Introduction
Primary penile cancer is a rare disease. The
incidence of penile cancer is heterogeneous among different
populations; however, it is rare in most of the developed world. In
the United States, the age-standardized incidence is
0.3–1.8/100,000 population (1,2). The
incidence of penile cancer is high in developing countries,
including Uganda (2.8/100,000), and areas of Brazil
(1.5–3.7/100,000). The reasons for this are thought to be as
follows: i) A high risk of HPV infection; ii) sufficient medical
aid not performed; and iii) a high smoking rate (3). Israeli Jews show the lowest incidence in
the world (0.1/100,000). The incidence of penile cancer in Japan is
approximately 0.4/100,000; this rate is similar to the rates in
other developed countries (4).
Previous studies have suggested that human
papillomavirus (HPV) infection is associated with penile cancer
(5–7).
Oncogenic HPV infection has been well established as a major risk
factor for cervical cancer and is associated with the development
of >99% of cervical carcinomas. Although it is known that HPV
can affect the squamous epithelium of the male genitalia (similarly
to the female genital tract) the association between penile cancer
and HPV has not been completely elucidated.
Cancer tissue specimens have recently been
investigated using HPV DNA assays, including polymerase chain
reactions (PCRs) and in situ hybridization (ISH). Although
PCRs show high sensitivity in the detection of HPV DNA, there are
some disadvantages associated with using PCRs to detect HPV DNA
(8,9),
as the assay requires highly trained laboratory personnel and
strict laboratory conditions must be implemented to avoid
contamination. Moreover, the morphological context is lost when a
PCR is used.
In contrast, ISH works by directly detecting the
signals of HPV DNA and the morphological context is preserved. The
results of ISH are interpreted similarly to the results of
immunohistochemical staining. ISH signal patterns of HPV DNA have
been reported to be some correlation with the physical status of
HPV in infected cells (10). The
integration of oncogenic HPV into the human genome is a crucial
stage of cervical cancer carcinogenesis; thus, the HPV signal
pattern, which possibly suggests the viral integration status, may
be a useful marker that can be used to predict the progression of
precancerous lesions. In spite of these advantages, ISH shows low
sensitivity. For pathologists who use ISH to detect HPV in tissue,
this is a major concern (11). ISH
assays using improved signal-detecting methods, which show higher
sensitivity, including the enzyme-categorized signal detecting
system, have been developed in recent years (12).
The majority of cervical cancers (>90%) express
HPV and the HPV vaccine has an important role to play in preventing
cervical. In the present study, we performed ISH to examine the HPV
gene expression in penile cancer tissue.
Patients and methods
The study population
Forty-one cases involving patients who underwent
penectomy and 3 cases involving patients who underwent tumor
resection to treat pathologically-diagnosed penile cancer were
included in the present study. All of the patients were treated at
Yokohama City University Medical Center (Yokohama, Japan) and its 7
affiliated hospitals between April 1990 and March 2010. The primary
tumor was removed by amputation or tumor resection. Ethical
approval and consent to participate: The present study was approved
by the Institutional Review Board of Yokohama City University and
written informed consent was obtained from the patients.
