Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most
common subtype of non-Hodgkin lymphoma (NHL), constituting up to
40% of all cases globally (1). DLBCL
is a highly heterogeneous disease. The standard front-line therapy
for DLBCL, which includes rituximab plus cyclophosphamide,
doxorubicin, vincristine and prednisone (R-CHOP), has improved the
survival rate of DLBCL patients (2).
However, ~33% of DLBCL patients have relapsed or refractory type of
disease, which was reported by Sehn et al (2) in the province of British Columbia in
2005, and the molecular mechanism underlying DLBCL development
remains to be fully understood (2–4). Although
certain indicators may assist in predicting prognosis in patients
with DLBCL, including the International Prognostic Index (IPI)
score, MYC proto-oncogene, and tumor location (5–7), the
development of novel biomarkers for estimating the efficacy of
therapeutic strategies and prognosis is required.
LAPTM4B exists as two alleles:
LAPTM4B*1 with one 19 bp segment (GenBank accession no.
AY219176) and LAPTM4B*2 with two tandem repeat segments
(GenBank accession no. AY219177) in the 5′ untranslated region of
exon 1 (8). Previous studies have
demonstrated that LAPTM4B polymorphisms were associated with
susceptibility to multiple types of cancer, including lung, breast,
gastric, colon, ovarian and primary liver cancer (9–16), which
suggested that LAPTM4B*2 may be associated with a
significantly increased risk of developing these types of cancer.
LAPTM4B*2 was also associated with poor prognosis in
patients with hepatocellular, lung or endometrial cancer (17–19). To
the best of our knowledge, no study has previously reported on the
association between LAPTM4B polymorphisms and clinical data
on DLBCL. The present study evaluated whether LAPTM4B
polymorphisms were associated with the susceptibility to and
prognosis of DLBCL.
Materials and methods
Patients and control cases
A total of 164 patients with DLBCL were enrolled
(for the overall survival analysis, 35 cases were not included
because of loss to follow up or accepting non first-line therapy),
which included 81 males and 83 females, mean age 53.08 years, with
2 individuals belonging to the LAPTM4B*1/3 genotype. The
diagnosis of the patients was confirmed by the Department of
Pathology (Peking University Cancer Hospital and Institute,
Beijing, China) according to the World Health Organization
classification. Final diagnosis of all patients was confirmed by
pathological assessment at the Beijing Cancer Hospital, Peking
University School of Oncology (Beijing, China), and all cases were
collected between June 2007 and December 2010. The Ann Arbor
staging classification system were used to determine the stage of
these patients (20). The data for
the 350 healthy control cases were quoted from the data of Cheng
et al (12), which included
225 males and 125 females, mean age 49.75 years. The clinical
research protocol of the present study was approved by the
Institutional Review Board (Peking University Cancer Hospital and
Institute). The present study was approved by the Research and
Ethics Committee of Peking University School of Oncology. Each
patient enrolled in the present study provided written informed
consent for participation.
DNA extraction
Blood samples were obtained from all patients with
DLBCL prior to genetic analysis. Genomic DNA was extracted from
peripheral-blood mononuclear cells using a blood genomic DNA
extraction kit according to the manufacturer's protocol (BioTeke
Corporation, Beijing, China). The genomic DNA was subsequently
dissolved in Tris-EDTA buffer and stored at −80°C.
Polymerase chain reaction (PCR)
analysis
The genomic DNA (30 ng/20 µl) was amplified using
GoTaq DNA polymerase (Promega Corporation, Madison, WI, USA) and
primers forward, 5′-GCCGACTAGGGGACTGGCGGA-3′ and reverse,
5′-CGAGAGCTCCGAGCTTCTGCC-3′ which correspond to the 72–92 and
255–275 bp of LAPTM4B, respectively (8). GAPDH was used as the positive internal
control in the present study, with the following primers: Forward,
5′-GTCTGCCCTAATTATCAGGTCCA-3′ and reverse,
5′-CCTGGCTCCTGGCATCTCT-3′. PCR reaction conditions were set using a
thermo cycler (Gene Cycler™; Bio-Rad Laboratories, Inc., Hercules,
CA, USA) as follows: Denaturation at 94°C for 2 min, followed by 35
cycles at 94°C for 30 sec, at 65°C for 30 sec, and at 72°C for 30
sec. The last cycle was followed by auto-extension at 72°C for 7
min. The amplified products were subsequently analyzed using
electrophoresis on a 10% polyacrylamide or 2% agarose gel.
