Introduction
Patients with human papillomavirus (HPV) -associated
oropharyngeal cancer (OPC) exhibit an improved prognosis in terms
of response and survival (1).
High-risk HPV types, particularly 16 and 18, shown serve a central
role in the development of head and neck cancer (2,3). It has
been identified that ~26% of head and neck squamous cell carcinoma
cases and 36% of oropharyngeal squamous cell carcinomas are
HPV-positive; additionally, the relative proportion of HPV-positive
head and neck squamous cell carcinomas has been increasing over the
past 20 years (2).
p16, also known as cyclin-dependent kinase inhibitor
2A, has been postulated as a surrogate marker for HPV (3). The p16/Rb/cyclin-D1 pathway is a key
regulator of the cell cycle. The p16 protein inhibits cdk4- and
cdk-6 cyclin D complexes, and prevents Rb phosphorylation. p16
protein is inactivated by the HPV viral oncoprotein E7 (2).
However, there is controversy regarding the
prognostic role of HPV in hypopharyngeal cancer. Certain studies
have advocated for it (4), whereas
others have reported that it does not have prognostic value
(5). Therefore, the present study
investigated the prognostic value of p16 expression status with
respect to the response to induction chemotherapy for advanced
hypopharyngeal squamous cell carcinoma (HPSCC), which has long been
the established treatment regimen at Chonnam National University
Medical School and Hwasun Hospital (Hwasun, South Korea) (6–8). The
present study also investigated tumor protein P53 (hereafter p53)
expression status, which has been reported to predict the treatment
response for advanced cancer (9,10).
Materials and methods
Patients and tumor specimens
A total of 45 patients over the age of 18 years (43
male, 2 female; age range, 46–82 years; mean, 63.0 years) that had
been diagnosed with locally advanced HPSCC between January 2004 and
December 2013 (for 10 years) were retrospectively reviewed.
Inclusion criteria were the following: Biopsy-confirmed SCC arising
in the hypopharynx; stage III or IV cancer; treatment with at least
two cycles of induction chemotherapy followed by concurrent
chemoradiation therapy and paraffin-embedded tumor tissue available
at diagnosis. All patients were staged again according to the
seventh edition of the American Joint Committee on Cancer staging
system (11).
Induction chemotherapy was performed with docetaxel
(70 mg/m2 on day 1), cisplatin (75 mg/m2 on
day 1), and fluorouracil (5-FU; 1,000 mg/m2 on days 1–4)
repeated every 3 weeks for up to three cycles. The treatment was
followed by cisplatin-based concurrent chemoradiation therapy
(CCRT). Radiotherapy was started within 4 weeks of the completion
of induction chemotherapy, and the primary tumor and neck area were
involved in the treatment field. Cisplatin (100 mg/m2, 1
day schedule) was administered on the same day of the start of the
radiation and repeated every 3 weeks, depending on creatinine
clearance.
The clinicopathological characteristics of patients,
including age, sex, history of smoking or alcohol consumption,
tumor location, stage, differentiation, Karnofsky performance
status, response to treatment, radiation dose, radiation type,
progression-free survival (PFS) and overall survival (OS) time and
follow-up information were all obtained from hospital records.
Patient characteristics are summarized in Table I.
 | Table I.Patient clinicopathological
characteristics. |
Table I.
Patient clinicopathological
characteristics.