Histopathological features
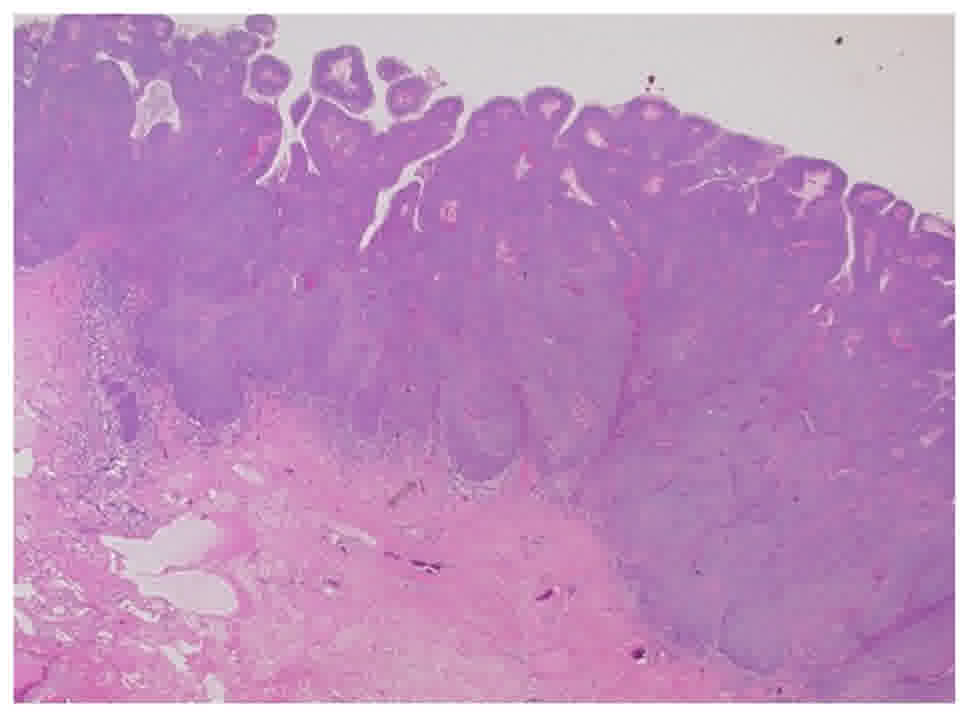
One pathologist (T.S.) performed a histological
review) using 3.5-µm-thick tissue sections that had been stained
with hematoxylin and eosin (Fig. 1).
The following pathological variables were investigated: The depth
of tumor invasion, the grade of histological differentiation, the
grade of infiltration, Broder's grade Yamamoto-Kohama (Y-K) grade,
and the presence/absence of lymphovascular embolization and
koilocytosis.
ISH
ISH was performed using tissue specimens
(thickness, 4-µm) that had been obtained during penectomy. The
sections were subjected to ISH studies with Ventana HPV III probes
(Ventana Medical Systems, Inc., Tucson, AZ, USA). The Ventana
INFORM HPV assay is able to detect both high-risk (HR) HPV (16, 18,
31, 33, 35, 45, 51, 55, 58, 59, 68, and 70) and low-risk (LR) HPV
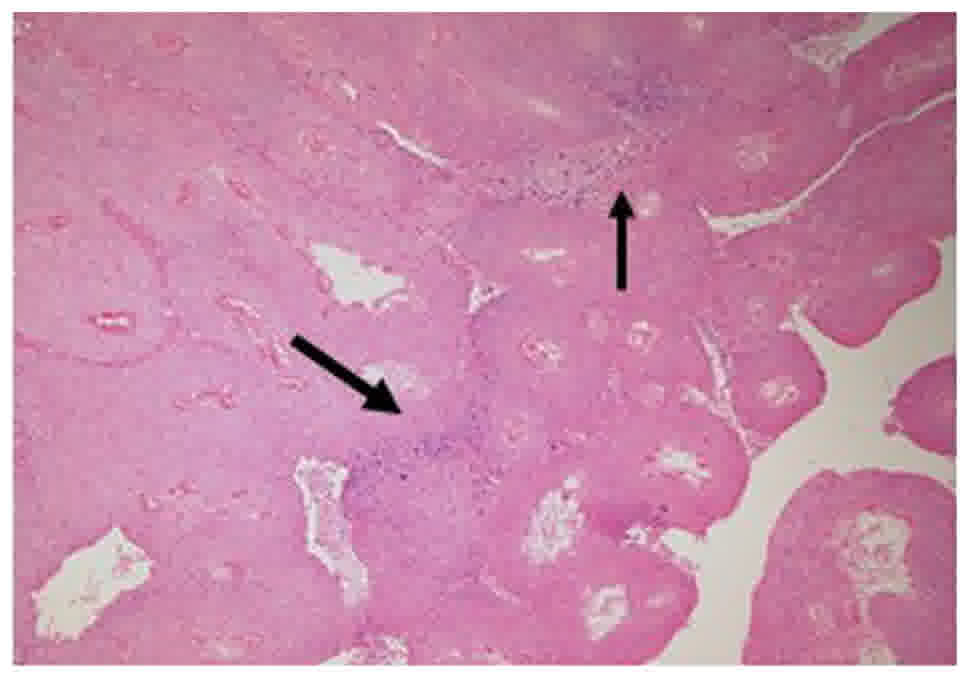
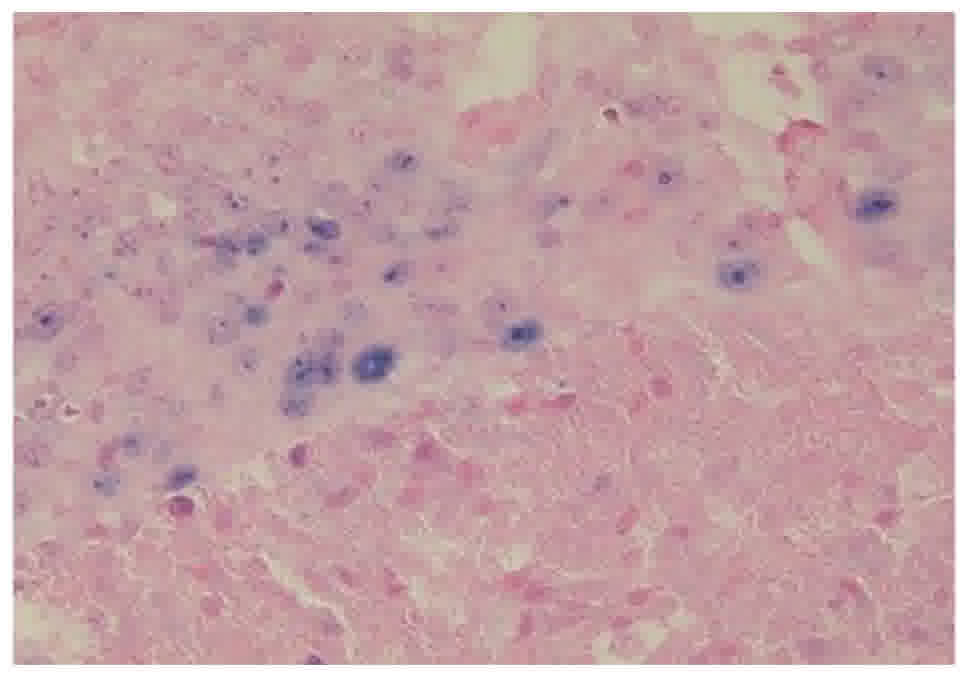
(6, 11, 42–44) types, just as with cervical cancer (13). A sandwich hybridization reaction that
consists of a fluorescein-labeled probe that is complimentary to
the HPV target, a primary biotinylated linking antibody (anti-FIC,
as well as antibiotin or antidigoxigenin), a secondary biotinylated
linking antibody, and an alkaline phosphatase conjugated avidin,
stains cells that are positive for HPV DNA with a blue color
(Figs. 2 and 3). An ISH iVIEW Blue BPlus Detection kit is
used to detect the labeling (Ventana Medical Systems, Inc.)
(8). The staining runs each included
appropriate positive and negative controls (provided by the
manufacturer).
Follow-up procedures
The follow-up procedures included a physical
examination every three months during the first 2 years, every 6
months in the third year and annually from the fourth year.
Computed tomography was performed every 6 months.
Statistical analysis
The Mann-Whitney U and chi-squared tests were
performed to analyze the patients' characteristics and preoperative
factors. Multivariate logistic regression analyses were used to
identify individual factors. The Kaplan-Meier product limit
estimator was used for the estimation of OS. The survival duration
(defined as the time between radical cystectomy and death) was
compared using a log-rank test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patients' characteristics
A total of 44 patients with penile cancer who
underwent penectomy were included in the present study. The mean
(median) age was 68.6±11.7 (69) years. The locations of the
cancerous lesions in these patients included the glans [n=32
(72.7%)], the foreskin [n=8 (18.2%)], and the body [n=4 (9.1%)].