Visualization was performed using GelRed (Biotium, Hayward, CA,
USA). All samples are repeated by two independent PCR analysis.
The DNA fragments were purified using the AxyPrep
DNA Gel Extraction kit according to the manufacturer's protocol
(Axygen Scientific, Inc., Union City, CA, USA). The purified
products were sequenced using an ABI 3730XL Avant Genetic analyzer
(Applied Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA,
USA), according the manufacturer's protocol. The sequences were
subsequently analyzed using Seqman software DNASTAR version 5.2
(DNASTAR Inc., Madison, WI, USA).
Statistical analysis
Statistical analysis was performed using SPSS 16.0
software (SPSS, Inc., Chicago, IL, USA). The χ2 test or
the Fisher's exact test was used to calculate genotype frequency
(including Hardy-Weinberg equilibrium) and other clinical
parametric distributions between DLBCL and control cases.
Unconditional logistic regression analysis models were used to
assess the association, adjusted by age and sex, between different
genotypes and cancer risks.
The clinical characteristics and response rate of
the patients were compared using the χ2 test or the
Fisher's exact test according to the different genotypes. The
association between LAPTM4B gene polymorphism and overall
survival (OS) and disease-free survival (DFS) was evaluated using
Kaplan-Meier curves and the log-rank test. All statistical tests
were two-sided. P<0.05 was considered to indicate a
statistically significant difference.
Results
LAPTM4B genotypes in patients with
DLBCL
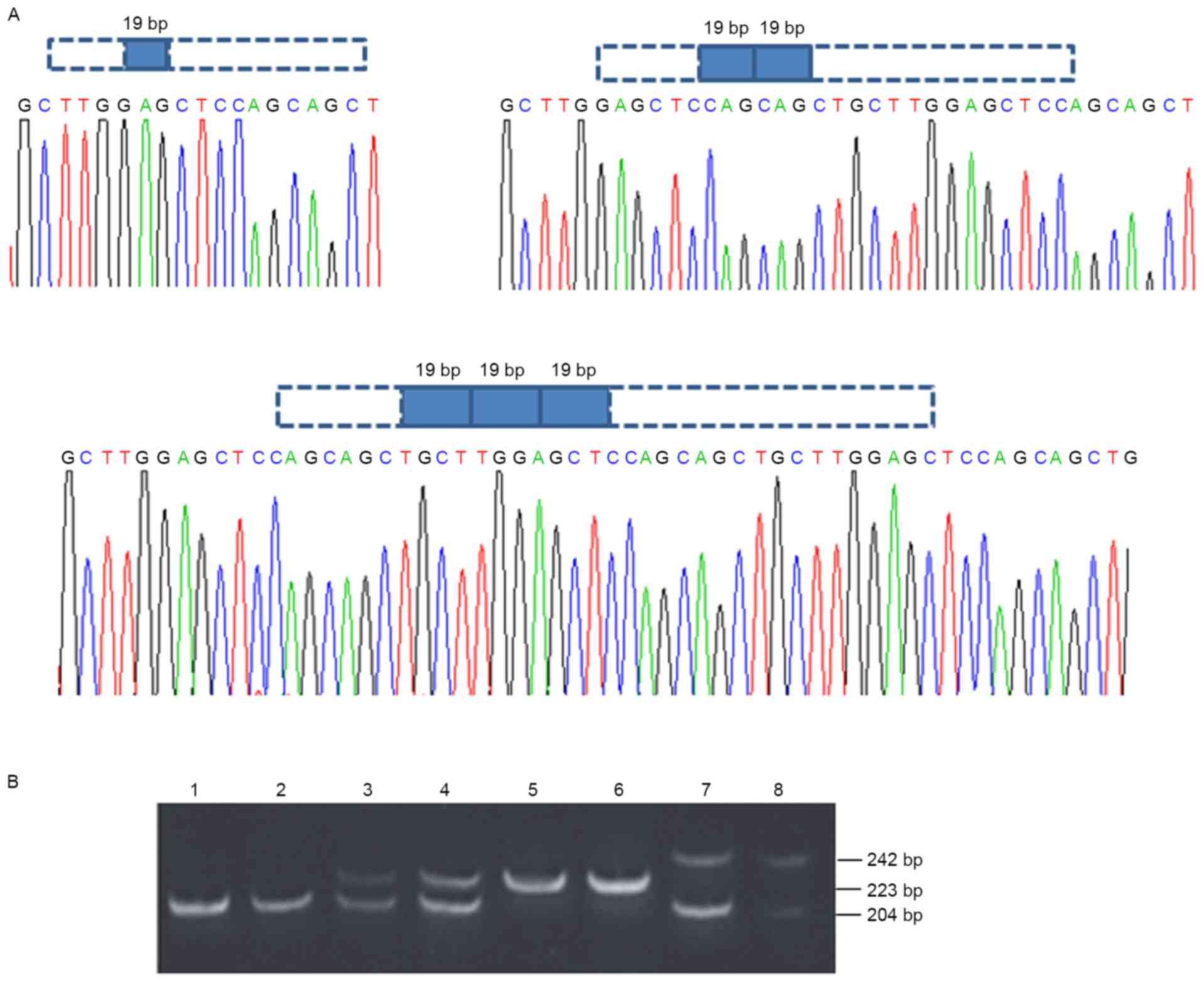
Using PCR analysis, the present study identified
four different LAPTM4B polymorphisms: LAPTM4B*1/1,
LAPTM4B*2/2, LAPTM4B*1/2 and LATPM4B*1/3. As indicated
in Fig. 1, a 204 bp fragment is
encoded by LAPTM4B*1/1, and a 223-bp fragment is encoded by
LAPTM4B*2/2. LAPTM4B*1/2 and LAPTM4B*1/3 are
