Introduction
Lung cancer is a common malignant tumor, whose
incidence and mortality rate show sharp upward trends (1,2). In China,
morbidity and mortality rates of lung cancer exhibit an obvious
increasing trend. Lung cancer has become the leading cause of
mortality compared to other cancer types, and the mortality rate
has been increased by 75.77% compared with that in the 1990s
(3).
In previous years, with the continuous development
of thoracoscopic surgery techniques and equipment, thoracoscopic
surgery for the radical treatment of lung cancer has drawn
increasing attention from clinicians. Thoracoscopic surgery has
been widely used in clinical treatment because of small operation
wound and rapid postoperative recovery, which provides surgical
opportunity for elderly patients with poor cardiopulmonary function
(4). Previous findings showed that
plasma D-dimer is the sign of hypercoagulability and fiber
coagulation hyperfunction state. It also has important significance
for clinical diagnosis, prognosis and staging of lung cancer
(5,6).
In addition, researchers have begun to focus on the relationship
between serum D-dimer level and different surgical methods
(thoracoscopy or thoracotomy) (7). In
the present study, the feasibility and safety of thoracoscopic
surgery for lung cancer were evaluated by retrospective analyses,
comparisons of intraoperative and postoperative cases of
thoracoscopic surgery and traditional thoracotomy for lung
cancer.
Materials and methods
General materials
Patients with lung cancer treated in the Department
of Thoracic Surgery of Ningbo No. 2 Hospital (Zhejiang, China) from
January 1, 2013 to December 31, 2016, were retrospectively
analyzed. The study was approved by the Ethics Committee of Ningbo
No. 2 Hospital and informed consents was signed by the patients.
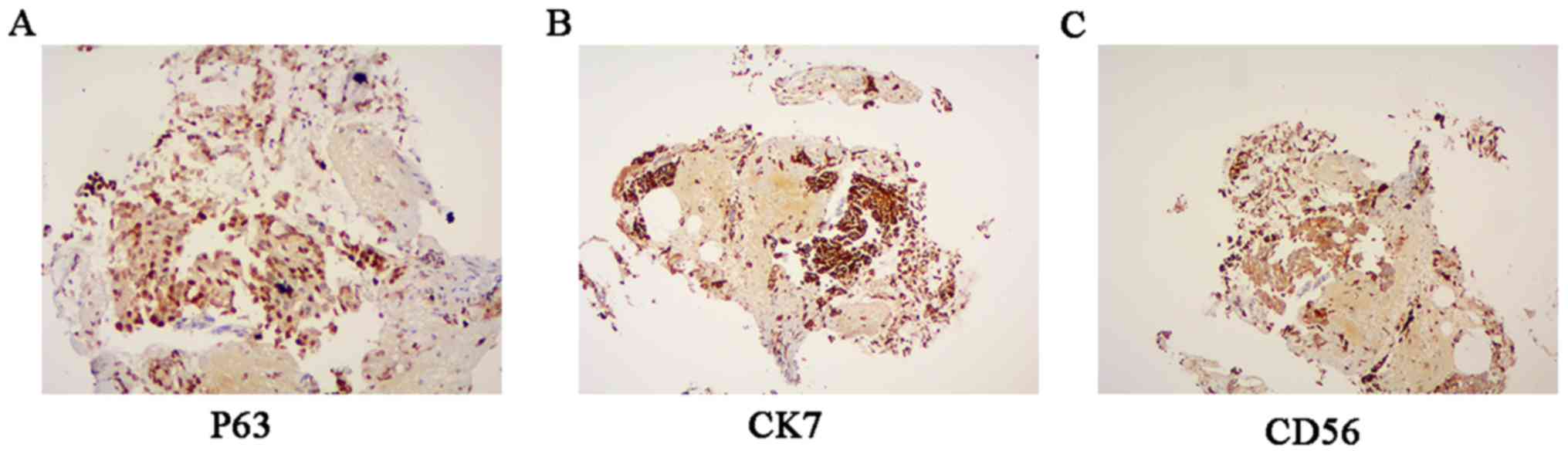
Inclusion criteria for the study were: i) Patients receiving
radical surgery for lung cancer and pathologically diagnosed with
lung cancer. Immunohistochemical images for lung squamous cell
carcinoma, adenocarcinoma and small cell carcinoma are shown in
Fig. 1A-C, respectively; ii) male or
female patients aged 18–70 years; iii) patients whose heart, brain,
lung, kidney and other visceral organs functions were well before
operation, and who could tolerate operations; iv) patients with no
malignant arrhythmia, thyroid dysfunction or past histories; v)
patients receiving thoracoscopic surgery who would not choose
thoracotomy at the midterm of thoracoscopic surgery or change
surgical methods during operation; and vi) patients who did not
take anticoagulants recently. A total of 218 patients were included
in the study, and divided into the thoracoscopy (n=98) and
thoracotomy (n=120) groups according to the different surgical
methods. The baseline data of the two groups of patients were
compared, and the differences were not statistically significant
(P>0.05) (Table I).
