Introduction
The overall incidence of oral cavity cancer in
general is decreasing (1).
Nevertheless, previous studies have revealed the incidence of oral
tongue squamous cell carcinoma (OTSCC) is increasing, particularly
in young adults <45 years of age (1–3). Patterns
in cancer epidemiology from 2000–2013 published by the
Surveillance, Epidemiology, and End Results Program 18 identified
~6,520 cases of tongue cancer, with an incidence rate that
increased from 2.6–3.3 per 100,000 (4).
The role of tobacco use and alcohol consumption,
traditional risk factors in the development of OTSCC, is well
established. However, exposure to such risk factors has not been
extensive, or may even be absent, in these young adults as compared
with in older individuals. Llewellyn et al (5) identified that even in patients >30
years old who smoked or consumed alcohol, the duration of exposure
was insufficient for the development of malignancy (5). Human papillomavirus (HPV) infection has
emerged as a potential risk factor for the development of OTSCC;
however, the results from prior studies are inconsistent with
regard to its potential role.
The etiology of HPV-associated head and neck SCC
(HNSCC) has been investigated in numerous epidemiologic studies,
and the subtypes HPV16 and HPV18 have been identified as the
causative agents (5). Patients with
HPV-positive HNSCC tend to be younger and have minimal tobacco and
alcohol use. HPV-positive HNSCC is most common in the oropharynx,
particularly in the tonsils and the base of the tongue, and is
usually well-differentiated. Anaya-Saavedra et al (6) revealed that high-risk HPV (HPV16 and
HPV18) is strongly associated with oral cancer, in their study of
oral cancer risk factors in Mexican patients (6). Conversely, other studies observed that
OTSCC in young Caucasian females is characteristically negative for
HPV. Possible causal factors may include genetic abnormalities,
such as Fanconi anemia, other oncogenic viral infections and/or
other environmental exposures, or may be associated with HPV types
other than HPV16 or 18 (7,8). This was based on the data that the
infection rate of the oral cavity and tongue is low, that the
incidence of HPV-associated cancer is decreasing in females and
that the increasing incidence of OTSCC in young Caucasian females
may not be due to HPV (6).
Patients with HPV-associated OTSCC have been
demonstrated to exhibit a better prognosis compared with patients
with non-HPV-associated OTSCC. Marur et al (9) concluded that questions associated with
the role of HPV, and the natural history of oral HPV infection,
remain. The result is that further studies are required for the
understanding of disease progression in order to optimize the
clinical management of patients with HNSCC with HPV positive
disease. With this background, the etiology, risk factors and
pathophysiology of OTSCC remain unknown.
The present study describes a case of OTSCC in a
21-year-old Caucasian female with insignificant conventional risk
factor exposure and atypical presentation.
Materials and methods
Ethical statement
The present retrospective study was approved by the
Meharry Medical College Institutional Review Board and the Medical
Executive Committee at Nashville General Hospital at Meharry
(Nashville, TN, USA).
Case report
A 21-year-old Caucasian female presented to the
emergency room of a city safety-net hospital with a one-week
history of a rapidly growing painful mass on the right side of the
tongue. The patient had initially noticed it as a ‘blister’, which
ruptured and ulcerated. The patient denied any constitutional
symptoms. The patient did not report a history of radiation
exposure and had no significant medical history. The patient
reported malignancies in multiple relatives, including ovarian
cancer (mother), brain cancer (uncle), cholangiocarcinoma (maternal
grandmother), lung/laryngeal cancer (paternal grandfather) and
unknown cancer types in four uncles. The patient denied any history
of smoking, alcohol consumption or illicit drug use. Examination
revealed an exophytic tender ulcer 3–4 cm in size on the right
lateral region of the tongue. The patient exhibited a palpable
right submandibular lymph node enlargement.
