As a common cancer and the leading cause of
cancer-associated mortality, lung cancer has always been
universally associated with poor patient prognosis (1). The incidence and mortality rates of lung
cancer occupy the first or second position in malignant tumors in
China and the United States (2,3). Until
2015, the 5-year total survival rate for lung cancer was ≤20% in
developed and developing countries (4). Between 40 and 50% of patients present
with distant metastases upon diagnosis with lung cancer have a poor
5-year survival rate of <5% (1).
Small cell lung cancer accounts for only 10% of lung cancer but
non-small cell lung cancer accounts for ~90%, including squamous
cell carcinoma, adenocarcinoma, large cell carcinoma, adenosquamous
carcinoma and sarcomatoid carcinoma (4).
As demonstrated in autopsy studies, lung cancer
metastases may be identified in every organ system (4). However, the gastrointestinal (GI) tract
is not a common site of metastasis for primary lung cancer when
compared with other sites, including bone, brain, liver and adrenal
glands (5). Gastrointestinal
metastases of lung cancer (GMLC) was caused by hematogenous spread
and occurred at the end-stage of lung cancer. The incidence of GMLC
was <2% in clinical studies, which was much lower compared with
its prevalence identified during autopsies (5–8). In
previous studies, GMLC was described primarily in case reports.
Systemic survival analyses and association between
clinicopathological factors, therapeutic factors and GI
complications were seldom discussed. The present study reviewed
>130 studies from the last 50 years and analyzed 366 cases of
GMLC to reveal its clinical and prognostic characteristics by
univariate and multivariate survival analyses.
The histological classification of primary lung
cancer was performed according to the 2004 World Health
Organization classification system of lung tumors (134). The Tumor-Node-Metastasis staging was
performed according to the 7th edition of the 2010 American Joint
Committee on Cancer Staging manual (135). The histological distribution data of
primary lung cancer was acquired from the International Lung Cancer
Consortium (136).
Squamous cell carcinoma (28.5%), adenocarcinoma
(27.6%) and large cell carcinoma (20.9%) were the three most common
histological types of GMLC. When the histological distributions
between GMLC and primary lung cancer were compared, it was observed
that there was an increased frequency of GMLC of large cell
carcinoma, small cell lung cancer and squamous cell carcinoma
compared with GMLC of adenocarcinoma and other types of cancer
(P<0.01; Table II).
The association between involved organs,
histological type and GI complications is presented in Table III. Perforation of the small
intestine (63.7%) occurred more frequently compared with
perforation of stomach and colorectum (P<0.001). The organs at
risk of hemorrhage, from most to least common, were the stomach,
colorectum and small intestine (P<0.05 in comparisons between
two organs). No obstruction occurred in all 36 patients with
gastric metastasis, and the incidence of obstruction was much lower
compared with colorectum (P=0.003) or small intestine (P=0.003). In
all the histological types of lung cancer analyzed, sarcomatoid
carcinoma exhibited the lowest likelihood of perforation and the
greatest likelihood of hemorrhage (P<0.05). The risks of
perforation of squamous cell carcinoma and small cell lung cancer
were increased compared with the risks associated with
adenocarcinoma (P<0.05). The risks of hemorrhage of squamous
cell carcinoma and small cell lung cancer were lower compared with
the risks for large cell carcinoma (P<0.05). No statistically
significant difference was observed between two other organs or
histological types (P>0.05). No significant association was
identified between histological type and GI obstruction
(P>0.05).
In total, there were 35 cases for which
immunohistochemical data were available. Information from this
limited number of cases illustrated that a typical
immunohistochemical staining of GMLC was positive for thyroid
transcription factor-1 (TTF-1; 84.4%, 27/32) and cytokeratin 7
(CK7, 96.6%, 28/29), but negative for CK20 (96.6%, 28/29) and
caudal-related homeodomain transcription 2 (CDX2, 100%, 23/23).
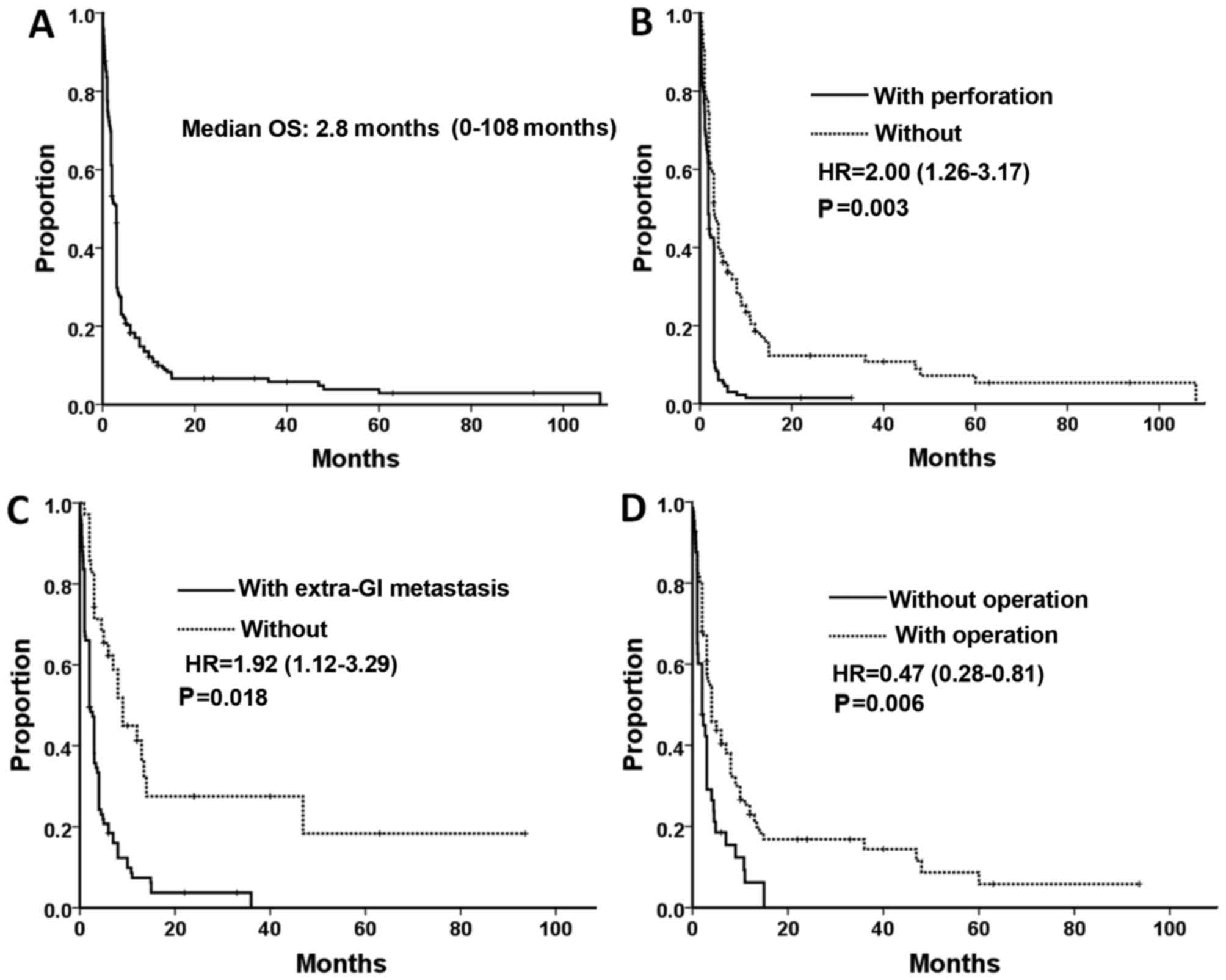
Survival rate data was available for 268 of the 366
patients studied. A total of 246 patients had succumbed to disease
by the end of the duration of the study, and the data of the other
22 patients were censored data. The median OS time was 2.8 months
(range, 0–108 months, Fig. 1A).
