Introduction
Warthin's tumor (WT), composed of cystic or
glandular spaces lined by oncocytic epithelium and lymphoid
reactive stroma, is the second most common benign salivary gland
neoplasm. It is exclusively found in or near the parotid gland, and
rarely been described in the minor salivary gland or other sites
such as the cervical lymph nodes (1).
Malignant lymphoma involving WT is uncommon and is almost
single-case reports with 28 cases, mostly are non-Hodgkin B-cell
lymphomas with a prevalence of follicular lymphomas (2–8). The
co-existence of WT and classical Hodgkin lymphoma (CHL) is
extremely rare with only 3 reported cases, which all occurred in
the parotid gland (3,4,7). Herin we
describe a case of mixed-cellularity CHL (MCCHL) that primarily
presented as part of the ectopic WT in a lymph node of the neck. To
our knowledge this is the first report describing a concomitant
occurrence of MCCHL within a heterotopic WT of the cervical lymph
nodes.
Case report
A 59-year-old male presented with a 1-month history
of two unapparent masses in his right neck. No pain, fever, night
sweats or weight loss was found. His medical history included a
40-year history of heavy smoking and 8-year history of
hypertension. On physical examination, two solitary, mobile, and
non-tender masses with a smooth surface was palpated in the right
neck.
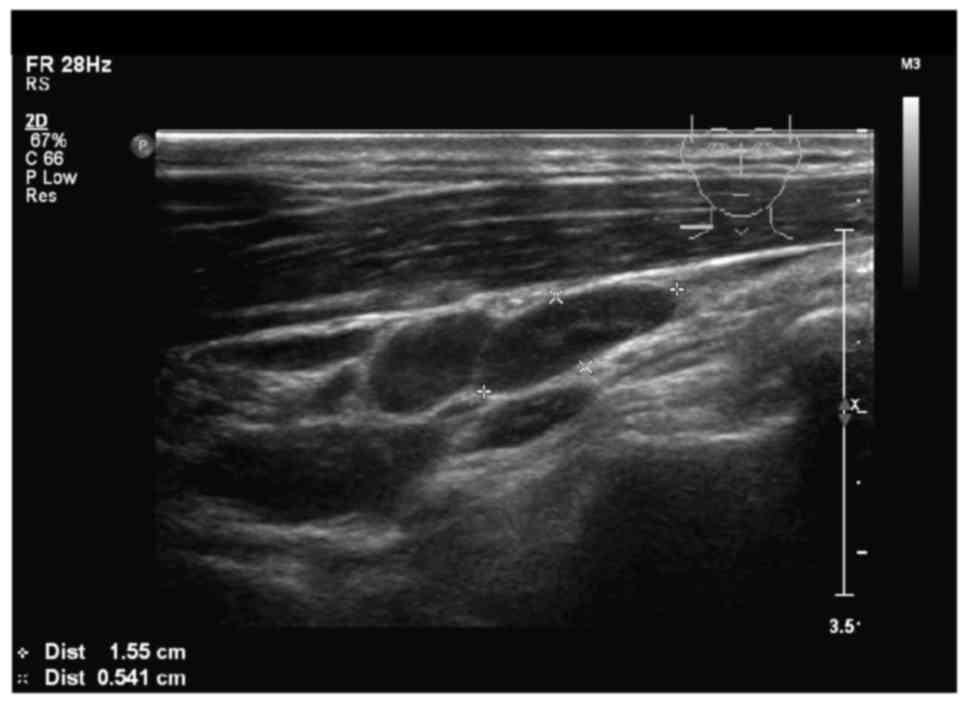
All laboratory tests including a complete blood
count and tumor markers were within normal limits. Ultrasound
sonography examination of the head and neck revealed two swollen
lymph nodes below the sternocleidomastoid muscle of the right neck,
were 1.5×0.5, 1.3×1.2 cm in size, respectively. It is no clear
boundary between the cortex and medulla of the lymph nodes
(Fig. 1). No other abnormalities were
found in the parotid gland, submaxillary gland, sublingual gland,
or left cavity. One of lymph nodes was completely resected, which
was easily extirpated. The tissue was subjected to a series of
pathological examinations.
