Introduction
Renal cell carcinoma (RCC) is the most common kidney
tumor, accounting for almost 3% of all human malignancies; 70–80%
of RCC cases are clear cell RCC (ccRCC) (1–3).
Metastasis and recurrence rates in ccRCC, as well as its poor
prognosis, lead to poor survival rates in patients (4). Currently, the pathogenesis of ccRCC
remains unclear.
Caspases serve an essential role in cell apoptosis.
Caspases-10 and −8 act as initiators, whereas caspase-9 acts as an
initiator of the intrinsic apoptosis pathway. Caspase-3 is
considered to be the main effector caspase involved in extrinsic
and intrinsic pathways (5).
Alteration of the apoptotic pathway is essential for tumor
development; thus, analysis of the expression levels of caspases in
tumor tissues is necessary for a deeper understanding of tumor
biology. In a previous study, immunopositivity of caspase-10 was
observed in 58 (97%) of 60 advanced gastric adenocarcinomas using
immunohistochemistry (IHC) using tissue microarrays (5). Tumor necrosis factor-related
apoptosis-inducing ligand, which induces apoptosis in Ewing's
sarcoma family tumors, requires caspase activation; furthermore,
caspase-10 was revealed to be activated earlier than other caspases
in the signaling pathway (6). cDNA
microarrays also revealed that caspase-10 was downregulated in
gastric carcinoma, compared with adjacent non-cancerous tissue
(7). The antitumor effect of
immunotherapeutic and chemotherapeutic agents is executed through
stimulation of apoptotic programs, via the activation of members of
the caspase family in susceptible cells. Resistance to
drug-inducing apoptosis in RCC cell lines is considered to be
correlated with downregulation of caspase-10 (8). Nevertheless, it remains unclear whether
caspase-10 is involved in tumor development, particularly in
RCC.
Matrix metalloproteinases (MMPs), a family of
zinc-dependent endopeptidases, are capable of degrading components
of the extracellular matrix and are implicated in tissue remodeling
and tumor infiltration (9). Using
various methods, a number of studies have analyzed MMP-9 expression
or its activities in tumor tissues, sera, plasma or urine of
patients with RCC. For example, IHC analysis revealed that MMP-9
levels in tumor tissues of RCC were significantly higher than those
in non-malignant tissues, and MMP-9 overexpression was positively
associated with clinical staging, pathological grade and
metastasis, and the shorter survival rate of RCC patients (9–12). In
addition, pro-MMP-9, but not activated MMP-9, was detected using
gelatin zymography and western blot in RCC samples (13). BIOTRAK activity assay systems and
in situ hybridization also established higher MMP-9 mRNA and
protein levels in tumor tissues than those in adjacent
non-malignant tissues (10,14). Additionally, cDNA microarray and
gelatin zymography revealed that MMP-9 transcript levels were
strongly correlated with MMP-9 enzymatic activity, disease-free
survival rate and metastasis in RCC, suggesting that MMP-9 may be
regulated at the transcript level and may be a candidate of
predictors of disease-free survival rate in RCC patients (15). Other studies investigated 16 patients
with ccRCC with ELISA assays, and revealed that MMP-9 levels in
sera, urine and plasma samples were higher in patients with ccRCC
than in healthy controls (14,16).
Gelatin zymography or ELISA were also used for analysis of sera and
urine of 16 patients with ccRCC, and revealed that MMP-9 activity
or expression levels in sera and urine may not be useful biomarkers
for kidney carcinomas, despite opposing conclusions in other
publications (17,18). Therefore, the majority of these
studies suggested that MMP-9 may be involved in the pathogenesis of
RCC.
Laminins (LMs) are large molecular-weight trimer
glycoproteins consisting of α, β and γ subunits, which integrate in
almost all basement membranes (BMs) (19). A previous report has suggested that LM
trimers are assembled inside the cell, and the extracellular
proteolytic processing of various subunits leads to their final
forms (20). In addition to their
function as a scaffold for BMs, LMs can also interact with cell
surface receptors, including integrins, to control signaling events
that regulate cell proliferation, migration and differentiation
(21,22). During tumor invasion, loss of the BM
barrier occurs and a discontinuous pattern of LM staining is
observed (23). IHC results indicated
that the loss of LM in tumor tissues was significantly correlated
with symptoms, tumor size and higher tumor grades in 75 RCC cases
(24). In other studies, which also
used IHC, tumor BMs of RCC revealed immunoreactivity for subunits
of LMα1, LMβ1, LMγ1 and LMβ2 (25,26).
Additionally, in cultured RCC cells, an abundant production of
LM111, but not of LM332, was observed, whereas xenografts of the
same cell revealed BM-confined immunoreactivity for LM111 and LM332
(25). Assessment of microarray data
of early metastatic and non-metastatic ccRCC samples confirmed
LMα1, LMα2 and LMα4 as potential target genes associated with early
metastatic ccRCC (27). Western blot
analysis conducted in another study revealed that LM levels in
urine of patients with RCC were significantly lower than those in
healthy controls (28). All these
results imply that abnormal expression of total LMs or certain LM
subunits are possibly correlated with RCC.