 | Table I.Comparisons of clinical data of
patients between the thoracotomy and the thoracoscopy groups. |
Table I.
Comparisons of clinical data of
patients between the thoracotomy and the thoracoscopy groups.
| General data | Thoracotomy group
(n=120) | Thoracoscopy group
(n=98) |
χ2/t/Z | P-value |
|---|
| Age (years) | 55.63±8.01 | 56.04±6.92 | 0.792 | 0.473 |
| Sex |
|
|
|
|
| M/F | 68/52 | 52/46 | 0.280 | 0.590 |
| Clinical symptoms, n
(%) |
|
|
|
|
|
Cough | 53 (44.17) | 45 (45.92) | 0.067 | 0.796 |
|
Expectoration | 20 (16.67) | 10 (10.20) | 2.730 | 0.099 |
|
Hemoptysis | 32 (26.67) | 24 (24.49) | 0.134 | 0.714 |
| Chest
distress | 12 (10.00) | 7 (7.14) | 0.554 | 0.457 |
|
Emaciation | 33 (27.50) | 28 (28.57) | 0.031 | 0.861 |
|
Pyrexia | 17 (14.17) | 11 (11.22) | 0.417 | 0.518 |
| No
symptom | 20 (16.67) | 16 (16.33) | 0.005 | 0.946 |
| Past history, n
(%) |
|
|
|
|
|
Smoking | 82 (68.33) | 60 (61.22) | 1.200 | 0.273 |
|
Hypertension | 23 (19.17) | 16 (16.33) | 0.296 | 0.586 |
|
Diabetes | 32 (26.67) | 21 (21.43) | 0.804 | 0.370 |
| COPD | 34 (28.33) | 19 (19.39) | 2.346 | 0.126 |
| The ASA grading, n
(%) |
|
|
|
|
| Grade
I | 42
(35.00) | 45 (45.92) |
|
|
| Grade
II | 65
(54.17) | 45 (45.92) |
|
|
| Grade
III | 13
(10.83) | 8 (8.16) |
|
|
| Maximum diameter of
lesion (cm) | 2.81±0.32 | 3.05±0.50 | 0.469 | 0.674 |
| Lesion site, n
(%) |
|
| −0.723 | 0.470 |
| Left
upper lobe | 28
(23.33) | 25 (25.51) |
|
|
| Left
lower lobe | 16 (13.33) | 15 (15.31) |
|
|
| Right
upper lobe | 28
(23.33) | 23 (23.47) |
|
|
| Right
middle lobe | 12 (10.00) | 10 (10.20) |
|
|
| Right
lower lobe | 36 (30.00) | 25 (25.51) |
|
|
| Pathological type, n
(%) |
|
| −1.903 | 0.057 |
| Squamous
carcinoma | 39 (32.50) | 42 (42.86) |
|
|
|
Adenocarcinoma | 46 (38.33) | 38 (38.78) |
|
|
|
Adeno-squamous carcinoma | 18 (15.00) | 10 (10.20) |
|
|
|
Others | 17 (14.17) | 8 (8.16) |
|
|
| Pathological stage,
n (%) |
|
| −0.444 | 0.657 |
| IA | 35 (29.17) | 31 (31.63) |
|
|
| IB | 42 (35.00) | 35 (35.71) |
|
|
|
IIA | 16 (13.33) | 12 (12.24) |
|
|
|
IIB | 17 (14.17) | 10 (10.20) |
|
|
|
IIIA | 9 (7.50) | 10 (10.20) |
|
|
|
IIIB | 1 (0.83) | 0 |
|
|
| Serum D-dimer
(mg/l) | 0.37±0.16 | 0.36±0.15 | −0.148 | 0.882 |
Methods
Preoperative preparations
Two groups of patients were treated with the same
preoperative preparations, including respiratory exercise, smoking
cessation, aerosol inhalation, correction of water, and electrolyte
disorders. All the patients underwent preoperative computed
tomography (CT), chest-enhanced CT and other tests for the
confirmation of the diagnosis and stage. Mediastinoscopy and biopsy
were not taken as routine examinations. Reserves and the
compensatory capacity of the heart, lung, liver and kidney and the
preserved skin of all the patients were comprehensively understood
and assessed prior to surgery. In addition, before operation,
gastrointestinal decompression tube and ureter were indwelt, and
broad-spectrum antibiotics were retentively used. After the
adequate preparation, surgical treatment was conducted.