Grossly, the excised specimen was well-demarcated,
measured 1.3×1.2×1.2 cm. It appeared as a multi-fissured mass in
part of cross section, and grayish tissue could be seen around the
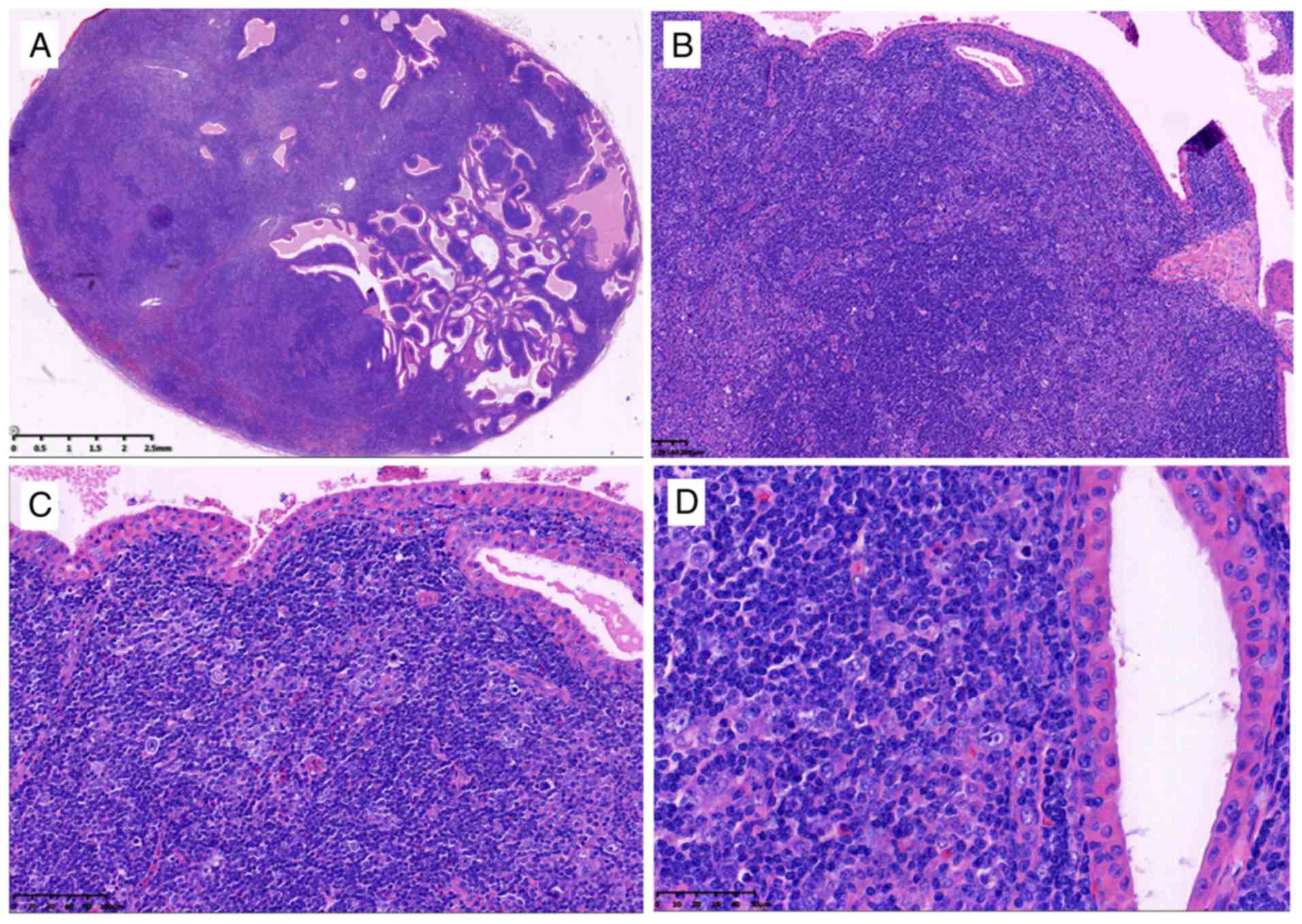
fissured spaces. Histological examination showed the presence of a
WT, composed of glandular or cystic structures, a papillary cystic
arrangement in some areas, lined with characteristic bilayered
epithelium, comprising columnar eosinophilic or oncocytic cells
surrounded by smaller basal cells (Fig.