The purpose of the present study was to investigate
the expression levels of caspase-10, MMP-9 and total LM in tumor
tissues and their adjacent non-malignant tissues of patients with
ccRCC, and further elucidate the possible correlation of the three
factors and ccRCC, and the possible correlation among these factors
and clinical data of patients with ccRCC.
Materials and methods
Patient tissue samples
Tumor tissues and adjacent non-malignant tumor
tissues were collected from 27 patients (14 male, 11 female and 2
unknown; mean age, 57.8; age range, 42–70) with ccRCC who underwent
surgical procedure at the Department of Urology, Harbin Medical
University Cancer Hospital (Harbin, China) from March 2015 to May
2017. Diagnosis of tumors was made by the usual clinical laboratory
criteria and confirmed postoperatively by histopathological
findings (16). The tumors were
classified for grade and stage according to the pathological
Tumor-Node-Metastasis (pTNM) classification (29). The clinical information of these 27
patients is summarized in Table I.
Written informed consent was obtained from all patients. All
experiments were conducted under approval from the Internal Review
Board of Harbin Medical University and in compliance with the
Declaration of Helsinki.
 | Table I.Clinical information of patients with
clear cell renal cell carcinoma. |
Table I.
Clinical information of patients with
clear cell renal cell carcinoma.
| Patient number | Sex | Age | Tumor stage | Tumor grade | Maximal tumor
diameter, cm |
|---|
| 1 | Female | 55 | T1aN0M0 | 1 | 3.5 |
| 2 | Male | 55 | T1aN0M0 | 1 | 3.5 |
| 3 | Female | 70 | T3aN0M0 | 3 | 7 |
| 4 | Male | 52 | T2aN0M0 | 2 | 8 |
| 5 | Female | 64 | T1bN0M0 | 1 | 4.7 |
| 6 | Male | 59 | T1aN0M0 | 1 | 3.8 |
| 7 | Male | 69 | UC | UC | 4.7 |
| 8 | Male | 42 | T4N1M1 | 4 | 9 |
| 9 | Female | 49 | T1bN0M0 | 1 | 5.5 |
| 10 | Female | 66 | T1bN0M0 | 1 | 7.6 |
| 11 | Female | 66 | T1aN0M0 | 1 | 3 |
| 12 | Female | 46 | UC | UC | UC |
| 13 | Female | 62 | T2aN0M0 | 2 | 8 |
| 14 | Female | 61 | T1aN0M0 | 1 | 4 |
| 15 | Male | 59 | T3b | 3 | 5 |
| 16 | Male | 46 | T1bN0M0 | 1 | 6.5 |
| 17 | Female | 67 | T3bN0M0 | 3 | 3.5 |
| 18 | UC | UC | UC | UC | UC |
| 19 | Male | 56 | T1bN0M0 | 1 | 4.5 |
| 20 | Female | 67 | T1aN0M0 | 1 | 4 |
| 21 | Male | 52 | T1aN0M0 | 1 | 3.5 |
| 22 | Male | 55 | T1aN0M0 | 1 | 4 |
| 23 | Male | 57 | T1aN0M0 | 1 | 3.5 |
| 24 | Male | 58 | T1bN0M0 | 1 | 6 |
| 25 | UC | UC | UC | UC | UC |
| 26 | Male | 44 | UC | UC | UC |
| 27 | Male | 69 | T2bN0M0 | 2 | 2.5 |
Tissue protein lysate preparation and
protein concentration determination
Tissue samples were lysed with cold
radioimmunoprecipitation assay buffer (cat. no. P0013B; Beyotime
Institute of Biotechnology, Shanghai, China) at 4°C overnight.
Following centrifugation at 14,000 × g at 4°C for 20 min, the
supernatant was harvested as tissue protein lysate, which was
stored at −80°C until use. The protein concentration of all tissue
protein lysates was measured using a bicinchoninic acid assay kit
(cat. no. P0011; Beyotime Institute of Biotechnology, Shanghai,
China) according to the manufacturer's protocols. Tissue protein
lysates were diluted to a concentration of 1 µg/ml prior to the any
subsequent experiments.
ELISA
Capsase-10, MMP-9 and total LM levels in tumor
tissues and adjacent non-malignant tissues of patients with ccRCC
were determined by a capase-10 ELISA kit (cat. no. JL45340;
Jianglaibio, Shanghai, China), MMP-9 ELISA kit (cat. no.
CSB-E08006h; Cusabio, Wuhan, China) and total LM ELISA kit (cat.
no. E-EL-H0128c; Elabscience, Houston, TX, USA), respectively. The
antibodies used in the LM ELISA kit were polyclonal antibodies
against all types of LMα, LMβ and LMγ subunits. All experiments
were performed according to the manufacturer's protocols for the
respective ELISA kits. All sample measurements were repeated
twice.
Statistical analysis
All sample measurements were repeated twice and the
data were presented as mean ± standard deviation. Statistical
analysis was performed using SigmaPlot 12.0 (Hulinks, Inc., Tokyo,
Japan). Paired Student's t-tests and Wilcoxon signed rank tests
were used to compare the difference between caspase-10, MMP-9 and
total LM levels in tumor tissues and their adjacent non-malignant
tissues in patients with ccRCC. Pearson's correlation was used to
analyze the correlation between ccRCC clinical data and caspase-10,
MMP-9 and total LM. P<0.05 was considered to indicate a
statistically significant difference.