|
|
| p16 expression,
n |
|---|
|
|
|
|
|---|
| Patient
demographics | Total, n (%) | Positive (%) | Negative (%) | P-value |
|---|
| Age, years |
|
|
| 0.533 |
| ≥70 | 14 (31.1) | 3 (27.3) | 11 (32.4) |
|
|
<70 | 31 (68.9) | 8 (72.7) | 23 (67.6) |
|
| Sex |
|
|
| 0.056 |
| Male | 43 (95.6) | 9 (81.8) | 34 (100.0) |
|
|
Female | 2
(4.4) | 2 (18.2) | 0
(0.0) |
|
| Smoking |
|
|
| 0.266 |
|
Never | 15 (33.3) | 5 (45.5) | 10 (29.4) |
|
|
Ex/current | 30 (66.7) | 6 (54.5) | 24 (70.6) |
|
| Alcohol |
|
|
| 0.266 |
|
Never/social | 15 (33.3) | 5 (45.5) | 10 (29.4) |
|
|
Heavy | 30 (66.7) | 6 (54.5) | 24 (70.6) |
|
| Anatomical site |
|
|
| 0.038 |
| Pyriform
sinus | 35 (77.8) | 7 (63.6) | 28 (82.4) |
|
| Posterior
wall | 8
(17.8) | 2
(18.2) | 6
(17.6) |
|
|
Postcricoid area | 2
(4.4) | 2
(18.2) | 0
(0.0) |
|
| Clinical stage |
|
|
| 0.153 |
| III | 16 (35.6) | 2 (18.2) | 14 (41.2) |
|
| IV | 29 (64.4) | 9 (81.8) | 20 (58.8) |
|
| T stage |
|
|
| 0.014 |
| T1-2 | 23 (51.1) | 2 (18.2) | 21 (61.8) |
|
| T3-4 | 22 (48.9) | 9 (81.8) | 13 (38.2) |
|
| N stage |
|
|
| 0.396 |
| N0-1 | 20 (44.4) | 4 (36.4) | 16 (47.1) |
|
| N2-3 | 25 (55.6) | 7 (63.6) | 18 (52.9) |
|
| Differentiation |
|
|
| 0.700 |
|
Well | 11 (24.4) | 4 (36.4) | 7
(20.6) |
|
|
Moderate | 11 (24.4) | 2 (18.2) | 9
(26.5) |
|
|
Poor | 7
(15.6) | 2 (18.2) | 5
(14.7) |
|
| NA | 16 (35.6) | 3 (27.3) | 13 (38.2) |
|
| PS |
|
|
| 0.014 |
| 0 | 29 (64.4) | 8 (72.7) | 21 (61.8) |
|
| 1 | 14 (31.1) | 1 (9.1) | 13 (38.2) |
|
| 2 | 2
(4.4) | 2 (18.2) | 0
(0.0) |
|
| Induction response
1 |
|
|
| 0.398 |
| CR | 17 (37.8) | 5 (45.5) | 12 (35.3) |
|
|
Non-CR | 28 (62.2) | 6 (54.5) | 22 (64.7) |
|
| Induction response
2 |
|
|
| 0.689 |
| PR,
CR | 41 (91.1) | 10 (90.9) | 31 (91.2) |
|
| Non-PR
or CR | 4
(8.9) | 1
(9.1) | 3
(8.8) |
|
| CRT response |
|
|
| 0.359 |
| CR | 37 (82.2) | 10 (90.9) | 27 (79.4) |
|
|
Non-CR | 8
(17.8) | 1
(9.1) | 7
(20.6) |
|
| RT dose, cGy |
|
|
| 0.533 |
|
≥6,500 | 31 (68.9) | 8 (72.7) | 23 (67.6) |
|
|
<6,500 | 14 (31.1) | 3 (27.3) | 11 (32.4) |
|
| RT type |
|
|
| 0.128 |
|
3D-CRT | 33 (73.3) | 10 (90.9) | 23 (67.6) |
|
|
Others | 12 (26.7) | 1
(9.1) | 11 (32.4) |
|
The response evaluation was based on the Response
Evaluation Criteria in Solid Tumor (RECIST 1.1) (12), which was assessed by physical
examination, laryngoscopy and imaging studies. A partial response
(PR) was defined as a >50% decrease in tumor size and a complete
response (CR) was defined as no visible or palpable disease. Stable
disease (SD) was defined as stationary or progressive disease. The
current study was approved by the Institutional Review Board of
Chonnam National University Hwasun Hospital (Hwasun, South
Korea).
Immunohistochemistry
Automated immunohistochemistry was performed using
the Bond-Max system (Leica Biosystems, Ltd., Newcastle, UK). Tissue
sections of 2 µm were cut from each paraffin block and dried for 1
h at 60°C. Slides were then covered with Bond Universal Covertiles
and placed into the Bond-Max instrument (Leica Biosystems, Ltd.).
All steps were performed according to the manufacturer's protocol
in the following order: i) Deparaffinization using Bond Dewax
Solution (Leica Biosystems, Ltd.) at 72°C for 30 min; ii)
heat-induced epitope retrieval using Bond Epitope Retrieval
Solution 1 (Leica Biosystems, Ltd.) for 20 min at 100°C; iii)
peroxide block placement on the slides for 5 min at ambient
temperature; iv) incubation with anti-p16 (1:50 dilution; cat no.
G175-407; BD Pharmingen; BD Biosciences, San Jose, CA, USA) or
anti-p53 (1:1,200 dilution; cat no. DO-7; Dako; Agilent
Technologies GmbH, Waldbronn, Germany) primary antibody for 15 min
at ambient temperature; v) incubation with Post Primary reagent
(Leica Biosystems, Ltd.) for 8 min at ambient temperature, followed
by washing using Bond Wash solution (Leica Biosystems, Ltd.) for 6
min; vi) Bond™ Polymer Refine Detection (ready-to-use dilution; cat
no. DS9800; Leica Biosystems, Ltd.) placement on the slides for 8
min at ambient temperature, followed by washing using Bond Wash
(Leica Biosystems, Ltd.) and distilled water for 4 min; vii) color
development with 3,3′-diaminobenzidine tetrahydrochloride chromogen
for 10 min at ambient temperature; and viii) hematoxylin
counterstaining for 5 min at ambient temperature, followed by
mounting of the slides. Normal human serum served as a negative
control. Stained tissues were viewed and images captured using a
light microscope under five fields in each sample (magnification,
×100).
