Introduction
In familial adenomatous polyposis (FAP) context,
extra-colonic features may include osteomas and dental
abnormalities, congenital hypertrophy or hyperplasia of the retinal
pigment epithelium, upper gastrointestinal tumors, epidermoid cysts
and lipomas, adrenal tumors, hepatoblastoma, brain tumors and
pancreatic cancer. Also, papillary thyroid cancer and fibromatosis
can occur (1,2).
The cribriform-morular papillary thyroid carcinoma
is the most common morphologic variant found in FAP-associated
thyroid carcinoma, exhibits nuclear and cytoplasmic accumulation of
β-catenin and is associate with germline or somatic mutation of
adenomatous polyposis coli (APC) and 3-catenin (CTNNB1)
genes (3).
Fibromatosis is a benign neoplasm with infiltrative
growth and consequent high potential to recur after surgical
excision (2,4,5). It occurs
predominantly in adults, sporadically or in association with FAP
syndrome (2). In FAP setting,
fibromatosis usually follows a surgical trauma, occurs in 15 to 20%
of the patients, is more frequent in women (ratio 1:3) (2,6), and has a
significantly increased rate of occurrence. Studies on APC
genotype-phenotype correlation identified that mutations in the
3′end and downstream of codon 1400 in the APC have an increased
risk of fibromatosis development (1).
Although breast fibromatosis is very rare (less than 0.2% of all
breast tumors), it occurs mainly as a sporadic form. Trauma and
previous surgery are the most important contributing factors
(6,7)
namely after the placement of breast prosthetics (5,6,8,9). This last
type can occur associated with either saline or silicone
prosthetics (6).
Pathophysiology of fibromatosis is still not
completely understood, but it could result from a disturbance of
cell proliferation following a trauma, a dysfunctional hormonal
dependence of the local fibroblasts, or a genetic disorder in the
regulation of fibroblast growth field (10). Alterations of the APC/β-catenin
pathway with resultant nuclear translocation of β-catenin were
described in the pathogenesis of both sporadic and FAP-associated
breast fibromatosis (11) but mostly
resulted from sporadic mutations in the β-catenin subunit (11). An unique case of bilateral
fibromatosis in Gardner syndrome was reported in 1970 by Haggitt
and Booth (12).
The relevance of illustrating the present case is to
alert that, in classic FAP, the possibility of this serious
complication must be considered in the decision to place breast
implants. We also aim to contribute to the knowledge of the
relationship between the APC gene mutation and the consequent
phenotype, in order to prevent the development of deleterious
conditions in FAP patients.
Case report
Clinical summary
We report a case of a 33-year-old woman with a
classic FAP, with a cribriform-morular morphologic variant of
papillary thyroid carcinoma (CMV-PTC) and also with bilateral
breast fibromatosis in the context of silicone prosthetics.
Previous family history was relevant, as her father had a colon
cancer diagnosed at the age of 34 that was found to be in the
context of FAP and died at the age of 38. At that time, at the age
of 16 years old, our patient was referred to our Family Risk
Consulting and underwent a flexible sigmoidoscopy that revealed few
adenomas. A nonsense mutation (c.935C>A) at codon 935 in exon 15
of APC gene was found and the patient was also diagnosed
with FAP.
The search of extra-colonic manifestations of the
disease found a papillary thyroid carcinoma cribriform-morular
variant treated with total thyroidectomy and with no signs of
relapse until now. No other extra-colonic manifestations were
found.
She underwent surveillance with annual colonoscopy
and the polyps' number and size allowed to postponed prophylactic
surgery. At the age of 23, the patient had about 80 colonic polyps
and underwent a rectum-sparing total colectomy, with ileorectal
anastomosis. Pathologic analysis of the colectomy specimen revealed
more than 100 tubular and tubulovillous adenomas with low-grade
dysplasia. The patient began to be followed with annual rectoscopy
and upper endoscopy according to Spigelman classification for
duodenal polyposis.
A breast augmentation surgery with retropectoral
silicone prosthetics was performed for cosmetic purposes, at the
age of 30 in another institution.
About one year later, she developed complaints of a
growing tenderness in the right breast. The magnetic resonance
imaging (MRI) showed a 10 cm longitudinal diameter mass in the
right breast, limited anteriorly by the pectoralis major muscle and
the silicone prosthetics, with invasion of the pectoralis minor
muscle and with an intrathoracic component between the 4th and the
5th rib and also, in the left breast, a 4 cm mass was detected,
without intrathoracic component. (Fig.