Results
Detection of caspase-10, MMP-9 and
total LM in tumor and adjacent non-malignant tissues of patients
with ccRCC by ELISA
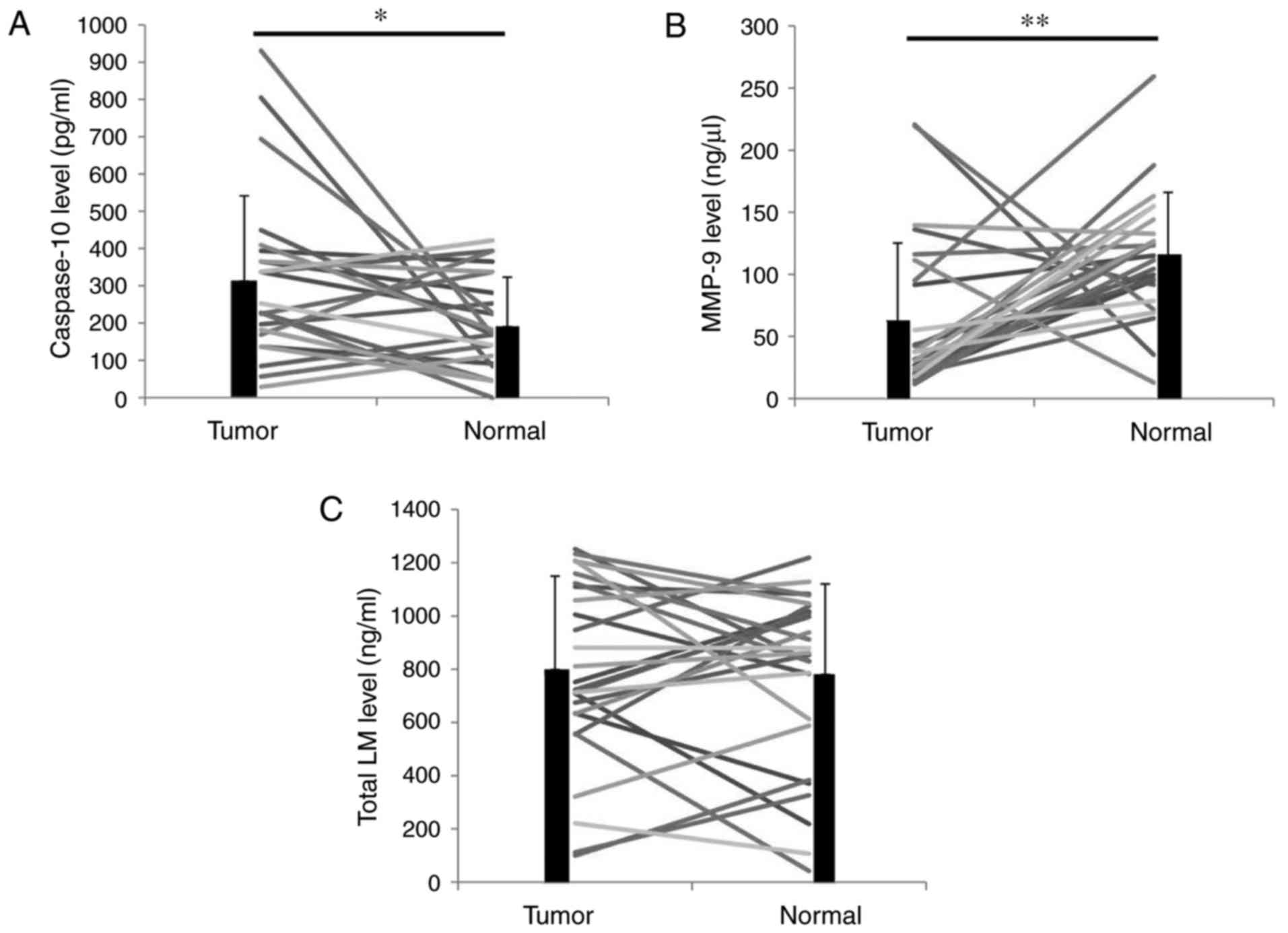
Tumor tissues and adjacent non-malignant tissues
were obtained from 27 patients with ccRCC. The protein
concentration of all tissue protein lysates was analyzed and
resuspended at 1 µg/ml. ELISA kits were then used to detect
caspase-10, MMP-9 and total LM levels in these protein lysates. The
caspase-10 levels in the tumor tissues were significantly higher
than those in the adjacent non-malignant tissues (P<0.05;
Fig. 1A). However, the MMP-9 levels
in the tumor tissues were significantly lower than those in the
adjacent non-malignant tissues (P<0.01; Fig. 1B). No statistical difference was
observed between the total LM levels in the tumor tissues and those
in the adjacent non-malignant tissues (P=0.757; Fig. 1C).