Thoracoscopy group
Patients were placed in the lateral position, and
were generally anesthetized through double-lumen endotracheal
intubation. Then patients received one-lung ventilation in the
lateral recumbent position for radical surgery for lung cancer. The
3-hole method was used for operations: The observation hole with
the diameter of 15 mm was located at the 7th and 8th intercostal of
the midaxillary line of patients, and the Strykerl088i-30
thoracoscopy was inserted. An operation mouth with the length of
30–50 mm was made at the 4th and 5th intercostal of the anterior
axillary line, and a deputy operation mouth with the length of
about 20 mm was made at the 6th and 7th intercostal of the
posterior axillary line or the 8th intercostal of the infrascapular
line. Ribs of patients in the thoracoscopy group were not cut, and
not distracted by a distractor. The cut lung lobes were placed in
the specimen bag and removed from the operation mouth to protect
the incision from the implantation metastasis and wound infection.
Routine mediastinal lymphadenectomy in the hilus of the lung was
conducted. At the end of the operation, the patients were monitored
and treated in the intensive care unit, a breathing machine was
used to assist breathing, and vital signs were dynamically
monitored. The trachea cannulas were removed under the condition
that patients woke up with normal vital signs and blood gas
analysis results. Analgesia pumps were not routinely used after
operation.
Thoracotomy group
Radical surgery for lung cancer was completed by
accessing the chest through conventional posterior incision.
D-dimer method
Patients were examined by extracting peripheral
blood preoperatively, immediately and 24 h after surgery. The blood
was preserved in a citrate anticoagulant vacuum tube for parallel
plasma D-dimer determination.
Observation indexes
The operation time, intraoperative blood loss, blood
transfusion, postoperative thoracic drainage time and volume,
postoperative hospital stay, the incidence rate from moderate to
severe pains in incisions at 6 h after operation (FACES®
Pain Rating Scale), the use rate of analgesics, the time of the
disappearance of pain in incisions after operation and relevant
postoperative complications within the perioperative period of
patients were observed. In addition, levels of the serum D-dimer in
the two groups of patients before operation, immediately after
operation and at 24 h after operation were observed. The change of
prothrombin time (PT), activated partial thromboplastin time
(APTT), thrombin time (TT), blood coagulation factor V and VII of
patients before and after surgery were also observed and
recorded.
Statistical analysis
SPSS 17.0 (SPSS, Inc., Chicago, IL, USA) statistical
software was used for analysis. Measurement data were expressed as
mean ± SD. Intergroup comparisons were detected using the t-test,
and comparisons among multiple groups or intragroup comparisons
were detected using the analysis of variance. Countable data were
expressed as a percentage or composition ratio, and intergroup
comparisons were detected using the χ2 test. Ranked data
were expressed as a percentage or composition ratio, and intergroup
comparisons were detected using the rank-sum test. Inspection level
was α=0.05.
Results
Intraoperative condition
Operations of all the patients were successfully
completed. The blood loss and transfusion rate in the thoracoscopy
were significantly lower than those in the thoracotomy group
(P<0.05), but there was no statistically significant difference
in the average operation time between the thoracoscopy and
thoracotomy groups (Table II).
| Table II.Comparison of intraoperative
condition of patients between the thoracotomy and thoracoscopy
groups. |
Table II.