Evaluation of immunohistochemical
staining
The staining results for p16 and p53 were
statistically examined in several ways. Fist, the evaluation of all
staining was performed as a blind assessment by one pathologist who
was a specialist in the head and neck region. Staining intensity
for p16 was scored between 0 and 3 (0, negative; 1, weakly
positive; 2, moderately positive; 3, strongly positive). The
percentage of the staining area was graded on a scale with five
grades: No staining, 0; <25% staining, 1; 25–49%, 2; 50–74%, 3;
and ≥75%, 4. The staining index for p16 was calculated as the
multiplication of the staining intensity and the staining area
scores. Tumors were categorized as high (staining index ≥6) or low
(staining index <6). Staining intensity >3 was evaluated as
positive. For p53, the group was divided into two groups: High
(staining area ≥10%), and low (staining area <10%).
Statistical analysis
The association between immunohistochemical staining
and clinicopathological parameters was examined using the
χ2 test and Fisher's exact test. Survival curves were
calculated using the Kaplan-Meier method, and a comparison of the
curves was performed using the log-rank test. PFS was calculated
from the start date of chemotherapy to the date of recurrence or
progression and OS was measured from the start date of treatment to
the date of mortality or date last seen. Variables were
incorporated in the univariate or multivariate Cox hazard
regression model. SPSS version 20.0 (IBM Corp., Armonk, NY, USA)
was used for statistical analyses. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
A total of 45 patients who had finished at least two
cycles of induction chemotherapy and CCRT were enrolled in the
present study. Of these patients, 35 (77.8%) received docetaxel,
cisplatin and 5-FU for induction chemotherapy, and 10 (22.2%)
received cisplatin and 5-FU for induction chemotherapy. The
majority of the patients underwent three cycles of induction
chemotherapy (40 patients, 88.9%) and the remaining five patients
underwent two cycles of induction chemotherapy. Following induction
chemotherapy, 17 patients (37.8%) exhibited CR and 28 patients
(62.2%) exhibited PR. The treatment was followed by cisplatin-based
CCRT. The CR rate was 82.2% (37 patients) and all others were 17.8%
(8 patients) following completion of all treatment.
Expression of p16 and p53
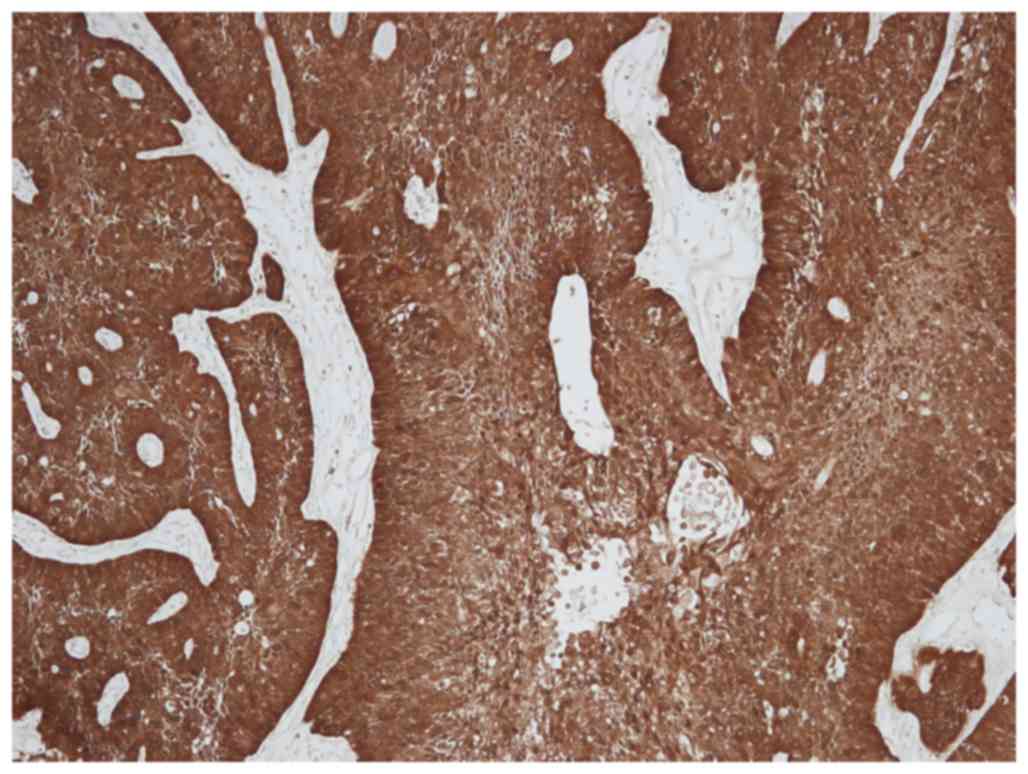
Staining for p16 was observed in the nucleus and
cytoplasm of the tumor cells and occasionally in the stroma
(Fig. 1). There were 11 patients
(24.4%) with p16-positive tumor cells. The correlation between p16
expression and clinicopathological parameters is presented in
Table I. No significant differences
were identified between the two types of responses of induction
chemotherapy (CR vs. non-CR; PR and CR vs. other) according to p16
status. No significant differences were identified in the response
following all treatments (chemotherapy and radiation therapy)
between groups with p16-positive and p16-negative staining.