Correlation of caspase-10, MMP-9 and
total LM protein levels in tumor and adjacent non-malignant tissues
of patients with ccRCC
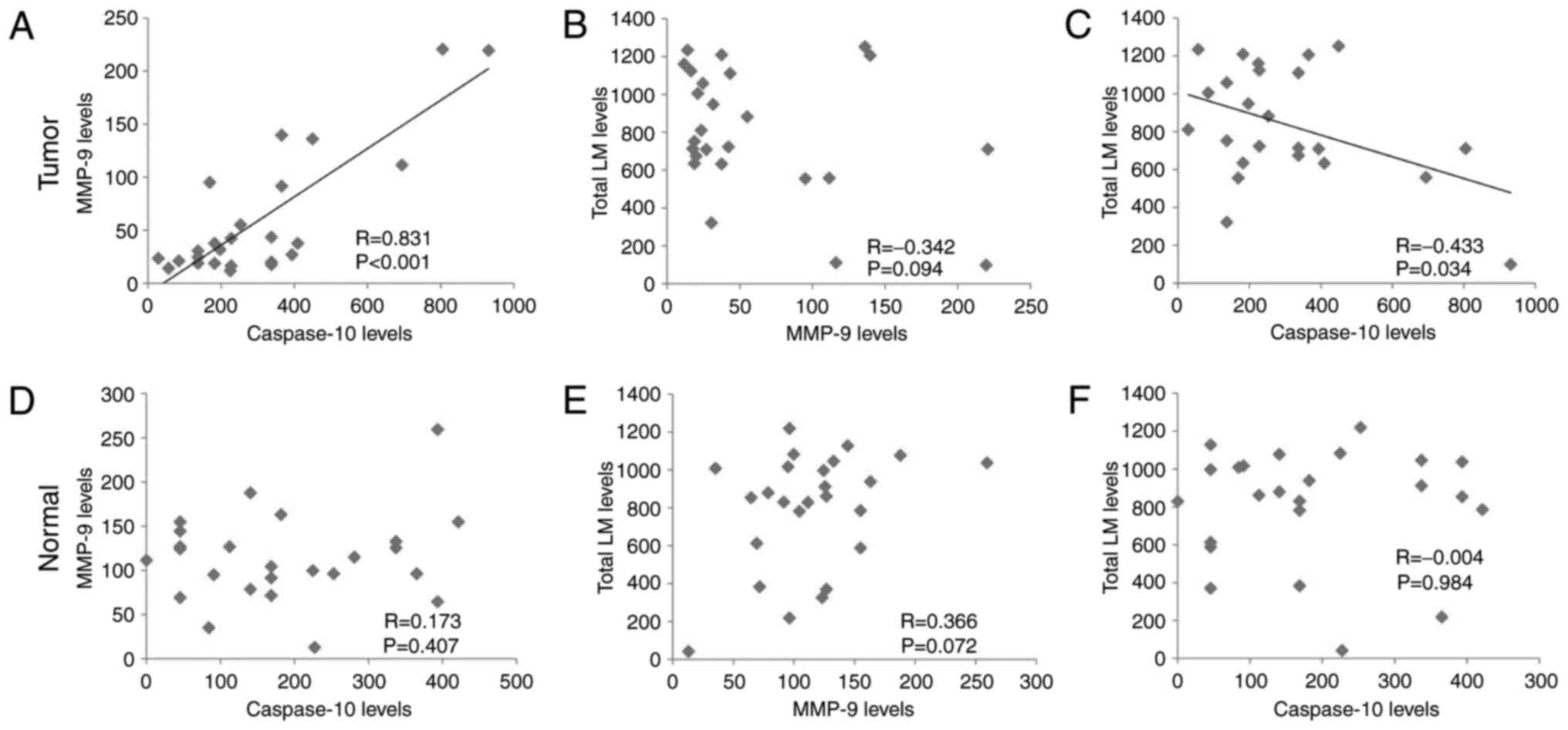
The protein levels of caspase-10, MMP-9 and total LM
in tumor and adjacent non-malignant tissues were subjected to
correlation analyses. In the tumor tissues, caspase-10 levels were
positively correlated with MMP-9 levels (P<0.001; Fig. 2A), but MMP-9 levels revealed no
correlation with total LM levels (P=0.094; Fig. 2B) and total LM levels were negatively
correlated with caspase-10 levels (P<0.05; Fig. 2C). In adjacent non-malignant tissues,
the levels of caspase-10, MMP-9 and total LM exhibited no
correlation among each other (Fig.
2D-F).