Comparison of intraoperative
condition of patients between the thoracotomy and thoracoscopy
groups.
| Intraoperative
condition | Thoracotomy group
(n=120) | Thoracoscopy group
(n=98) |
χ2/t | P-value |
|---|
| Operative time
(min) | 126.17±39.23 | 132.23±32.56 | 1.106 | 0.276 |
| Intraoperative
blood loss (ml) | 234.23±53.72 | 110.64±18.25 | −6.316 | <0.001 |
| Blood transfusion n
(%) | 27 (22.50) | 8 (8.16) | 8.227 | 0.004 |
Postoperative condition
Postoperative recovery condition
The postoperative hospital stay, the thoracic
drainage time and volume in the thoracoscopy group were shorter or
smaller than those in the thoracotomy group (P<0.05) (Table III). No pain pump was used in both
groups. Postoperative pain was assessed by the FACES®
Pain Rating Scale at 6 h after operation. The incidence rate of
moderate to severe pain in incisions, the use rate of analgesics
and the average time of the disappearance of pain in incisions in
the thoracoscopy were lower than those in the thoracotomy group
(P<0.05) (Table III).
| Table III.Comparison of postoperative recovery
condition of patients between the thoracotomy and thoracoscopy
groups. |
Table III.
Comparison of postoperative recovery
condition of patients between the thoracotomy and thoracoscopy
groups.
| Postoperative
condition | Thoracotomy group
(n=120) | Thoracoscopy group
(n=98) |
χ2/t | P-value |
|---|
| Thoracic drainage
time (days) | 6.27±2.13 | 4.38±1.92 | −5.670 | <0.001 |
| Thoracic drainage
volume (ml) | 1453.57±611.25 | 1024.78±556.95 | −5.743 | <0.001 |
| Postoperative
hospital stay (days) | 13.84±2.31 | 10.12±2.56 | −5.694 | <0.001 |
| Incidence rate of
moderate to severe pains in incisions at 6 h after operation, n
(%) | 72 (60.00) | 20 (20.41) | 34.667 | <0.001 |
| Use rate of
analgesics, n (%) | 68 (56.67) | 18 (18.37) | 33.126 | <0.001 |
| Average time of the
disappearance of pain in incisions (h) | 72.58±20.98 | 28.67±14.37 | −53.642 | <0.001 |
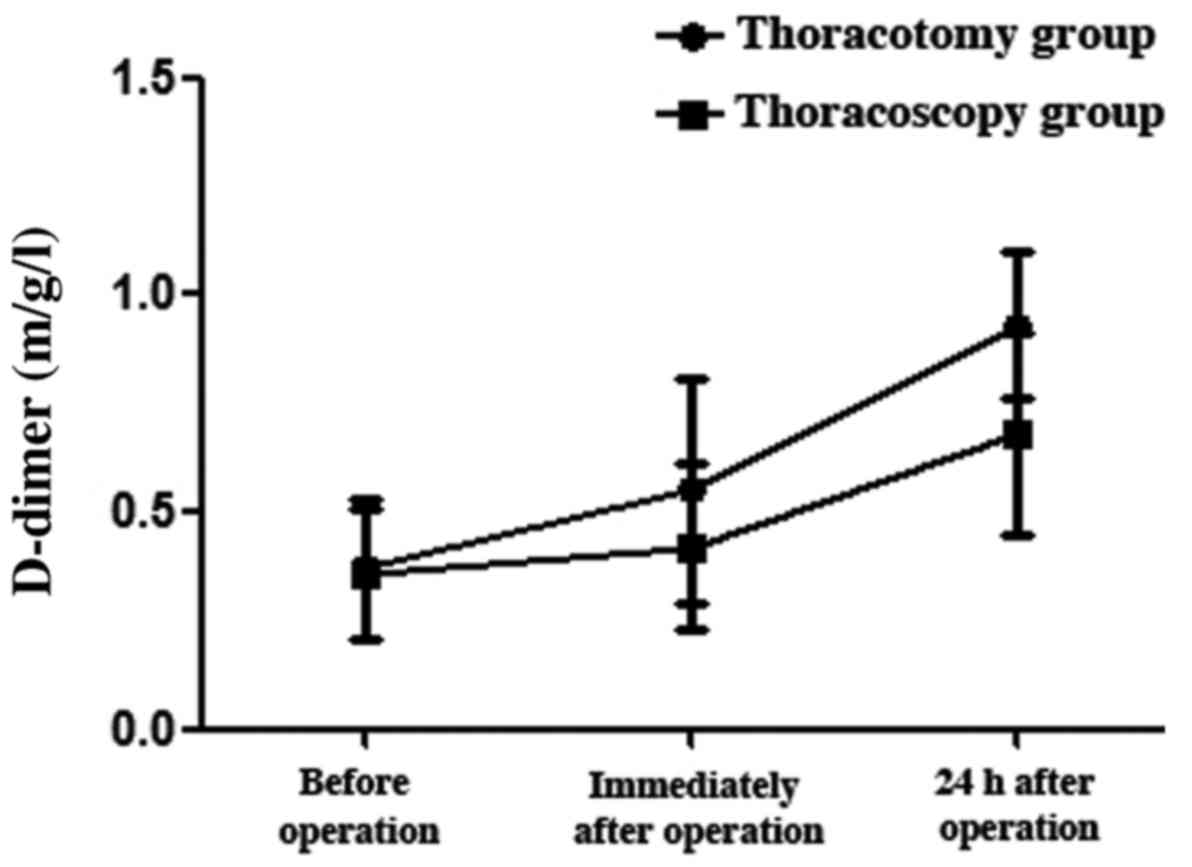
Changes in serum D-dimer after
operation
The level of serum D-dimer in the two groups after
operation was significantly higher than that before operation, and
the serum D-dimer level of patients was further increased at 24 h
after operation (P<0.05). The comparison between the two groups
showed that the levels of serum D-dimer in the thoracoscopy group
immediately and at 24 h after operation were significantly lower
than those in the thoracotomy group (P<0.05) (Table IV and Fig.