Univariate Cox analysis (Table V)
revealed that patients from the Americas exhibited poorer prognoses
compared with patients from Asia (P<0.001). It was also
indicated that the survival rates for patients with small cell lung
cancer and sarcomatoid carcinoma were increased compared with
patients with squamous cell carcinoma (unadjusted hazard ratios
(HRs), 0.62 (P=0.03) and 0.34 (P=0.005), respectively). The other
prognostic factors, which indicate a poor survival outcome,
included synchronous metastasis, perforation of GMLC, extra-GI
metastasis and lack of abdominal surgery (P<0.05). Patients with
multiple metastases exhibited marginal poorer prognoses compared
with patients with solitary metastases (P=0.06). There were no
statistical significance between overall survival rate and other
factors, (sex, age, organs of GI metastasis, and surgery on the
primary lung cancer) (P>0.05).
In multivariate analysis, following adjustment for
prognostic factors, the region where the patients were from,
histological type, GI perforation, extra-GI metastasis and
abdominal surgery remained prognostic factors for survival rate.
Other factors were not significant (Table
V; Fig. 1B-D).
As the digestive tract remains a rare site of
metastasis of primary lung cancer, GMLC was previously described
primarily in case reports (8). The
clinical incidence of GMLC was <2% in patients with primary lung
cancer and >10% in autopsy-associated studies (5–8). The
majority of GMLC cases occurred at the end-stage of lung cancer,
and misdiagnosis and missed diagnosis occurred frequently (138). In the present study, the sex and age
of the patients with GMLC was similar with cases reported in
previous studies with small sample sizes (7,8). In the
present study, the majority of the patients were elderly men.
The intestines, particularly the small intestine,
were the main organs involved in GMLC, owing to their abundant
blood supply. There were certain patients that presented with
metastases in multiple GI organs, due to the lethality of the first
involved organ and the involvement of additional GI organs. On
account of the significant difference between the GMLC incidences
from clinical and autopsy-associated studies, the majority of the
patients with GMLC were subclinical with minimal or no symptoms.
The symptoms of GMLC always appeared alongside clinical
complications, including GI perforation, hemorrhage and
obstruction. The incidence of severe complications differed between
organs due to differences in individual anatomical structures of
the organs. Previous studies (129,132,139)
reported that the incidence of perforation in the small intestine
was markedly increased compared with the incidence in the
colorectum. The present study indicated similar findings. The
probability and quantity of hemorrhage may depend on the incubation
time of GMLC and the inner diameter of the involved organ.
Metastases are able to grow for a longer period of time in the
large gastric cavity, leading to more bleeding in the stomach
compared with other organs. In the present study, no obstruction
was identified in the stomach, and it was hypothesized that this
may be associated with the wider inner diameter of the stomach
compared with other GI organs.
In the present study, >3/4 of GMLC cases analyzed
were squamous cell carcinoma, adenocarcinoma and large cell
carcinoma. The high incidence of squamous cell carcinoma and
adenocarcinoma was due to their high prevalence in primary lung
cancer. The highest risk of GI metastasis was identified in large
cell carcinoma, whereas the lowest risk of all the major
histological types of GI metastasis was identified in
adenocarcinoma. This finding is partly consistent with the autopsy
data from Antler et al (6). On
the other hand, different histological types of lung cancer exhibit
different GI complications. A previous study on metastasis in the
small intestine indicated that large cell carcinoma is associated
with the greatest likelihood of perforation, whereas adenocarcinoma
is most closely associated with the lowest rate of perforation in
all the histological types (69). The
present study partly confirmed this result and suggested that
sarcomatoid carcinoma was associated with a lower rate of
perforation and a greater rate of hemorrhages of the GI tract
(Table III). This may be due to the
relatively compact structure of sarcomatoid carcinoma with its
differentiation of connective tissues. A number of previous studies
(112,140) have suggested that GI perforation may
be caused by chemotherapy, but other studies (106,141)
indicated that GI perforation is brought about mainly by ischemia
and necrosis of metastases, obstruction and high pressure in the GI
cavity. In the present study, in which only a quarter of the total
studies contained data on GI perforation, patients with or without
chemotherapy experience statistically similar incidences of
perforation and obstruction. The risk of hemorrhage may be
decreased by chemotherapy, which may lead to tumor atrophy and
ischemia.
The diagnosis of GMLC is not easy owing to its
non-specific symptoms, although its complications are well known.
When patients with lung cancer complain of potential GMLC symptoms
(abdominal pain, nausea, vomiting, anemia, hematochezia, melena,
constipation or other changes in bowel habits), particularly those
that cannot be explained by primary lung cancer or undergoing
chemotherapy or radiotherapy treatment, GMLC should be considered.
