Introduction
Pulmonary hamartoma is the most common benign tumor
of the lung, accounting for ~75% of all pulmonary benign tumors.
Pulmonary sclerosing hemangioma (PSH), which originates from type
II pneumocytes, is a rare lung tumor, accounting for 3–5% of benign
lung lesions. Pulmonary hamartoma and PSH usually present as a
well-defined, peripheral, solitary lung nodule or mass on computed
tomography (CT) examination, and calcification may occasionally be
present (1–6). These morphological features are not
specific enough to differentiate the lesions from other pulmonary
tumors. Fluorodeoxyglucose positron emission tomography/CT
(18F-FDG PET/CT), which can provide morphological and
metabolic information on tumors, has been reported to be useful in
differentiating benign pulmonary tumors from malignancies. Usually,
benign lung tumors display a lack of metabolic activity or light to
moderate FDG uptake on PET/CT, which corresponds to their
slow-growing behavior (7,8).
However, a few studies have suggested that certain
benign pulmonary tumors, such as PSH, may be low-grade
malignancies, since cases of lymph node and lung metastases have
been reported (9–14), or that the malignant transformation of
lung benign tumors may be possible, such as the transformation of
pulmonary hamartoma into adenocarcinoma, sarcoma or squamous cell
carcinoma (15–17). Thus, it is also important to compare
and analyze the characteristics of 18F-FDG PET/CT in
benign lung tumors and to evaluate their metabolic activities to
choose the proper clinical management. Thus, the present study
investigated the characteristics of 18F-FDG PET/CT in
PSH versus pulmonary hamartoma.
Materials and methods
Patients
Between November 2015 and August 2017, 12 cases with
pathologically defined PSH and 14 cases with pulmonary hamartoma
undergoing 18F-FDG PET/CT examination in the Department
of Nuclear Medicine, Shanghai Pulmonary Hospital (Tongji University
School of Medicine, Shanghai, China) were enrolled in the present
study. The patient characteristics are listed in Table I.
 | Table I.Patient data. |
Table I.
Patient data.
| Characteristic | Pulmonary sclerosing
hemangioma | Pulmonary
hamartoma |
|---|
| Total patients,
n | 12 | 14 |
| Mean age (range),
years | 55 (39–66) | 59 (46–72) |
| Sex, n |
|
|
| Male | 1 | 9 |
|
Female | 11 | 5 |
| Mean size (range),
cm | 1.9 (0.6–2.9) | 1.7 (0.7–3.1) |
| Lesions, n |
|
|
|
Single | 12 | 14 |
|
Multiple | 0 | 0 |
| Localization, n |
|
|
| RUL | 0 | 2 |
| RML | 2 | 5 |
| RLL | 4 | 3 |
| LUL | 0 | 3 |
| LLL | 6 | 1 |
| Localization, n |
|
|
|
Central | 0 | 0 |
|
Peripheral | 12 | 14 |
| Calcification, n |
|
|
| With | 3 | 4 |
|
Without | 9 | 10 |
| Shape, n |
|
|
|
Round | 12 | 14 |
|
Irregular | 0 | 0 |
| Margin, n |
|
|
|
Smooth | 10 | 8 |
|
Lobular | 2 | 6 |
18F-FDG PET/CT scans and
image analysis
An FDG PET/CT scan was performed on a Biograph 64
system (Siemens Healthineers, Erlangen, Germany) with a 21.6-cm
axial field of view. Patients were required to fast for at least 6
h prior to imaging, and serum glucose levels were kept at <7.4
mmol/l. Images were obtained ~60 min after intravenous
administration of 3.7–5.6 MBq of FDG per kilogram of body weight.
In total, 6 or 7 bed positions from the base of the skull to the
mid-thighs were imaged. PET images were acquired for 1.5 min per
bed position. CT was performed on the same scanner without contrast
administration. The CT scan data were collected under the following
conditions: 120 kV, 101 mAs (adjusted by auto mA) and a gantry
rotation speed of 0.5 sec. All CT scans were obtained using 5-mm
thick axial slices. PET/CT images were analyzed based on CT
features and semi-quantitative measurement on the basis of
standardized maximum uptake value (SUVmax). SUVmax was calculated
as decay-corrected maximum activity concentration in the lesion
divided by administered activity divided by body weight in
kilograms.
Pathological examination. In this study, all 12
patients with PSH and all 14 patients with pulmonary hamartoma
underwent resection of the lesion by video-assisted thoracoscopic
surgery within 2 weeks of the FDG PET/CT scans. The lung lesions
were obtained, and the slides of paraffin-embedded samples were
used for common hematoxylin and eosin and immunohistochemical
staining. The sections were reviewed by 2 experienced pathologists
for the histopathological confirmation of tumor type.