2). There was no significant difference of PT, APTT and TT in
the two groups before and after surgery (P>0.05). Coagulation
factor V and VII were elevated after surgery compared with those
before surgery (P<0.05). No significant differences were
identified between the two groups (P>0.05) (Table V).
| Table IV.Comparison of changes in serum
D-dimer of patients after operation between the thoracotomy and
thoracoscopy groups (mg/l). |
Table IV.
Comparison of changes in serum
D-dimer of patients after operation between the thoracotomy and
thoracoscopy groups (mg/l).
| Serum D-dimer | Thoracotomy group
(n=120) | Thoracoscopy group
(n=98) | t | P-value |
|---|
| Before
operation | 0.37±0.16 | 0.36±0.15 | −0.148 | 0.882 |
| Immediately after
operation | 0.55±0.26 | 0.42±0.19 | 4.001 | <0.001 |
| At 24 h after
operation | 0.93±0.17 | 0.68±0.23 | 8.585 | <0.001 |
| F-value | 277.785 | 67.492 |
|
|
| P-value | <0.001 | <0.001 |
|
|
| P1:2 | <0.001 | 0.132 |
|
|
| P1:3 | <0.001 | <0.001 |
|
|
| P2:3 | <0.001 | <0.001 |
|
|
| Table V.The changes of blood coagulation
indexes before and after operation of the two groups (mean ±
SD). |
Table V.
The changes of blood coagulation
indexes before and after operation of the two groups (mean ±
SD).
| Groups | Time | PT (sec) | APTT (sec) | TT (sec) | Coagulation factor
V(g/l) | Coagulation factor
VII(g/l) |
|---|
| Thoracoscopy | Before surgery | 12.32±0.87 | 28.65±2.65 | 17.32±2.34 | 2.19±0.43 | 2.19±0.43 |
|
| After surgery | 12.88±0.88 | 31.22±2.12 | 18.32±3.02 |
1.81±0.32a |
1.81±0.32a |
| Thoracotomy | Before surgery | 12.45±0.98 | 28.98±2.01 | 17.43±2.19 | 2.23±0.52 | 2.23±0.52 |
|
| After surgery | 12.78±0.97 | 32.43±1.35 | 18.97±3.21 |
1.82±0.54a |
1.82±0.54a |
Postoperative complications
Although the total incidence rate of postoperative
complications in the thoracoscopy was lower than that in the
thoracotomy group, there was no statistically significant
difference between the two groups. Only the incidence rate of wound
infection in the thoracoscopy was significantly lower than that in
the thoracotomy group (P<0.05) (Table
VI). Among the patients, there were 28 patients with
arrhythmia, which was improved after observation or through
treatment with antiarrhythmic drugs; there were 3 patients with
atelectasis, which was improved through active expectoration,
anti-infection, bronchoscopy suction and other treatments; there
were 46 patients with pulmonary infection, which was improved by
active expectoration and anti-infection treatments; there were 4
patients with air leak at 5 days after operation, which was stopped
by the intrapleural injection of albumins and other treatments;
there were 3 patients with empyema, which was improved by receiving
thoracic close drainage, rinse, nutrition support and
anti-infection treatments; there was 1 patient with thoracic
hemorrhage and 1 patient with chylothorax, who were treated with
thoracotomy again; and there were 12 patients with wound infection
due to obesity and the history of diabetes, who were discharged
after the wound dressing was changed and anti-infection treatment
was conducted (Table V).
| Table VI.Comparison of condition of
postoperative complications of patients between the thoracotomy and
thoracoscopy groups [n (%)]. |
Table VI.