heterozygous. The 204 bp and 223-bp fragments were both detected in
LAPTM4B*1/2. The 204 and 242 bp fragments were observed in
two individuals with LAPTM4B*1/3.
The present study detected a significant difference
in the distribution of DLBCL between male and female patients
(P<0.002; Table I). No significant
differences in allele frequency were identified between the DLBCL
and control cases (Table II). In the
350 controls, the frequency of the LAPTM4B*2 allele was
24.1%, whereas the frequency in patients with DLBCL was 26.5%.
 | Table I.Distribution of age and sex in
control and DLBCL cases. |
Table I.
Distribution of age and sex in
control and DLBCL cases.
| Characteristic | Control cases, n
(n=350) | DLBCL cases, n
(n=162) |
P-valuea |
|---|
| Age |
|
| 0.732 |
|
≤50 | 165 | 79 |
|
|
>50 | 185 | 83 |
|
| Sex |
|
| 0.002 |
|
Male | 225 | 81 |
|
|
Female | 125 | 81 |
|
| Table II.Distribution of LAPTM4B
alleles in controls (n=350) and DLBCL cases (n=162). |
Table II.
Distribution of LAPTM4B
alleles in controls (n=350) and DLBCL cases (n=162).
| Alleles | Controls, n
(%) | DLBCL cases, n
(%) | OR (95%
CI)a |
|---|
|
LAPTM4B*1 | 531 (75.9) | 238 (73.5) |
|
|
LAPTM4B*2 | 169 (24.1) | 86
(26.5) | 1.175
(0.866–1.596) |
The distribution of LAPTM4B genotypes in
control and DLBCL cases are displayed in Table III. The genotype frequencies for the
polymorphism were in agreement with the Hardy-Weinberg equilibrium
(P=0.898). No significant differences in the distribution of
LAPTM4B*1/2 and LAPTM4B*2/2 genotypes when compared
with LATPM4B*1/1 were detected between the DLBCL and control
cases (P=0.462 and P=0.368, respectively). The odds ratios of
LATPM4B*1/2 and LATPM4B*2/2 genotypes in patients
with DLBCL compared with patients with LATPM4B*1/1 is
1.160-fold (95% CI=0.781–1.724) and 1.446-fold (95%
CI=0.648–3.227), respectively.
| Table III.Distribution of LAPTM4B
genotypes in controls (n=350) and DLBCL cases (n=162). |
Table III.