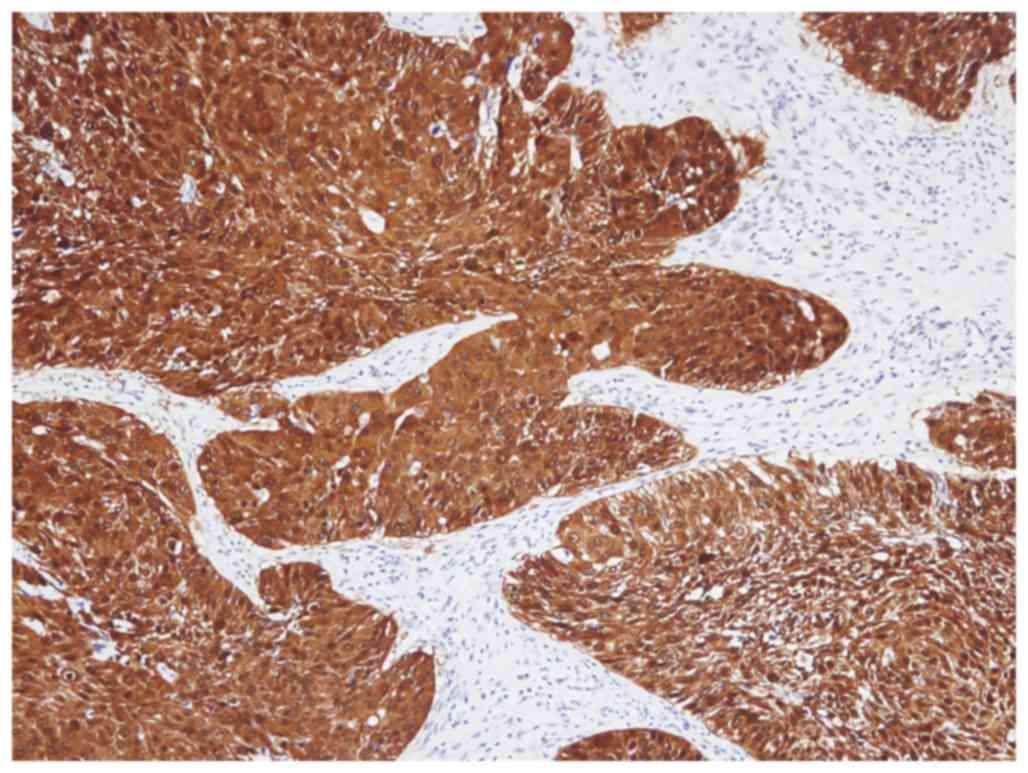
p53 frequently stained the nucleus of tumor cells
and was occasionally observed in the cytoplasm (Fig. 2). There were 30 patients (66.7%) with
high expression levels of p53. The associations between
p16-positivity and low p53, and between p16-negativity and high p53
were analyzed; however, no significant difference was identified
(P>0.05; Table II). No
association between low p53 expression and chemotherapy response
was observed (data not shown).
| Table II.Expression of p53 stratified by p16
status. |
Table II.
Expression of p53 stratified by p16
status.
|
|
| p16 status, n |
|---|
|
|
|
|
|---|
| p53 expression | Total, n (%) | Positive (%) | Negative (%) | P-value |
|---|
| p53 |
|
|
| 0.198 |
|
Low | 15 (33.3) | 2 (18.2) | 13 (38.2) |
|
|
High | 30 (66.7) | 9 (81.8) | 21 (61.8) |
|
Survival according to p16 status
A univariate analysis for PFS and OS time was
performed. A good response to induction chemotherapy (PR and CR vs.
other) was demonstrated to significantly decrease the risk of
mortality (P<0.001; Table
III).
| Table III.Univariate survival analysis. |
Table III.