A fine needle aspiration of the right
jugulodigastric lymph node revealed poorly differentiated squamous
cell carcinoma. The patient underwent a panendoscopy and
examination under anesthesia that indicated a 2.5 cm ulcerated and
indurated lesion of the right lateral region of the tongue. An
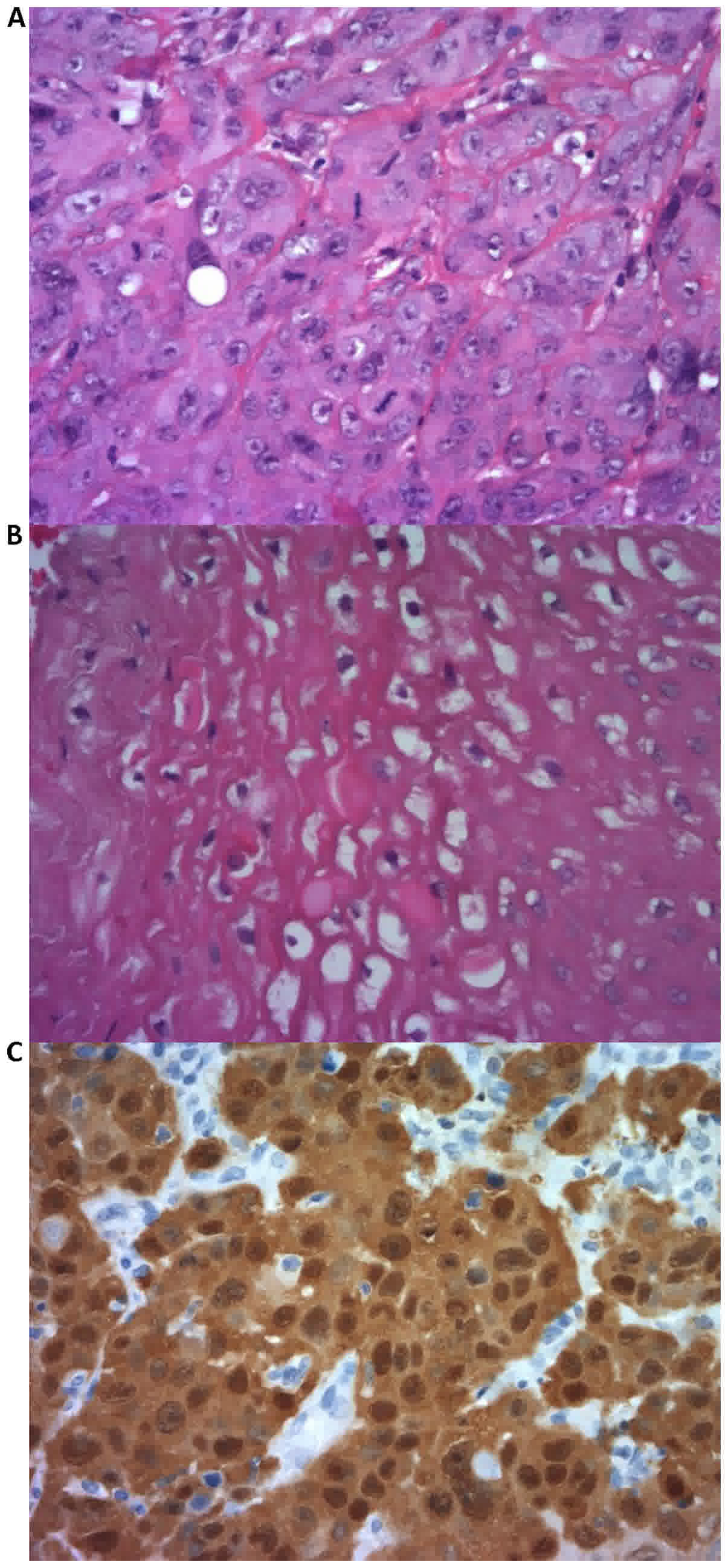
incisional biopsy revealed a well-moderately differentiated
invasive SCC, characterized by sheets of large cells with
pleomorphic vesicular nuclei, sparse eosinophilic cytoplasm, with
individual cell keratinization and focal keratin pearl formation,
and numerus mitotic figures (Fig.