Distribution of LAPTM4B
genotypes in controls (n=350) and DLBCL cases (n=162).
| Genotypes | Controls, n
(%) | DLBC cases, n
(%) |
P-valuea | OR (95% CI) |
|---|
|
LAPTM4B*1/1 | 199 (56.9) | 87 (53.7) |
|
|
|
LAPTM4B*1/2 | 133 (38.0) | 64 (39.5) | 0.462 | 1.160
(0.781–1.724) |
|
LAPTM4B*2/2 | 18 (5.1) | 11 (6.8) | 0.368 | 1.446
(0.648–3.227) |
LAPTM4B genotypes and
clinicopathological parameters in DLBCL
The present study also assessed the distribution of
clinical parameters, including age and sex, among different
LAPTM4B genotypes in patients with DLBCL (Table IV). There were no statistically
significant associations between the genotype distribution of
LAPTM4B in patients with DLBCL and clinicopathological
parameters (Table IV).
| Table IV.Association between the distribution
of LAPTM4B genotypes and clinicopathological parameters in
DLBCL cases. |
Table IV.
Association between the distribution
of LAPTM4B genotypes and clinicopathological parameters in
DLBCL cases.
|
| LAPTM4B
genotypes |
|
|---|
|
|
|
|
|---|
| Parameters | *1/1 | *1/2 | *2/2 |
P-valuea |
|---|
| Sex |
|
Male | 43 | 31 | 7 | 0.64 |
|
Female | 44 | 33 | 4 |
|
| Age |
|
≤50 | 46 | 29 | 4 | 0.456 |
|
>50 | 41 | 35 | 7 |
|
| B
symptomsb |
|
Positive | 36 | 21 | 5 | 0.494 |
|
Negative | 51 | 43 | 6 |
|
| LDH |
|
Positive | 45 | 37 | 4 | 0.392 |
|
Negative | 42 | 27 | 7 |
|
|
β2-MG |
|
Positive | 23 | 19 | 5 | 0.532 |
|
Negative | 58 | 42 | 6 |
|
| Stage |
|
I–II | 40 | 31 | 4 | 0.757 |
|
III–IV | 47 | 33 | 7 |
|
| Bulky mass |
| ≥10
cm | 9 | 7 | 2 | 0.766 |
| <10
cm | 78 | 57 | 9 |
|
| Localized |
|
Yes | 13 | 10 | 2 | 0.961 |
| No | 74 | 54 | 9 |
|
| No extra
nodalc |
| ≤1 | 68 | 46 | 7 | 0.474 |
|
>1 | 19 | 18 | 4 |
|
| Incidence site |
| Lymph
node | 50 | 36 | 6 | 0.977 |
| Extra
lymph | 37 | 28 | 5 |
|
| IPI score |
|
0–2 | 66 | 43 | 5 | 0.102 |
|
3–5 | 21 | 21 | 6 |
|
| Molecular
subtypes |
|
GCB | 12 | 16 | 0 | 0.102 |
|