2A-D). The cystic spaces contained eosinophilic material with
occasional crystal formation. The lymphoid component comprised
diffusely infiltrating abnormal lymphoid tissue, consisting of a
large number of small lymphocytes with admixture of occasional
eosinophils, plasma cells and histiocytes. Classic binucleated
Reed-Sternberg (RS) cells and other types of RS cells with large,
pleomorphic nucleus and prominent eosinophilic nucleoli were easily
observed in the mixed background (Fig.
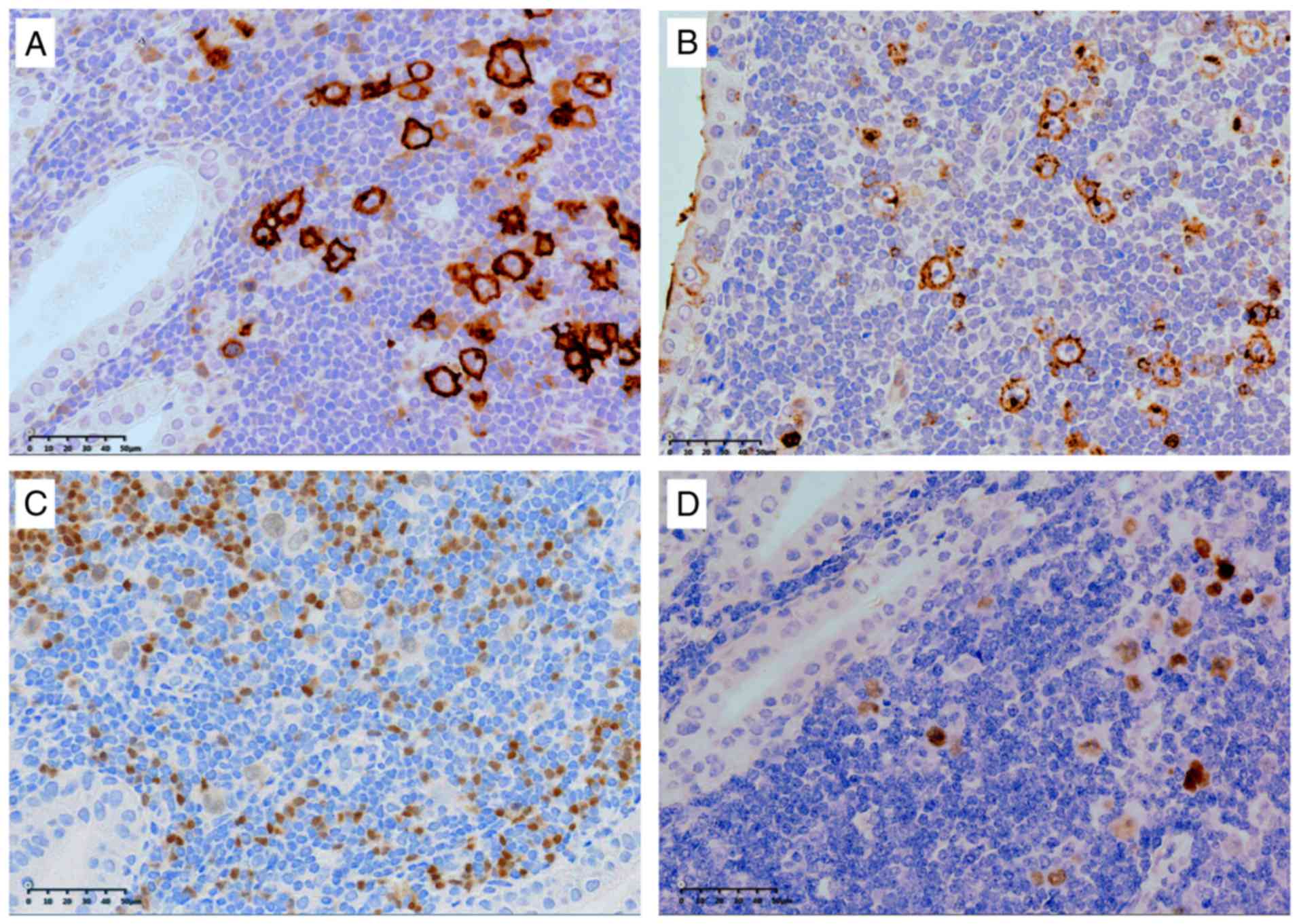
2B-D). Immunohistochemically, the RS cells were strongly
positive for CD30 (Fig. 3A) and CD15
(Fig. 3B) and LMP1, and a weak
positivity for PAX5 (Fig. 3C), but
negative for CKpan, CD45, CD3, CD20, CD10, BCL6, MUM-1, CD21, CD23,
CD68, ALK, or PD-1. The Ki-67 proliferative index was more than 60%
and EBER in situ hybridization was also positive in RS cells
(Fig. 3D). A diagnosis of MCCHL with
coexistent heterotopic WT of the cavical lymph node was made based
on the findings described above.
