Introduction
Schwannomas are common intraspinal tumors frequently
observed in the cervical and lumbar regions (1). Spinal schwannomas are slow-growing
lesions that primarily arise from the dorsal sensory roots, leading
to changes in radicular sensory processes that may result in
debilitating effects. Spinal schwannomas are commonly confined to
one side of the spine. Patients commonly present with pain, with
weakness being a less common symptom.
Surgery is currently the primary treatment for
schwannomas and aims to restore neurological function, ambulation
and bladder control, and improve life quality, with two major
surgical approaches used: The posterior midline approach or the
unilateral hemilaminectomy approach (2–9).
The posterior midline approach requires resecting
the muscles, ligaments, spinous processes and part of the lamina.
Clinical biomechanical studies have demonstrated that the posterior
midline approach may cause postoperative spinal instability and
long-lasting back pain, and limit the range of motion due to
ligament and joint damage. In contrast, unilateral hemilaminectomy,
which decreases the damage to the interspinous and supraspinous
ligaments and lamina, may be associated with a decrease in the
severity of these postoperative complications (10,11).
However, surgical vision is restricted within the unilateral spinal
canal and there is limited operative space (7,10).
Currently, the paraspinal tubular retractor system has been
commonly used in spine discectomies. It is minimally invasive to
the paraspinal muscles and the vertebrae, while preserving the
facet joint. Unlike unilateral hemilaminectomy, the paraspinal
tubular retractor system offers a wide surgical area as the tubular
retractor is able to adjust its angle, and provides improved access
for pathological excision, which may be achieved using
non-expandable retractors. In previous studies, lumbar disc
herniations have been treated using the tubular retractor system
(11–14). The present study introduces a novel
surgical approach for lumbar intraspinal schwannomas which was
observed to exhibit good clinical efficacy.
Materials and methods
Inclusion and exclusion criteria
The study described in the present study has been
carried out in accordance with the Code of Ethics of The World
Medical Association (the Declaration of Helsinki) for experiments
involving humans. The present study was approved by, and carried
out according to the Fujian Medical University (Fuzhou, China)
Human Investigations or Ethics Committee protocol. Informed written
consent was obtained for experimentation with all patients. The
privacy rights of the patients were always observed. Two types of
tumor were included in the study. Extramedullary spinal tumors with
the majority of their mass residing unilaterally intraspinal were
confirmed through clinical manifestations and imaging studies.
Small-sized tumors were identified with a threshold transverse
diameter ≤2 cm and a height that was less than or equal to the
height of one vertebra in radial length. A clinical examination was
conducted on all patients who were identified as potentially
possessing schwannomas following review of imaging reports, in
order to confirm the affected spaces.
On the basis of imaging studies, several types of
schwannoma were excluded from the present study. The patients that
required internal fixation following surgical removal were excluded
from the present study.
Patients
A total of 56 patients (24 male and 32 female) who
were admitted to the Affiliated Union Hospital of Fujian Medical
University (Fuzhou, China) between November 2011 and April 2015
qualified for the present study. Patients were undergoing a
microsurgical procedure using a paraspinal keyhole approach with a
tubular retractor system. Pathologies of schwannomas were
retrospectively analyzed. The age of disease onset ranged from 16
to 72 years, with a mean age of 45.6 years. Patients aged between
40 and 50 comprised the largest group of patients (42.86% or 24
cases). Two patients were selected for in depth analysis.
Clinical manifestations
Patients reported a mean disease history of 13.66
months (ranging from 1 to 31 months). Clinical manifestations
varied with location and size of the tumors as well as whether
spinal cord compression was evident (15,16). Early
symptoms included irritation, itchiness, palsy and sense of
expansion. Symptoms associated with cord compression were prominent
in the late phase. Specific distributions of the patients' symptoms
were summarized as follows: 32 cases of radiculalgia, 34 of
paresthesia, 17 of dyskinesia and 4 bowel or bladder dysfunction
cases.
Imaging examinations
All the patients received plain and T1-weighted
magnetic resonance imaging (MRI) and computed tomography (CT). MRI
clearly revealed the shape of tumors and compression-induced
shifting of the spine (17–20). CT scans clearly revealed signs of
foramen expansion, bone destruction and tumor outgrowth (21). MRI, T1-weighted MRI and CT
three-dimensional reconstructions were conducted postoperatively.
T1-weighted MRI and CT scans were used to assess the condition of
tumor resections and the effects of surgery on tumor-induced cord
compressions. CT three-dimensional reconstructions were used to
reveal the effect of surgery on the bony structure of the
vertebrae.