As part of systemic metastases, GMLC is caused by hematogenous
dissemination (8). In previous
studies (88,141), 42.9–100.0% of the patients with GMLC
had extra-GI metastasis, and this ratio was 70.5% in the present
study. Therefore, it is necessary for patients with GMLC to undergo
sufficient evaluations prior to initiation of treatment (142). On the other hand, it was reported
that GMLC was more common in patients with metastases in adrenal
glands, kidneys and celiac lymph nodes compared with in patients
with other type of metastases (5).
However, this finding was not supported by the data in the present
study.
Laboratory examination, endoscopy,
gastroenterography, computed tomography (CT) and positron-emission
tomography (PET)-CT may aid the diagnosis of GMLC (120). In a study by Kim et al
(141) on the signs of GMLC in CT,
it was reported that positive signs could be identified in 93% of
patients, including localized GI wall thickening, the presence of a
mass in the GI cavity, regional glandular enlargement, indigitation
and perforation. PET-CT was able to assist the detection of
subclinical GMLC and systemic evaluation of extra-GI metastases
(133,143,144).
Pathology was a critical factor in diagnosis. The pathology of
primary lung cancer should be reviewed and compared with that of
GMLC. In the present study, in the majority of cases of GMLC
considered, there was positive immunohistochemical staining for
thyroid transcription factor 1 and cytokeratin-7 but negative
staining for CK20 and CDX2, which was consistent with a previous
study (8).
As the end-stage of lung cancer, GMLC was always
associated with a poor prognosis (69). In the present study, the median OS
time was 2.8 months and 53.4% of the patients succumbed to disease
within 3 months of diagnosis of GMLC. Only 9.0% (24/268) of
patients were reported to survive for >1 year and 2 patients
(0.7%) with large cell carcinoma survived >7 years. Patients in
the dataset analyzed by the present study generally exhibited
longer overall survival times compared with patients assessed by
Garwood et al (69). The
patients that Garwood et al (69) studied are part of the present dataset.
All patients in the study by Garwood et al (69) exhibited perforation of the small
intestine, which appears to be associated with shorter OS (based on
comparisons between the results of the present study and Garwood
et al) (69). In the present
study, there were five factors, including region, histological
type, GI perforation, extra-GI metastasis and surgical resection,
which formed the final components included in the multivariate Cox
model. Although it was indicated that the survival times for Asian
patients were longer compared with American patients, region was
not a useful factor in determining survival times as American
studies assessed in the present study were undertaken on average
~20 years earlier compared with the studies from Asia. With an
adjusted hazard ratio of 5.57 (P=0.002), it was indicated that
patients with adenosquamous carcinoma had a significantly poorer
prognosis compared with patients with squamous cell carcinoma based
on multivariate Cox analysis. However, only four cases of
adenosquamous carcinoma were available in the present survival
analysis, so this result is of limited value. Perforation of GMLC
and extra-GI metastasis were indicated to be negative prognostic
factors, but abdominal surgery appeared to be a positive prognostic
factor. However, the selective bias of the patients, particularly
in treatment choice, must be considered in the present
retrospective study. The patients with less severe general
conditions were more likely to undergo surgery than those in
critical conditions.
The present study revealed that, due to the
increasing incidence of lung cancer, as well as the ability of
modern medicine to prolong the life of lung cancer patients, GMLC
is no longer rare. On the basis of the assessment performed in the
present study, the histological distribution of GMLC was different
from that of primary lung cancer. Early detection, diagnosis and
treatment are central to improving patient prognosis. Sufficient
and careful evaluations, targeted surgeries and systemic therapies
for specific patients following discussion between
multi-disciplinary teams of medics are able to improve the survival
rate and quality of life of patients (138,145).
The main purpose of surgery is to relieve symptoms while causing
the least trauma possible to the patient. Data from the present
study revealed that >30% of the patients had multiple metastases
in their GI tract, therefore careful investigations during the
surgery are required to avoid subclinical metastases being
missed.
The present study was funded by grants from the
Natural Science Foundation of Zhejiang Province of China (nos.
LY14H160030 and LY13H160011), the National Program on Key Basic
Research Project of China (973 Program; no. 2014CB542003), the
National Natural Science Foundation of China (no. 30801341) and the
Zheng Shu Elite Scholarship for Clinical Medicine.
|
1
|
Mao Y, Yang D, He J and Krasna MJ:
Epidemiology of Lung Cancer. Surg Oncol Clin N Am. 25:439–445.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Frank CD, Roy HD, Lynn T and Rogerio CL:
Non-small Cell Lung CancerDeVita, Hellman and Rosenberg's Cancer:
Principles & Practice of Oncology. 10th Edition. Wolters Kluwer
Health Corp.; Philadelphia: pp. 495–502. 2015
|
|
5
|
Yoshimoto A, Kasahara K and Kawashima A:
Gastrointestinal metastases from primary lung cancer. Eur J Cancer.
42:3157–3160. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Antler AS, Ough Y, Pitchumoni CS, Davidian
M and Thelmo W: Gastrointestinal metastases from malignant tumors
of the lung. Cancer. 49:170–172. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang CJ, Hwang JJ, Kang WY, Chong IW, Wang
TH, Sheu CC, Tsai JR and Huang MS: Gastro-intestinal metastasis of
primary lung carcinoma: clinical presentations and outcome. Lung
Cancer. 54:319–323. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rossi G, Marchioni A, Romagnani E,
Bertolini F, Longo L, Cavazza A and Barbieri F: Primary lung cancer
presenting with gastrointestinal tract involvement:
Clinicopathologic and immunohistochemical features in a series of
18 consecutive cases. J Thorac Oncol. 2:115–120. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chongbo S and Gaojia Z: A case report of
small intestinal metastasis of lung cancer. Chin J Clin Oncol.
20:3191993.(In Chinese).
|
|
10
|
Zhiqiang C and Chenghai Z: Lung cancer
with its first symptom of gastrointestinal hemorrhage: a case
report. J Jinan Univ (Med Ed). 17:1321996.(In Chinese).
|
|
11
|
Yuyuan Y: Bowel obstruction caused by
colonic metastasis of squamous cell lung cancer: a case report.
