocomial infection is a common cause of death in patients
with advanced lung cancer. The antibiotic-based treatment is the
main treatment approach for the lung cancer patients with pulmonary
infection (5). The effect of
conventional antibiotic treatment is limited with the emergence of
drug resistance. So, it would be of significant value to understand
the distribution of drug resistance in patients with advanced lung
cancer. This approach could further improve the treatment effect
and extend their survival time (6).
The present study summarized the characteristics of nosocomial
infection in chemotherapy patients with advanced NSCLS. We also
discussed the impact of nosocomial infection on the survival of
patients.
Materials and methods
General information
Retrospective analysis was used to analyze the
information of the 169 chemotherapy patients with NSCLC and
nosocomial infection during hospitalization; 170 patients without
nosocomial infection were also involved as a control group. All the
patients were diagnosed as non-small cell lung cancer by fiberoptic
bronchoscopy and biopsy. All the patients in observation group had
nosocomial infection. There were 126 males and 44 females in the
observation group. The ages ranged from 45 to 70 with a mean age of
61±1.0 years. The duration of disease ranged from 3 months to 2
years with a mean value of 5.1±0.2 months. Other clinical data of
the patients in observation group included length of
hospitalization, invasive operation, combination of two or more
medical diseases, the use of prophylactic antibiotics, use of
glucocorticoids and immunosuppressive agents. The patients with
immune system disease and the patients who were combined with
malignant tumors were excluded. The study obtained approval from
the Ethics Committee of Binzhou City Central Hospital and all the
participants signed the informed consent before enrollment.
Observation indicators
The distribution of pathogens in nosocomial
infection in patients with advanced NSCLC was statistically
analyzed. The distribution of major drug resistance of
Gram-negative (G−) and Gram-positive (G+)
were analyzed. The survival conditions of the patients were
studied. The risk factors of nosocomial infection in patients with
NSCLC were analyzed by univariate and multivariate logistic
analyses.
Bacterial culture and species
identification
According to the ‘National Clinical Laboratory
Procedures’, routine testing methods were utilized. Drug
susceptibility test was performed by paper diffusion method (K-B
method). CLSI 2008–2010 operation procedures and result evaluation
standards were used. Columbia blood plate, MH plates, identifying
culture medium and drug sensitive slips were provided by the Oxoid
(London, UK). The quality control strains viz. Staphylococcus
aureus ATCC 25923, Pseudomonas aeruginosa ATCC 27853 and
Escherichia coli ATCC 25922 were provided by provincial CDC
clinical laboratory test center. The KB method is mainly used for
the detection of ampicillin, cefotaxime, cefepime, ceftazidime,
imipenem, clindamycin, vancomycin, erythromycin, roxithromycin,
gentamicin and amikacin. The corresponding biological reagents were
procured from Hangzhou Tianhe Microoragnism Reagents Co., Ltd.
(Hangzhou, China). MH agar plates were stored at 4°C before use.
Technicians with >5 years laboratory experience had performed
all operations in strict accordance with the instructions.
Survey methods
The investigators were trained in a unified manner.
The informed consent of the respondents was obtained. The
investigators were familiar with the contents of the questionnaire
and solutions to the frequently asked questions. Reliability
coefficient was applied with values ranged from 0 to 1. The
reliability of this study was 0.996. Two tests were performed using
the same questionnaire on all subjects with an interval of 30 days
to obtain the stability coefficient.
Statistical analysis
SPSS 21.0 software was utilized for statistical
analyses (IBM, Armonk, NY, USA). The data were expressed as mean ±
standard deviation. The t-test was used to compare the mean of the
two groups. The χ2 test was used to compare the rates of
the two groups. The univariate and multivariate logistic regression
analysis was used for the analysis of correlation between the
factors and the disease. P<0.05 was considered as statistically
significant.
Results
The distribution of pathogens in
nosocomial infection in chemotherapy patients with advanced
NSCLC
G+ infection accounted for 45.6% cases.