Statistical analysis
SPSS 21.0 software for Windows (IBM Corp., Armonk,
NY, USA) was used for the statistical analysis (18). Data are expressed as the mean ±
standard deviation. The association between tumor size and SUVmax
was analyzed through Pearson's correlation and linear regression
analysis, and the tumor size and SUVmax of two groups were compared
using Student's t-test. The 95% confidence level was chosen to
determine the significance between groups, with P<0.05
indicating a statistically significant difference. The cut-off
value for the differential diagnosis of PSH and pulmonary hamartoma
was obtained through the receiver operating characteristic (ROC)
analysis. The areas under the curve, and the sensitivity and
specificity of differential diagnosis were calculated.
Results
As shown in Table I,
the mean age of the 12 patients with PSH was 55±9 years. The number
of women was greater than that of men, with a ratio of 11:1. The 12
PSHs were all located in the bilateral middle and lower lungs.
Among the 12 PSH lesions, 3 lesions exhibited calcification. For
the 14 cases of pulmonary hamartoma, the mean age was 59±7 years,
and the ratio of women to men was 5:9. These 14 lesions were
diffusely located in the bilateral lungs, and the ratio of right-to
left-sided lesions was 5:2. Among the 14 pulmonary hamartoma
lesions, 4 exhibited calcification.
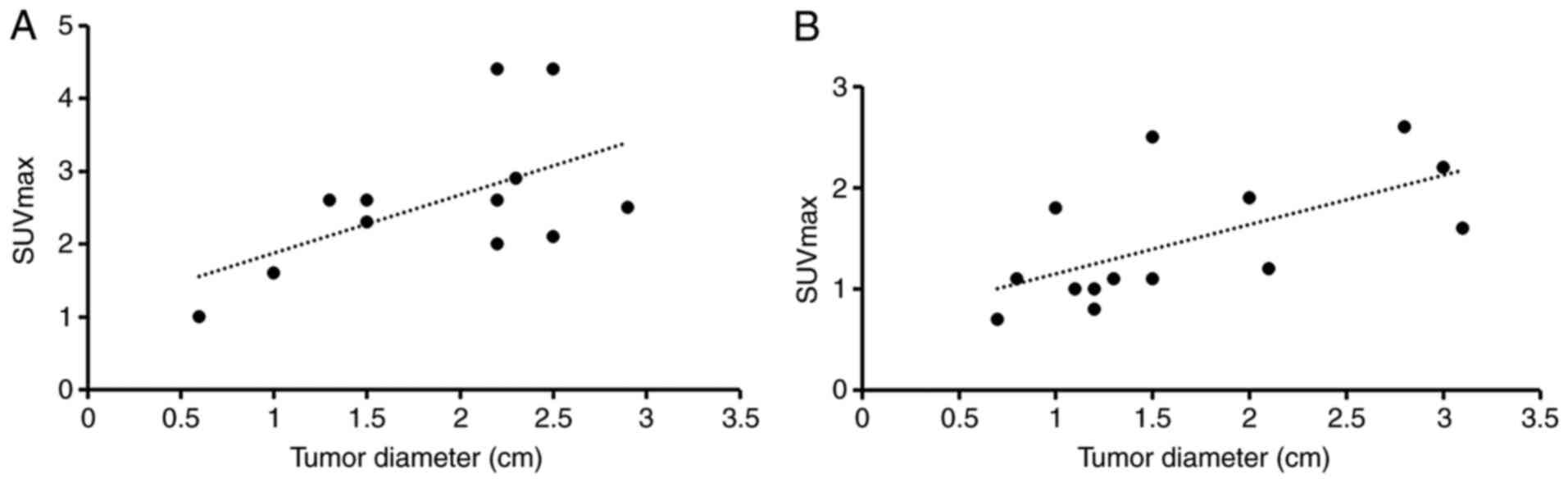
For the 12 patients with PSH, the mean diameter of
all 12 lesions was 1.9±0.7 cm, ranging from 0.6 to 2.9 cm. The mean
SUVmax was 2.6±1.0, with a SUVmax ranging from 1.0 to 4.4. There