Chin J Cancer. 18:1431999.(In Chinese).
|
|
12
|
Jianguo S, Xiufeng Z and Qingmei J: A case
report of rectal metastasis of small cell lung cancer. Chin J
Cancer Prev Treat. 7:3692000.(In Chinese).
|
|
13
|
Jun Q, Wenyong S, Dechuan L, Rongcan L and
Guiquan L: A case report of lung cancer with right colonic
metastasis. J Coloproctol Surg. 7:492001.(In Chinese).
|
|
14
|
Xiaoqiang L, Delong Z, Yimeng Z and
Chunbao Z: Gastric metastasis of primary lung cancer: one case
report. Suzhou Med. 24:1602001.(In Chinese).
|
|
15
|
Xiaoning C, Jinlong C and Shilian Z: Bowel
obstruction caused by ileum metastasis of lung cancer: a case
report. Chin J Prim Med Pharm. 9:7952002.(In Chinese).
|
|
16
|
Xin T, Wang W, Xu Y, Yang Y, Hao W and Li
Y: A case report of rectal metastasis of lung cancer. Zhongguo Fei
Ai Za Zhi. 5:4572002.(In Chinese).
|
|
17
|
Jinlin L and Xiaoming L: Jejunal
metastasis of lung cancer: one case report. J Abdom Surg.
15:592002.
|
|
18
|
Hui C, Yaoguang L and Yin L: A case report
of gastric metastasis of lung cancer. J Guangxi Med Univ.
21:7662004.(In Chinese).
|
|
19
|
Huili Z and Hanmeng Y: Bowel idigitation
caused by intestinal metastasis of lung cancer: one case report.
Med J CASC. 6:352004.
|
|
20
|
Yan L and Chongqin Y: Ileum metastasis of
lung adenocarcinoma: a case report. Chin J Geriatr. 24:382–383.
2005.
|
|
21
|
Xiangtao M, Liwei Y, Jing F, Shan W, Ruyi
D and Zhirong C: A case report of colonic metastasis of
undifferentiated lung cancer. Chin J Clin Oncol. 33:3582006.(In
Chinese).
|
|
22
|
Xiangtao M, Liwei Y, Jing F, Shan W, Ruyi
D and Zhirong C: Colonic metastasis of squamous cell lung cancer: a
case report and review. Cancer Res Prev Treat. 33:6312006.
|
|
23
|
Yong L, Yuguo H, Yongcan L, Hongzhe Y and
Fengxia J: A case of colonic metastasis of lung cancer. Chin J
Thorac Cardiovasc Surg. 23:1132007.
|
|
24
|
Jianzhong D, Pin Z and Yi W: A case of
multiple bowel perforations caused by jejunum metastasis of lung
cancer. Chin J Surg. 46:772008.(In Chinese).
|
|
25
|
Lixia L and Weimin Z: Small intestinal
metastasis of lung cancer: a case report. J Prac Med.
24:38532008.
|
|
26
|
Xuan W, He H, Muyan C, Liping L, Yuanyuan
Z and Li Z: Small intestinal metastasis of non-small cell lung
cancer: Case report and literature review. Chin J Cancer.
27:447–448. 2008.(In Chinese).
|
|
27
|
Wei H, Baojin H and Weiru X: A case report
of gastric metastasis of primary lung cancer. Chin J Oncol.
30:6982008.(In Chinese).
|
|
28
|
Yingman W, Xiangmin L and Haixia Z: Small
intestinal metastasis of lung cancer: case report and literature
review. J Fourth Mil Med Univ. 30:962009.
|
|
29
|
Qian L, JIangyang L, Xiaohong W, Yi Y and
Lin L: Clinical and pathological analysis of lung giant cell
carcinoma with neuroendocrine differentiation metastatic to small
intestine. J Diag Pathol. 16:100–103. 2009.
|
|
30
|
Miao Z, Li R and Guangqin Z: A case of
gastrointestinal haemorrhage caused by small intestinal metastasis
of squamous cell lung cancer. Med J Chin PAPF. 21:605–606.
2010.
|
|
31
|
Fenghui Z and Yunping Z: A case of choroid
membrane and rectal metastasis of lung cancer. Chin J Clin Oncol.
37:8782010.(In Chinese).
|
|
32
|
Liu Y, Zhang L, Han X and Zhou T: A case
report and literature review of small intestinal metastasis of
large cell lung cancer. Zhongguo Fei Ai Za Zhi. 13:655–658.
2010.(In Chinese). PubMed/NCBI
|
|
33
|
Zhidong L, Weijun Z, Funan L, Yimin D and
Jixian S: Bowel perforation caused by colonic metastasis of small
cell lung cancer: a case report. J Basic Clin Oncol. 23:451–452.
2010.
|
|
34
|
Mo S, Lei D, Wei J, Bin Y and Hongjiang W:
Bowel indigitation caused by small intestinal metastasis of lung
cancer. J Dalian Med Univ. 32:374–375. 2010.
|
|
35
|
Lei Y, Xishan W, Xinshu D and Li L:
Multiple small intestinal metastasis of lung cancer. Chin J Oncol.
32:5252010.(In Chinese).
|
|
36
|
Wang Y, An T, Yang L, Wang Z, Zhuo M, Duan
J, Wang J and Wu M: Primary lung cancer with gastrointestinal
metastasis: 2 case report and literature review. Zhongguo Fei Ai Za
Zhi. 14:278–280. 2011.(In Chinese). PubMed/NCBI
|
|
37
|
Wu W, Mu J, Tong L and Liu Z: Primary lung
squamous cell carcinoma ileocecal metastasis: one case report and
literature review. Int J Respir. 31:1225–1227. 2011.
|
|
38
|
Xu L, Zijun L, Yahuan G and Juntao Y:
Esophagus metastasis of mucoepidermoid lung carcinoma: case report
and literature review. Cancer Res Prev Treat. 38:14622011.
|
|
39
|
Hong Z, Xiaojing L and Honglin W: Duodenal
metastases from primary squamous cell carcinoma of the lung: one
case report. J Chin Oncol. 18:319–320. 2012.(In Chinese).
|
|
40
|
Junni C, Bo Y, Yanli Z, Jie L and Fen W:
Gastric metastasis of primary lung cancer: one case report
Guangdong. Med J. 33:13692012.
|
|
41
|
Pezzuto A, Mariotta S, Fioretti F and
Uccini S: Metastasis to the colon from lung cancer presenting with
severe hyponatremia and dyspnea in a young male: A case report and
review of the literature. Oncol Lett. 5:1477–1480. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Huang YM, Hsieh TY, Chen JR, Chien HP,
Chang PH, Wang CH and Huang JS: Gastric and colonic metastases from
primary lung adenocarcinoma: A case report and review of the
literature. Oncol Lett. 4:517–520. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sakai H, Egi H, Hinoi T, Tokunaga M,
Kawaguchi Y, Shinomura M, Adachi T, Arihiro K and Ohdan H: Primary
lung cancer presenting with metastasis to the colon: A case report.