A thorough staging examination including contrast
enhanced computed tomography of the chest, abdomen and pelvis, and
bone marrow biopsy revealed no evidence of dissemination of CHL.
Staging workup demonstrated Ann Arbor stage IA. The patient
received four courses of chemotherapy (ABVD: Adriamycin, bleomycin,
vincristine, and dacarbazine) followed by local consolidative
radiotherapy (20 Gy). At the time of this report, the patient has
been followed up for 6 months, without evidence of disease or
lymphomas disseminated.
Discussion
WT is the second most common benign salivary gland
neoplasm, composed of glandular and often cystic structures lined
by characteristic bilayered oncocytic epithelium and abundant
lymphoid stroma. It usually presents in the fifth to seventh
decades of life and has a slight male predominance with a
male-to-female ratio of 4.6:1, that mostly affects to the heavy
smokers. WT typically occurrs intraparotid or periparotid gland and
occasionally been seen in the small salivary gland (9).
Heterotopic salivary gland tissue may occur in the
lymph node, external auditory canal, middle ear, mandible, tongue,
thyroid, and in the upper and lower neckregions (1). The neoplasms may arise from heterotopic
salivary tissue in uncommon cases, and 60–80% were benign. WT is
the frequent lesion, following by pleomorphic adenoma. The lesions
arising from heterotopic salivary tissue may present as a mass,
cyst or draining sinus.
The histogenesis of WT and heterotopic WT remains
unclear. A predominant theory is that WT develops from heterotopic
salivary ductal inclusions in intra/peri parotid, cervical lymph
nodes or other ectopic site (10). It
may stimulates and acts by smoking, The histogenesis may underlie
the heterotopic WT and the tumorigenesis of malignant lymphoma
developing in WT. The present case was primary heterotopic WT in
the cervical lymph node based on the typical histologic changes and
no tumor found in three major salivary glands or minor salivary
glands.
Malignant transformation in WT is unusual, and may
involve either the epithelial or lymphoid component. Lymphomas
associated with WT are very rare with 29 reported cases including
our case in the English literature. With available information,
there was a male predominance (males, n=25, 86%) with a mean age of
65 years (range, 49–102). The vast majority of cases (n=20, 80%)
affected the parotid gland. Pathologically, the more types were
follicular lymphoma (12/29, 41%), DLBCL (5/29, 17%) and CHL (4/29,
14%). Small lymphocytic leukemia/lymphoma (2 case, 7%), extranodal
mucosa-associated lymphoid tissue (MALT)-type (1 case, 3%), mantle
cell lymphoma (1 case, 3%), nodular lymphocyte-predominant Hodgkin
lymphoma (NLPHL, 1 case, 3%), T-cell lymphoma (TCL, peripheral
T-cell lymphoma, 1 case; T-lymphoblastic lymphoma, 1 case, 7%), and
not classified lymphoma (1 case, 3%) were also recorded. On
survival analysis, the lymphoma type (DLBCL and TCL had poor
prognosis, P=0.001) and tumor stage (I/II vs. III/IV, P=0.048)
(11) carried prognostic
significance. Further analysis showed that 4 cases of concomitan
heterotopic WT involving lymphoma had been reported (2,5,6). 3 of 4 cases were NHL and 1 case (ours)
was CHL. The majority of them were male (3/4 cases) and the
anatomical site of all cases was the lower neckregions (Table I).
 | Table I.Summary of lymphomas involving
heterotopic WT and CHL first diagnosed in WT. |
Table I.