Univariate survival analysis.
| Variable | PFS, OR (95%
CI) | P-value | OS, OR (95%
CI) | P-value |
|---|
| Age | 0.704
(0.311–1.594) | 0.400 | 0.647
(0.277–1.510) | 0.314 |
| Gender | 1.671
(0.225–12.400) | 0.616 | 22.289
(0.015–33,910.767) | 0.406 |
| Smoking | 1.322
(0.598–2.920) | 0.490 | 1.427
(0.630–3.232) | 0.395 |
| Alcohol | 1.187
(0.529–2.666) | 0.678 | 1.339
(0.577–3.108) | 0.497 |
|
Anatomic site |
|
|
|
|
|
Pyriform sinus |
| 0.522 |
| 0.460 |
|
Posterior wall | 1.438
(0.532–3.887) | 0.474 | 1.568
(0.578–4.256) | 0.377 |
|
Postcricoid area | 2.058
(0.474–8.940) | 0.336 | 2.089
(0.480–9.090) | 0.326 |
| Clinical stage | 1.418
(0.629–3.196) | 0.400 | 1.542
(0.663–3.582) | 0.314 |
| T stage | 1.936
(0.886–4.228) | 0.098 | 2.066
(0.926–4.607) | 0.076 |
| N stage | 1.191
(0.554–2.563) | 0.654 | 1.273
(0.581–2.789) | 0.546 |
|
Differentiation |
|
|
|
|
|
Well |
| 0.618 |
| 0.547 |
|
Moderate | 1.280
(0.386–4.237) | 0.686 | 1.609
(0.449–5.765) | 0.465 |
|
Poor | 2.087
(0.624–6.983) | 0.232 | 2.500
(0.694–9.006) | 0.161 |
| NA | 1.129
(0.382–3.335) | 0.827 | 1.424
(0.442–4.587) | 0.553 |
| PS |
|
|
|
|
| 0 |
| 0.874 |
| 0.828 |
| 1 | 1.105
(0.490–2.491) | 0.810 | 1.186
(0.521–2.698) | 0.684 |
| 2 | 0.647
(0.085–4.920) | 0.674 | 0.664
(0.087–5.058) | 0.692 |
| Induction response
1 | 0.570
(0.246–1.320) | 0.189 | 0.587
(0.252–1.368) | 0.217 |
| Induction response
2 | 0.082
(0.023–0.296) | <0.001 | 0.082
(0.023–0.296) | <0.001 |
| CRT response | 0.517
(0.204–1.310) | 0.164 | 0.472
(0.186–1.201) | 0.115 |
| RT dose | 1.165
(0.491–2.765) | 0.729 | 1.088
(0.456–2.598) | 0.848 |
| RT type | 2.321
(0.838–6.432) | 0.105 | 2.065
(0.745–5.727) | 0.163 |
| p16 status | 1.128
(0.468–2.720) | 0.788 | 0.938
(0.371–2.373) | 0.892 |
| p53 status | 1.649
(0.696–3.911) | 0.256 | 1.530
(0.642–3.644) | 0.337 |
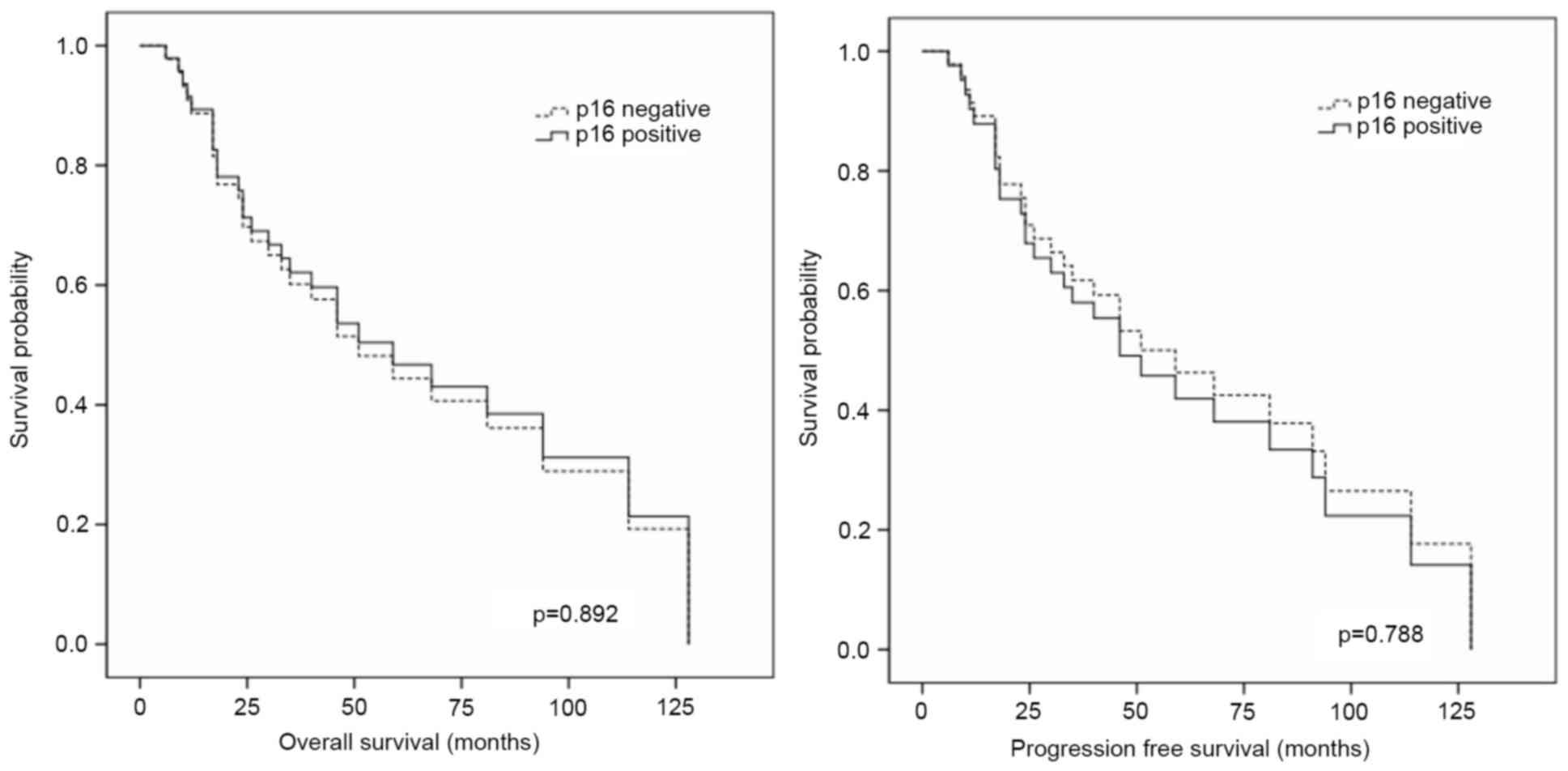
There was no significant difference in the survival