World J Surg Oncol. 10:1272012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hsing CT, Kim HY, Lee JH, Han JS, Lee JH,
Chang JS, Choi SR and Jeong JS: Gastrointestinal metastasis from a
primary adenocarcinoma of the lung presenting with acute abdominal
pain. Korean J Gastroenterol. 59:382–385. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pratto D, Resial M, Wulfson A, Gennaro M,
Brarda M and Schmidt A: Jejuno-jejunal intussusception as
presentation of a primary lung carcinoma: a case report. Acta
Gastroenterol Latinoam. 42:50–52. 2012.(In Chinese). PubMed/NCBI
|
|
46
|
Cedres S, Mulet-Margalef N, Montero MA,
Martinez P, Martinez A and Felip E: Rectal metastases from squamous
cell carcinoma: A case report and review of the literature. Case
Rep Med. 2012:9475242012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Lee PC, Lo C, Lin MT, Liang JT and Lin BR:
Role of surgical intervention in managing gastrointestinal
metastases from lung cancer. World J Gastroenterol. 17:4314–4320.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Fujiwara A, Okami J, Tokunaga T, Maeda J,
Higashiyama M and Kodama K: Surgical treatment for gastrointestinal
metastasis of non-small-cell lung cancer after pulmonary resection.
Gen Thorac Cardiovasc Surg. 59:748–752. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Salemis NS, Nikou E, Liatsos C, Gakis C,
Karagkiouzis G and Gourgiotis S: Small bowel perforation secondary
to metastatic non-small cell lung cancer. A rare entity with a
dismal prognosis. J Gastrointest Cancer. 43:391–395. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yamada H, Akahane T, Horiuchi A, Shimada
R, Shibuya H, Hayama T, Nozawa K, Ishihara S, Matsuda K and
Watanabe T: A case of lung squamous cell carcinoma with metastases
to the duodenum and small intestine. Int Surg. 96:176–181. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ceretti AP, Goi G, Barabino M, De Nicola
E, Strada D, Bislenghi G and Opocher E: Colonic metastasis from
primary carcinoma of the lung. Case report. Ann Ital Chir.
82:229–232. 2011.(In Italian). PubMed/NCBI
|
|
52
|
Bugiantella W, Cavazzoni E, Graziosi L,
Valiani S, Franceschini MS and Donini A: Small bowel metastasis
from lung cancer: A possible cause of acute abdomen. Case report
and literature review. G Chir. 32:120–122. 2011.PubMed/NCBI
|
|
53
|
Lin HC, Yu CP, Lin HA and Lee HS: A case
of lung cancer metastasized to the gastrointestinal anastomosis
site where the primary gastric cancer was resected 17 years ago.
Lung Cancer. 72:255–257. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Azevedo CR, Cezana L, Moraes ES, Begnami
MD, Junior Paiva TF, Dettino AL and Fanelli MF: Synchronous thyroid
and colon metastases from epidermoid carcinoma of the lung: Case
report. Sao Paulo Med J. 128:371–374. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Trouillet N, Robert B, Charfi S, Bartoli
E, Joly JP and Chatelain D: Gastric metastases. An endoscopic
series of ten cases. Gastroenterol Clin Biol. 34:305–309. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Guerin E, Gilbert O and Dequanter D: Acute
abdomen: A rare presentation of lung cancer metastasis. Case Rep
Med. 2009:9038972009. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Koch B, Tannapfel A, Vieth M and Grun R:
Gastric metastasis from small cell lung cancer. Pneumologie.
63:585–587. 2009.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Yun IS, Lee JY, Lee JS, Lee JY, Byun JM,
Kim EJ, Park JY and Park JK: Jejunal intussusception with
gastrointestinal bleeding caused by metastatic lung cancer. Korean
J Gastroenterol. 51:377–380. 2008.(In Koren). PubMed/NCBI
|
|
59
|
Aokage K, Yoshida J, Ishii G, Takahashi S,
Sugito M, Nishimura M, Ochiai A and Nagai K: Long-term survival in
two cases of resected gastric metastasis of pulmonary pleomorphic
carcinoma. J Thorac Oncol. 3:796–799. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Kim MS, Kook EH, Ahn SH, Jeon SY, Yoon JH,
Han MS, Kim CH and Lee JC: Gastrointestinal metastasis of lung
cancer with special emphasis on a long-term survivor after
operation. J Cancer Res Clin Oncol. 135:297–301. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Goh BK, Yeo AW, Koong HN, Ooi LL and Wong
WK: Laparotomy for acute complications of gastrointestinal
metastases from lung cancer: Is it a worthwhile or futile effort?
Surg Today. 37:370–374. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Kostakou C, Khaldi L, Flossos A,
Kapsoritakis AN and Potamianos SP: Melena: A rare complication of
duodenal metastases from primary carcinoma of the lung. World J
Gastroenterol. 13:1282–1285. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Ohashi K, Kiura K, Takigawa N, Mizushima
T, Ino H, Tabata M, Ueoka H and Tanimoto M: Successful treatment of
a patient with gastric and duodenal metastases from large cell
carcinoma of the lung with carboplatin and gemcitabine. Anticancer
Res. 26:4695–4696. 2006.PubMed/NCBI
|
|
64
|
Karamouzis MV, Linardou H, Papadopoulos G,
Bousboukea E, Kanaloupiti D, Bitza M, Spourlis N and Bafaloukos D:
Gastrointestinal solitary metastases from squamous cell lung
cancer. Lung Cancer. 55:251–252. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Kanemoto K, Kurishima K, Ishikawa H,
Shiotani S, Satoh H and Ohtsuka M: Small intestinal metastasis from
small cell lung cancer. Intern Med. 45:967–970. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Casella G, Di Bella C, Cambareri AR, Buda
CA, Corti G, Magri F, Crippa S and Baldini V: Gastric metastasis by
lung small cell carcinoma. World J Gastroenterol. 12:4096–4097.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Altintas E, Sezgin O, Uyar B and Polat A:
Acute upper gastrointestinal bleeding due to metastatic lung
cancer: An unusual case. Yonsei Med J. 47:276–277. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Miyazaki K, Satoh H and Sekizawa K:
Metastasis to appendix from lung adenocarcinoma. Int J Gastrointest
Cancer. 36:59–60. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Garwood RA, Sawyer MD, Ledesma EJ, Foley E
and Claridge JA: A case and review of bowel perforation secondary
to metastatic lung cancer. Am Surg. 71:110–116. 2005.PubMed/NCBI
|
|
70
|
Morgan MW, Sigel B and Wolcott MW:
Perforation of a metastatic carcinoma of the jejunum after cancer
chemotherapy. Surgery. 49:687–689. 1961.PubMed/NCBI
|
|
71
|
Tillotson PM and Douglas RG Jr: Metastatic
tumor of the small intestine. Three cases presenting unusual
clinical and roentgenographic findings. Am J Roentgenol Radium Ther
Nucl Med. 88:702–706. 1962.PubMed/NCBI
|
|
72
|
Hayashi K, Masuoka S and Kitade F: A case
report of perforation of intestinal metastasis of lung cancer.