was no significant correlation between the lesion size and SUVmax
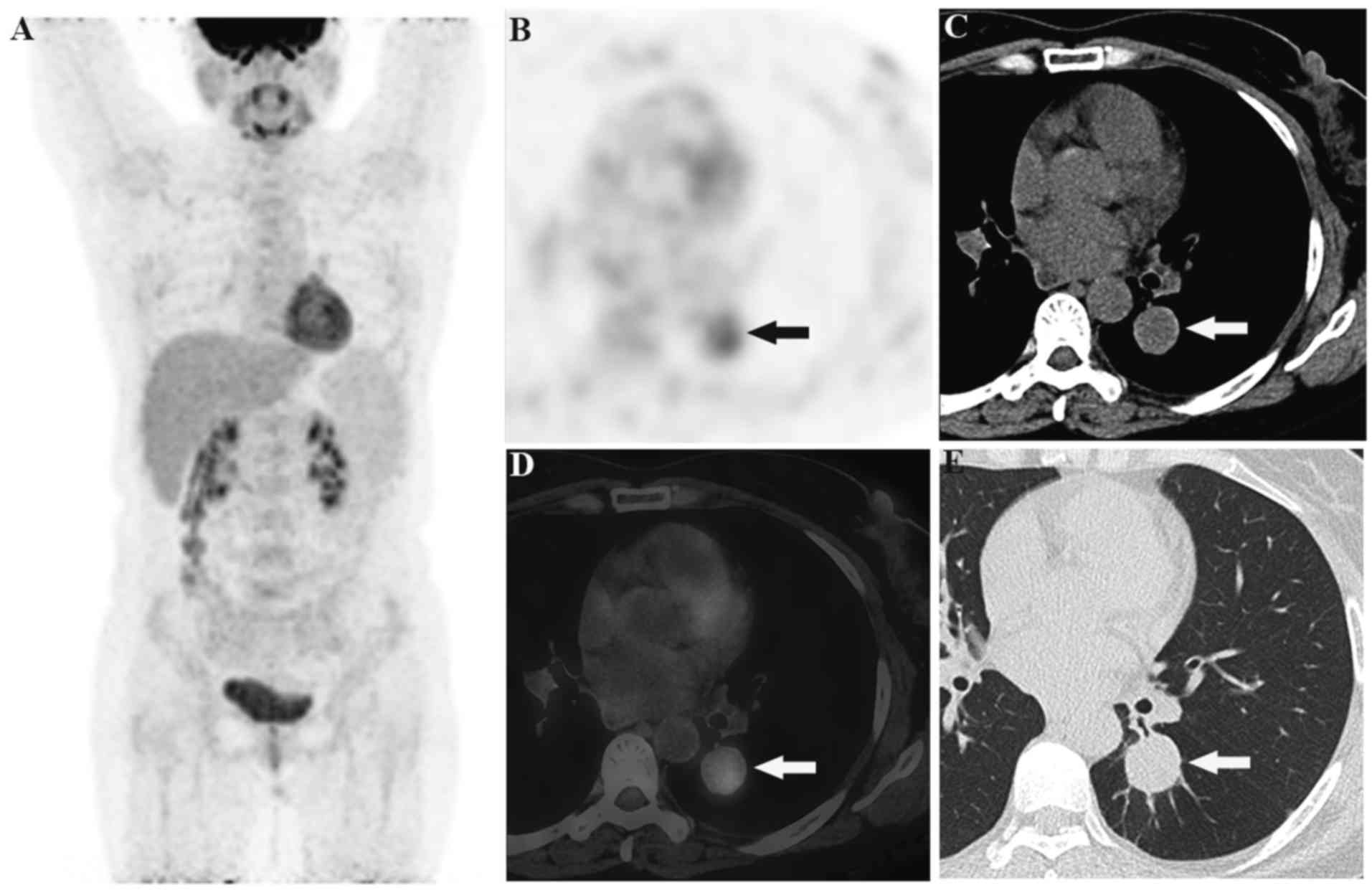
of PSH (P>0.05, r=0.560, r2=0.314) (Fig. 1A). In total, 6 out of 12 PSHs (50%)
displayed increased SUVmax values >2.5, with SUVmax values of
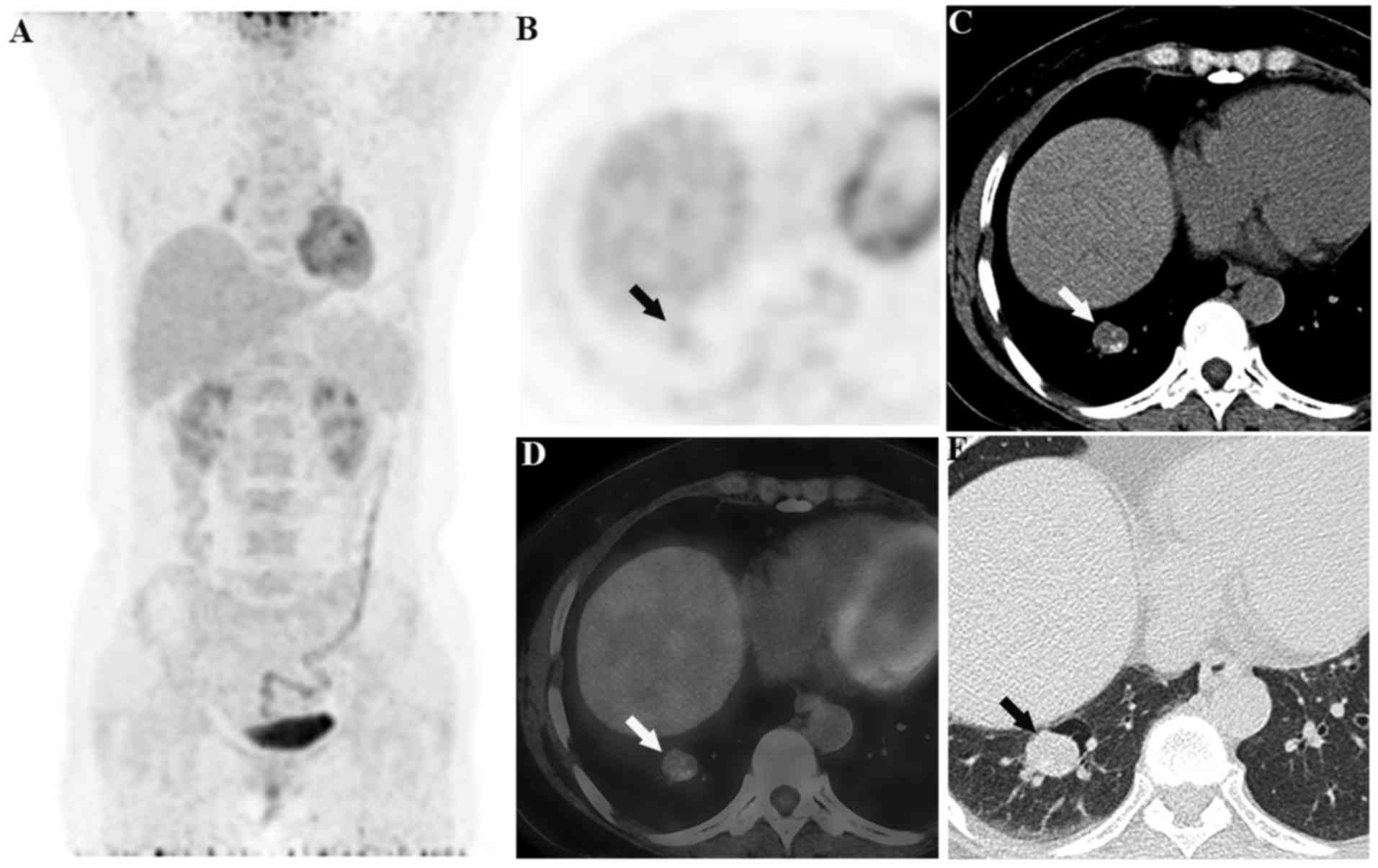
2.6, 2.6, 2.6, 2.9, 4.4 and 4.4, respectively (Figs. 2 and 3).
Fig. 2 presents a case of PSH with an
SUVmax of 4.4, and Fig. 3 presents a
second case of PSH with an SUVmax of 2.6 and calcification. In
addition, no case of PSH with lymph node or lung metastases was
observed in the study.
For the 14 cases with pulmonary hamartoma, the mean
diameter and SUVmax of all lesions were 1.7±0.8 cm (ranging from
0.7 to 3.1 cm) and 1.5±0.6 (ranging from 0.7 to 2.6), respectively.