(PFS or OS) times between p16-positive and p16-negative staining
groups (P>0.05; Table III and
Fig. 3). Furthermore, according to
multivariate analysis, p16 did not alter the PFS or OS time
(P>0.05; Table IV).
| Table IV.Multivariate survival analysis. |
Table IV.
Multivariate survival analysis.
| Variable | PFS, OR (95%
CI) | P-value | OS, OR (95%
CI) | P-value |
|---|
| p16 status | 0.828
(0.224–3.059) | 0.777 | 0.601
(0.153–2.366) | 0.466 |
| p53 status | 1.531
(0.554–4.232) | 0.412 | 1.342
(0.476–3.787) | 0.578 |
| Age | 1.051
(0.371–2.982) | 0.925 | 0.793
(0.252–2.499) | 0.692 |
|
Differentiation |
|
|
|
|
|
Well |
| 0.709 |
| 0.648 |
|
Moderate | 1.053
(0.225–4.922) | 0.948 | 1.243
(0.241–6.423) | 0.795 |
|
Poorly | 2.318
(0.428–12.538) | 0.329 | 2.820
(0.482–16.495) | 0.250 |
| NA | 1.095
(0.265–4.530) | 0.901 | 1.296
(0.289–5.813) | 0.735 |
| Anatomic site |
|
|
|
|
|
Pyriform sinus |
| 0.208 |
| 0.173 |
|
Posterior wall | 2.425
(0.629–9.355) | 0.198 | 2.474
(0.643–9.527) | 0.188 |
|
Postcricoid area | 6.111
(0.523–71.447) | 0.149 | 7.655
(0.583–100.499) | 0.121 |
| T stage | 1.942
(0.716–5.264) | 0.192 | 2.340
(0.817–6.701) | 0.113 |
| N stage | 1.337
(0.494–3.624) | 0.568 | 1.670
(0.572–4.877) | 0.348 |
| RT dose | 1.870
(0.518–6.752) | 0.339 | 1.457
(0.394–5.396) | 0.573 |
| RT type | 2.644
(0.792–8.826) | 0.114 | 2.080
(0.611–7.077) | 0.241 |
| PS |
|
|
|
|
| 0 |
| 0.390 |
| 0.464 |
| 1 | 1.371
(0.498–3.771) | 0.541 | 1.402
(0.512–3.839) | 0.511 |
| 2 | 0.136
(0.006–2.998) | 0.206 | 0.170
(0.007–4.229) | 0.280 |
Discussion
The present study examined the degree to which HPV
may be involved in hypopharyngeal cancer. For oropharyngeal cancer,
an increased trend of occurrence in young adults and non-smokers
was previously reported, and changes in environmental risk factors,
including changes in smoking patterns and an increase in oral HPV
infections, have been postulated (13–15).