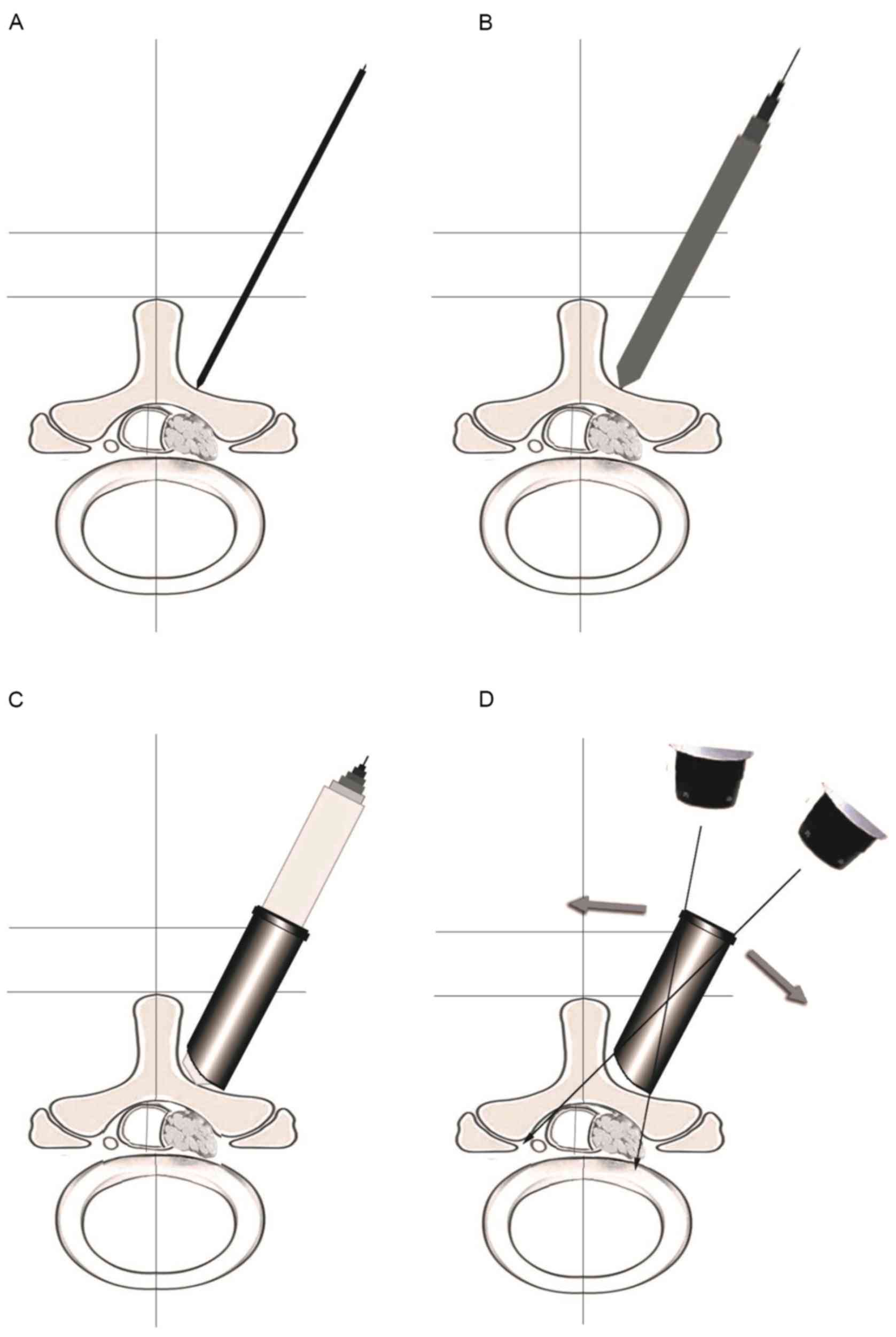
Surgical procedure
Patients received general anesthesia via
endotracheal intubation, while in a prone position and with a
vacant abdomen (on a high-intensity foam pad). Following a detailed
analysis of the tumor location and size based on the preoperative
MRI and CT, the intervertebral space was confirmed. The surgical
approach that would cause the least damage to the paraspinal
muscles and nerve roots was selected following assessment of the
impact of the approach on spinal stability. The location of the
corresponding intervertebral space was marked at the midline using
a paperclip, which indicated the site of incision when X-rayed.
Following preoperative preparation, an incision (1.5–2.0 cm) was
made parallel to the spine at 2.0 cm to the midline of the spinous
process. The incision site may have varied according to the
location, size and the specific position detected by X-rays of the
tumor. A Kirschner wire was inserted into the incision under the
guidance of the C-arm X-ray machine. Blunt dissection was guided
gradually to form a surgical pathway via the multifidus gap using
the tubular retractor system. The surgical pathway was fixated when
it reached the surface of the lamina. The superficial soft tissue
of the lamina and fiavum ligament were bluntly dissected under the
microscope. Part of the lamina was removed using a micro drill to
reveal the spinal dura mater. Tumor resection and nerve
decompression were completed under clear and full vision following
adequate microscopic adjustment (Fig.
1).
Response evaluation criteria
The length of the surgery and any signs of
hemorrhage were evaluated during surgery. Postoperative evaluations
included the length of bed rest, the duration of the hospital stay
and any postoperative complications. Follow-up visits ranged from 6
months to 47 months, with a mean duration of 25.61 months. Several
parameters were measured preoperatively and at 1 week, 3 months and
6 months postsurgery. These parameters included the Japanese
Orthopedic Association (JOA) score, the JOA improvement rate [JOA
postoperative improvement (%) = (postoperative - preoperative JOA
score)/(29 - preoperative JOA score) × 100%] and the visual analog
scale (VAS) score. MRI and CT scans were performed preoperatively,
immediately following surgery and at the 6-month postoperative
visit to confirm the efficacy of the resections and evaluate spinal
stability.