Nihon Geka Hokan. 34:816–819. 1965.(In Japanese). PubMed/NCBI
|
|
73
|
Wootton DG, Morgan SC and Hughes RK:
Perforation of a metastatic bronchogenic carcinoma to the jejunum.
Ann Thorac Surg. 3:57–59. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Wellmann KF, Chafiian Y and Edelman E:
Small bowel perforation from solitary metastasis of clinically
undetected pulmonary giant cell carcinoma. Am J Gastroenterol.
51:145–150. 1969.PubMed/NCBI
|
|
75
|
Midell AI and Lochman DJ: An unusual
metastatic manifestation of a primary bronchogenic carcinoma.
Cancer. 30:806–809. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Inalsingh CH, Hazra T and Prempree T:
Unusual metastases from carcinoma of the lung. J Can Assoc Radiol.
25:242–244. 1974.PubMed/NCBI
|
|
77
|
Ramanathan T, Skene-Smith H, Singh D and
Sivanesan S: Small intestinal perforation due to secondaries from
Bronchogenic carcinoma. Br J Dis Chest. 70:121–124. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Winchester DP, Merrill JR, Victor TA and
Scanlon EF: Small bowel perforation secondary to metastatic
carcinoma of the lung. Cancer. 40:410–415. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Ejeckam GC, Abele R, Thomas J and Heringer
R: Abdominal crisis due to metastasizing lung carcinoma to the
small bowel. Can J Surg. 22:351–353. 1979.PubMed/NCBI
|
|
80
|
Sternberg A, Giler S, Segal I, Shmuter Z
and Kott I: Small bowel perforation as the presenting symptom of
squamous cell carcinoma of the lung. Clin Oncol. 6:181–186.
1980.PubMed/NCBI
|
|
81
|
Leidich RB and Rudolf LE: Small bowel
perforation secondary to metastatic lung carcinoma. Ann Surg.
193:67–69. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Rosencrans DL: Small bowel perforation
caused by metastatic lung carcinoma. Ann Surg.
197:1201983.PubMed/NCBI
|
|
83
|
Quero Hernandez J, Tabernero Zubieta J,
Martin Moreno A, Morales Caballero T, de la Higuera Torres-Puchol
J, Parra Miras F and de la Higuera Rojas J: Pulmonary large-cell
carcinoma with multiple metastases in the small intestine. Rev Clin
Esp. 165:285–286. 1982.PubMed/NCBI
|
|
84
|
Catrambone G, Pesce L, Mazza M and Iurilli
L: Perforation of the small intestine secondary to metastasis of
pulmonary carcinoma. Minerva Chir. 38:55–59. 1983.PubMed/NCBI
|
|
85
|
Nicolosi A, Paderi R, Onnis P and Cafini
D: Ileal perforation caused by metastasis of bronchogenic
carcinoma. Minerva Chir. 40:567–570. 1985.PubMed/NCBI
|
|
86
|
Quayle AR, Holt S and Clark RG: Jejunal
perforation secondary to metastatic bronchogenic carcinoma.
Postgrad Med J. 61:163–165. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Vesth N, Jensen KH and Karkov J:
Perforating small intestinal metastasis from a primary lung tumor.
Ugeskr Laeger. 147:34921985.PubMed/NCBI
|
|
88
|
McNeill PM, Wagman LD and Neifeld JP:
Small bowel metastases from primary carcinoma of the lung. Cancer.
59:1486–1489. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Pang JA and King WK: Bowel haemorrhage and
perforation from metastatic lung cancer. Report of three cases and
a review of the literature. Aust NZJ Surg. 57:779–783. 1987.
View Article : Google Scholar
|
|
90
|
Cavenaile JC, Blairon J and Limbosch JM:
Jejunal perforation indicating the metastatic extension of a
bronchial neoplasm. Acta Chir Belg. 88:155–157. 1988.PubMed/NCBI
|
|
91
|
Hwang GS, Yeh PF, Lee YC, Perng RP and Li
WY: Small bowel perforation secondary to metastatic carcinoma of
lung. Zhonghua Yi Xue Za Zhi (Taipei). 41:159–164. 1988.(In
Chinese). PubMed/NCBI
|
|
92
|
Koury HI and Kenady D: Perforation of a
metastatic lung adenocarcinoma of the jejunum. Am J Gastroenterol.
83:462–463. 1988.PubMed/NCBI
|
|
93
|
Shatikhin VA, Vasil'ev AV and Bychkov MB:
Metastasis of lung cancer to the small intestine with its
perforation. Klin Med (Mosk). 66:135–136. 1988.PubMed/NCBI
|
|
94
|
Shirani J and Brackett JW: Lung cancer
presenting as small bowel perforation. Conn Med. 53:455–456.
1989.PubMed/NCBI
|
|
95
|
Joyce WP, Huddy SP, Corbishley C and
Wright NL: Small bowel complications of metastatic lung carcinoma.
Ir J Med Sci. 159:149–150. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Woods JM IV and Koretz MJ: Emergency
abdominal surgery for complications of metastatic lung carcinoma.