The UICC stage classifications were as follows: Stage 1 [n=24
(54.5%)], stage 2 [n=10 (22.7%)], stage 3 [n=4 (9.1%)], and stage4
[n=6 (13.6%)]. Most of the patients were usual type, and three
patients were verrucus type. None showed basaloid or warty types.
The mean tumor size was 3.5±2.6 cm (median 3.7 cm, range 0.25–10
cm). The surgical treatments included partial penectomy [n=29
(65.9%)], total penectomy [n=12 (27.3%)], and tumor resection
preserving the penis [n=3 (6.8%)]. Inguinal canal lymph-node
resection was performed in 16 cases (36.4%) and receiver
intra-pelvic node resection was performed in two cases (4.5%).
Lymph-node resection was not performed in the other 26 cases
(59.1%). Thirteen patients (29.5%) received adjuvant chemotherapy.
Adjuvant radiation therapy was performed in 6 cases (13.6%). The
mean follow-up period was 44.1 months (median, 23.5). Fifteen cases
(34.1%) showed recurrence or progression. Nine patients (20.5%)
died due to penile cancer, 8 (18.2%) died due to other reasons, and
one patient (2.3%) survived with recurrent penile cancer; the
remaining 26 cases (59.1%) survived without recurrence. The
pathological T stage, tumor differentiation, nuclear grade, and
Broder's classification are summarized in Table I. Eighteen cases (40.9%) showed
koilocytosis. Preoperative CT revealed lymph-node metastasis in ten
cases (22.7%); the remaining 34 cases (77.3%) showed no lymph-node
swelling. Two cases (4.5%) showed distant metastasis.
 | Table I.Clinicopathological features. |
Table I.
Clinicopathological features.
|
|
| HR HPV |
|
|---|
|
|
|
|
|
|---|
| Variable | Total | Positive (n=5) | Negative (n=39) | P-value |
|---|
| Mean age (years) | 68.6±11.7 | 72.8±11.5 | 68.0±10.9 | 0.335a |
| Location |
Glans/foreskin/shaft |
Glans/foreskin/shaft |
| 0.754 |
|
| 32/8/4 | 4/1/0 | 28/7/4 |
|
| Mean size (cm) | 3.5±2.6 | 3.44±1.53 | 3.77±2.51 | 0.912a |
| T stage | T1/T2/T3/T4 | T1/T2/T3/T4 |
| 0.335 |
|
| 25/12/5/2 | 2/3/0/0 | 23/9/5/2 |
|
| Differentiation | Well/mod/poor | Well/mod/poor |
| 0.044 |
|
| 21/17/6 | 0/3/2 | 21/14/4 |
|
| Nuclear grade | G1/G2/G3 | G1/G2/G3 |
| 0.243 |
|
| 13/22/9 | 0/3/2 | 13/19/7 |
|
| Broders | G1/G2/G3/G4 | G1/G2/G3/G4 |
| 0.019 |
|
| 17/10/9/8 | 0/0/2/3 | 17/10/7/5 |
|
| Infiltration
grade | α/β/γ | α/β/γ |