Statistical analysis
Data are expressed as the mean ± standard
deviations. JOA and VAS scores at distinct time periods were
compared using standard and repeated measures analysis of variance;
multiple comparison between the groups was performed using the
S-N-K method. Analyses were performed using SPSS software (version
18.0; SPSS Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Example case reports
Two cases were selected for in-depth analysis.
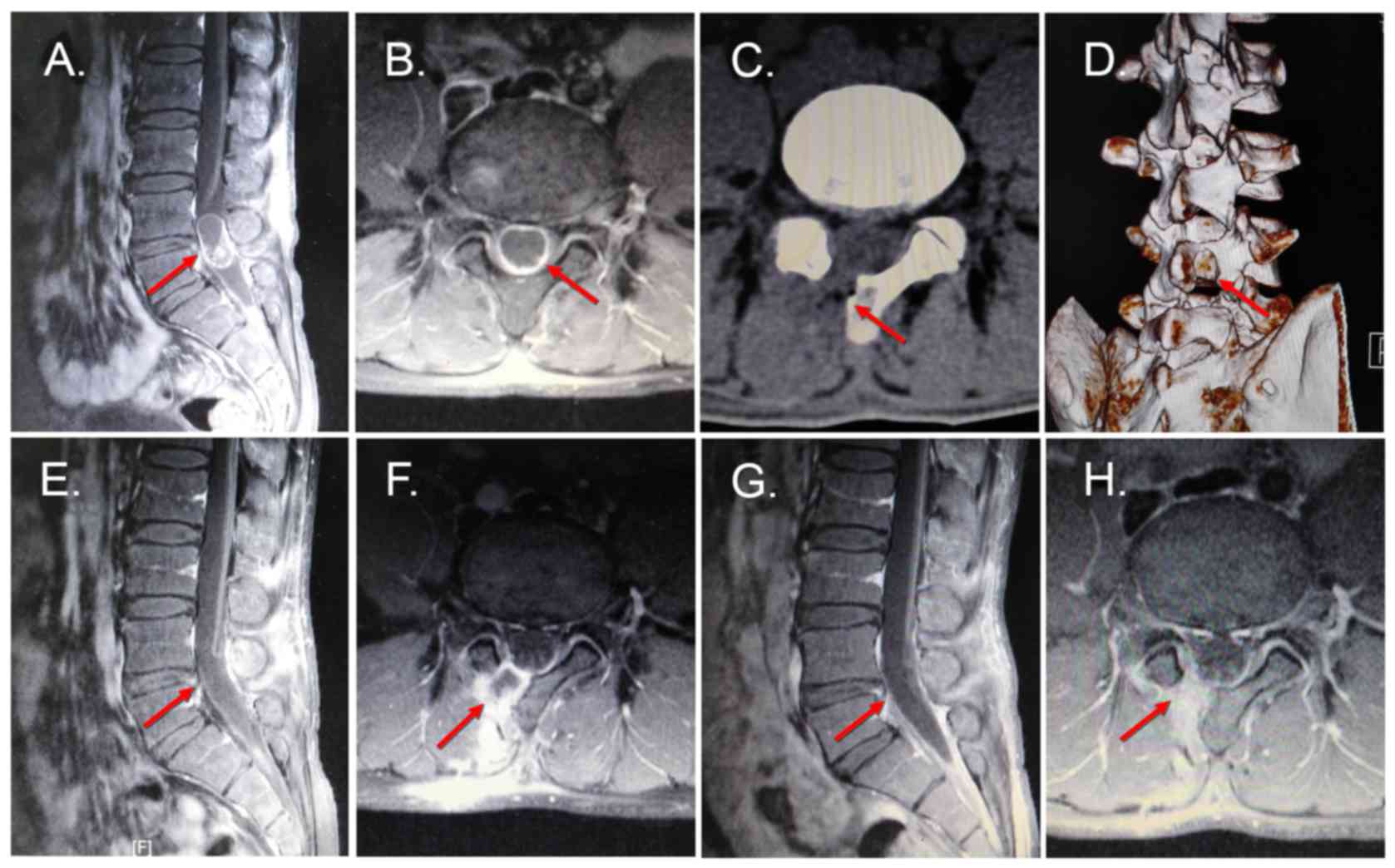
Case I. A 33-year-old male exhibited repeat right leg pain
and numbness for 5 months becoming aggravated over the course of 5
days. The patient reported no symptoms of limb weakness, unsteady
gait or bowel and bladder dysfunctions. The preliminary examination
revealed a negative straight leg raising sign in the bilateral
lower extremities as well as a normal pulse in the bilateral
dorsalis pedis. MRI indicated a space-occupying lesion in the
lumbar 4–5 transpinal canal (2.9×1.6×1.4 cm). The patient underwent
microsurgery using the paraspinal keyhole approach for lumbar
intraspinal extramedullary schwannomas combined with the tubular
retractor system. This approach relieved the pain postoperatively
(Fig. 2).