Non-GCB | 61 | 41 | 9 |
|
|
Other | 14 | 7 | 2 |
|
Associations between LATPM4B genotypes
and prognosis of patients with DLBCL
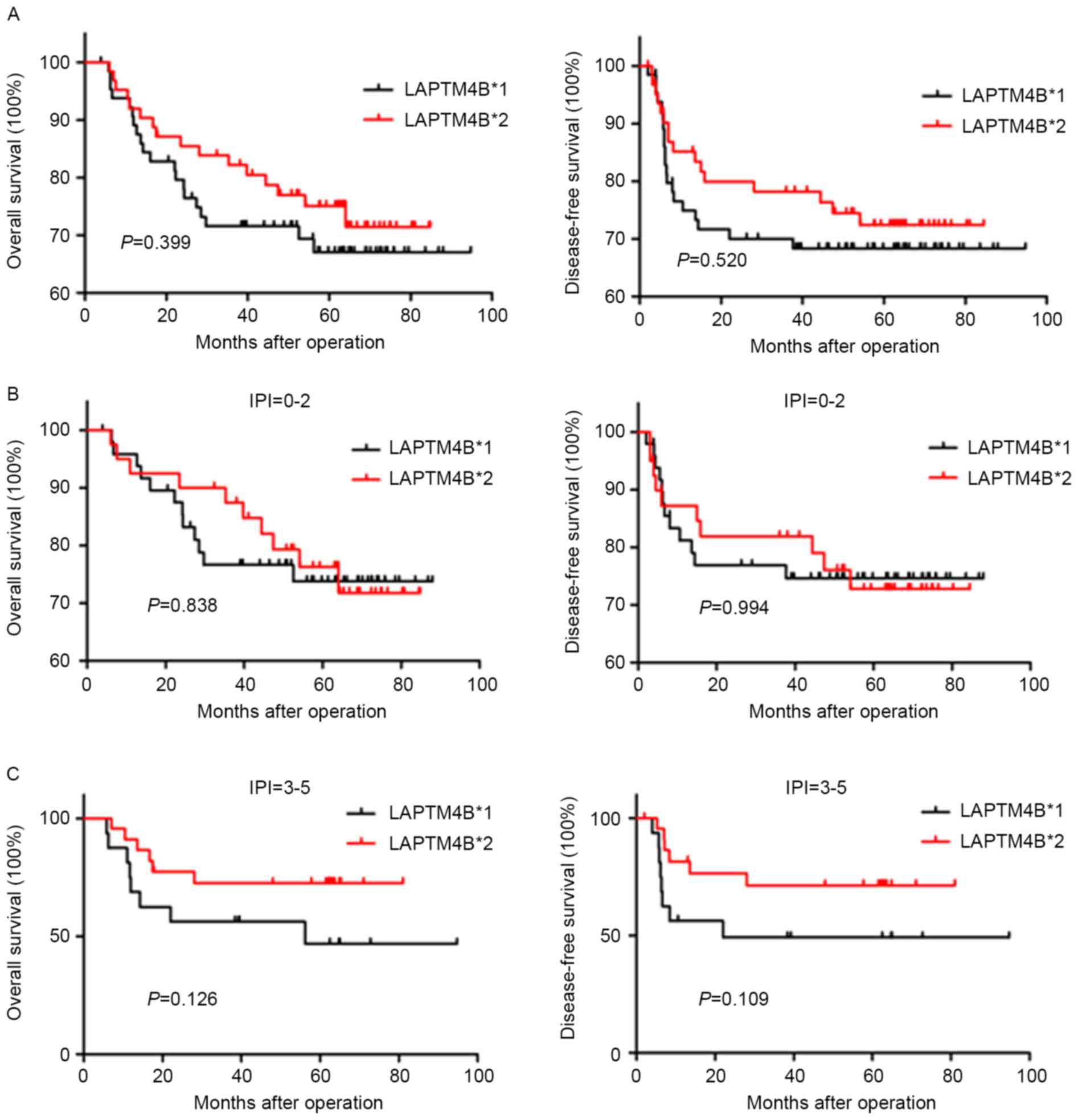
In the present study, follow-up data ranging from
3.9–94.8 months (mean, 50.5 months) was obtained for 129 patients
with DLBCL. At the end date of the follow-up, a total of 93
patients survived and 36 succumbed to disease. Survival analysis
was conducted in the 129 patients to examine the effect of
LATPM4B polymorphism on the prognosis of patients with
DLBCL. Kaplan-Meier analysis and log-rank test indicated that
LAPTM4B*2 was not associated with decreased OS and
DFS (P=0.399 and P=0.520, respectively). However, patients with the
LAPTM4B*2 genotype and IPI score 3–5 (n=40) tend to exhibit
longer durations of OS and DFS compared with patients with the
LAPTM4B*1 genotype (P=0.126 and 0.109, respectively;
Fig. 2).
Discussion
The present study demonstrated that the presence of
the LAPTM4B*2 allele was not associated with a
markedly increased risk of developing DLBCL compared with
LAPTM4B*1. However, in patients with IPI score 3–5, a
significantly increased risk of developing DLBCL was identified in
patients with the LAPTM4B*2/2 genotype compared with those
that exhibited the LAPTM4B*1/1 genotype. A total of three
tandem repeats comprising 19 bp segments were detected in 2/164 of
the patients with DLBCL. Furthermore, patients with DLBCL that
exhibited LAPTM4B*2 had a tendency to have increased
durations of OS and DFS compared with those with LAPTM4B*1,
particularly those that also exhibited IPI score 3–5. To the best
of our knowledge, the present study is the first to demonstrate,
albeit not statistically, that LAPTM4B*2 is a more useful
prognostic indicator for DLBCL compared with LAPTM4B*1.
However, this finding is not consistent with the results of
previous studies, including those assessing hepatocellular
carcinoma, lung and breast cancer (17,18,21).