Staphylococcus aureus and coagulase-negative staphylococci
were the most common species. The proportion of G−
infection was 54.4%, of which Pseudomonas aeruginosa and
Klebsiella pneumoniae were most common (Table I).
 | Table I.The distribution of pathogens in
nosocomial infection in chemotherapy patients with advanced
NSCLC. |
Table I.
The distribution of pathogens in
nosocomial infection in chemotherapy patients with advanced
NSCLC.
| Pathogen species | No. of strains
(n) | Proportion (%) |
|---|
| G+ |
| 45.6 |
| Staphylococcus
aureus | 41 | 24.3 |
|
Coagulase-negative | 36 | 21.3 |
|
Staphylococcus |
|
|
| G− |
| 54.4 |
| Pseudomonas
aeruginosa | 27 | 16.0 |
| Klebsiella
pneumoniae | 23 | 13.6 |
| Escherichia
coli | 19 | 11.2 |
| Enterobacter
cloacae | 14 | 8.3 |
| Enterobacter
aerogenes | 9 | 5.3 |
The main drug resistance distribution
of G−
The most common drug-resistant antibiotics for
Pseudomonas aeruginosa were sulfamethoxazole, ciprofloxacin
and cefotaxime, while the most common drug-resistant antibiotics
for Klebsiella pneumoniae infection were sulfonamides and
gentamicin (Table II).
| Table II.The main drug resistance distribution
of G− [n (%)]. |
Table II.
The main drug resistance distribution
of G− [n (%)].
| Antibiotics | Pseudomonas
aeruginosa (n=27) | Klebsiella
pneumoniae (n=23) |
|---|
| Cefotaxime | 13 (48.1) | 5 (21.7) |
| Cefepime | 9 (33.3) | 6 (26.1) |
| Ceftazidime | 9 (33.3) | 6 (26.1) |
| Amikacin | 6 (22.2) | 4 (17.4) |
| Ciprofloxacin | 15 (55.6) | 5 (21.7) |
| Levofloxacin | 7 (25.9) | 6 (26.1) |
| Imipenem | 7 (25.9) | 0 (0) |
| Meropenem | 6 (22.2) | 0 (0) |
| Sulfamethoxazole | 16 (59.3) | 11 (47.8) |
| Gentamicin | 12 (44.4) | 9 (39.1) |
The main drug resistance distribution
of G+
The most common drug-resistant antibiotics for
Staphylococcus aureus were penicillin G, ampicillin and
sulfamethoxazole, while the most common drug-resistant antibiotics
for coagulase-negative staphylococci were penicillin G, ampicillin
and sulfamethoxazole. Both of the G+ bacteria were
sensitive to vancomycin and teicoplanin, and even more sensitive to
imipenem or meropenem (Table
III).
| Table III.The main drug resistance distribution
of G+ [n (%)]. |
Table III.
The main drug resistance distribution
of G+ [n (%)].
| Antibiotics | Staphylococcus
aureus (n=41) | Coagulase-negative
staphylococci (n=36) |
|---|
| Penicillin G | 40 (97.6) | 35 (97.2) |
| Ampicillin | 39 (95.1) | 34 (94.4) |
| Erythromycin | 18 (43.9) | 11 (30.6) |
| Roxithromycin | 19 (46.3) | 9 (25.0) |
| Vancomycin | 0 (0) | 0 (0) |
| Teicoplanin | 0 (0) | 0 (0) |
| Sulfamethoxazole | 23 (56.1) | 20 (55.6) |
| Gentamicin | 12 (29.3) | 11 (30.6) |
| Ciprofloxacin | 11 (26.8) | 16 (44.4) |
| Levofloxacin | 17 (41.5) | 13 (36.1) |
The characteristics of distribution of
nosocomial infection sites
Nosocomial infections were most commonly found in
respiratory system followed by the urinary system and digestive
system, infections in skin, soft tissue and other parts (such as
intracranial infection and intra-articular infection) (Table IV).
| Table IV.The characteristics of distribution
of nosocomial infection sites. |
Table IV.