Arch Surg. 125:583–585. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Nakano Y, Kamimori T, Shoji S, Taruya E
and Tanaka I: A case of jejunal metastasis from pulmonary
adenocarcinoma occurring as perforative peritonitis. Nihon Kyobu
Shikkan Gakkai Zasshi. 29:649–653. 1991.(In Japanese). PubMed/NCBI
|
|
98
|
Yasunaga A, Shibata O, Sasaki T, Tohara K,
Hadama T, Uchida Y, Yasunaga T and Adachi Y: A case of perforation
of the metastatic site of lung carcinoma in the small bowel. Kyobu
Geka. 44:596–599. 1991.(In Japanese). PubMed/NCBI
|
|
99
|
Beluffi L, Agostini M, Ruck F, Valenghi D,
Morotti L and Marsetti M: Peritonitis caused by jejunal perforation
resulting from metastasis of pulmonary carcinoma. Minerva Chir.
47:1023–1026. 1992.(In Italian). PubMed/NCBI
|
|
100
|
Gitt SM, Flint P, Fredell CH and Schmitz
GL: Bowel perforation due to metastatic lung cancer. J Surg Oncol.
51:287–291. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Ryo H, Sakai H, Ikeda T, Hibino S, Goto I,
Yoneda S and Noguchi Y: Gastrointestinal metastasis from lung
cancer. Nihon Kyobu Shikkan Gakkai Zasshi. 34:968–972. 1996.(In
Japanese). PubMed/NCBI
|
|
102
|
Cossavella D, Paino O, Luc Realis A,
Clerico G, Catania S, Pozzo M and Trompetto M: A rare form of
intestinal perforation: adenocarcinoma of the ileum. Presentation
of a clinical case. Minerva Chir. 53:431–433. 1998.(In Italian).
PubMed/NCBI
|
|
103
|
Fischer M, Papp J, Kulka J, Zsiray M,
Kempler P and Szalay F: Upper gastrointestinal bleeding and
intestinal perforation due to multiple duodenojejunal metastases
from a silent bronchogenic adenosquamous carcinoma. Endoscopy.
30:S791998. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Shiraishi Y, Nakajima Y, Katsuragi N,
Hanaoka T, Konno H and Tanaka S: Metastatic lung tumor: report of
two cases. Kyobu Geka. 56:47–50. 2003.PubMed/NCBI
|
|
105
|
Yokota T, Yamada Y, Sakata N, Kikuchi S,
Kunii Y, Tezuka F, Suzuki H and Yamauchi H: Emergency abdominal
surgery for small bowel perforation secondary to metastatic lung
cancer. Tohoku J Exp Med. 188:265–270. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Ise N, Kotanagi H, Morii M, Yasui O, Ito
M, Koyama K and Sageshima M: Small bowel perforation caused by
metastasis from an extra-abdominal malignancy: Report of three
cases. Surg Today. 31:358–362. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Polak M, Kupryjańczyk J and Rell KW: A
rare case of colonic perforation in a sole site of latent lung
cancer metastasis. Pol Tyg Lek. 45:179–181. 1990.(In Polish).
PubMed/NCBI
|
|
108
|
Rahman R, Bernstein Z, Vaickus L,
Penetrante R, Arbuck S, Kopec I, Vesper D, Douglass HO Jr and Foon
KA: Unusual gastrointestinal complications of interleukin-2
therapy. J Immunother (1991). 10:221–225. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Fletcher MS: Gastric perforation secondary
to metastatic carcinoma of the lung: a case report. Cancer.
46:1879–1882. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Schmidt G, Börsch G, von Liebe S and Böhm
E: Gastric perforation secondary to metastatic bronchogenic
carcinoma. Hepatogastroenterology. 32:103–105. 1985.PubMed/NCBI
|
|
111
|
Opanasenko NS: Gastric perforation into
the left pleural cavity after pleuropulmonectomy for pulmonary
cancer. Klin Khir. 56–57. 2000.(In Russian). PubMed/NCBI
|
|
112
|
Suzaki N, Hiraki A, Ueoka H, Aoe M,
Takigawa N, Kishino T, Kiura K, Kanehiro A, Tanimoto M and Harada
M: Gastric perforation due to metastasis from adenocarcinoma of the
lung. Anticancer Res. 22:1209–1212. 2002.PubMed/NCBI
|
|
113
|
Sanli Y, Adalet I, Turkmen C, Kapran Y,
Tamam M and Cantez S: Small bowel metastases from primary carcinoma
of the lung: Presenting with gastrointestinal hemorrhage. Ann Nucl
Med. 19:161–163. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Tomas D, Ledinsky M, Belicza M and Kruslin
B: Multiple metastases to the small bowel from large cell bronchial
carcinomas. World J Gastroenterol. 11:1399–1402. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Misra SP, Dwivedi M, Misra V, Dharmani S
and Gupta M: Duodenal metastases from squamous cell carcinoma of
the lung: Endoscopic management of bleeding and biliary and
duodenal obstruction. Indian J Gastroenterol. 23:185–186.
2004.PubMed/NCBI
|
|
116
|
Katsinelos P, Paroutoglou G, Beltsis A,
Pilpilidis I, Papaziogas B, Mimidis K and Tsolkas P: Hematemesis as
a presenting symptom of lung cancer with synchronous metastases to
the esophagus and stomach. A case report. Rom J Gastroenterol.
13:251–253. 2004.PubMed/NCBI
|
|
117
|
Kobayashi O, Murakami H, Yoshida T, Cho H,
Yoshikawa T, Tsuburaya A, Sairenji M, Motohashi H, Sugiyama Y and
Kameda Y: Clinical diagnosis of metastatic gastric tumors:
Clinicopathologic findings and prognosis of nine patients in a
single cancer center. World J Surg. 28:548–551. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Capasso L, Iarrobino G, D'Ambrosio R,
Carfora E, Ventriglia R and Borsi E: Surgical complications for
gastric and small bowel metastases due to primary lung carcinoma.
Minerva Chir. 59:397–403. 2004.PubMed/NCBI
|
|
119
|
Renault PA, Arotçarena R, Calès V, Lippa
A, Benichou M, Laurent P and Laborde Y: Metastatic obstruction of
the small bowel revealing or complicating squamous-cell lung
cancer. Two cases and a review of the literature. Rev Pneumol Clin.
59:161–165. 2003.PubMed/NCBI
|
|
120
|
Yamamoto M, Matsuzaki K, Kusumoto H,
Uchida H, Mine H, Kabashima A, Maehara Y and Sugimachi K: Gastric
metastasis from lung carcinoma. Case report.