| 0.406 |
|
| 8/32/4 | 0/4/1 | 8/28/3 |
|
| Y-K grade | G1/G2/G3/G4 | G1/G2/G3/G4 |
| 0.141 |
|
| 1/17/17/9 | 0/1/1/3 | 1/16/16/6 |
|
| Vascular
invasion | Yes/no | Yes/no |
| 0.055 |
|
| 11/33 | 3/2 | 8/31 |
|
| Lymph node
invasion | Yes/no | Yes/no |
| 0.367 |
|
| 4/40 | 1/4 | 3/36 |
|
| Koilocytosis | Yes/no | Yes/no |
| 0.965 |
|
| 18/26 | 2/3 | 16/23 |
|
| N stage | 0/1/2/3 | 0/1/2/3 |
| 0.177 |
|
| 34/1/5/4 | 3/0/2/0 | 31/1/3/4 |
|
ISH
Five of the 44 cases (11.4%) showed the expression
of HR HPV. None of the patients showed the expression of LR HPV
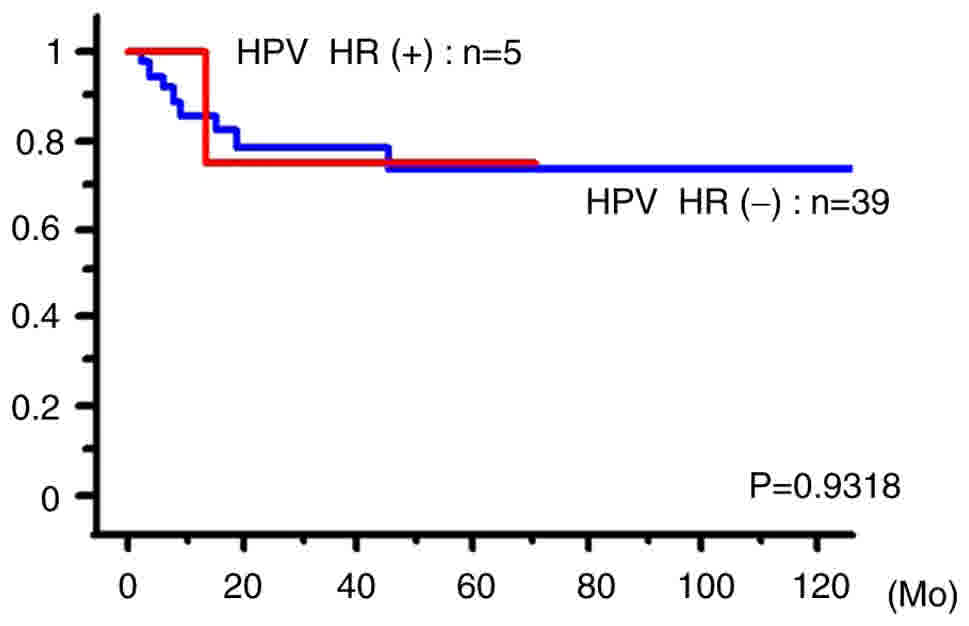
(Table I). We next examined the
correlation between the expression of HR HPV and age, tumor
location, tumor size, T stage, pathological differentiation,
nuclear grade, Broder's classification, pattern of invasion, Y-K
grade, vascular invasion, lymphoid invasion, koilocytosis, and
lymph-node metastasis. Patients with a well-differentiated status
(P=0.044) and Broder's Grade 1 (P=0.019) showed a significantly
lower rate of HPV positivity. The HPV expression was not
significantly associated with the cancer-specific survival
(P=0.932; Fig. 4).
Discussion
HPV is reportedly detectable by ISH in 30–80% of
cervical cancer cases. The rate of HPV positivity in the present
study (11.4%) was low in comparison to previous reports (14). Some possible reasons for this are as
follows: i) Japanese penile cancer patients show a lower rate of
HPV positivity; ii) an HPV genotype that is not detectable by this
kit might play a role in penile cancer; or iii) the HPV gene volume
might be lower in comparison to cervical cancer.
Histologically, the expression of HPV is thought to
be positively associated with tumor differentiation and
keratinocytosis. However, a negative association has been reported
between the HPV expression and tumor differentiation (15). The present study revealed that poorly
differentiated cancer was associated with a higher rate of HPV
positivity. Previous studies of patients with solid cancers have
also reported that patients with poorly differentiated tumors
showed a higher rate of HPV positivity. HPV expressions in reported
organs were varied by organ (Table
II) (16–25).
| Table II.Previous studies of HPV expression in
solid malignancies. |
Table II.