1A). Focal clusters of malignant cells demonstrated
koilocytotic atypia characterized by cytoplasmic
vacuolization with thickening of the cytoplasmic membrane and mild
variation in the size and shape of the nuclei (Fig. 1B). A neck computed tomography scan
indicated a right lateral tongue mass with irregular enhancement in
the right parapharyngeal region, and magnetic resonance imaging
(MRI) demonstrated a 1.2×1.8×1.3 cm mass at the intersection of the
mid and posterior third of the right tongue without crossing the
raphe of the tongue. The enlarged lymph nodes involved levels IB,
II and III. Chest radiography indicated no abnormalities and the
brain MRI was negative for metastatic disease. Therefore, the final
staging was stage III (T3N1M0) based on the 6th edition of the
International Union Against Cancer (UICC) and the American Joint
Committee on Cancer (AJCC) (10).
The patient received neoadjuvant chemotherapy with
weekly carboplatin and paclitaxel. Following ten cycles, there was
significant clinical and radiological evidence of regression in the
size of the primary tumor and the lymph node. The patient then
underwent a partial right glossectomy with supraomohyoid neck
dissection. Histopathology indicated foci of well-poorly
differentiated SCC with marked degeneration and foreign body
granuloma. The neck dissection specimen demonstrated a small focus
of metastatic SCC in one of nine lymph nodes. Post-operatively, the
patient received chemotherapy with carboplatin and paclitaxel and
concurrent radiation for nine weeks. Radiotherapy was complicated
by dysphagia, for which the patient required a percutaneous
gastrostomy tube. Follow-up imaging and endoscopic examination
indicated no evidence of recurrence over the next three years.
The patient was eventually lost to follow-up, but
returned to the oncology clinic fifteen years post-surgery. At this
visit, the patient exhibited mild hypothyroidism, but no other
significant long-term toxicities from the treatment and was disease
free.
Koilocytotic atypia in an SCC of the head and
neck has been considered to be pathognomonic for HPV. At the time
of diagnosis, it was not standard practice to confirm the presence
of HPV in OTSCC, so that was not performed. The presence of
multiple relatively rare cancer types in the relatives, who were
also fairly young, was noteworthy. The young patient age and the
aggressiveness of the tongue cancer led to additional exploration
of the possibility of an unusually aggressive HPV strain and/or HPV
in the background of an underlying genetic condition, potentially
Lynch syndrome. The presence of actively replicating HPV in the
tumor was explored via immunohistochemical staining for cellular
p16, which is frequently elevated in HPV-positive SCC and is the
clinical lab surrogate marker for HPV.
In light of the relatively low incidence of certain
Lynch Syndrome-associated malignancies in the general population,
including endometrial, ovarian, gall bladder and brain cancer, a
number of genetic pedigrees have clearly indicated that indexed
patients are at risk (11). Based on
the history provided by the patient, immunohistochemical staining
was performed for four proteins, of which at least one is typically
underexpressed in individuals with Lynch Syndrome. These four
proteins are all involved in DNA mismatch repair and are MutL
homolog (MLH) 1, MLH2, MutS homolog 6 (MSH6) and PMS1 homolog 2
(PMS2).