Hepatogastroenterology. 49:363–365. 2002.PubMed/NCBI
|
|
121
|
Ito Y, Suzuki M, Oyamada Y, Kou H,
Takeshita K, Asano K and Yamaguchi K: A case of relapsed small cell
lung cancer recognized by simple metastasis to the duodenum. Nihon
Kokyuki Gakkai Zasshi. 39:30–34. 2001.(In Japanese). PubMed/NCBI
|
|
122
|
Fukata T, Fukino S, Hayashi E, Okada K,
Tamai N and Nakashima H: A case of G-CSF-producing large cell
carcinoma of the lung with gastric metastasis. Kyobu Geka.
53:798–803. 2000.(In Japanese). PubMed/NCBI
|
|
123
|
Berger A, Cellier C, Daniel C, Kron C,
Riquet M, Barbier JP, Cugnenc PH and Landi B: Small bowel
metastases from primary carcinoma of the lung: clinical findings
and outcome. Am J Gastroenterol. 94:1884–1887. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Centeno Cortés C, Clavero Borau MJ,
Rubiales Sanz A and Martín López-Lara F: Intestinal bleeding in
disseminated non-small cell lung cancer. Lung Cancer. 18:101–105.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Akahoshi K, Chijiiwa Y, Hirota I, Ohogushi
O, Motomatsu T, Nawata H and Sasaki I: Metastatic large-cell lung
carcinoma presenting as gastrointestinal hemorrhage. Acta
Gastroenterol Belg. 59:217–219. 1996.PubMed/NCBI
|
|
126
|
Raijman I: Duodenal metastases from lung
cancer. Endoscopy. 26:752–753. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Gateley CA, Lewis WG and Sturdy DE:
Massive lower gastrointestinal haemorrhage secondary to metastatic
squamous cell carcinoma of the lung. Br J Clin Pract. 47:276–277.
1993.PubMed/NCBI
|
|
128
|
Maeda J, Miyake M, Tokita K, Iwahashi N,
Nakano T, Tamura S, Hada T and Higashino K: Small cell lung cancer
with extensive cutaneous and gastric metastases. Intern Med.
31:1325–1328. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Mosier DM, Bloch RS, Cunningham PL and
Dorman SA: Small bowel metastases from primary lung carcinoma: A
rarity waiting to be found? Am Surg. 58:677–682. 1992.PubMed/NCBI
|
|
130
|
Park SW, Cho HJ, Choo WS, Chung KS, Kim
HY, Yoo JY, Kim JS and Shin HS: A case of intestinal hemorrhage due
to small intestinal metastases from primary lung cancer. Korean J
Intern Med. 6:79–84. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Spedini C, Lombardi C and Buffoli F:
Multiple mucosal gastrointestinal metastases from primary
asymptomatic bronchogenic carcinoma. Recenti Prog Med. 81:442–444.
1990.PubMed/NCBI
|
|
132
|
Ono H, Okabe M, Kimura T, Kawakami M,
Nakamura K, Danjo Y, Takasugi H and Nishihara H: Colonic metastasis
from primary carcinoma of the lung: Report of a case and review of
Japanese literature. Clin J Gastroenterol. 2:89–95. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Stinchcombe TE, Socinski MA, Gangarosa LM
and Khandani AH: Lung cancer presenting with a solitary colon
metastasis detected on positron emission tomography scan. J Clin
Oncol. 24:4939–4940. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Travis WD, Brambilla E, Nicholson AG,
Yatabe Y, Austin JH, Beasley MB, Chirieac LR, Dacic S, Duhig E,
Flieder DB, et al: The 2015 World Health Organization
classification of lung tumors: impact of genetic, clinical and
radiologic advances since the 2004 classification. J Thorac Oncol.
10:1243–1260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Edge S, Byrd D, Compton C, Fritz A, Greene
F and Trotti A: AJCC Cancer Stageing Manual. Springer; New York:
2010
|
|
136
|
Kim CH, Lee YC, Hung RJ, McNallan SR, Cote
ML, Lim WY, Chang SC, Kim JH, Ugolini D, Chen Y, et al: Exposure to
secondhand tobacco smoke and lung cancer by histological type: A
pooled analysis of the International Lung Cancer Consortium
(ILCCO). Int J Cancer. 135:1918–1930. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Cox D and Oakes N: Analysis of Survival
Data. Chapman and Hall; New York: 1984
|
|
138
|
Guo Z, Han B and Wang Y: The status of
diagnosis and therapy for gastrointestinal metastasis from primary
lung cancer. Zhongguo Fei Ai Za Zhi. 14:69–71. 2011.(In Chinese).
PubMed/NCBI
|
|
139
|
Hillenbrand A, Sträter J and Henne-Bruns
D: Frequency, symptoms and outcome of intestinal metastases of
bronchopulmonary cancer. Case report and review of the literature.
Int Semin Surg Oncol. 2:132005. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Yuen JS, Chow PK and Ahmed Q: Metastatic
lung cancer causing bowel perforations: Spontaneous or
chemotherapy-related? ANZ J Surg. 72:245–246. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Kim SY, Ha HK, Park SW, Kang J, Kim KW,
Lee SS, Park SH and Kim AY: Gastrointestinal metastasis from
primary lung cancer: CT findings and clinicopathologic features.
AJR Am J Roentgenol. 193:W197–W201. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Di JZ, Peng JY and Wang ZG: Prevalence,
clinicopathological characteristics, treatment, and prognosis of
intestinal metastasis of primary lung cancer: A comprehensive
review. Surg Oncol. 23:72–80. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Israel O, Yefremov N, Bar-Shalom R, Kagana
O, Frenkel A, Keidar Z and Fischer D: PET/CT detection of
unexpected gastrointestinal foci of 18F-FDG uptake: Incidence,
localization patterns and clinical significance. J Nucl Med.
46:758–762. 2005.PubMed/NCBI
|
|
144
|
Kim MS, Cheon GJ, Lim SM, Kim CH and Lee
JC: F-18 FDG PET-CT imaging of intestinal metastasis from primary
lung cancer. Clin Nucl Med. 33:870–871. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Kini S, Kapadia RM and Amarapurkar A:
Intussusception due to intestinal metastasis from lung cancer.
Indian J Pathol Microbiol. 53:141–143. 2010. View Article : Google Scholar : PubMed/NCBI
|