However, the present study identified no association between HPV
infection and age or smoking history in hypopharyngeal cancer. The
present study included 14 patients <60 years of age (although
only one patient was <50 years old) with HPSCC in the current
study, of whom only 3 exhibited p16-positive tumors (data not
shown). Age, smoking status or alcohol-drinking status did not
correlate with p16-positive expression. The present study revealed
that 11 patients (24.4%) were positive for p16 expression in
advanced HPSCC, which is slightly higher compared with other
reports (4,16,17).
However, p16 expression status did not predict chemoradiotherapy
response or survival rate in the present study. There remains
controversy regarding the role of p16 in the prognosis of HPSCC.
Certain studies have demonstrated that patients with HPV tend to
have improved prognoses (16,18), although others have reported the
opposite (5,19).
p53 has been reported to be a prognostic factor and
predictive marker of the response to chemotherapy in various types
of head and neck cancer, including oropharyngeal carcinoma
(9,20,21). In
HPV-associated oropharyngeal cancer, p53 expression is low owing to
HPV E6 protein activity, which targets p53 for ubiquitination and
degradation (22). This can preserve
the apoptotic function of p53 and thus enable radiation-induced
apoptosis (23). Therefore, the
present study also investigated p53 expression in HPSCC; 30
patients (66.7%) exhibited high p53 expression levels. However,
there was no association between p16-positivity and low p53
expression. Furthermore, low p53 expression was not associated with
chemotherapy response in the present study.
The staining results for p16 and p53 were examined
for staining intensity and percentage of staining. However, despite
the use of these analytic methods, no significance was identified
between p16 or p53 expression and clinicopathological parameters,
treatment response, or survival. A limitation of the present study
was the small sample size; thus, additional studies with more cases
are warranted.
In the present study, p16 expression status was not
identified to predict the response to chemotherapy in patients with
HPSCC. Furthermore, no association between high p16 expression and
the survival time of patients with HPSCC was identified.
Acknowledgements
The present study was supported by the Chonnam
National University Hospital Biomedical Research Institute (grant
no. HCRI 14 016-1). The abstract was presented at the AAO-HNSF
Annual Meeting and OTO Expo 2015, September 27-30, 2015 (Dallas,
TX, USA).
References
|
1
|
Kumar B, Cordell KG, Lee JS, Worden FP,
Prince ME, Tran HH, Wolf GT, Urba SG, Chepeha DB, Teknos TN, et al:
EGFR, p16, HPV titer, Bcl-xL and p53, sex, and smoking as
indicators of response to therapy and survival in oropharyngeal
cancer. J Clin Oncol. 26:3128–3137. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Geißler C, Tahtali A, Diensthuber M,
Gassner D, Stöver T and Wagenblast J: The role of p16 expression as
a predictive marker in HPV-positive oral SCCHN-a retrospective
single-center study. Anticancer Res. 33:913–916. 2013.PubMed/NCBI
|
|
3
|
Sritippho T, Pongsiriwet S,
Lertprasertsuke N, Buddhachat K, Sastraruji T and Iamaroon A: p16-a
possible surrogate marker for high-risk human papillomaviruses in
oral cancer? Asian Pac J Cancer Prev. 17:4049–4057. 2016.PubMed/NCBI
|
|
4
|
Shaughnessy JN, Farghaly H, Wilson L,
Redman R, Potts K, Bumpous J, Silverman C and Dunlap NE: HPV: A
factor in organ preservation for locally advanced larynx and
hypopharynx cancer? Am J Otolaryngol. 35:19–24. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wilson DD, Rahimi AS, Saylor DK, Stelow
EB, Jameson MJ, Shonka DC, Reibel JF, Levine PA and Read PW: p16
not a prognostic marker for hypopharyngeal squamous cell carcinoma.