Comparison of condition of
postoperative complications of patients between the thoracotomy and
thoracoscopy groups [n (%)].
| Complication | Thoracotomy group
(n=120) | Thoracoscopy group
(n=98) | χ2 | P-value |
|---|
| Arrhythmia | 17 (14.17) | 11 (11.22) | 0.417 | 0.518 |
| Atrial
fibrillation | 10 (8.33) | 6 (6.12) | 0.388 | 0.533 |
|
Supraventricular
tachycardia | 4 (3.33) | 5 (5.10) | 0.055 | 0.815 |
|
Ventricular premature
beat | 1 (0.83) | 0 | 0.000 | 1.000 |
|
Ventricular fibrillation | 0 | 0 | 0.000 | 1.000 |
| Sinus
bradycardia | 2 (1.67) | 0 | 0.325 | 0.569 |
| Lung |
|
|
|
|
|
Atelectasis | 1 (0.83) | 2 (2.04) | 0.031 | 0.860 |
|
Pulmonary infection | 26 (21.67) | 20 (20.41) | 0.051 | 0.821 |
|
Pulmonary air leak after
operation | 2 (1.67) | 2 (2.04) | 0.000 | 1.000 |
| Empyema | 2 (1.67) | 1 (1.02) | 0.000 | 1.000 |
| Chylothorax | 1 (0.83) | 0 | 0.000 | 1.000 |
| Thoracic
hemorrhage | 0 | 1 (1.02) | 0.000 | 1.000 |
| Incision
infection | 10 (8.33) | 2 (2.04) | 4.106 | 0.043 |
| Deep venous
thrombosis | 3 (2.50) | 0 | 0.984 | 0.321 |
| Total | 62 (51.67) | 39 (39.80) | 3.057 | 0.080 |
Discussion
Since the 1990s, video-assisted thoracoscopic
surgery has been increasingly widely used in the treatment of
benign and malignant pulmonary diseases. Compared with traditional
thoracotomy, thoracoscopic surgery is characterized by minimal
trauma, mild postoperative pain, fewer postoperative complications,
short hospital stay, good aesthetic appearance and other advantages
(8). However, a study has shown that
thoracoscopic surgery has no major advantages compared with
traditional thoracotomy, but has a long operation time and may
increase intraoperative complications (9). Kuritzky and Ng (10) found that no significant difference was
shown regarding the curative effect in the treatment of elderly
patients with non-small cell lung cancer between thoracoscopic lung
surgery and thoracotomy. Nevertheless, the amount of bleeding and
complication conditions are better in thoracoscopic lung surgery
with shorter postoperative hospitalization time and lighter early
inflammatory reaction. Nwogu et al (11) suggested that full thoracoscopical lung
resection of lymph node dissection in the treatment of peripheral
lung cancer is safe, effective, and feasible with less
postoperative pleural fluid. It can achieve the effect of
conventional thoracic surgery in terms of radical lymph node
dissection. Gopaldas et al (12) showed that the single hole
thoracoscopic lobectomy for the treatment of early peripheral lung
cancer is a safe and effective operation.
In the present study, the blood loss and transfusion
rate in the thoracoscopy were less than those in the thoracotomy
group, but the average operation time and postoperative
complications in the two groups were equivalent. This was mainly
because when the retrospectively analyzed patients were included,
the thoracoscopic surgery techniques of the Department of Thoracic
Surgery of our hospital has become relatively more mature, and
clinicians were relatively more experienced, which obviously made
the thoracoscopic surgery more safe and reliable than that before
the techniques were advanced. In thoracoscopic surgery, the field
of vision is wide and clear, the anatomical structure is clear, the
incision is small and the errhysis volume is small, thus leading to
little intraoperative blood loss in thoracoscopic surgery. A
prospective study of Flores et al (13) showed that the number of patients with
postoperative complications, including atrial fibrillation,
persistent pulmonary air leak, atelectasis, and pneumonia, in the
thoracoscopy was significantly less than that in the thoracotomy
group. However, in the present study, the incidence rate of
postoperative complications in the two groups was equivalent, and
only the incidence rate of wound infection in the thoracoscopy was
significantly lower than that in the thoracotomy group. In our
study, complications in the thoracoscopy group were mainly
distributed in pulmonary infection and arrhythmia. Pulmonary
infection was mainly due to the history of smoking and pulmonary
diseases in recent years, while preoperative and postoperative
banning on smoking increased the psychological burden of patients.