There was a significant correlation between the lesion size and
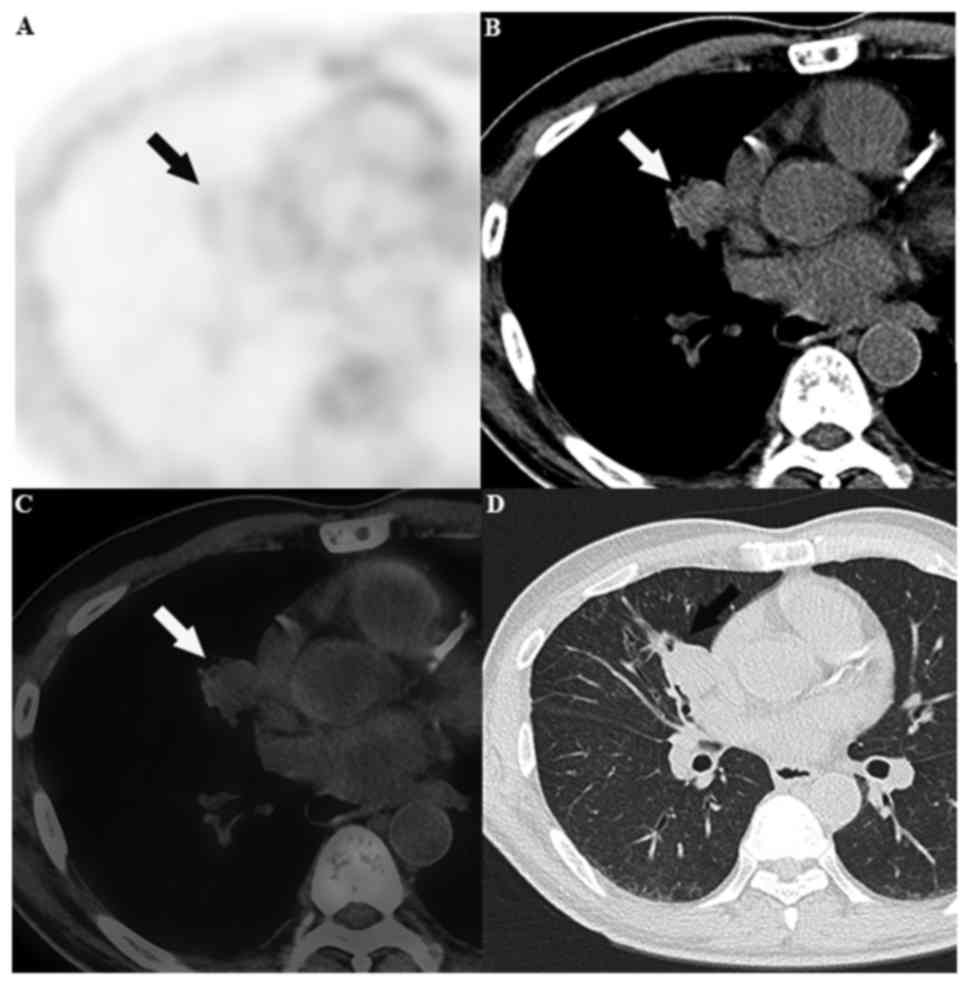
SUVmax (r=0.625, r2=0.391, P<0.05; Fig. 1B). Moreover, only 1 lesion out of 14
pulmonary hamartomas (7%) displayed increased SUVmax values
>2.5, with a value of 2.6 (Fig.
4).
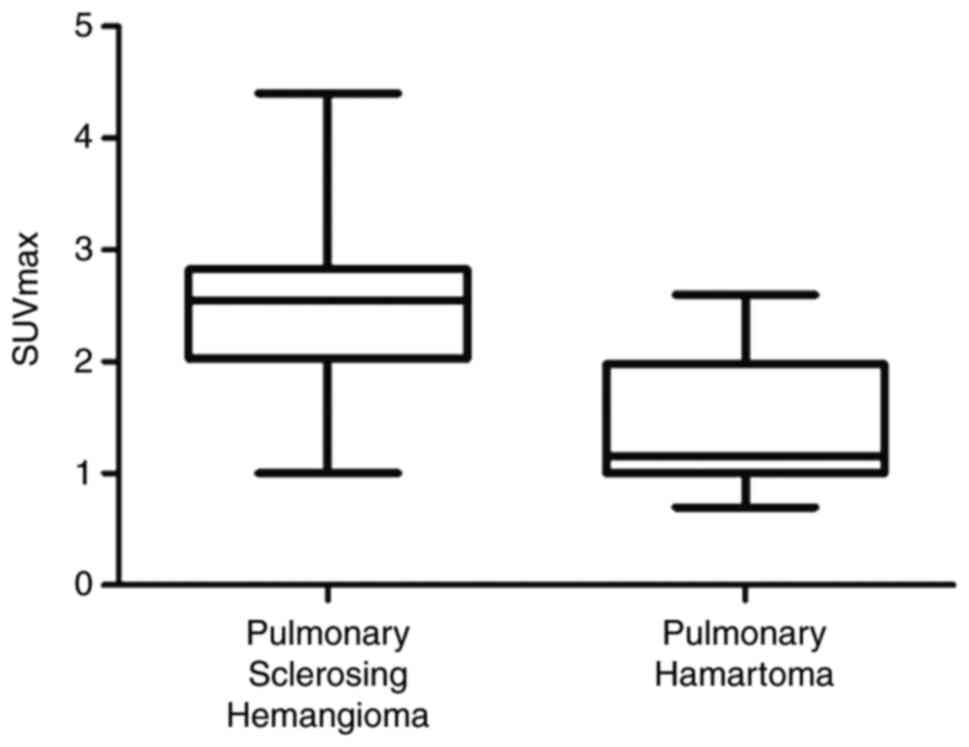
Furthermore, there was no significant difference
between the lesion size of PSH and that of pulmonary hamartoma
(P>0.05), but the SUVmax of PSH was significantly higher than
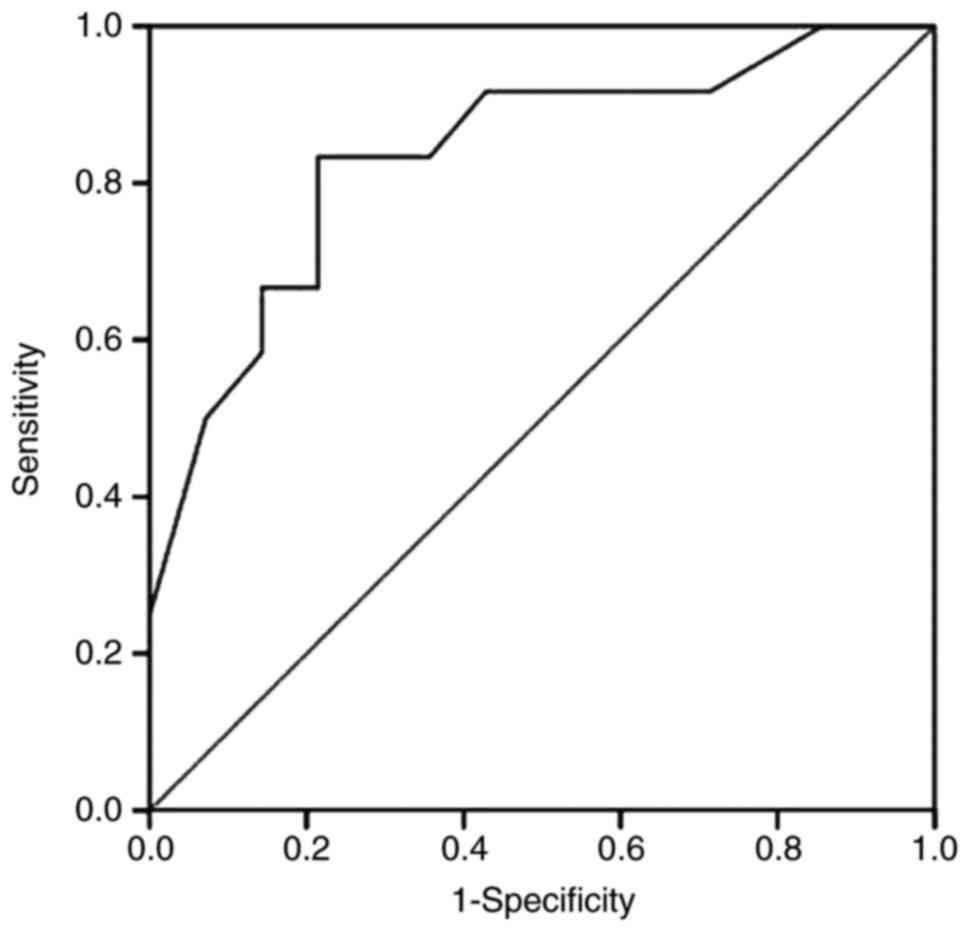
that of pulmonary hamartoma (P<0.05; Fig. 5). As a cutoff for the differential
diagnosis of PSHs versus pulmonary hamartomas, the SUVmax of 1.95
was applied (Fig. 6). The resulting
sensitivity and specificity for 18F-FDG PET/CT to
differentiate PSHs from pulmonary hamartomas was 83.3 and 78.6 %,
respectively.
Discussion
PSH has been reported to show various FDG
accumulations, with an SUVmax ranging from the background value to
5.3, and the results of the present study were similar to these of
previously reported cases (7,19–21). FDG
PET/CT scan results are usually interpreted as positive for
malignancy when the SUVmax of a lung nodule or mass exceeds 2.5
(22). In the present study, the
SUVmax of 50% of the PSHs exceeded 2.5. The high FDG accumulation
in PSH should be associated with the tumor size or with potential
low-grade malignancy. Lin et al (7) observed that larger PSHs tended to show
higher FDG uptake on PET/CT scan. Lee et al (21) reported that the SUVmax was
significantly correlated with tumor size in 8 cases of PSH.
However, in the present study of 12 PSH cases, there was no
significant correlation between the SUVmax and the tumor size.
Moreover, although no case of PSH with lymph node or lung
metastases was observed in the present study, the increased FDG in
PSH may be mainly associated with the potential low-grade malignant
nature.