Correlation of ccRCC clinical data
with the levels of caspase-10, MMP-9 and total LM
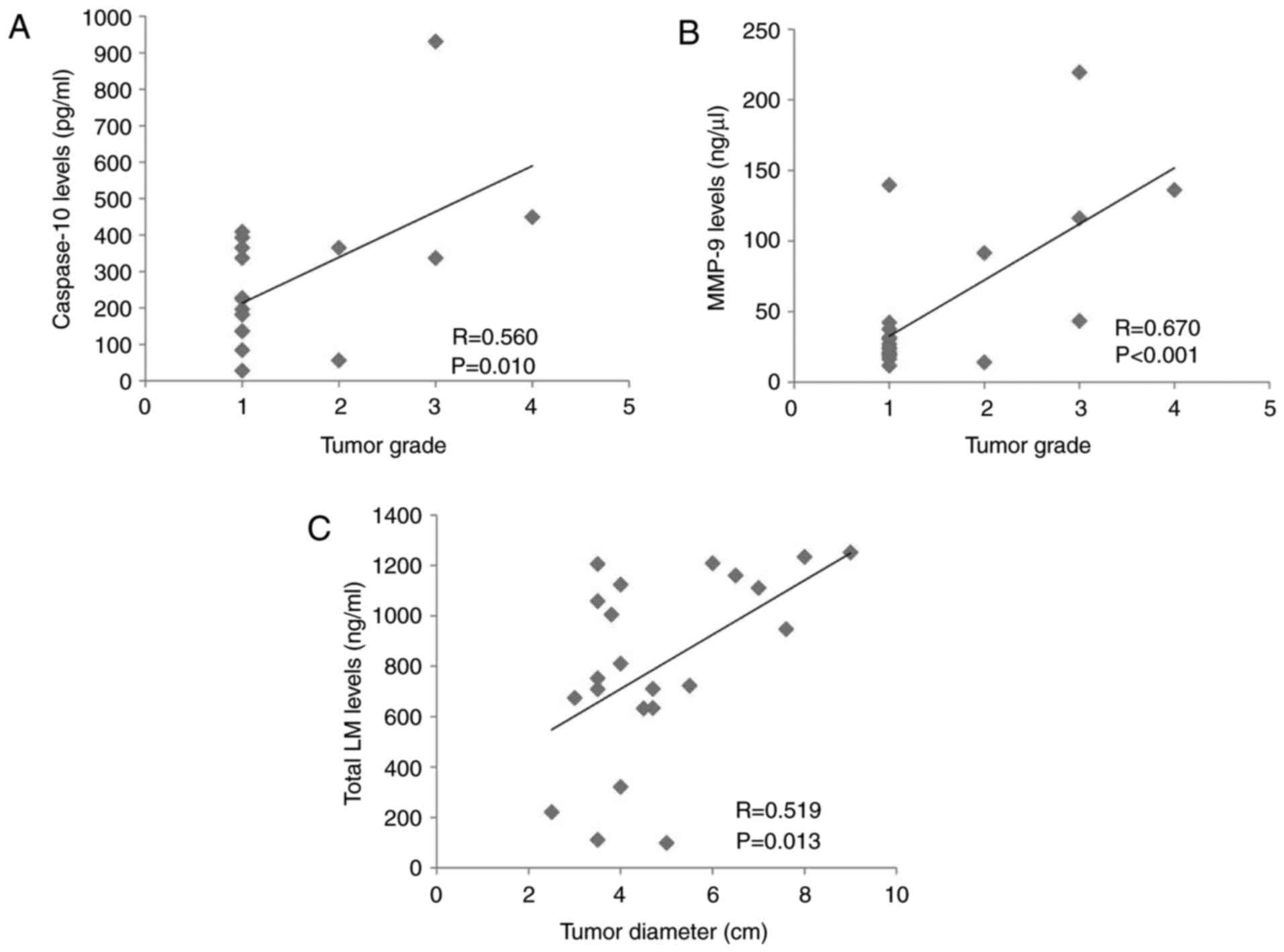
The clinical data of the patients with ccRCC
involved in the present study are presented in Table I. Positive correlation was revealed
between tumor grades and maximal tumor diameters (P<0.05), but
no other correlation was revealed among the parameters of the
clinical data of patients with ccRCC (data not shown). Analyses
were next performed between the levels of caspase-10, MMP-9 and
total LM and the clinical data of patients with ccRCC, including
age, sex, tumor grade and maximal tumor diameters. The
statistically significant data are included in Fig. 3. The tumor grade of patients with
ccRCC was positively correlated with caspase-10 levels (P<0.05;
Fig. 3A) and MMP-9 levels
(P<0.001; Fig. 3B) in the tumor
tissue. In addition, the maximal tumor diameter was positively
correlated with the level of total LM in the tumor tissue
(P<0.05; Fig. 3C).
Discussion
In the present study, caspase-10, MMP-9 and total LM
levels in tumor and adjacent non-malignant tissue from 27 patients
with ccRCC were detected by ELISA. The tumor tissues revealed
significantly higher levels of caspase-10 and lower levels of MMP-9
than the adjacent non-malignant tissues, but similar total LM
levels. Statistical analysis indicated that caspase-10 levels were
positively correlated with MMP-9 levels (P<0.001), but
negatively correlated with total LM levels (P<0.05) in the tumor
tissues. Correlation analyses confirmed that levels of caspase-10
(P<0.05) and MMP-9 (P<0.001) in tumor tissues were positively
correlated with ccRCC tumor grades, and total LM levels in the
tumor tissues were positively correlated with the tumor size in
patients with ccRCC.
Caspase-10 has been investigated in tumor-related
studies mainly due to its involvement in cell apoptosis. To the
best of our knowledge, the current study is the first report on
caspase-10 detection in tumor tissues from patients with ccRCC.