The characteristics of distribution
of nosocomial infection sites.
| Infection
sites | Infection cases
(case) | Infection rate
(%) |
|---|
| Respiratory
system | 102 | 60.4 |
| Digestive
system | 35 | 20.7 |
| Urinary system | 51 | 30.2 |
| Blood system | 21 | 12.4 |
| Skin and soft
tissue | 10 | 5.9 |
| Other parts | 3 | 1.8 |
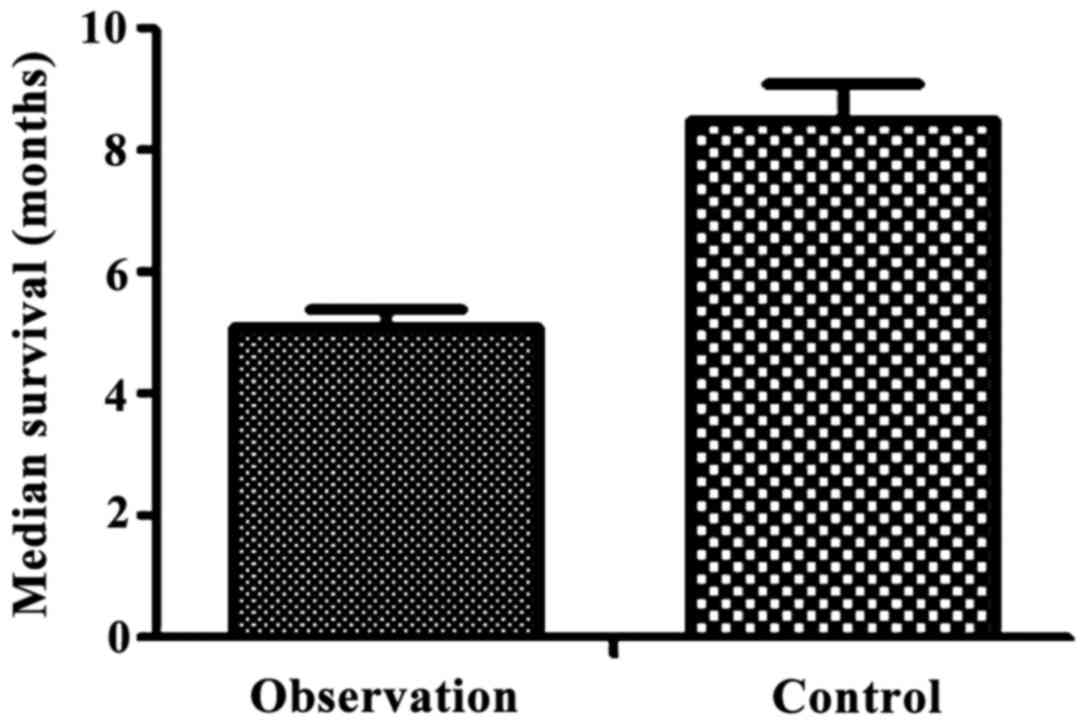
Comparison of the survival conditions
between observation group and control group
The median survival time of the observation group
was 5.1±0.3 months, while the median survival time of the control
group was 8.5±0.6 months. Therefore, the median survival time of
the observation group was significantly shorter than that of the
control group (t=65.928, P<0.05) (Fig.
1). The median survival time of the observation group was
5.1±0.3 months, while the median survival time of the control group
was 8.5±0.6 months. So, the median survival time of the observation
group was significantly shorter than that of the control group
(t=65.928, P<0.05).
Analyses of risk factors of nosocomial
infection in patients with advanced with NSCLC
Invasive operation, combination of two or more
diseases, the use of glucocorticoids and immunosuppressive agents
in the course of treatment were observed commonly for NSCLC
patients who were older than 60 years and have been hospitalized
for 30 days or more (Table V).
| Table V.Analysis of risk factors of nosocomial
infection in patients with advanced NSCLC. |
Table V.