LAPTM4B has two known protein isoforms: LAPTM4B-24
(226 aa) and LAPTM4B-35 (317 aa) (22). Previous studies have indicated that
LAPTM4B-35 is able to activate the binding of phosphoinositide
3-kinase (PI3K)/protein kinase B (Akt) to p85α subunits, and
thereby facilitate cancer cell multidrug resistance and inhibit
apoptosis (23). Liu et al
(22,24) used a polyclonal antibody to
demonstrate that LAPTM4B-35 and LAPTM4B-24 may differ in expression
and function in tissues and multiple cell lines of hepatocellular
carcinoma. The balance of LAPTM4B-35 and LAPTM4B-24 may affect
malignant transformation. Multiple studies have revealed that
LAPTM4B-35 may participate in malignant transformation and tumor
invasion (25–28). However, a recent report demonstrated
that the LAPTM4B-24 isoform was able to stimulate mechanistic
target of rapamycin complex (mTORC)1 through vacuolar-type
H+-ATPase via the influx of leucine resulting from the
binding of LAT1-4F2hc to lysosomes (29). LAPTM4B-24 may also promote cell growth
and proliferation and regulate immune responses by decreasing
transforming growth factor β1 production in human regulatory T
cells (29,30).
Although as aforementioned there are two known
isoforms of LAPTM4B, the present study suggested that another
isoform may exist due to the LAPTM4B*2 allele. The 19 bp
difference in the first exon of LAPTM4B between LAPTM4B*1
and LAPTM4B*2 may alter the open reading frame, thereby
resulting in two different protein isoforms: LAPTM4B-35 and
LAPTM4B-40 (8,17). Previous studies have demonstrated that
LAPTM4B polymorphisms were associated with an increased risk of
multiple types of cancer, including ovarian, breast and gallbladder
cancer (13,31,32). These
findings suggest that the 19 bp sequence may serve an important
function in transcriptional regulation, or a different protein
isoform encoded by LAPTM4B*2 may affect cancer cell function
(8). Yang et al (17) indicated that LAPTM4B*2 was
associated with tumor recurrence and poor histopathological
differentiation, and is an independent prognostic factor in
hepatocellular carcinoma. Other studies have reported similar
results for lung cancer, and endometrial and gallbladder carcinoma
(18,19,32).
In the present study, the LAPTM4B*2 allele
was not associated with a significantly increased risk of
developing DLBCL, and there was no significant association with
survival in patients with DLBCL. However, there was a tendency for
patients with LAPTM4B*2 to have improved OS and DFS compared
with patients with LAPTM4B*1 in DLBCL, and this pattern was
more evident in cases with IPI score 3–5.
The 19 bp sequence may serve a crucial role in
transcriptional regulation, including binding with transcription
factors, microRNAs or non-coding linker RNA in patients with DLBCL,
which discriminates its function with that of other types of
cancer, including hepatocellular carcinoma (15,17).
Therefore, the different LAPTM4B protein isoforms may have diverse
functions in patients with LAPTM4B*2 compared with those
with LAPTM4B*1 in DLBCL. The results of the present study on
LAPTM4B alleles in patients with DLBCL may provide
additional evidence that different LAPTM4B protein isoforms could
serve multiple functions. For example, it was previously reported
that LAPTM4B-35 may activate the PI3 K/Akt signaling pathway, and
LAPTM4B-24 may activate mTORC1 (23,29).
Identifying the isoform that predominates in the induction of the
19 bp sequence in various types of cancer should be investigated in
further studies.
The present study assessed the association between
LAPTM4B polymorphisms and prognosis of patients with DLBCL.
It was indicated that LAPTM4B*2 may be a more useful
prognostic indicator for DLBCL compared with
LAPTM4B*1, particularly in cases with IPI score 3–5
compared with IPI score 0–2 (although this trend was not
statistically significant). IPI is a crucial indicator for
selecting the appropriate therapeutic strategies in DLBCL. In
DLBCL, patients with IPI score 0–2 have good prognosis with the
rate of 5-year survival reaching 80% (33). In the present study, the lack of
association between LAPTM4B*2 allele and survival of
patients with IPI score 0–2 may be due to the small number of cases
in the present study. However, there is a poor rate of 5-year
survival (<50%) following the standard R-CHOP treatment in
patients with IPI score 3–5 (33).
LAPTM4B*2 allele may be a good indicator for patients with
IPI score 3–5 and may be used to guide clinical therapy to reduce
unnecessary drug treatment.
Acknowledgements
The present study was supported by National Natural
Science Foundation of China (grant no. 81470368) and the Beijing
Natural Science Foundation (grant no. 7152030).