Previous studies of HPV expression in
solid malignancies.
| Author, year | Organ | No. of
patients | Detection
methods | HPV detectable rate
(%) | (Refs.) |
|---|
| Gillison et
al, 2000 | Head and neck | 253 | PCR, ISH | 25 | (18) |
| Li et al,
2003 | Tonsil | 86 | PCR | 46 | (19) |
| Ritchie et
al, 2003 | Oropharynx | 139 | PCR | 21 | (20) |
| Ansink et
al,1994 | Vulva | 60 | PCR | 32 | (21) |
| Bosch et
al,1997 | Cervix | 1,035 | PCR | 93 | (22) |
| ter Harmsel et
al, 1999 | Cervix | 159 | PCR | 100 | (23) |
| Wiener et
al, 1992 | Penis | 29 | PCR | 31 | (24) |
| Bezerra et
al, 2001 | Penis | 82 | PCR | 30.50 | (17) |
| Lont et al,
2006 | Penis | 171 | PCR | 29 | (16) |
| Senba et al,
2006 | Penis | 65 | PCR, ISH | ISH 53.8, PCR
81.5 | (25) |
In cervical cancer, HPV plays an important role in
cancer development and HPV vaccination is widely performed.
According to a previous report more than 90% of cervical cancer
patients are positive for HPV-DNA (26). Some reports have shown that HPV
vaccination might prevent squamous cell carcinoma in the anus,
skin, and neck (26,27). On the other hand, in cancers other
than cervical cancer, the rate of HPV positivity varies by country
and age and there is no apparent correlation between cancer
development and HPV infection (28,29). The
female sexual partners of patients with penile cancer do not have
an increased incidence of cervical cancer. At present, there is no
recommendation for the use of HPV vaccination in boys due to the
differences in the HPV-associated risk patterns in relation to
penile and anal cancer. Furthermore, the epidemiological effects of
HPV vaccination and its acceptance in girls will have to be
assessed before any further recommendations can be made (30,31).
It is not clear whether the prognosis of
HPV-associated penile cancer differs from that of
non-HPV-associated penile cancer. The 5-year disease-specific
survival of patients with HPV-positive penile cancer was reported
to be significantly better than that of HPV-negative penile cancer
(93% vs. 78%) in one study (16),
while another study reported that there was no difference in the
rates of lymph node metastasis or 10-year survival (17).
The details of the correlation between the
expression of HPV and the prognosis remain unknown. Sonpavde et
al reported that HPV-expression-positive penile cancer was
associated with a favorable outcome (32). The present study showed no significant
association between the rate of HPV expression and the outcome;
however, the study population was relatively small.
There were no significant differences in the rate of
koilocytosis. This means that koilocytosis might have been the
result of an active HR HPV infection or the presence of
koilocytosis might indicate a previous HPV infection.
In conclusion, HR HPV was detected in 5 of 44
(11.4%) penile cancer cases. LR HPV was not detected in any of the
cases. There was some correlation between the expression of HR HPV
and the tumor differentiation and keratinization (Border's
classification). The OS of the HPV-positive patients did not differ
from that of the HPV-negative patients. Although ISH using INFORM
HPVIII does not detect the HPV genotype, this method is easy to use
and might be useful for examining penile cancer tissue, as it is
for cervical cancer tissue.
Acknowledgements
Grants from KAKENHI grants (16K20152) from the
Ministry of Education, Culture, Sports, Science and Technology of
Japan and grant for 2016–2017 Research Development Fund (nos.
WJ2810) of Yokohama City University.
References
|
1
|
Lu B, Wu Y, Nielson CM, Flores R,
Abrahamsen M, Papenfuss M, Harris RB and Giuliano AR: Factors
associated with acquisition and clearance of human papillomavirus
infection in a cohort of US men: A prospective study. J Infect Dis.