Experimental methods
Cellular p16 immunohistochemistry
(surrogate marker for HPV)
Tumor tissue blocks were retrieved ~12 years
post-surgery and sectioned for confirmation of tumor grade and
cellular p16 staining. The resulting slides were deparaffinized
using the standard xylene/ethanol/PBS protocol. Antigen retrieval
was performed for 20 min at 98°C (60°C preheat/70°C cool down)
using the LabVision™ PT module and PT Module Tris pH 9 Buffer
(Thermo Fisher Scientific, Inc., Waltham, MA, USA). Immunostaining
was mechanically performed on the LabVision™ Autostainer using the
CINtec® p16INK4a detection system (REF 9517;
Roche Diagnostics, Tucson AZ, USA). Staining was performed
according to the manufacturer's protocol, with the exception that
following the 30 min room temperature incubation with primary
antibody the slides was stringently washed for 5 min in TBS
containing 0.1% Tween 20. The kit included the ready-to-use
CINtec® monoclonal mouse anti-Human p16INK4a
antibody (Clone E6H4) and the negative control monoclonal mouse
anti-rat oxytocin-related neurophysin. The slides were
counterstained for 1 min with 1:5 dilution of Ready-to-Use Mayer's
hematoxylin (Thermo Fisher Scientific, Inc., cat. no., TA-060-MH),
dehydrated by sequential 1 min incubations in 95% ethanol, two
rounds of 100% ethanol and 2 rounds of 100% xylene (Thermo Fisher
Scientific, Inc.) and coverslipped using Cytoseal XYL (Thermo
Fisher Scientific, Inc. cat. no., 9312-4). Images were captured
using a Nikon EclipAcse E400 (Nikon Corporation, Tokyo, Japan)
equipped with a Motic 5 MP digital webcam (Motic Instruments INC,
Canada). Hematoxylin and eosin (H&E) staining was performed
using Hematoxylin 7211 and Eosin-Y Alcoholic kit (Thermo Fisher
Scientific, Inc.).
p16 positive staining was concluded based on strong
diffuse nuclear and cytoplasmic staining in >70% of malignant
cells. No staining, faint diffuse nuclear and cytoplasmic staining,
small foci of staining or staining in non-malignant cells were
considered negative results. The positive control was a tonsil
cancer biopsy previously determined to be p16 positive as part of
the standard clinical laboratory procedure.
Lynch Syndrome protein
immunohistochemistry (IHC)
Antigen retrieval, processing and staining methods,
and image capture were conducted as previously described for p16
IHC. Antibodies for the four proteins were as follows: OAAF03051
MSH2, ARP41348P050 MSH6 antibody N-terminal region 100 and
OAAF04086 PMS2 antibody (Aviva Systems Biology, San Diego CA, USA)
and BDB550838 MLH-1 (BD Biosciences, Franklin Lakes NJ, USA).
As these mutations tend to be germline, all cells
from individuals who do not have a mutation in one of these genes
(histologically normal or tumor cells) should demonstrate evidence
of the protein. The patterns of normal cellular expression of these
proteins are as follows: MLH1 exhibits general nuclear expression
with exclusion from nucleoli; MSH2 exhibits ubiquitous nuclear
expression with exclusion from nucleoli and may be detected in
vesicles; MSH6 exhibits nuclear expression with exclusion from
nucleoli, and additional lower cytoplasmic expression in certain
tissues (malignant cells for example); and normal tissues generally
demonstrate weak to moderate nuclear positivity for PMS2, again
with exclusion from nucleoli (12).
Results
Confirmation of OTSCC and the presence
of histopathological and immunohistochemical hallmarks of HPV
Archival OTSCC tissue was processed for standard
histopathological analysis using H&E staining (Fig. 1A). The original diagnosis of moderate
to well-differentiated OTSCC was confirmed, as was the presence of
koilocytotic atypia (Fig. 1B),
generally accepted as being pathognomonic for the presence of
actively replicating HPV. The presence of HPV was additionally
explored through use of the clinical lab-based methodology of IHC
staining for elevated cellular p16, a surrogate marker for actively
replicating HPV. Diffuse strong nuclear and cytoplasmic staining
was observed in >70% of malignant cells (Fig. 1C), which meets the diagnostic criteria
for HPV infection.