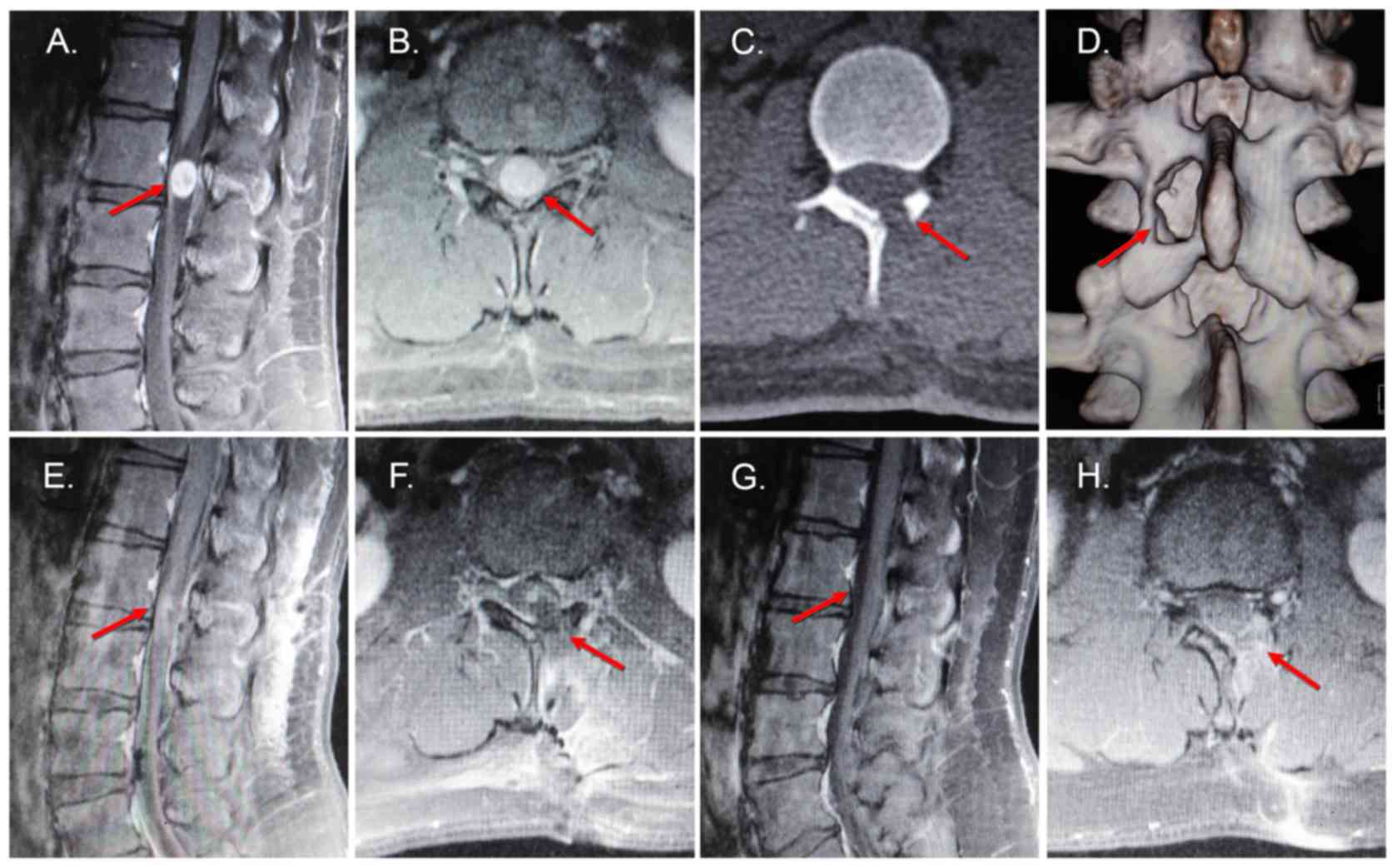
Case II
A 16-year-old male exhibited lower back pain, left
leg pain and numbness for 6 months. No symptoms of limb weakness,
unsteady gait or bowel and bladder dysfunctions were reported. The
preliminary examination revealed a negative straight leg raising
sign in bilateral lower extremities as well as a normal pulse in
the bilateral dorsalis pedis. MRI indicated a space-occupying
lesion in the lumbar 2 transpinal canal (1.5×1.0×0.9 cm). The
patient underwent microsurgery using the paraspinal keyhole
intervention for lumbar intraspinal extramedullary schwannomas
combined with the tubular retractor system. Pain and numbness were
alleviated postoperatively and the pain was eliminated by the
3-month follow-up visit (Fig. 3).