Analysis of risk factors of nosocomial
infection in patients with advanced NSCLC.
| Risk factors | Cases | Infection rate
(%) |
|---|
| Sex |
|
|
| Male | 125 | 74.0 |
|
Female | 44 | 26.0 |
| Age (years) |
|
|
|
≥60 | 100 | 59.2 |
|
<60 | 69 | 40.8 |
| Length of
hospitalization |
|
|
| ≥30
days | 95 | 65.1 |
| <30
days | 74 | 34.9 |
| Invasive
operation |
|
|
|
Yes | 115 | 68.0 |
| No | 54 | 32.0 |
| Combination of two
or more medical diseases |
|
|
|
Yes | 100 | 59.2 |
| No | 69 | 40.8 |
| Preventive use of
antimicrobial agents |
|
|
|
Yes | 75 | 44.4 |
| No | 94 | 55.6 |
| Use of
glucocorticoids |
|
|
|
Yes | 123 | 72.8 |
| No | 46 | 27.2 |
| Use of
immunosuppressive agents |
|
|
|
Yes | 111 | 65.7 |
| No | 58 | 34.3 |
Multivariate logistic analysis of
nosocomial infection in patients with advanced NSCLC
Multivariate regression analysis showed that age
over 60 years, invasive operation, combination of two or more
diseases, the use of glucocorticoids and immunosuppressive agents
were independent risk factors for nosocomial infection in patients
with advanced NSCLC (Table VI).
| Table VI.Multivariate logistic analysis of
nosocomial infection in patients with advanced NSCLC. |
Table VI.
Multivariate logistic analysis of
nosocomial infection in patients with advanced NSCLC.
| Independent risk
factors | Partial regression
coefficient | Standard error | P-value | OR value | χ2
value |
|---|
| Age over 60
years | 0.321 | 0.203 | 0.012 | 1.025 | 6.361 |
| Invasive
operation | 0.565 | 0.256 | 0.002 | 0.785 | 10.253 |
| Combination of two
or more medical diseases | 0.296 | 0.134 | 0.032 | 1.323 | 4.377 |
| Preventive use of
antimicrobial agents | −0.326 | 0.135 | 0.004 | 0.811 | 6.581 |
| Use of
glucocorticoids | 0.409 | 0.158 | 0.003 | 0.623 | 8.956 |
| Use of
immunosuppressive agents | 0.713 | 0.135 | <0.05 | 2.305 | 21.309 |
Discussion
The concurrent chemo-radiotherapy is the main
clinical treatment method for elderly patients with advanced lung
cancer. However, cancer therapies result in reduced tolerance and
immune capacity in patients (7,8). This
compromised immune capacity resulted in high chances of nosocomial
infection. In addition, lung cancer is usually combined with a
variety of medical diseases. In elderly patients, the organ
dysfunction and decreased immunity made them prone to various
complications (9). The infection is
extremely harmful for patients and could even lead to death.
Previous studies have confirmed that nosocomial infection has
become a serious threat to patients with advanced NSCLC leading to
death (10). Therefore, the infection
in these patients due to long-term chemo-radiotherapy is a
difficult problem for the clinicians to solve. The aim of the
present study was to analyze the characteristics of nosocomial
infection and its impact on the survival of patients with advanced
NSCLC during chemotherapy.
In the present study, pathogens of nosocomial
infection have shown that G− infection is the main type
of infection. Further, the mechanism of the emergency of drug
resistance of Pseudomonas aeruginosa is complex. It could be
explained by the ability of Pseudomonas aeruginosa to
colonize with high variability (11).
While the Klebsiella pneumoniae is a common
extended-spectrum β-lactamases (ESBLs) strain, the gene of
lactamases is the main cause of drug resistance. Klebsiella
pneumoniae could produce lactamases for plasmid binding and
transduction, which led to the emergency of drug resistance
(12). This study found that the
G− Klebsiella pneumoniae and Pseudomonas
aeruginosa were highly sensitive to imipenem and meropenem.
Infection may not be effectively controlled in G−
infected patients with advanced NSCLC but it could lead to serious
consequences. So imipenem or meropenem could be considered for
early treatment of the above patients. G+ infection is
sensitive to vancomycin and teicoplanin. Thus, imipenem or
meropenem could be considered for the early treatment of
G+ infected patients with advanced NSCLC.