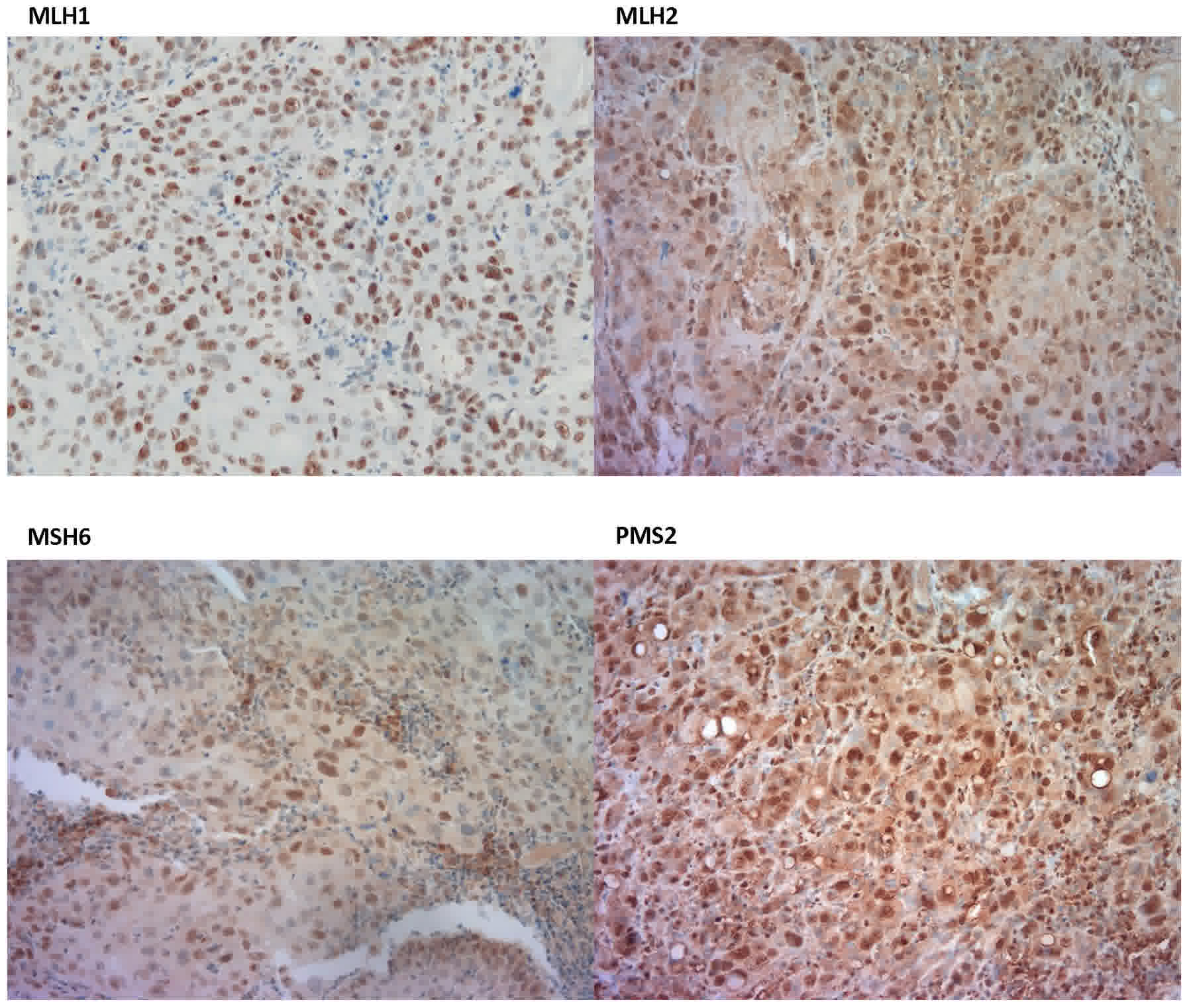
Lynch Syndrome protein
immunohistochemistry
Lynch Syndrome is a syndrome in which a protein
involved in DNA mismatch repair is not expressed due to a gene
mutation. The four most common proteins associated with this
syndrome are MLH1, MLH2, MSH6 and PMS2. IHC staining demonstrated
normal expression levels and patterns for all four of these
proteins (Fig. 2), concluding that
the patient was not affected by Lynch Syndrome.
Discussion
The present study provides an illustration of a case
of OTSCC in a young Caucasian adult, albeit one of only 21 years
old. The causality, risk factors and association with HPV infection
are unknown. A previous study examined a case in a patient as young
as 19 years of age which is consistent with current trends
(13). This referenced case as well
as the case in the present study, demonstrate an emerging
population of young women at increasing risk of tongue cancer.