Study results
The operative time ranged between 75 and 126 min,
with a mean time of 96.21 min. Intraoperative hemorrhages ranged
between 25 and 65 ml, with a mean volume of 38.54 ml. No blood
transfusions were performed. Patients concluded bed rest following
a mean of 2.55±0.5 days postoperatively and ambulated with a waist
guard (Table I). The complication
rate was low, with only 2 patients demonstrating cerebrospinal
fluid leakage and 1 patient exhibiting nerve root injury. The
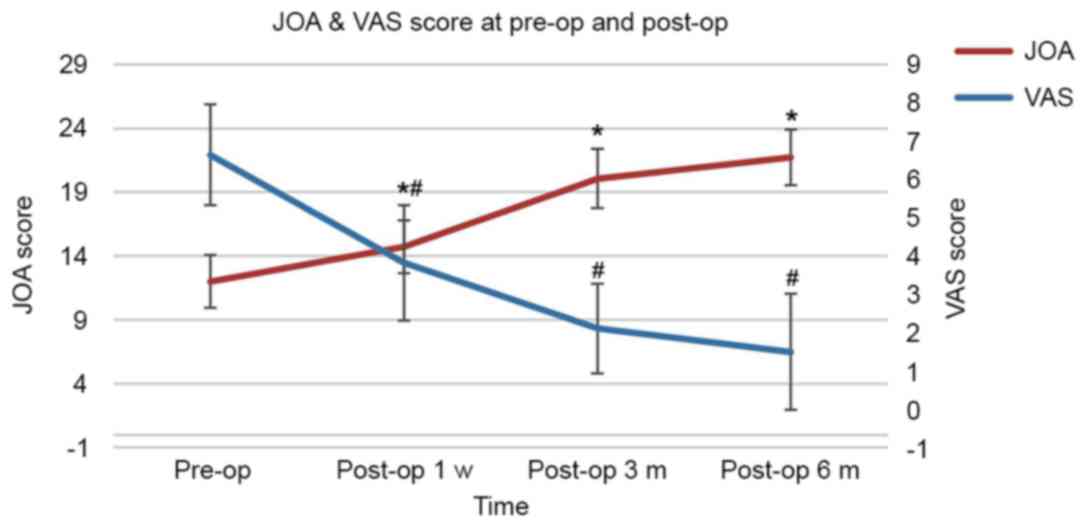
preoperative lumbar JOA scores were 12.00±2.07 and steadily
increased at the 1-week (14.73±2.05), 3-month (20.07±2.32) and
6-month (21.75±2.18) follow-up visits. The rate of improvement in
the JOA scores also increased, with the 1-week (47.8%) and 6-month
(57.35%) postoperative scores increasing over the preoperative
(16.07%) JOA scores (Table II and
Fig. 4). The preoperative VAS score
(6.64±1.31) was higher than the postoperative scores and steadily
declined at 1 week (3.82±1.51), 3 months (2.11±1.17) and 6 months
(1.50±1.51) postsurgery. There was a significant difference between
the preoperative and postoperative data (P<0.05). During the
6-month follow-up, no recurrent tumors appeared in any of the 56
patients. No atrophy was observed in the spinal physiology and
there were no reports of damage induced by paraspinal muscle
injuries.
 | Table I.Surgery results and postoperative
data. |
Table I.
Surgery results and postoperative
data.
| Op time (min) | Intra-op hemorrhage
(ml) | Time in bed
(days) | Length of hospital
stay (days) |
|---|
| 96.21±14.64 | 28.54±9.72 | 2.55±0.5 | 5.68±0.72 |
| Table II.Preoperative and postoperative JOA and
VAS scores. |
Table II.
Preoperative and postoperative JOA and
VAS scores.
| Scores | Pre-op | 1 week post-op | 3 months post-op | 6 months post-op |
|---|
| JOA | 12.00±2.07 |
14.73±2.05a |
20.07±2.32a |
21.75±2.18a |
| JOA improvement
(%) |
| 16.07 | 47.48 | 59.77 |
| VAS | 6.64±1.31 |
3.82±1.51b |
2.11±1.17b |
1.50±1.51b |
Discussion
Intraspinal extramedullary schwannoma is one of the
most common intraspinal tumors (1,22). It is
classified anatomically into extramedullary, paraspinal and
intradural-extramedullary schwannomas, and pathologically into
Schwann cell tumors, neurofibromas and malignant schwannomas. On
the basis of its association with the spinal dura mater,
schwannomas are further classified as subdural-extramedullary,
intradural-extramedullary, extradural, paraspinal and
intramedullary (22). Intraspinal
schwannoma is a slowly developing tumor with insidious onset, which
lacks specific early stage signs and symptoms. The most common
clinical manifestation is radiating pain due to radicular lesions
caused by tumor infiltration. Unfortunately, misdiagnosis is
common. The majority of schwannomas are benign tumors that are
insensitive to chemotherapy, therefore prompt surgical resection
following diagnosis is the optimal solution (22,23).
Total posterior laminectomy combined with tumor
resection is the most common surgical approach for schwannomas.
This method removes the lamina, spinous process, interspinous
ligament and paraspinal soft tissue, completely exposing the
structures inside the spine. The approach enables surgical
manipulation for various types of intraspinal extramedullary
schwannoma in distinct locations (2,3). However,
postoperative complications may include pain, decreased stability
of the spine and cerebrospinal fluid leakage (24). In certain patients, the zygapophyseal
joints are excised, warranting internal fixation and fusion
following tumor resection to decrease the risk of iatrogenic spinal
deformity (25,26). A number of previous studies have
demonstrated that internal fixation and fusion increase the risk of
disc degeneration of the nearby vertebrae (27–30).