199:362–371. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
da Costa WH, de Oliveira Rosa RA, Santana
TB, Benigno BS, da Cunha IW, de Cássio Zequi S, Guimaraes GC and
Lopes A: Prognostic factors in patients with penile carcinoma and
inguinal lymph node metastasis. Int J Urol. 22:669–673. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bleeker MC, Heideman DA, Snijders PJ,
Horenblas S, Dillner J and Meijer CJ: Penile cancer: Epidemiology,
pathogenesis and prevention. World J Urol. 27:141–150. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Iwasawa A, Kumamoto Y and Fujinaga K:
Detection of human papillomavirus deoxyribonucleic acid in penile
carcinoma by polymerase chain reaction and in situ
hybridization. J Urol. 149:59–63. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Giuliano AR, Nielson CM, Flores R, Dunne
EF, Abrahamsen M, Papenfuss MR, Markowitz LE, Smith D and Harris
RB: The optimal anatomic sites for sampling heterosexual men for
human papillomavirus (HPV) detection: The HPV detection in men
study. J Infect Dis. 196:1146–1152. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nielson CM, Flores R, Harris RB,
Abrahamsen M, Papenfuss MR, Dunne EF, Markowitz LE and Giuliano AR:
Human papillomavirus prevalence and type distribution in male
anogenital sites and semen. Cancer Epidemiol Biomarkers Prev.
16:1107–1114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rombaldi RL, Serafini EP, Villa LL, Vanni
AC, Baréa F, Frassini R, Xavier M and Paesi S: Infection with human
papillomaviruses of sexual partners of women having cervical
intraepithelial neoplasia. Braz J Med Biol Res. 39:177–187. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cohen C, Lawson D, Jiang J and Siddiqui
MT: Automated in situ hybridization for human papilloma
virus. Appl Immunohistochem Mol Morphol. 22:619–622. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lodde M, Mian C, Mayr R, Comploj E, Trenti
E, Melotti R, Campodonico F, Maffezzini M, Fritsche HM and Pycha A:
Recurrence and progression in patients with non-muscle invasive
bladder cancer: Prognostic models including multicolor fluorescence
in situ hybridization molecular grading. Int J Urol.
21:968–972. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hopman AH, Kamps MA, Smedts F, Speel EJ,
Herrington CS and Ramaekers FC: HPV in situ hybridization:
Impact of different protocols on the detection of integrated HPV.
Int J Cancer. 115:419–428. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pirog EC: Immunohistochemistry and in
situ hybridization for the diagnosis and classification of
squamous lesions of the anogenital region. Semin Diagn Pathol.
32:409–418. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ishida M, Ohashi S, Kizaki Y, Naito J,
Horiguchi K and Harigaya T: Expression profiling of mouse placental
lactogen II and its correlative genes using a cDNA microarray
analysis in the developmental mouse placenta. J Reprod Dev.
53:69–76. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stratton KL and Culkin DJ: A contemporary
review of HPV and penile cancer. Oncology (Williston Park).
30:245–249. 2016.PubMed/NCBI
|
|
14
|
Weaver MG, Abdul-Karim FW, Dale G,
Sorensen K and Huang YT: Detection and localization of human
papillomavirus in penile condylomas and squamous cell carcinomas
using in situ hybridization with biotinylated DNA viral
probes. Mod Pathol. 2:94–100. 1989.PubMed/NCBI
|
|
15
|
Klussmann JP, Weissenborn SJ, Wieland U,
Dries V, Eckel HE, Pfister HJ and Fuchs PG: Human
papillomavirus-positive tonsillar carcinomas: A different tumor
entity? Med Microbiol Immunol. 192:129–132. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lont AP, Kroon BK, Horenblas S, Gallee MP,
Berkhof J, Meijer CJ and Snijders PJ: Presence of high-risk human
papillomavirus DNA in penile carcinoma predicts favorable outcome
in survival. Int J Cancer. 119:1078–1081. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bezerra AL, Lopes A, Santiago GH, Ribeiro
KC, Latorre MR and Villa LL: Human papillomavirus as a prognostic
factor in carcinoma of the penis: Analysis of 82 patients treated
with amputation and bilateral lymphadenectomy. Cancer.
91:2315–2321. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gillison ML, Koch WM, Capone RB, Spafford
M, Westra WH, Wu L, Zahurak ML, Daniel RW, Viglione M, Symer DE, et
al: Evidence for a causal association between human papillomavirus
and a subset of head and neck cancers. J Natl Cancer Inst.