Using ELISA, it was confirmed that caspase-10 levels in tumor
tissues from patients with ccRCC were significantly higher than
those in the adjacent non-malignant tissues. Furthermore,
caspase-10 levels in tumor tissues were positively correlated with
the tumor grades of patients with ccRCC. These results indicated
that caspase-10 may promote tumor development and be a potential
pathological marker for ccRCC. Furthermore, it was revealed that
caspase-10 levels were positively correlated with MMP-9 levels
(P<0.001) and negatively correlated with total LM levels
(P<0.05) in the tumor tissues. These results imply that
caspase-10 may promote tumor development of ccRCC via upregulation
of MMP-9 and downregulation of LMs, which should be clarified in
future studies.
MMP-9 protein expression levels in patients with RCC
have been reported in a number of studies, the majority of which
analyzed MMP-9 levels in tumor tissue samples by IHC. The findings
of these investigations revealed that MMP-9 levels in tumor tissues
were higher than those in the adjacent non-malignant tissues, and
MMP-9 overexpression was positively correlated with tumor grades of
patients with RCC (9–12). In the present study, MMP-9 levels were
analyzed by ELISA; it was revealed that MMP-9 levels were
significantly lower in tumor tissues than in the adjacent
non-malignant tissues of ccRCC, which is contradictory to previous
studies (9–12). The different tissue samples and
methods used for detection of MMP-9 levels may have led to these
discrepancies in results. The contradictory results may also imply
the complexities of the role of MMP-9 in the pathogenesis of RCC.
In the present study, it was confirmed that MMP-9 levels in tumor
tissues were positively correlated with tumor grades of ccRCC
(P<0.001), which is consistent with the results of previous
studies (9,11). The finding from the present study
indicated that MMP-9 may promote tumor development in ccRCC.
However, this point also seems to be contradictory to the
relatively lower MMP-9 levels in the tumor tissues, compared with
those in the adjacent non-malignant tissues. Therefore, it is
hypothesized that MMP-9 levels in the tumor and the adjacent
non-malignant tissues may be independent, or be two different
isoforms of MMP-9 with different functions. Further analyses of the
various molecular weights of MMP-9 in the tumor and adjacent
non-malignant tissues of RCC cases and their functions using
experimental models may be of use. MMP-9 is known to enhance tumor
migration and angiogenesis via degradation of extracellular matrix
molecules including LMs (30). In the
present study, MMP-9 levels in the tumor tissues of ccRCC tended to
be negatively correlated with the total LM levels (P=0.094). This
result suggested that MMP-9 may contribute to the pathogenesis of
ccRCC via degradation of LMs. The lack of statistical significance
may be caused by the limited numbers of samples analyzed or
targeting of only certain LM subunit(s)/trimer(s) by MMP-9.
Therefore, it is necessary to clarify what LM subunits or LM
trimers are influenced by MMP-9 in ccRCC.
During tumor invasion, the BM barrier is removed,
and a discontinuous pattern of LM staining is observed (23). In RCC, LM loss in the tumor tissues,
as established by IHC, was suggested to be correlated with
symptoms, tumor size and a higher tumor grade (24). However, in the present study, no
differences in total LM levels in the tumor and adjacent
non-malignant tissues of ccRCC were revealed by ELISA. These
discrepancies in results may be due to the different detection
methods used. ELISAs which used coating and primary antibodies
against LMs in the present study may have a relatively higher
specificity than IHC, in which only the primary antibody is used.
In the present study, it was also demonstrated that total LM levels
in tumor tissues were positively correlated with tumor size in
patients with ccRCC, which is similar to the findings of a previous
study (24). This result suggested
that LMs in tumor tissues may promote the tumor development in
ccRCC. Therefore, considering the results obtained, it can be
concluded that certain LM subunit(s) or trimer(s) likely contribute
to tumor development. LM has 5 α, 3 β and 3 γ subunits and their
distribution is tissue-specific (20). LM exists extensively in malignant
cells, non-malignant cells, BM and endothelial cells of blood
vessels (20). Therefore, in tumor
tissues of patients with RCC, the total LM levels reflect the
levels of various LM subunits in all cells and tissues involved. It
has been suggested that RCC tumor tissues may have LMα1-4, LMβ1-3
LMγ1-2 subunits (25–27). In future studies, it is necessary to
define what LM subunit(s) contributed to the total LM changes in
RCC tumor tissues and to elucidate the possible mechanisms of
pathogenesis.
It is well accepted that decreased expression levels
of caspase-3 and LMs and increased MMP-9 in tumor tissue were
linked to the pathogenesis of tumor development in various
malignant types of cancer (23,31,32). By
contrast, increased caspase-10, decreased MMP-9 and unchanged total
LMs were revealed in the tumor tissues of ccRCC in the present
study. These apparently discrepant results provide new and
important insights into the pathogenesis of ccRCC. The positive
correlation between caspase-10 and MMP-9, the negative correlation
between caspase-10 and total LMs imply that caspase-10, MMP-9 and
LMs may regulate each other in vivo and contribute to the
pathogenesis of ccRCC. In the present study, tumor grades were
positively correlated with maximal tumor diameters in patients with
ccRCC. Caspase-10 and MMP-9 were positively correlated with tumor
grades but not tumor diameters, whereas total LMs were positively
correlated with tumor diameters but not tumor grades; these results
appear to be contradictory. It is hypothesized that caspase-10 and
MMP-9 may contribute directly to tumor invasion (one factor of
tumor grade) and indirectly to tumor diameters (another factor of
tumor grade) by regulation of LMs.