The increased causes of respiratory infection may be
due to the special anatomical structure of the respiratory system,
the location of primary lesions and the use of ventilator
treatment. Collectively this made the nosocomial infection
pathogens penetration easier into the body through the respiratory
tract. In addition, urinary tract infection may be related to the
indwelling catheter in patients (13), long-term bed rest, prostatitis in
elderly male patients (14,15) and reproductive system inflammation in
elderly female patients (16,17). Gastrointestinal infections may be
related to toxic side effects of chemotherapy, especially
myelosuppression (18). The
occurrence of nosocomial infections, regardless of the infection
site, severity, affected the quality of life in the form of reduced
body rehabilitation ability and less outdoor activities.
Our study on risk factors related to nosocomial
infection in patients older than 60 years has shown that
self-management ability, immunity capacity, bone marrow
hematopoietic function and nutritional status were gradually
decreased. Especially the combination of more than two kinds of
medical diseases could significantly reduce the body anti-infective
ability. So, toxic effects of radiotherapy and chemotherapy become
more prominent causing increased incidence of nosocomial infection
(19–21). Invasive operation itself is the source
of iatrogenic infection. The implementation of persistent thoracic
drainage on the patients with severe pleural effusion could lead to
the loss of albumin leading to decline in immune capacity.
Prolonged treatment with indwelling drainage and retrograde
injection are other factors responsible for nosocomial infection.
The use of glucocorticoids and immunosuppressive agents could
significantly inhibit the body's immune capacity leading to
nosocomial infection.
In conclusion, G− infection is the
dominant type of nosocomial infection in patients with advanced
NSCLC. G− infection, in respiratory system is sensitive
to imipenem or meropenem and the infection seriously affect the
survival of patients.
References
|
1
|
Takagi Y, Hosomi Y, Oshita F, Okamoto H,
Seki N, Minato K, Aono H, Yamada K, Okuma Y, Hida N, et al:
Feasibility study of docetaxel plus bevacizumab as first line
therapy for elderly patients with advanced non-small-cell lung
cancer: Thoracic Oncology Research Group (TORG) 1014. BMC Cancer.
15:740–750. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kanda S, Horinouchi H, Fujiwara Y,
Nokihara H, Yamamoto N, Sekine I, Kunitoh H, Kubota K, Tamura T and
Ohe Y: Cytotoxic chemotherapy may overcome the development of
acquired resistance to epidermal growth factor receptor tyrosine
kinase inhibitors (EGFR-TKIs) therapy. Lung Cancer. 89:287–293.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen J, Chen J, Ding HY, Pan QS, Hong WD,
Xu G, Yu FY and Wang YM: Use of an artificial neural network to
construct a model of predicting deep fungal infection in lung
cancer patients. Asian Pac J Cancer Prev. 16:5095–5099. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Huang BT, Lu JY, Lin PX, Chen JZ, Kuang Y
and Chen CZ: Comparison of two RapidArc delivery strategies in
stereotactic body radiotherapy of peripheral lung cancer with
flattening filter free beams. PLoS One. 10:e01275012015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kubota K, Sakai H, Katakami N, Nishio M,
Inoue A, Okamoto H, Isobe H, Kunitoh H, Takiguchi Y, Kobayashi K,
et al: Tokyo Cooperative Oncology Group: A randomized phase III
trial of oral S-1 plus cisplatin versus docetaxel plus cisplatin in
Japanese patients with advanced non-small-cell lung cancer:
TCOG0701 CATS trial. Ann Oncol. 26:1401–1408. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhuang X, Herbert JM, Lodhia P, Bradford
J, Turner AM, Newby PM, Thickett D, Naidu U, Blakey D, Barry S, et
al: Identification of novel vascular targets in lung cancer. Br J
Cancer. 112:485–494. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morichika D, Sato-Hisamoto A, Hotta K,
Takata K, Iwaki N, Uchida K, Minami D, Kubo T, Tanimoto M and Kiura
K: Fatal Candida septic shock during systemic chemotherapy in lung
cancer patient receiving corticosteroid replacement therapy for
hypopituitarism: A case report. Jpn J Clin Oncol. 44:501–505. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saito M, Saito W, Kanda A, Ohguro H and
Ishida S: A case of paraneoplastic optic neuropathy and outer
retinitis positive for autoantibodies against collapsin response
mediator protein-5, recoverin, and α-enolase. BMC Ophthalmol.