Park and Heller (31)
suggested that a surgical approach should cause minimum damage to
the nearby nerves and blood vessels while maximally exposing the
tumors and important structures surrounding them. It was reported
that between 60 and 70% of the intraspinal extramedullary
schwannomas were located laterally or posterolaterally, therefore
removing part of the lamina was also an option (32). Hemilaminectomy preserves the
interspinous and supraspinous ligaments as well as the
intervertebral joints and the unilateral paraspinal muscles. In
addition, this surgical approach maintained the integrity and
stability of the posterior vertebral column and decreased recovery
time, achieving excellent clinical efficacy (4–9).
As microsurgery advances, the tubular retractor
system has been used in microscopic discectomy for prolapsed
intervertebral disc and decompression for spinal stenosis (33–36). In
contrast with traditional open surgery, surgery with a tubular
retractor system significantly decreases the durations of
postoperative bed rest and hospital stays. This approach was
characterized by minimal trauma, less hemorrhage and more rapid
healing (11,37,38). The
Department of Neurosurgery at Union Hospital applied this tubular
retractor system in the treatment of lumbar disc herniations and
spinal stenosis between 2008 and 2010 with high efficacy (39). Considering the feasibility of the
hemilaminectomy approach for surgical removal of the intraspinal
extramedullary tumors as well as the experience gained in the
practice of the tubular retractor system, the paraspinal keyhole
approach was adopted in the present study in microsurgery for
eligible patients with intraspinal extramedullary tumors. The
present retrospective study selected patients with postoperative
pathological reports indicating diagnoses of intraspinal
extramedullary schwannomas.
There are several considerations that should be made
when considering the application of this combined surgical
technique for treatment of intraspinal schwannomas. First, patients
should be placed in a prone position with their abdomens vacant.
This position decreases the spinal vascular pressure and
cerebrospinal fluid, decreases intraoperative hemorrhaging,
facilitates surgical manipulations and avoids intracranial
hypotonic headaches caused by loss of cerebrospinal fluid.
Secondly, the optimal diameter of the pathway should be based on
the location and size of the tumor. A minimal possible pathway
ensures surgical manipulations and adequate depth-of-field of the
microscopic images to decrease muscle and nerve injury.
The present study revealed that the cannula should
be inserted alongside the Kirschner wire following angulation of
the wire by the C-arm X-ray machine. Laterally pulling should be
avoided in blunt dissection to decrease tissue damage. Movement
should be avoided once the pathway is fixated. This may decrease
muscle damage commonly observed when traditional surgical
retractors cause excessive traction. In contrast with dilators,
this method also decreases unnecessary nerve damage or nerve root
irritation caused by movement.
Parts of the tumors were small and located
unilaterally inside the spine and outside the spinal dura mater.
Following wearing down part of the lamina using a micro drill,
tumor resection was completed. For larger tumors, the incision area
of the spinal dura mater exposed the upper and lower poles of the
tumor. Full exposure decreased unnecessary traction and nerve root
irritation during the tumor resection. Dural tenting sutures should
be applied carefully to enable microscopic observation of the
surgical field and to achieve epidural hemostasis.
During the initial surgical process, it was easy to
separate the tumor and spinal cord along the thickened arachnoid
caused by adhesions between the two tissues. As the rate of the
complete tumor resection was high, initial complete resection was
desirable. If a secondary surgical procedure was required for a
large tumor or recurrent tumor (including the presence of a tumor
closely adhering to the spinal cord), suction and
electrocoagulation were utilized for careful ‘peeling’. If the
adhesions were not able to be fully ‘peeled off’, intratumoral
resection may be followed by ‘peeling off’ the tumor capsule.
Adhesions may be carefully separated between the tumor and the
spinal cord or the arachnoid and nerve roots. Intraoperative
manipulation should be gentle and careful. Ineffective manipulation
should be minimized. Traction of the spinal cord should be
performed gently so that irritation of the spinal cord and nerve
root may be avoided. The peritumoral tortuous vessels should be
protected, and the impact of resection and electrocautery on the
function and blood supply of the spine should be minimized.
The dural sac should be carefully sutured following
tumor resection to close the incision and decrease the incidence of
cerebrospinal fluid leakage. The use of an artificial dural patch
for the dural repair following resection of the epidural tumor
close to the nerve roots is recommended. Application of fibrin glue
to the dural repair site prevented cerebrospinal fluid from
leaking, minimized the adhesions between dura mater and the
surrounding tissues, and decreased the difficulty of repeat
surgeries.
Minimally invasive surgery should not be
deliberately performed for larger tumors which did not meet the
inclusion criteria of the present study. Instead, such tumors
should be treated with hemilaminectomy or posterior open
laminectomy on the basis of the characteristics of the tumor for
complete resection.