The lower number of tissue samples of patients with
ccRCC and the application of only one detection method are
limitations of the present study. Therefore, further studies with a
greater number of tissue samples and detection methods would be of
benefit. In addition, the correlation among caspase-10, MMP-9 and
LM in in vitro and in vivo experimental models of
ccRCC should be investigated in future studies.
Acknowledgements
Not applicable.
Funding
This study was supported by the Scientific Research
Fund of Heilongjiang Provincial Education Department (grant nos.
12521262 and 12531415), the Scientific Research Fund of
Heilongjiang Provincial Health Bureau (grant nos. 2011-031 and
2012-566), the Natural Science Foundation of Heilongjiang Province
of China (grant no. QC2016129) and the Postdoctoral Grant of
Heilongjiang Province (grant no. LBH-Z14154).
Availability of data and materials
The datasets analyzed during the current study are
available from the corresponding author on reasonable request.
Authors' contributions
HQ, XL, CL and YC designed the study. YSC, LT, WW,
DL, YX and YC gathered samples and data. WZ and XL provided project
guidance. HQ, XL, WZ, LM, XT, JS, YSC, LT, WW, DL and YX performed
the experiments and data analysis. XL and YC revised the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All experiments were performed with the approval of
the Internal Review Board of Harbin Medical University and in
compliance with the Declaration of Helsinki. Informed consent was
obtained from all patients prior to mortality or from their
families following mortality for inclusion of autopsy data.
Consent for publication
The patients involved in this study provided written
informed consent for the publication of any associated data and
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
RCC
|
renal cell carcinoma
|
|
ccRCC
|
clear cell RCC
|
|
IHC
|
immunohistochemistry
|
|
MMP-9
|
matrix metalloproteinase-9
|
|
LM
|
laminin
|
|
BMs
|
basement membranes
|
References
|
1
|
Diaz JI, Mora LB and Hakam A: The mainz
classification of renal cell tumors. Cancer Control. 6:571–579.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rosner I, Bratslavsky G, Pinto PA and
Linehan WM: The clinical implications of the genetics of renal cell
carcinoma. Urol Oncol. 27:131–136. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Novara G, Ficarra V, Antonelli A, Artibani
W, Bertini R, Carini M, Cosciani Cunico S, Imbimbo C, Longo N,
Martignoni G, et al: Validation of the 2009 TNM version in a large
multi-institutional cohort of patients treated for renal cell
carcinoma: Are further improvements needed? Eur Urol. 58:588–595.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yoo NJ, Kim HS, Kim SY, Park WS, Kim SH,
Lee JY and Lee SH: Stomach cancer highly expresses both initiator
and effector caspases: An immunohistochemical study. APMIS.
110:825–832. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mitsiades N, Poulaki V, Mitsiades C and
Tsokos M: Ewing's sarcoma family tumors are sensitive to tumor
necrosis factor-related apoptosis-inducing ligand and express death
receptor 4 and death receptor 5. Cancer Res. 61:2704–2712.
2001.PubMed/NCBI
|
|
7
|
Liu LX, Liu ZH, Jiang HC, Qu X, Zhang WH,
Wu LF, Zhu AL, Wang XQ and Wu M: Profiling of differentially
expressed genes in human gastric carcinoma by cDNA expression
array. World J Gastroenterol. 8:580–585. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kolenko V, Uzzo RG, Bukowski R, Bander NH,
Novick AC, His ED and Finke JH: Dead or dying: Necrosis versus
apoptosis in caspase-deficient human renal cell carcinoma. Cancer
Res. 59:2838–2842. 1999.PubMed/NCBI
|
|
9
|
Kallakury BV, Karikehalli S, Haholu A,
Sheehan CE, Azumi N and Ross JS: Increased expression of matrix
metalloproteinases 2 and 9 and tissue inhibitors of
metalloproteinases 1 and 2 correlate with poor prognostic variables
in renal cell carcinoma. Clin Cancer Res. 7:3113–3119.
2001.PubMed/NCBI
|
|
10
|
Bhuvarahamurthy V, Kristiansen GO,
Johannsen M, Johannsen M, Loening SA, Schnorr D, Jung K and Staack
A: In situ gene expression and localization of metalloproteinases
MMP1, MMP2, MMP3, MMP9, and their inhibitors TIMP1 and TIMP2 in
human renal cell carcinoma. Oncol Rep. 15:1379–1384.
2006.PubMed/NCBI
|
|
11
|
Lin H, Pan JC, Zhang FM, Huang B, Chen X,
Zhuang JT, Wang H, Mo CQ, Wang DH and Qiu SP: Matrix
metalloproteinase-9 is required for vasculogenic mimicry by clear
cell renal carcinoma cells. Urol Oncol. 33:168.e9–16. 2015.