Summary of lymphomas involving
heterotopic WT and CHL first diagnosed in WT.
| Author (year) | Age | Sex | Subtype | Location | Involved organs | Stagea | Follow-up
(months) | (Refs.) |
|---|
| Miller et
al | 49 | M | NHL (small cleaved
follicular center) | Angle of
mandible | No | IA | AWD, 5 m | (2) |
| Park et
al | 68 | F | NHL (follicular
center) | Periparorid LN | No | IA | NED, 63 m | (5) |
| Gorai et
al | 102 | M | NHL (DLBCL) | Neck LN |
| NA | Died of body
debility, 10 m | (6) |
| Melato et
al | 69 | M | CHL (mixed
cellularity) | Right parotid | Inguinal and cervical
LN | NA | DOD, 13 m | (3) |
| Badve et
al | 76 | M | CHL (no
distinguish) | Left
interparotid | Left mediastinum | NA | NED, 24 m | (4) |
| Liu et al | 78 | M | CHL
(lymphocyte-rich) | Right parotid | Hilar, mediastinal,
Abdominal LN | IVB | DOD, 7 m | (7) |
| Present study | 59 | M | CHL (mixed
cellularity) | Right cervical
LN | No | IA | NED, 6 m |
|
The primary salivary Hodgkin lymphoma (HL) including
CHL and NLPHL is also rare, mostly occurred in the parotid,
representing only 3.5 to 6% of primary parotid gland lymphomas and
0.3% of all HL cases in general (12,13).
Agaimy et al (14) reported 9
cases of intraparotid HL, are the largest group that have been
reported. As mentioned above, there were only 3 cases reported of
CHL involving WT, which all occured in the parotid gland (Table I) (3,4,7). The present case arised from heterotopic
WT in the neck, that is the first one reported. All reported cases
including our case were older male (59–78 years). Pathologically, 2
cases contained a mixed-cellularity subtype, and 1 was
lymphocyte-rich subtype. The other case was not further
distinguished with regard to the lymphoma subtype. Patients were
followed up for 6 to 24 months, and 2 were died of disease, 2 were
no evidence of disease.
The development of malignant lymphoma in WT and
heterotopic WT is incompletely understood. Intra-/peri-glandular
lymph nodes or WT lymphoid stroma might be either the site of
origin of the lymphoma or the site of secondary involvement by
disseminated disease (7,15). The possibility for the lymphoma to
originate in the lymphoid tissue of WT is supported by several
reports indicating that WT-associated lymphoma may remain a
localized disease for long periods of time (2,5). On the
other hand, the major studies indicate that the lymphoid stroma in
WT belongs to the systemic lymphoid tissue and can be involved in
disseminated lymphoma (3,4,7). In the
advanced stages, the distinction between primary and secondary
lymphomas may be impossible and unnecessary. Concerning the site of
origin of CHL in WT evidences are inconclusive, in 3 of the 4
reported cases, the disease was simultaneously present in WT and in
cervical lymph nodes, whereas, in the other case, it exclusively
involved an intraparotid. Although few, the prognosis of those
collision tumors seems to be related to the Ann Arbor stage of
CHL.
In conclusion the present study reports the first
case that is MCCHL arising from heterotopic WT of the cervical
lymph node. It shows that neoplasms arising from heterotopic
salivary tissue should be considered in the differential diagnosis
for isolated neck masses, and the lymphoid stroma of heterotopic WT
may be the site of CHL. Accurate diagnosis can be established after
removal, and hence, it has to be carefully investigated,
considering that the histological diagnosis of CHL may be very
insidious especially in the context of WT with abundant lymphoid
stroma. The present study also expands the anatomical site of
malignant lymphomas associated with WT.