14:5–10. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gómez MT, Jiménez MF, Aranda JL, Rodríguez
M, Novoa NM and Varela G: The risk of bilobectomy compared with
lobectomy: A retrospective analysis of a series of matched cases
and controls. Eur J Cardiothorac Surg. 46:72–75. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Andreas S, Rittmeyer A, Hinterthaner M and
Huber RM: Smoking cessation in lung cancer-achievable and
effective. Dtsch Arztebl Int. 110:719–724. 2013.PubMed/NCBI
|
|
11
|
Fernández Lorente A, Brooks Acosta S,
Vinageras Neninger E, Alvarez Barroso MC, Brito Wilkinson B, Troche
Concepción M, Martínez Pérez LB, González Viada CE, Diaz Crespo T
and Casacó Parada AR: Effect of blockade of the EGF system on wound
healing in patients vaccinated with CIMAvax® EGF. World
J Surg Oncol. 11:2752013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Goss GD, O'Callaghan C, Lorimer I, Tsao
MS, Masters GA, Jett J, Edelman MJ, Lilenbaum R, Choy H, Khuri F,
et al: Gefitinib versus placebo in completely resected
non-small-cell lung cancer: Results of the NCIC CTG BR19 study. J
Clin Oncol. 31:3320–3326. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Huang YH, Terabe M, Pendleton CD,
Khursigara Stewart D, Bera TK, Pastan I and Berzofsky JA:
Identification and enhancement of HLA-A2.1-restricted CTL epitopes
in a new human cancerantigen-POTE. PLoS One. 8:643–665. 2013.
|
|
14
|
Ai Yang SS, Hsu K, Herbert C, Cheng Z,
Hunt J, Lewis CR and Thomas PS: Mitochondrial DNA mutations in
exhaled breath condensate of patients with lung cancer. Respir Med.
107:911–918. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Noro R, Yoshimura A, Yamamoto K, Miyanaga
A, Mizutani H, Minegishi Y, Seike M, Kubota K, Kosaihira S, Hino M,
et al: East Japan Chesters Group: Alternating chemotherapy with
amrubicin plus cisplatin and weekly administration of irinotecan
plus cisplatin for extensive-stage small cell lung cancer.
Anticancer Res. 33:1117–1123. 2013.PubMed/NCBI
|
|
16
|
Kikuchi R, Isowa N, Tokuyasu H, Kawasaki
Y, Onuma H, Miura H, Terada M, Takada T, Gejyo F, Suzuki E, et al:
Three cases of resected pleomorphic carcinoma. Ann Thorac
Cardiovasc Surg. 16:264–269. 2010.PubMed/NCBI
|
|
17
|
Tanaka J, Tajima S, Ito R, Shimaoka Y,
Kuriyama H, Kagamu H, Terada M, Takada T, Gejyo F, Suzuki E, et al:
Non-small cell lung carcinoma dying of acute respiratory failure
due to aerogenous metastasis. Nihon Kokyuki Gakkai Zasshi.
47:652–657. 2009.(In Japanese). PubMed/NCBI
|
|
18
|
Van Arsdale SA: Chest mass mimicking an
implanted port. Clin J Oncol Nurs. 12:673–674. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wampler GL, Ahlgren JD, Lokich JJ, Gullo
JJ and Phillips JA: Dichloromethotrexate, infusional cisplatin, and
infusional 5-fluorouracil for locally advanced or metastatic
non-small cell lung cancer. A MAOP study. Am J Clin Oncol.
14:442–445. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Belch AR, Urtasun RC, Bodnar D, Kinney B
and Amy R: Use of hemibody irradiation as a non-cross-resistant
agent in combination with systematic chemotherapy in small cell
lung cancer. NCI Monogr. 11:271–274. 1988.
|
|
21
|
Evans WK, Feld R, Murray N, Pater J,
Shelley W, Willan A, Osoba D, Levitt M, Coy P, Hodson I, et al: The
use of VP-16 plus cisplatin during induction chemotherapy for
small-cell lung cancer. Semin Oncol. 13 Suppl 3:10–16.
1986.PubMed/NCBI
|