Uhlén et al (8)
analyzed 51 patients with pulmonary hamartoma by 18F-FDG
PET/CT and found a median SUVmax of 1.4, which was similar to that
in the present study. Unlike in PSH, there was a significant
correlation between the SUVmax and the tumor size of pulmonary
hamartoma in the present study. Moreover, although there was no
marked difference between the tumor size, density, shape and margin
of the PSHs and pulmonary hamartomas, the study showed
significantly higher FDG accumulation in the PSHs than in the
pulmonary hamartomas. Chung et al (23) suggested that the presence of a
hemangiomatous or papillary component in the tumor may lead to
increased FDG uptake. Lee et al (21) attempted to analyze the mechanism or
histological influencing factors of the increased FDG uptake of
PSH. However, there were no clear histopathological factors
influencing SUVmax in the study, including the tumor component, and
glucose transporter protein-1 (GLUT-1) and GLUT-4 expression.
Therefore, influencing factors on the increased FDG uptake of PSH
should be further investigated with larger sample sizes.
PSH or pulmonary hamartoma usually presents as a
well-defined, peripheral, solitary lung nodule or mass on CT
examination, and calcification may occasionally be present. Thus,
the majority of PSHs or pulmonary hamartomas could be diagnosed as
benign lesions. Due to the poor specificity of the radiological
characteristics, few lesions are directly diagnosed as PSH or
pulmonary hamartoma even on contrast-enhanced CT examination
(1–6).
To the best of our knowledge, the present study is the first report
on the 18F-FDG PET/CT characteristics of PSH versus
those of pulmonary hamartoma. The present study showed
significantly higher FDG accumulation in PSHs than that in
pulmonary hamartomas, which may aid the differential diagnosis. The
cut-off SUVmax value of 1.95 for the differential diagnosis of PSH
and pulmonary hamartoma was obtained through ROC analysis. Among
the 12 PSHs, the SUVmax of only 2 lesions was <1.95 (1.0 and
1.6). Meanwhile, the SUVmax of 3 lesions out of the 14 pulmonary
hamartomas was >1.95 (2.2, 2.5 and 2.6). When the SUVmax of lung
lesions with certain types of benign features, including a round
shape, a clear boundary and calcification, exceeds 2.5, it should
be distinguished from lung malignancies. In addition, PSH may be
low-grade malignancy, since cases of lymph node and lung metastases
have been reported. Thus, FDG PET/CT could be useful for the
differential diagnosis of low-grade malignancy of PSH, particularly
when the SUVmax of PSH exceeds 2.5, or when lymph node and lung
metastases are displayed on PET/CT images (9–14), which
would be of great assistance in the clinical treatment.
In conclusion, although the morphological features
of the two lesion types were not specific, PSH showed significantly
higher FDG accumulation than pulmonary hamartoma, and thus, the
SUVmax of 18F-FDG PET/CT may be useful in the
differential diagnosis between PSH and pulmonary hamartoma. The
main limitation of the present study was the small number of cases,
which does not allow for high statistical power. In addition, a
correlation analysis between histopathological factors and SUVmax
was not performed in the present study, which is another main
limitation. Therefore, further studies with a large study
population are warranted to confirm the findings of the present
study.
Acknowledgements
Not applicable.
Funding
This study is in part supported by the National
Science Foundation for Scholars of China (grant no. 81571703), the
Outstanding Young Talents Program of Shanghai Municipal Commission
of Health and Family Planning (grant no. 2017YQ027) and funding
sponsored by Shanghai Pujiang Program (grant no. 2015PJD006).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article
Authors' contributions
HW and LJ conceived and designed the experiments.
YH, QT, QZ, YL and XW collected and analyzed the imaging and
pathology data. LJ wrote the paper.
Ethics approval and consent to
participate
This retrospective study was approved by the Ethics
Committee of Shanghai Pulmonary Hospital (Tongji University School
of Medicine, Shanghai, China).
Consent for publication
The patients in the present study provided written
informed consent for the publication of any associated data and
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sugio K, Yokoyama H, Kaneko S, Ishida T
and Sugimachi K: Sclerosing hemangioma of the lung: radiographic
and pathological study. Ann Thorac Surg. 53:295–300. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Iyoda A, Hiroshima K, Shiba M, Haga Y,
Moriya Y, Sekine Y, Shibuya K, Iizasa T and Fujisawa T:
Clinicopathological analysis of pulmonary sclerosing hemangioma.
Ann Thorac Surg. 78:1928–1931. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Neuman J, Rosioreanu A, Schuss A, Turi G,
Yung E, Trow TK, Williams L and Katz DS: Radiology-pathology
conference: Sclerosing hemangioma of the lung. Clin Imaging.