Tobacco and alcohol use have been well-documented as
risk factors for OTSCC. This fact is additionally confirmed by the
decreasing trends in OTSCC, which is congruent with decreasing
tobacco and alcohol use. However, the increasing incidence of OTSCC
in young adults has indicated that there are emerging factors
separate from tobacco and alcohol use. A unique feature of OTSCC in
young patients has been the relative lack of these established risk
factors. Previous studies and case reports continue to highlight
this novel trend of the disease in young adults (1,2,5,7). These
patients exhibit insignificant contact with the known predisposing
factors to oral tongue cancer. Even in patients <30 years old
with a history of tobacco or alcohol use, the duration of exposure
has been demonstrated to be insufficient for the development of
malignancy (5). The patient in the
present study did not report any significant risk factors, raising
suspicions of the tongue cancer being HPV-associated. With the
significant family history of malignancies, Lynch Syndrome was also
considered.
Evidence for HPV included the initial suggestion on
the pathology report of koilocytotic atypia and the
confirmed strong p16 staining. The possibility of an underlying
genetic risk that may have resulted in enhanced aggressive tongue
cancer was also explored; however, the four Lynch Syndrome proteins
were all detected at normal levels with normal intracellular
distribution patterns. We hypothesized that there was something
unique about the HPV genotype in this particularly aggressively
growing tumor. However, it was not possible to purify DNA of a
quality that would allow extensive evaluation by PCR or sequencing,
and so the virus could not be genotyped (data not shown).
The HPV serotypes usually implicated in head and
neck cancer are 16 and 18 (14). The
prevalence of HPV16 had been estimated at 20–35%, with the highest
incidence of HPV infection noted in non-Hispanic Caucasian patients
in the United States (14). Though
young adult patients have been identified to present with similar
symptoms to older adults, they tend to exhibit shorter symptom
duration prior to diagnosis, and are more likely to be diagnosed at
an advanced stage owing to the higher rate of regional involvement
(5). OTSCC is increasingly being
regarded as a biologically different entity compared with cancer
affecting other oral sites. It is more aggressive and generally
associated with a higher rate of metastasis (15). The patient of the present study, who
already exhibited lymph node involvement with the short duration of
the symptoms, exemplified this situation.
The prognosis of OTSCC in young adults is uncertain.
Certain studies have suggested higher disease recurrence and poor
prognosis in young adults, while others have identified similar
outcomes in this patient group as compared with in older adults:
Pitman et al (16)
demonstrated that with equivalent treatment, outcomes for young
patients are analogous to those of older patients with OTSCC.
Goepfert et al (17) and
Vargas et al (18) observed
that OTSCC in young females was not associated with worse outcomes
compared with a matched cohort of other patients. This has
suggested that age may be an independent prognostic factor for
survival, as demonstrated by Garavello et al (19). The patient of the present study
received a combination of chemotherapy and radiation and did not
demonstrate any recurrence of disease during follow up. The 5-year
relative survival demonstrated by Bello et al (15) indicated an overall higher survival
rate among younger adults aged 20–44 years for OTSCC (64%) compared
with adults >45 years (51%).
Oral tongue cancer incidence, presentation and
causative factors, treatment protocol, survival and prognosis,
particularly in young adults, continue to evolve and necessitate
future studies.
Acknowledgements
The authors would like to thank Ms. Faye Jornadal,
(Nashville General Hospital at Meharry, Nashville, TN, USA), for
facilitating the acquisition of medical record information. The
Meharry Office of Scientific Editing and Publications (grant no.
NIH S21MD000104) provided formatting assistance.