92:709–720. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li W, Thompson CH, Xin D, Cossart YE,
O'Brien CJ, McNeil EB, Gao K, Scolyer RA and Rose BR: Absence of
human papillomavirus in tonsillar squamous cell carcinomas from
Chinese patients. Am J Pathol. 163:2185–2189. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ritchie JM, Smith EM, Summersgill KF,
Hoffman HT, Wang D, Klussmann JP, Turek LP and Haugen TH: Human
papillomavirus infection as a prognostic factor in carcinomas of
the oral cavity and oropharynx. Int J Cancer. 104:336–344. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ansink AC, Krul MR, De Weger RA, Kleyne
JA, Pijpers H, Van Tinteren H, De Kraker EW, Helmerhorst TJ and
Heintz AP: Human papillomavirus, lichen sclerosus, and squamous
cell carcinoma of the vulva: Detection and prognostic significance.
Gynecol Oncol. 52:180–184. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bosch FX, Muñoz N and de Sanjosé S: Human
papillomavirus and other risk factors for cervical cancer. Biomed
Pharmacother. 51:268–275. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
ter Harmsel B, Smedts F, Kuijpers J, van
Muyden R, Oosterhuis W and Quint W: Relationship between human
papillomavirus type 16 in the cervix and intraepithelial neoplasia.
Obstet Gynecol. 93:46–50. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wiener JS, Effert PJ, Humphrey PA, Yu L,
Liu ET and Walther PJ: Prevalence of human papillomavirus types 16
and 18 in squamous-cell carcinoma of the penis: A retrospective
analysis of primary and metastatic lesions by differential
polymerase chain reaction. Int J Cancer. 50:694–701. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Senba M, Kumatori A, Fujita S,
Jutavijittum P, Yousukh A, Moriuchi T, Nakamura T and Toriyama K:
The prevalence of human papillomavirus genotypes in penile cancers
from northern Thailand. J Med Virol. 78:1341–1346. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Muñoz N, Bosch FX, de Sanjosé S, Herrero
R, Castellsagué X, Shah KV, Snijders PJ and Meijer CJ:
International Agency for Research on Cancer Multicenter Cervical
Cancer Study Group: Epidemiologic classification of human
papillomavirus types associated with cervical cancer. N Engl J Med.
348:518–527. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Furihata M, Inoue K, Ohtsuki Y, Hashimoto
H, Terao N and Fujita Y: High-risk human papillomavirus infections
and overexpression of p53 protein as prognostic indicators in
transitional cell carcinoma of the urinary bladder. Cancer Res.
53:4823–4827. 1993.PubMed/NCBI
|
|
28
|
Philippou P, Shabbir M, Ralph DJ, Malone
P, Nigam R, Freeman A, Muneer A and Minhas S: Genital lichen
sclerosus/balanitis xerotica obliterans in men with penile
carcinoma: A critical analysis. BJU Int. 111:970–976. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
D'Hauwers KW, Depuydt CE, Bogers JJ, Noel
JC, Delvenne P, Marbaix E, Donders AR and Tjalma WA: Human
papillomavirus, lichen sclerosus and penile cancer: A study in
Belgium. Vaccine. 30:6573–6577. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Newman PA, Logie CH, Doukas N and Asakura
K: HPV vaccine acceptability among men: A systematic review and
meta-analysis. Sex Transm Infect. 89:568–574. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Fisher H, Trotter CL, Audrey S,
MacDonald-Wallis K and Hickman M: Inequalities in the uptake of
human papillomavirus vaccination: A systematic review and
meta-analysis. Int J Epidemiol. 42:896–908. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sonpavde G, Pagliaro LC, Buonerba C, Dorff
TB, Lee RJ and Di Lorenzo G: Penile cancer: Current therapy and
future directions. Ann Oncol. 24:1179–1189. 2013. View Article : Google Scholar : PubMed/NCBI
|