References
|
1
|
International Agency for Research on
Cancer, . World Cancer Report 2014. http://publications.iarc.fr/Non-Series-Publications/World-Cancer-Reports/World-Cancer-Report-2014July.
2014
|
|
2
|
Sehn LH, Donaldson J, Chhanabhai M,
Fitzgerald C, Gill K, Klasa R, MacPherson N, O'Reilly S, Spinelli
JJ, Sutherland J, et al: Introduction of combined CHOP plus
rituximab therapy dramatically improved outcome of diffuse large
B-cell lymphoma in British Columbia. J Clin Oncol. 23:5027–5033.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Perry AR and Goldstone AH: High-dose
therapy for diffuse large-cell lymphoma in first remission. Ann
Oncol. 9 Suppl 1:S9–S14. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fisher RL, Gaynor ER, Dahlberg S, Oken MM,
Grogan TM, Mize EM, Glick JH, Coltman CA Jr and Miller TP:
Comparison of a standard regimen (CHOP) with three intensive
chemotherapy regimens for advanced non-Hodgkin's lymphoma. N Engl J
Med. 328:1002–1006. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
International Non-Hodgkin's Lymphoma
Prognostic Factors Project: A predictive model for aggressive
non-Hodgkin's lymphoma. N Engl J Med. 329:987–994. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ruzinova MB, Caron T and Rodig SJ: Altered
subcellular localization of c-Myc protein identifies aggressive
B-cell lymphomas harboring a c-MYC translocation. Am J Surg Pathol.
34:882–891. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhou Z, Sehn LH, Rademaker AW, Gordon LI,
Lacasce AS, Crosby-Thompson A, Vanderplas A, Zelenetz AD, Abel GA,
Rodriguez MA, et al: An enhanced International Prognostic Index
(NCCN-IPI) for patients with diffuse large B-cell lymphoma treated
in the rituximab era. Blood. 123:837–842. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shao GZ, Zhou RL, Zhang QY, Zhang Y, Liu
JJ, Rui JA, Wei X and Ye DX: Molecular cloning and characterization
of LAPTM4B, a novel gene unregulated in hepatocellular carcinoma.
Oncogene. 22:5060–5069. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Deng LJ, Zhang QY, Liu B and Zhou RL:
Relationship between LAPTM4B gene polymorphism and susceptibility
of lung cancer. Beijing Da Xue Xue Bao. 37:302–505. 2005.(In
Chinese). PubMed/NCBI
|
|
10
|
Fan M, Liu Y, Zhou R and Zhang Q:
Association of LAPTM4B gene polymorphism with breast cancer
susceptibility. Cancer Epidemiol. 36:364–368. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu Y, Zhang QY, Qian N and Zhou RL:
Relationship between LAPTM4B gene polymorphism and susceptibility
of gastric cancer. Ann Oncol. 18:311–316. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cheng XJ, Xu W, Zhang QY and Zhou RL:
Relationship between LAPTM4B gene polymorphism and susceptibility
of colorectal and esophageal cancers. Ann Oncol. 19:527–532. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xu Y, Liu Y, Zhou R, Meng F, Gao Y, Yang
S, Li X, Yang M and Lou G: LAPTM4B polymorphisms is associated with
ovarian cancer susceptibility and its prognosis. Jpn J Clin Oncol.
42:413–419. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li C, Zhou Q, Wang Y, Chen X, Yang X and
Zhu D: Relationship between LAPTM4B gene polymorphism and
susceptibility of lung cancer. Zhongguo Fei Ai Za Zhi. 9:109–112.
2006.(In Chinese). PubMed/NCBI
|
|
15
|
Wang S, Zhang QY and Zhou RL: Relationship
between LAPTM4B gene polymorphism and susceptibility of primary
liver cancer. Ann Oncol. 23:1864–1869. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang B, Xu J, Zhou R and Zhang Q:
Association of LAPTM4B gene polymorphism with nasopharyngeal
carcinoma susceptibility in a Chinese population. Med Oncol.
30:4702013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang H, Zhai G, Ji X, Xiong F, Su J and
McNutt MA: LAPTM4B allele *2 is a marker of poor prognosis
following hepatic tumor resection for hepatocellular carcinoma.