View Article : Google Scholar
|
|
12
|
Kawata N, Nagane Y, Igarashi T, Hirakata
H, Ichinose T, Hachiya T, Takimoto Y and Takahashi S: Strong
significant correlation between MMP-9 and systemic symptoms in
patients with localized renal cell carcinoma. Urology. 68:523–527.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kamiya N, Kishimoto T, Suzuki H, Sekita N,
Nagai Y, Oosumi N, Kito H, Tochigi N, Shinbo M, Nemori R, et al:
Increased in situ gelatinolytic activity in renal cell tumor
tissues correlates with tumor size, grade and vessel invasion. Int
J Cancer. 106:480–485. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lein M, Jung K, Laube C, Hübner T,
Winkelmann B, Stephan C, Hauptmann S, Rudolph B, Schnorr D and
Loening SA: Matrix-metalloproteinases and their inhibitors in
plasma and tumor tissue of patients with renal cell carcinoma. Int
J Cancer. 85:801–804. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cho NH, Shim HS, Rha SY, Kang SH, Hong SH,
Choi YD, Hong SJ and Cho SH: Increased expression of matrix
metalloproteinase 9 correlates with poor prognostic variables in
renal cell carcinoma. Eur Urol. 44:560–566. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
DI Carlo A: Evaluation of neutrophil
gelatinase-associated lipocalin (NGAL), matrix metalloproteinase-9
(MMP-9) and their complex MMP-9/NGAL in sera and urine of patients
with kidney tumors. Oncol Lett. 5:1677–1681. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Di Carlo A: Matrix metalloproteinase-2 and
−9 in the sera and in the urine of human oncocytoma and renal cell
carcinoma. Oncol Rep. 28:1051–1056. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
DI Carlo A: Matrix metalloproteinase-2 and
−9 and tissue inhibitor of metalloproteinase-1 and −2 in sera and
urine of patients with renal carcinoma. Oncol Lett. 7:621–626.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Schéele S, Nyström A, Durbeej M, Talts JF,
Ekblom M and Ekblom P: Laminin isoforms in development and disease.
J Mol Med (Berl). 85:825–836. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Durbeej M: Laminins. Cell Tissue Res.
339:259–268. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yurchenco PD and Patton BL: Developmental
and pathogenic mechanisms of basement membrane assembly. Curr Pharm
Des. 15:1277–1294. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Miner JH and Yurchenco PD: Laminin
functions in tissue morphogenesis. Annu Res Cell Dev Biol.
20:255–284. 2004. View Article : Google Scholar
|
|
23
|
Patarroyo M, Tryggvason K and Virtanen I:
Laminin isoforms in tumor invasion, angiogenesis and metastasis.
Semin Cancer Biol. 12:197–207. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Morell-Quadreny L, Rubio J, Lopez-Guerrero
JA, Casanova J, Ramos D, Iborra I, Solsona E and Llombart-Bosch A:
Disruption of basement membrane, extracellular matrix
metalloproteinases and E-cadherin in renal-cell carcinoma.
Anticancer Res. 23:5005–5010. 2003.PubMed/NCBI
|
|
25
|
Lohi J, Tani T, Leivo I, Linnala A, Kangas
L, Burgeson RE, Lehto VP and Virtanen I: Expression of laminin in
renal-cell carcinomas, renal-cell carcinoma cell lines and
xenografts in nude mice. Int J Cancer. 68:364–371. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rissanen J, Korhonen M, Lehto VP and
Virtanen I: Laminin alpha1 chain in human renal cell carcinomas and
integrin-mediated adhesion of renal cell carcinoma cells to human
laminin isoforms. J Pathol. 200:157–167. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang H, Huo P, Hu G, Wei B, Kong D and Li
H: Identification of gene markers associated with metastasis in
clear cell renal cell carcinoma. Oncol Lett. 13:4755–4761. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sherief MH, Low SH, Miura M, Kudo N,
Novick AC and Weimbs T: Matrix metalloproteinase activity in urine
of patients with renal cell carcinoma leads to degradation of
extracellular matrix proteins: Possible use as a screening assay. J
Urol. 169:1530–1534. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sobin LH and Wittekind CH: International
Union Against Cancer (UICC) TNM classification of malignant tumors.
6th edition. Wiley-Liss; New York; pp. 193–195. 2002
|
|
30
|
Visse R and Nagase H: Matrix
metalloproteinases and tissue inhibitors of metalloproteinases
structure, function, and biochemistry. Circ Res. 92:827–839. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tian HY, Li ZX, Li HY, Wang HJ, Zhu XW and
Dou ZH: Effects of 14 single herbs on the induction of caspase-3 in
tumor cells: A brief review. Chin J Integr Med. 19:636–640. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Himelstein BP, Canete-Soler R, Bernhard
EJ, Dilks DW and Muschel RJ: Metalloproteinases in tumor
progression: The contribution of MMP-9. Invasion Metastasis.
14:246–258. 1994.-1995. PubMed/NCBI
|