A study has revealed that more than 400 cigarettes a year, combined
with basic pulmonary diseases and the forced expiratory volume in
one second (FEV1%) less than or equal to 60% are high-risk factors
for the incidence of complications of lung cancer surgeries
(14). At present, it is still
controversial whether the incidence rate of postoperative
arrhythmia in patients with lung cancer is affected by
thoracoscopic surgery or the traditional thoracotomy method.
Arrhythmia is a common complication of thoracic tumor surgery,
commonly manifesting as atrial fibrillation, and its incidence rate
is more than 20% (15,16). The results of the present study
indicated that the number of patients with arrhythmia including
atrial fibrillation in the thoracoscopy group was not significantly
reduced compared with that in the conventional thoracotomy group.
This result is similar to that obtained in the study of Park et
al (17). However, a study
revealed that the incidence rate of arrhythmia in the pulmonary
lobectomy under the thoracoscopy is significantly lower than that
in the conventional thoracotomy (18).
D-dimer is the product degraded from fibrin polymers
under the action of plasmin after fibrin monomers form fibrin
polymers through the crosslinking of the activation factor, XIII,
and it is a specific index embodying human secondary fibrinolysis
hyperthyroidism (19). Surgical
injury and anesthetic stimulation can lead to increased levels of
prothrombin fragment, fibrinopeptide A and other substances, which
can alter the coagulation status of the body. In research by Allaix
et al (20), suspected VTE
patients with negative D-dimer were followed up for 6 months.
Thrombosis occurred in only 1.9% of patients. VTE patients with a
high level of D-dimer are usually recovered to a normal status in
about a month. In the present study, the levels of serum D-dimer
immediately and at 24 h after operation in the two groups were
significantly higher than that before operation, and the change in
serum D-dimer in the thoracotomy was more obvious than that in the
thoracoscopy group. Since the trauma of thoracoscopic surgery is
small, the incidence rate of postoperative hypercoagulable state of
blood is lower than that of traditional thoracotomy, and similar
results have been reported in many articles regarding the
thoracoscopic and laparoscopic surgeries (21). Previous findings have shown that serum
D-dimer level is increased in a variety of malignant tumors, and it
is closely related to tumor stage, lymph node metastasis and other
factors (22). Some studies have
indicated that the increased level of serum D-dimer is
significantly associated with poor prognosis of lung cancer
(6,19). Therefore, the main reason for the
increase in serum D-dimer level in this study needs to be further
studied.
With the continuous development of thoracoscopic
surgery techniques and equipment, radical surgery for lung cancer
using thoracoscopy has achieved good results. The advantages of
thoracoscopic surgery in the perioperative period have become
increasingly apparent, and its relatively reduced effect on the
postoperative hypercoagulable state of blood has drawn increasing
attention.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YY interpreted the data and drafted this manuscript.
HS conceived and designed this study. YZ and HH collected and
analyzed the data. ZY finally revised and approved the manuscript.
All authors read and approved the final manuscript
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Ningbo No. 2 Hospital. Patients who participated in
this research, signed the informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen WQ, Zhang SW and Zou XN: A study on
the estimation and trend of death of lung cancer in China. Chin J
Lung Cancer. 13:488–493. 2010.(In Chinese).
|
|
4
|
Nakamura H and Taniguchi Y: Robot-assisted
thoracoscopic surgery: current status and prospects. Gen Thorac
Cardiovasc Surg. 61:127–132. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vandlac AA, Cowan NG, Chen Y, Anderson RE,
Conlin MJ, La Rochelle JC, Amling CL and Koppie TM: Timing,
incidence and risk factors for venous thromboembolism in patients
undergoing radical cystectomy for malignancy: A case for extended
duration pharmacological prophylaxis. J Urol. 191:943–947. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang PP, Sun JW, Wang XY, Liu XM and Li
K: Preoperative plasma D-dimer levels predict survival in patients
with operable non-small cell lung cancer independently of venous
thromboembolism. Eur J Surg Oncol. 39:951–956. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Qi Y and Fu J: Research on the coagulation
function changes in non small cell lung cancer patients and
analysis of their correlation with metastasis and survival. J BUON.