References
|
1
|
Li R, Koch WM, Fakhry C and Gourin CG:
Distinct epidemiologic characteristics of oral tongue cancer
patients. Otolaryngol Head Neck Surg. 148:792–796. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Patel SC, Carpenter WR, Tyree S, Couch ME,
Weissler M, Hackman T, Hayes DN, Shores C and Chera BS: Increasing
incidence of oral tongue squamous cell carcinoma in young white
women, age 18 to 44 years. J Clin Oncol. 29:1488–1494. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
American Cancer Society, . Cancer Facts
& Figures 2012. Atlanta: American Cancer Society; 2012
|
|
4
|
Surveillance, Epidemiology and End Results
(SEER) Program (www.seer.cancer.gov) SEER*Stat Database:
Incidence-SEER 9 Regs Research Data, Nov 2015 Sub (1973-2013)
<Katrina/Rita Population Adjustment>-Linked To County
Attributes-Total U.S., 1969–2014 Counties, National Cancer
Institute, DCCPS, Surveillance Research Program. Surveillance
Systems Branch. released April 2016, based on the November, 2015
submission.
|
|
5
|
Llewellyn CD, Linklater K, Bell J, Johnson
NW and Warnakulasuriya S: An analysis of risk factors for oral
cancer in young people: A case-control study. Oral Oncol.
40:304–313. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Anaya-Saavedra G, Ramírez-Amador V,
Irigoyen-Camacho ME, García-Cuellar CM, Guido-Jiménez M,
Méndez-Martínez R and García-Carrancá A: High association of human
papillomavirus infection with oral cancer: A case-control study.
Arch Med Res. 39:189–197. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Koch WM, Lango M, Sewell D, Zahurak M and
Sidransky D: Head and neck cancer in nonsmokers: A distinct
clinical and molecular entity. Laryngoscope. 109:1544–1551. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Siebers TJ, Merkx MA, Slootweg PJ,
Melchers WJ, van Cleef P and de Wilde PC: No high-risk HPV detected
in SCC of the oral tongue in the absolute absence of tobacco and
alcohol-a case study of seven patients. Oral Maxillofac Surg.
12:185–188. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Marur S, D'Souza G, Westra WH and
Forastiere AA: HPV-associated head and neck cancer: A virus-related
cancer epidemic. Lancet Oncol. 11:781–789. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
TNM Classification of Malignant Tumours.
6th edition. Sobin LH and Wittekind Ch: John Wiley & Sons;
Hoboken, New Jersey USA: pp. 22–263. 2002
|
|
11
|
Backes FJ and Cohn DE: Lynch Syndrome.
Clin Obstet and Gynecol. 54:199–214. 2011. View Article : Google Scholar
|
|
12
|
Shia J: Immunohistochemistry versus
microsatellite instability testing for screening colorectal cancer
patients at risk for hereditary nonpolyposis colorectal cancer
syndrome. Part I. The utility of immunohistochemistry. J Mol Diagn.
10:293–300. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Randhawa T, Shameena P, Sudha S and Nair
R: Squamous cell carcinoma of tongue in a 19-year-old female.
Indian J Cancer. 45:128–130. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gillison ML: Human
papillomavirus-associated head and neck cancer is a distinct
epidemiologic, clinical, and molecular entity. Semin Oncol.
31:744–754. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bello IO, Soini Y and Salo T: Prognostic
evaluation of oral tongue cancer: Means, markers and perspectives
(II). Oral Oncol. 46:636–643. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pitman KT, Johnson JT, Wagner RL and Myers
EN: Cancer of the tongue in patients less than forty. Head Neck.
22:297–302. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Goepfert RP, Kezirian EJ and Wang SJ: Oral
tongue squamous cell carcinoma in young women: A matched
comparison-do outcomes justify treatment intensity? ISRN
Otolaryngol. 2014:1–6. 2014. View Article : Google Scholar
|
|
18
|
Vargas H, Pitman KT, Johnson JT and Galati
LT: More aggressive behavior of squamous cell carcinoma of the
anterior tongue in young women. Laryngoscope. 110:1623–1626. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Garavello W, Spreafico R and Gaini RM:
Oral tongue cancer in young patients: A matched analysis. Oral
Oncol. 43:894–897. 2007. View Article : Google Scholar : PubMed/NCBI
|