30:409–412. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Edey AJ and Hansell DM: Incidentally
detected small pulmonary nodules on CT. Clin Radiol. 64:872–884.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lei Y, Yong D, Jun-Zhong R, Zhi Y and
Zi-Tong W: Treatment of 28 patients with sclerosing hemangioma (SH)
of the lung. J Cardiothorac Surg. 7:342012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shin SY, Kim MY, Oh SY, Lee HJ, Hong SA,
Jang SJ and Kim SS: Pulmonary sclerosing pneumocytoma of the lung:
CT characteristics in a large series of a tertiary referral center.
Medicine (Baltimore). 94:e4982015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lin KH, Chang CP, Liu RS and Wang SJ: F-18
FDG PET/CT in evaluation of pulmonary sclerosing hemangioma. Clin
Nucl Med. 36:341–343. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Uhlén N, Grundberg O, Jacobsson H, Sundin
A, Dobra K, Sánchez-Crespo A, Axelsson R and Kölbeck KG: 18F-FDG
PET/CT Diagnosis of bronchopulmonary carcinoids versus pulmonary
hamartomas. Clin Nucl Med. 41:263–267. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Miyagawa-Hayashino A, Tazelaar HD, Langel
DJ and Colby TV: Pulmonary sclerosing hemangioma with lymph node
metastases: Report of 4 cases. Arch Pathol Lab Med. 127:321–325.
2003.PubMed/NCBI
|
|
10
|
Katakura H, Sato M, Tanaka F, Sakai H,
Bando T, Hasegawa S, Nakashima Y and Wada H: Pulmonary sclerosing
hemangioma with metastasis to the mediastinal lymph node. Ann
Thorac Surg. 80:2351–2353. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chien NC, Lin CW and Tzeng JE: Sclerosing
haemangioma with lymph node metastasis. Respirology. 14:614–616.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Komatsu T, Fukuse T, Wada H and Sakurai T:
Pulmonary sclerosing hemangioma with pulmonary metastasis. Thorac
Cardiovasc Surg. 54:348–349. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maeda R, Isowa N, Miura H, Tokuyasu H,
Kawasaki Y and Yamamoto K: Bilateral multiple sclerosing
hemangiomas of the lung. Gen Thorac Cardiovasc Surg. 57:667–670.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kamaleshwaran KK, Rajan F, Mehta S,
Mohanan V and Shinto AS: Multiple pulmonary sclerosing hemangiomas
(pneumocytoma) mimicking lung metastasis detected in fluorine-18
fluorodeoxyglucose positron emission tomography/computed
tomography. Indian J Nucl Med. 29:168–170. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hedlund GL, Bisset GS III and Bove KE:
Malignant neoplasms arising in cystic hamartomas of the lung in
childhood. Radiology. 173:77–79. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rossi G1, Cavazza A, Valli R, Torricelli
P, Richeldi L, Rivasi F and Brambilla E: Atypical lipomatous tumour
(lipoma-like well-differentiated liposarcoma) arising in a
pulmonary hamartoma and clinically presenting with pneumothorax.
Lung Cancer. 39:103–106. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee BJ, Kim HR, Cheon GJ, Koh JS, Kim CH
and Lee JC: Squamous cell carcinoma arising from pulmonary
hamartoma. Clin Nucl Med. 36:130–131. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jiang L, Tan H, Panje CM, Yu H, Xiu Y and
Shi H: Role of 18F-FDG PET/CT Imaging in Intrahepatic
Cholangiocarcinoma. Clin Nucl Med. 41:1–7. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hara M, Iida A, Tohyama J, Miura N,
Shiraki N, Itoh M, Ohba S and Tateyama H: FDG-PET findings in
sclerosing hemangioma of the lung: A case report. Radiat Med.
19:215–218. 2001.PubMed/NCBI
|
|
20
|
Chen Q, Wu LJ, Hu H, Song J, Wu Y, Yan J
and Shi J: A case of pulmonary sclerosing hemangioma with low
(18)FDG uptake in PET. Oncol Lett. 3:646–648. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee E, Park CM, Kang KW, Goo JM, Kim MA,
Paeng JC, Lee HJ, Park HS and Chung DH: 18F-FDG PET/CT features of
pulmonary sclerosing hemangioma. Acta Radiol. 54:24–29. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lowe VJ, Fletcher JW, Gobar L, Lawson M,
Kirchner P, Valk P, Karis J, Hubner K, Delbeke D, Heiberg EV, et
al: Prospective investigation of positron emission tomography in
lung nodules. J Clin Oncol. 16:1075–1084. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chung MJ, Lee KS, Han J, Sung YM, Chong S
and Kwon OJ: Pulmonary sclerosing hemangioma presenting as solitary
pulmonary nodule: Dynamic CT findings and histopathologic
comparisons. AJR Am J Roentgenol. 187:430–437. 2006. View Article : Google Scholar : PubMed/NCBI
|