The mean operative time of the 56 patients in the
present study was 96.21 min. The mean intraoperative hemorrhage was
38.54 ml. After 3 days of bed rest, patients successfully ambulated
with a waist guard. In the 1-month follow-up, 27 patients recovered
their original physical activity and worked normally. In the last
follow-up, MRI images of patients did not reveal residual tumors.
The three-dimensional reconstruction of CT scans indicated complete
vertebral structure without spondylolisthesis or spinal
deformity.
Although the present study demonstrated satisfactory
efficacy in treating lumbar intraspinal extramedullary schwannomas
with the method described, further clinical evidence with a larger
sample size and longer follow-up periods is required to further
support the advantages of this approach. The learning curve in
microneurosurgery is relatively steep (35), therefore surgical skill and experience
are important factors in determining a successful outcome. The
results of the present study indicate that the microsurgical
paraspinal keyhole approach for lumbar intraspinal extramedullary
schwannomas combined with the tubular retractor system, is
feasible. Further evidence is required to exclude the biases caused
by inconsistent micromanipulation of surgeons and individual
differences between the patients.
In conclusion, the results of the present study
suggest that the microsurgical paraspinal keyhole approach with a
tubular retractor system is suitable for lumbar intraspinal
extramedullary schwannomas if the surgical indications and
limitations are fully understood. It is associated with several
advantages including decreased hemorrhaging, decreased hospital
stays and an improved postoperative maintenance of spinal
stability.
References
|
1
|
Gottfried ON, Binning MJ and Schmidt MH:
Surgical approaches to spinal schwannomas. Contemporary
Neurosurgery. 27:1–9. 2005. View Article : Google Scholar
|
|
2
|
McCormick PC: Surgical management of
dumbbell tumors of the cervical spine. Neurosurgery. 38:294–300.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Samii M, Babu RP, Tatagiba M and Sepehrnia
A: Surgical treatment of jugular foramen schwannomas. J Neurosurg.
82:924–932. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chiou SM, Eggert HR, Laborde G and Seeger
W: Microsurgical unilateral approaches for spinal tumour surgery:
Eight years' experience in 256 primary operated patients. Acta
Neurochir (Wien). 100:127–133. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Naganawa T, Miyamoto K, Hosoe H, Suzuki N
and Shimizu K: Hemilaminectomy for removal of extramedullary or
extradural spinal cord tumors: Medium to long-term clinical
outcomes. Yonsei Med J. 52:121–129. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sario-glu AC, Hanci M, Bozkuş H, Kaynar MY
and Kafadar A: Unilateral hemilaminectomy for the removal of the
spinal space-occupying lesions. Minim Invasive Neurosurg. 40:74–77.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chiou SM, Eggert H, Laborde G and Seeger
W: Microsurgical unilateral approaches for spinal tumour surgery:
Eight years' experience in 256 primary operated patients. Acta
Neurochir (Wien). 100:127–133. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Eggert H, Scheremet R, Seeger W and
Gaitzsch J: Unilateral microsurgical approaches to extramedullary
spinal tumours. Operative technique and results. Acta Neurochir
(Wien). 67:245–253. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sridhar K, Ramamurthi R, Vasudevan MC and
Ramamurthi B: Limited unilateral approach for extramedullary spinal
tumours. Br J Neurosurg. 12:430–433. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bertalanffy H, Mitani S, Otani M,
Ichikizaki K and Toya S: Usefulness of hemilaminectomy for
microsurgical management of intraspinal lesions. Keio J Med.
41:76–79. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee GW, Jang SJ, Shin SM, Jang JH and Kim
JD: Clinical and radiological outcomes following microscopic
decompression utilizing tubular retractor or conventional
microscopic decompression in lumbar spinal stenosis with a minimum
of 10-year follow-up. Eur J Orthop Surg Traumatol. 24 Suppl
1:S145–S151. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chotigavanichaya C, Korwutthikulrangsri E,
Suratkarndawadee S, Ruangchainikom M, Watthanaapisith T,
Tanapipatsiri S and Chotivichit A: Minimally invasive lumbar
disectomy with the tubular retractor system: 4–7 years follow-up. J
Med Assoc Thai. 95 Suppl 9:S82–S86. 2012.PubMed/NCBI
|
|
13
|
Kunert P, Kowalczyk P and Marchel A:
Minimally invasive microscopically assisted lumbar discectomy using
the METRx X-Tube system. Neurol Neurochir Pol. 44:554–559.
2010.PubMed/NCBI
|
|
14
|
Lee CK, Park JY and Zhang HY: Minimally
invasive transforaminal lumbar interbody fusion using a single
interbody cage and a tubular retraction system: Technical tips, and
perioperative, radiologic and clinical outcomes. J Korean Neurosurg
Soc. 48:219–224. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schwartz TH and McCormick PC: Spinal cord
tumors in adultsYoumans Neurological Surgery. Winn HR: 4. 5th
edition. pp. 4817–4834. WB Saunders Philadelphia; PA, USA: 2004
|
|
16
|
Devereaux MW: Neck and low back pain. Med
Clin North Am. 87:643–662. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wu G, Ghimire P, Zhu L, Baral A and Su J:
Magnetic resonance imaging characteristics of primary intraspinal
peripheral primitive neuroectodermal tumour. Can Assoc Radiol J.