Acknowledgements
Not applicable.
Funding
The present study was funded by the 2017 Zhejiang
Natural Fund (grant no. LY17H160009).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LJ interpreted the patient data and was a major
contributor in writing the manuscript. ZM undertook collection of
images and reference literature. Each author read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Consent for publication
The patient provided written informed consent for
the publication of case and clinical images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ferlito A, Bertino G, Rinaldo A, Mannarà
GM and Devaney KO: A review of heterotopia and associated salivary
gland neoplasms of the head and neck. J Laryngol Otol. 113:299–303.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miller R, Yanagihara ET, Dubrow AA and
Lukes RJ: Malignant lymphoma in the Warthin's tumor. Report of a
case. Cancer. 50:2948–2950. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Melato M, Falconieri G, Fanin R and
Baccarani M: Hodgink's disease occurring in a Warthin's tumor:
First case report. Pathol Res Pract. 181:615–620. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Badve S, Evans G, Mady S, Coppen M and
Sloane J: A case of Warthin's tumor with coexistent Hodgkin's
disease. Histopathology. 22:280–281. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Park CK, Manning JT Jr, Battifora H and
Medeiros LJ: Follicle center lymphoma and Warthin tumor involving
the same anatomic site. Report of two cases and review of the
literature. Am J Clin Pathol. 113:113–119. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gorai S, Numata T, Kawada S, Nakano M,
Tamaru J and Kobayashi T: Malignant lymphoma arising from
heterotopic Warthin's tumor in the neck: Case report and review of
the literature. Tohoku J Exp Med. 212:199–205. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu YQ, Tang QL, Wang LL, Liu QY, Fan S
and Li HG: Concomitant lymphocyte-rich classical Hodgkin's lymphoma
and Warthin's tumor. Oral Surg Oral Med Oral Pathol Oral Radiol.
116:e117–e120. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chu CY, Pan SC and Chang KC: EBV-positive
diffuse large B-cell lymphoma of the elderly involving Warthin
tumor. Pathol Int. 65:677–679. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eveson JW and Simpson RHW: Warthin
tumourBarnes L, Eveson JW, Reichart P and Sidransky D: WHO
classification of tumours: Pathology and genetics of head and neck
tumours. IARC Press; Lyon: pp. 263–265. 2005
|
|
10
|
Kuzenko YV, Romanuk AM, Dyachenko OO and
Hudymenko O: Pathogenesis of Warthin's tumors. Interv Med Appl Sci.
8:41–48. 2016.PubMed/NCBI
|
|
11
|
Carbone PP, Kaplan HS, Musshoff K,
Smithers DW and Tubiana M: Report of the committee on Hodgkin
disease staging classification. Cancer Res. 31:1860–1861.
1971.PubMed/NCBI
|
|
12
|
Feinstein AJ, Ciarleglio MM, Cong X,
Otremba MD and Judson BL: Parotid gland lymphoma: Prognostic
analysis of 2140 patients. Laryngoscope. 123:1199–1203. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Paliga A, Farmer J, Bence-Bruckler I and
Lamba M: Salivary gland lymphoproliferative disorders: A Canadian
tertiary center experience. Head Neck Pathol. 7:381–388. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Agaimy A, Wild V, Märkl B, Wachter DL,
Hartmann A, Rosenwald A and Ihrler S: Intraparotid classical and
nodular lymphocyte-predominant Hodgkin lymphoma: Pattern analysis
with emphasis on associated lymphadenoma-like proliferations. Am J
Surg Pathol. 39:1206–1212. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Giaslakiotis K, Androulaki A, Panagoulias
G, Kyrtsonis MC, Lazaris AC, Kanakis DN and Patsouris ES: T cell
lymphoblastic lymphoma in parotidectomy for Warthin's tumor: Case
report and review of the literature. Int J Hematol. 89:359–364.
2009. View Article : Google Scholar : PubMed/NCBI
|