22:462–467. 2017.PubMed/NCBI
|
|
8
|
Laursen LO, Petersen RH, Hansen HJ, Jensen
TK, Ravn J and Konge L: Video-assisted thoracoscopic surgery
lobectomy for lung cancer is associated with a lower 30-day
morbidity compared with lobectomy by thoracotomy. Eur J
Cardiothorac Surg. 49:870–875. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Spartalis E, Mantonakis E, Athanasiou A
and Moris D: Lobectomy by video-assisted thoracic surgery or
muscle-sparing thoracotomy for stage 1 lung cancer: Could
cost-effectiveness give the answer? J Am Coll Surg. 221:8902015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kuritzky AM and Ng T: Video-assisted
thoracic surgery vs muscle-sparing thoracotomy: Prioritizing
randomized trial to assess complications and long-term survival
over cost comparisons: In reply to Spartalis and colleagues. J Am
Coll Surg. 221:890–891. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nwogu CE, D'Cunha J, Pang H, Gu L, Wang X,
Richards WG, Veit LJ, Demmy TL, Sugarbaker DJ, Kohman LJ, et al:
Alliance for clinical trials in oncology: VATS lobectomy has better
perioperative outcomes than open lobectomy: CALGB 31001, an
ancillary analysis of CALGB 140202 (Alliance). Ann Thorac Surg.
99:399–405. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gopaldas RR, Bakaeen FG, Dao TK, Walsh GL,
Swisher SG and Chu D: Video-assisted thoracoscopic versus open
thoracotomy lobectomy in a cohort of 13,619 patients. Ann Thorac
Surg. 89:1563–1570. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Flores RM, Park BJ, Dycoco J, Aronova A,
Hirth Y, Rizk NP, Bains M, Downey RJ and Rusch VW: Lobectomy by
video-assisted thoracic surgery (VATS) versus thoracotomy for lung
cancer. J Thorac Cardiovasc Surg. 138:11–18. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Suzuki M, Otsuji M, Baba M, Saitoh Y,
Iizasa T, Shibuya K, Sekine Y, Yoshida S and Fujisawa T:
Bronchopleural fistula after lung cancer surgery. Multivariate
analysis of risk factors. J Cardiovasc Surg. 43:263–267. 2002.
|
|
15
|
Muranishi Y, Sonobe M, Menju T, Aoyama A,
Chen-Yoshikawa TF, Sato T and Date H: Atrial fibrillation after
lung cancer surgery: Incidence, severity, and risk factors. Surg
Today. 47:252–258. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang L and Gao S: Systematic review and
meta-analysis of atrial fibrillation Prophylaxis After Lung
Surgery. J Cardiovasc Pharmacol. 67:351–357. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Park BJ, Zhang H, Rusch VW and Amar D:
Video-assisted thoracic surgery does not reduce the incidence of
postoperative atrial fibrillation after pulmonary lobectomy. J
Thorac Cardiovasc Surg. 133:775–779. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Imperatori A, Mariscalco G, Riganti G,
Rotolo N, Conti V and Dominioni L: Atrial fibrillation after
pulmonary lobectomy for lung cancer affects long-term survival in a
prospective single-center study. J Cardiothorac Surg. 7:42012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ay C, Dunkler D, Pirker R, Thaler J,
Quehenberger P, Wagner O, Zielinski C and Pabinger I: High D-dimer
levels are associated with poor prognosis in cancer patients.
Haematologica. 97:1158–1164. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Allaix ME, Krane MK, Zoccali M, Umanskiy
K, Hurst R and Fichera A: Postoperative portomesenteric venous
thrombosis: Lessons learned from 1,069 consecutive laparoscopic
colorectal resections. World J Surg. 38:976–984. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Diao D, Zhu K, Wang Z, Cheng Y, Li K, Pei
L and Dang C: Prognostic value of the D-dimer test in oesophageal
cancer during the perioperative period. J Surg Oncol. 108:34–41.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang PP, Sun JW, Wang XY, Liu XM and Li
K: Preoperative plasma D-dimer levels predict survival in patients
with operable non-small cell lung cancer independently of venous
thromboembolism. Eur J Surg Oncol. 39:951–956. 2013. View Article : Google Scholar : PubMed/NCBI
|