64:240–245. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Teksam M, Casey SO, Michel E, Benson M and
Truwit CL: Intraspinal epidermoid cyst: Diffusion-weighted MRI.
Neuroradiology. 43:572–574. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kukreja K, Manzano G, Ragheb J and Medina
LS: Differentiation between pediatric spinal arachnoid and
epidermoid-dermoid cysts: Is diffusion-weighted MRI useful? Pediatr
Radiol. 37:556–560. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tang L, Cianfoni A and Imbesi SG:
Diffusion-weighted imaging distinguishes recurrent epidermoid
neoplasm from postoperative arachnoid cyst in the lumbosacral
spine. J Comput Assist Tomogr. 30:507–509. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
McCormick PC, Post KD and Stein BM:
Intradural extramedullary tumors in adults. Neurosurg Clin N Am.
1:591–608. 1990.PubMed/NCBI
|
|
22
|
Dickman C, Fehlings M and Gokaslan ZL:
Spinal Cord and Spinal Column Tumors: Principles and Practice.
Thieme; New York, NY: pp. 7122006
|
|
23
|
Hussein AA, El-Karef E and Hafez M:
Reconstructive surgery in spinal tumours. Eur J Surg Oncol.
272:196–199. 2001. View Article : Google Scholar
|
|
24
|
Seppälä MT, Haltia MJ, Sankila RJ,
Jääskeläinen JE and Heiskanen O: Long-term outcome after removal of
spinal schwannoma: A clinicopathological study of 187 cases. J
Neurosurg. 83:621–626. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sridhar K, Ramamurthi R, Vasudevan MC and
Ramamurthi B: Giant invasive spinal schwannomas: Definition and
surgical management. J Neurosurg. 94 Suppl 2:S210–S215. 2001.
|
|
26
|
Zander T, Rohlmann A, Klöckner C and
Bergmann G: Influence of graded facetectomy and laminectomy on
spinal biomechanics. Eur Spine J. 12:427–434. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wigfield CC, Skrzypiec D, Jackowski A and
Adams MA: Internal stress distribution in cervical intervertebral
discs: The influence of an artificial cervical joint and simulated
anterior interbody fusion. J Spinal Disord Tech. 16:441–449. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sköld C, Tropp H and Berg S: Five-year
follow-up of total disc replacement compared to fusion: A
randomized controlled trial. Eur Spine J. 22:2288–2295. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wei J, Song Y, Sun L and Lv C: Comparison
of artificial total disc replacement versus fusion for lumbar
degenerative disc disease: A meta-analysis of randomized controlled
trials. Int Orthop. 37:1315–1325. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chang UK, Kim DH, Lee MC, Willenberg R,
Kim SH and Lim J: Changes in adjacent-level disc pressure and facet
joint force after cervical arthroplasty compared with cervical
discectomy and fusion. J Neurosurg Spine. 7:33–39. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Park AE and Heller JG: Cervical
laminoplasty: Use of a novel titanium plate to maintain canal
expansion-surgical technique. J Spinal Disord Tech. 17:265–271.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Acioly MA, Carvalho CH, Koerbel A, Heckl
S, Tatagiba M and Gharabaghi A: The role of the trigeminocardiac
reflex in postoperative hearing function in non-vestibular
schwannoma cerebellopontine angle tumors. J Clin Neurosci.
18:237–240. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Palmer S: Use of a tubular retractor
system in microscopic lumbar discectomy: 1 year prospective results
in 135 patients. Neurosurg Focus. 13:E52002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Parikh K, Tomasino A, Knopman J, Boockvar
J and Härtl R: Operative results and learning curve:
Microscope-assisted tubular microsurgery for 1- and 2-level
discectomies and laminectomies. Neurosurg Focus. 25:E142008.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ranjan A and Lath R: Microendoscopic
discectomy for prolapsed lumbar intervertebral disc. Neurol India.
54:190–194. 2006.PubMed/NCBI
|
|
36
|
Yoshimoto M, Takebayashi T, Kawaguchi S,
Tsuda H, Ida K, Wada T, Suzuki D and Yamashita T: Minimally
invasive technique for decompression of lumbar foraminal stenosis
using a spinal microendoscope: Technical note. Minim Invasive
Neurosurg. 54:142–146. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Foley KT, Smith MM and Rampersaud YR:
Microendoscopic approach to far-lateral lumbar disc herniation.
Neurosurg Focus. 7:e51999. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Fessler RG and Khoo LT: Minimally invasive
cervical microendoscopic foraminotomy: An initial clinical
experience. Neurosurgery. 51 Suppl 5:S37–S45. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chunmei Chen, Fenggang Cai, Weiqiang
Zhang, Rui Wang, Yan Chen, Feng Li, et al: The comparison between
paraspinal sleeve approach with posterior midline approach
microsurgical treatment of lumbar disc herniation. Chin J
Neurosurg. 30:677–681. 2014.(In Chinese).
|