PLoS One. 7:e349842012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tang H, Tian H, Yue W, Li L, Li S, Gao C,
Si L, Qi L, Lu M and Hu W: LAPTM4B polymorphism is associated with
non-small cell lung cancer susceptibility and prognosis. Oncol Rep.
31:2454–2460. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Meng F, Li H, Zhou R, Luo C, Hu Y and Lou
G: LAPTM4B gene polymorphism and endometrial carcinoma risk and
prognosis. Biomarkers. 18:136–43. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Narayanan S and Savage KJ: Staging and
prognostic factorsNon-Hodgkin Lymphomas. Armitage JO, Mauch PM,
Harris NL, Coiffier B and Dalla-Favera R: 2nd. Lippincott Williams
& Wilkins; Philadelphia, PA: pp. 149–171. 2010
|
|
21
|
Li X, Kong X, Chen X, Zhang N, Jiang L, Ma
T and Yang Q: LAPTM4B allele *2 is associated with breast cancer
susceptibility and prognosis. PLoS One. 7:e449162012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liu XR, Zhou RL, Zhang QY, Zhang Y, Jin
YY, Lin M, Rui JA and Ye DX: Structure analysis and expressions of
a novel tetratransmembrane protein, lysosoma-associated protein
transmembrane 4 beta associated with hepatocellular carcinoma.
World J Gastroenterol. 10:1555–1559. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li L, Wei XH, Pan YP, Li HC, Yang H, He
QH, Pang Y, Shan Y, Xiong FX, Shao GZ and Zhou RL: LAPTM4B: A novel
cancer-associated gene motivates multidrug resistance through
efflux and activating PI3K/AKT signaling. Oncogene. 29:5785–5795.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu X, Zhou R, Zhang Q, Zhang Y, Shao G,
Jin Y, Zhang S, Lin M, Rui J and Ye D: Identification and
characterization of LAPTM4B encoded by a human hepatocellular
carcinoma-associated novel gene. Beijing Da Xue Xue Bao.
35:340–347. 2003.(In Chinese). PubMed/NCBI
|
|
25
|
He J, Shao G and Zhou R: Effects of the
novel gene, LAPTM4B, highly expression in hepatocellular carcinoma
on cell proliferation and tumorigenesis of NIH3T3 cells. Beijing Da
Xue Xue Bao. 35:348–352. 2003.(In Chinese). PubMed/NCBI
|
|
26
|
Yang H, Xiong F, Wei X, Yang Y, McNutt MA
and Zhou R: Overexpression of LAPTM4B-35 promotes growth and
metastasis of hepatocellular carcinoma in vitro and in vivo. Cancer
Lett. 294:236–244. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhou L, He XD, Yu JC, Zhou RL, Shan Y and
Rui JA: Overexpression of LAPTM4B-35 attenuates epirubucin-induced
apoptosis of gallbladder carcinoma GBC-SD cells. Surgery.
150:25–31. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shao GZ, Zhou RL, Zhang QY, Zhang Y, Liu
JJ, Rui JA, Wei X and Ye DX: Molecular cloning and characterization
of LAPTM4B, a novel gene upregulated in hepatocellular carcinoma.
Oncogene. 22:5060–5069. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Milkereit R, Persaud A, Vanoaica L, Guetg
A, Verrey F and Rotin D: LAPTM4b recruits the LAT1-4F2hc Leu
transporter to lysosomes and promotes mTORC1 activation. Nat
Commun. 6:72502015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Huygens C, Lienart S, Dedobbeleer O,
Stockis J, Gauthy E, Coulie PG and Lucas S: Lysosomal-associated
Transmembrane Protein 4B (LAPTM4B) Decreases Transforming Growth
Factor β1 (TGF-β1) Production in Human Regulatory T Cells. J Biol
Chem. 290:20105–20116. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Xiao M, Jia S, Wang H, Wang J, Huang Y and
Li Z: Overexpression of LAPTM4B: An independent prognostic marker
in breast cancer. J Cancer Res Clin Oncol. 139:661–667. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhai G, Yan K, Ji X, Xu W, Yang J, Xiong
F, Su J, McNutt MA and Yang H: LAPTM4B allele *2 is a marker of
poor prognosis for gallbladder carcinoma. PLoS One. 7:e452902012.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sehn LH, Berry B, Chhanabhai M, Fitzgerald
C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J,
et al: The revised international prognostic index (R-IPI) is a
better predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007. View Article : Google Scholar : PubMed/NCBI
|