Arch Otolaryngol Head Neck Surg. 138:556–561. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ahn JS, Cho SH, Kim OK, Lee JK, Yang DH,
Kim YK, Lee JJ, Lim SC, Kim HJ, Chung WK and Chung IJ: The efficacy
of an induction chemotherapy combination with docetaxel, cisplatin,
and 5-FU followed by concurrent chemoradiotherapy in advanced head
and neck cancer. Cancer Res Treat. 39:93–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bae WK, Hwang JE, Shim HJ, Cho SH, Lee JK,
Lim SC, Chung WK and Chung IJ: Phase II study of docetaxel,
cisplatin, and 5-FU induction chemotherapy followed by
chemoradiotherapy in locoregionally advanced nasopharyngeal cancer.
Cancer Chemother Pharmacol. 65:589–595. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bae WK, Hwang JE, Shim HJ, Cho SH, Lee KH,
Han HS, Song EK, Yun HJ, Cho IS, Lee JK, et al: Multicenter phase
II study of weekly docetaxel, cisplatin, and S-1 (TPS) induction
chemotherapy for locally advanced squamous cell cancer of the head
and neck. BMC Cancer. 13:1022013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Temam S, Flahault A, Périé S, Monceaux G,
Coulet F, Callard P, Bernaudin JF, St Guily JL and Fouret P: p53
gene status as a predictor of tumor response to induction
chemotherapy of patients with locoregionally advanced squamous cell
carcinomas of the head and neck. J Clin Oncol. 18:385–394. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bristow RG, Benchimol S and Hill RP: The
p53 gene as a modifier of intrinsic radiosensitivity: Implications
for radiotherapy. Radiother Oncol. 40:197–223. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Frisch M, Hjalgrim H, Jaeger AB and Biggar
RJ: Changing patterns of tonsillar squamous cell carcinoma in the
United States. Cancer Causes Control. 11:489–495. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nasman A, Attner P, Hammarstedt L, Du J,
Eriksson M, Giraud G, Ahrlund-Richter S, Marklund L, Romanitan M,
Lindquist D, et al: Incidence of human papillomavirus (HPV)
positive tonsillar carcinoma in Stockholm, Sweden: An epidemic of
viral-induced carcinoma? Int J Cancer. 125:362–366. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Shin A, Jung YS, Jung KW, Kim K, Ryu J and
Won YJ: Trends of human papillomavirus-related head and neck
cancers in Korea: National cancer registry data. Laryngoscope.
123:E30–E37. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dalianis T, Grün N, Koch J, Vlastos A,
Tertipis N, Nordfors C, Näsman A, Wendt M, Romanitan M, Bersani C,
et al: Human papillomavirus DNA and p16(INK4a) expression in
hypopharyngeal cancer and in relation to clinical outcome, in
Stockholm, Sweden. Oral Oncol. 51:857–861. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rodrigo JP, Hermsen MA, Fresno MF,
Brakenhoff RH, Garcia-Velasco F, Snijders PJ, Heideman DA and
García-Pedrero JM: Prevalence of human papillomavirus in laryngeal
and hypopharyngeal squamous cell carcinomas in northern Spain.
Cancer Epidemiol. 39:37–41. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kanyilmaz G, Ekinci O, Muge A, Celik S and
Ozturk F: HPV-associated p16 INK4A expression and response to
therapy and survival in selected head and neck cancers. Asian Pac J
Cancer Prev. 16:253–258. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ang SH, Haaland B, Acharyya S, Thu MM,
Krisna SS, Hwang SG, Tan PH, Ng QS, Tan DS, Tai WM, et al:
Interactions between clinical factors, p16, and cyclin-D1
expression and survival outcomes in oropharyngeal and
hypopharyngeal squamous cell carcinoma. Head Neck. 37:1650–1659.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shinohara S, Kikuchi M, Tona R, Kanazawa
Y, Kishimoto I, Harada H, Imai Y and Usami Y: Prognostic impact of
p16 and p53 expression in oropharyngeal squamous cell carcinomas.
Jpn J Clin Oncol. 44:232–240. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim MJ, Ki MS, Kim K, Shim HJ, Hwang JE,
Bae WK, Chung IJ, Lee DH, Lee JK, Yoon TM, et al: Different protein
expression associated with chemotherapy response in oropharyngeal
cancer according to HPV status. BMC Cancer. 14:8242014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chung CH and Gillison ML: Human
papillomavirus in head and neck cancer: Its role in pathogenesis
and clinical implications. Clin Cancer Res. 15:6758–6762. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Peltenburg LT: Radiosensitivity of tumor
cells. Oncogenesis and apoptosis. Q J Nucl Med. 44:355–364.
2000.PubMed/NCBI
|