1A). The breast bilateral tumors were diagnosed in core
biopsies as fibromatosis. The patient was under levothyroxine and
an etonogestrel subdermal implant medication that was removed after
the histological diagnosis of fibromatosis.
 | Figure 1.(A) MRI at diagnosis. Lesion on the
right breast with 10 cm in longitudinal diameter, limited
anteriorly by the pectoralis major muscle and the silicone
prosthetics. Invasion of the pectoralis minor muscle and an
intrathoracic component between the 4th and the 5th rib was also
observed. Lesion in the left breast with 4 cm was detected, without
intrathoracic component. (B) MRI after 2 months of hormonal therapy
with tamoxifen. Lesion on the right breast increased in size to 12
cm in transversal largest cross shaft. Lesion in the left breast
did not experience increase in size (3,9×1,9 cm). (C) MRI before
surgical treatment, one year after the diagnosis. Lesion on the
right breast increased in size (13,7×9,6×14,5 cm). Lesion in the
left breast is similar in size comparing with previous studies
(6,4×5,4×3,1 cm). |
Treatment with 40 mg per day of tamoxifen was
started one month later but no regression of the mammary
fibromatosis masses was observed (Fig.
1B). Surgical treatment with bilateral mastectomy and removal
of the prosthetics was performed one year after the diagnosis
(Fig. 1C). For the right breast,
resection of 4th and 5th costal arches and plastic surgical
reconstruction of the thoracic wall with a myocutaneous retail from
latissimus dorsi muscle was also carried out. Resection was made
with negative surgical margins for both breast tumors.
A relapse in the right thoracic wall, confirmed by a
core biopsy, occurred one year after and was again surgically
removed.
Currently, regarding the colonic tumors, the patient
is controlled and well and maintains appropriated surveillance for
new relapses of fibromatosis 24 months after second surgery.
APC mutation analysis
Mutation analysis of exons 1–14 of the APC
gene was performed by denaturing gradient gel electrophoresis
(DGGE) as described previously and by direct sequencing for some
exons (13,14). Exon 15 mutations were analyzed using
the protein truncation test (PTT), according to a method formerly
described (14). All DGGE and PTT
fragments showing an aberrant electrophoretic banding pattern were
sequenced using the Big Dye terminator cycle sequencing kit
(Applied Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA,
USA) on an automatic ABI Prism™ 310 Genetic Analyzer (Applied
Biosystems; Thermo Fisher Scientific, Inc.), in accordance with the
manufacturer's instructions. Mutation was compared with the
description of Genbank M74088 for APC gene.
Immunohistochemical studies
Immunostainings were performed by Ventana Bench Mark
ULTRA. The peroxidase-indirect-polymer method Ventana Ultraview
DAB, cat. no. 760-500, was used for primary antibodies
anti-estrogen receptor (Ventana Rabbit Monoclonal SP1, cat. no.
790-4324; Ventana Medical Systems, Inc., Tucson, AZ, USA). For
anti-β-catenin (Mouse Monoclonal cat. no. 5H10, ref. 80226,
1:1,000; Invitrogen; Thermo Fisher Scientific, Inc.) and
anti-cytokeratin (Dako Mouse Monoclonal AE1/AE3 cat. no. 3515,
1:100; Agilent Technologies, Inc., Santa Clara, CA, USA) Ventana
Optiview DAB cat. no. 760-700 was used. Sections with 3 µm thick
were cut, unto Superfrost plus slides from paraffin-embedded
routine tissue blocks. The heat mediated antigen retrieval was
Ventana CC1 52 min for primary antibodies anti-estrogen receptor;
40 min for anti-β-catenin; and a mixed CC1 16 min and Protease 3, 4
min for anti-AE1/AE3. As positive controls: A composite breast
tissue was used for anti-estrogen receptor, a composite colon
tissue for anti-β-catenin and a skin tissue for AE1/AE3. For
negative controls, primary antibodies were omitted during the
staining.
Mutational findings
A nonsense mutation (c.935C>A) at codon 935 in
exon 15 of APC gene was found in this patient, resulting in
a truncated protein.
Thyroid, total colon and bilateral
breast surgical specimens-histopathologic and immunohistochemical
findings
The total thyroidectomy showed identical right and
left lobes, both with 3×3×2 cm. In the right lobe, a well
delimitated intra-glandular, white nodule, with 6 mm was observed.
This tumor presented histological features compatible with the
CMV-PTC. Tumor cells showed strong cytoplasmic and nuclear
expression with β-catenin (Fig. 2).
Remaining thyroid parenchyma with no alterations.
The rectum-sparing total colectomy measured 153 cm,
had more than 100 tubular and tubulovillous adenomas <5 mm and
included appendix with no alterations.
The resected specimen from the right breast
mastectomy weighted 2,123 g, measured 24×19×11 cm and included two
segments of ribcage, with 9,5 cm. The specimen removed from the
left breast weighted 442 g and measured 17×11×6 cm. White, firm,
fibrotic lesions with infiltrative margins, were identified. The
prosthetics were intact. The excision was considered complete in
both breasts.
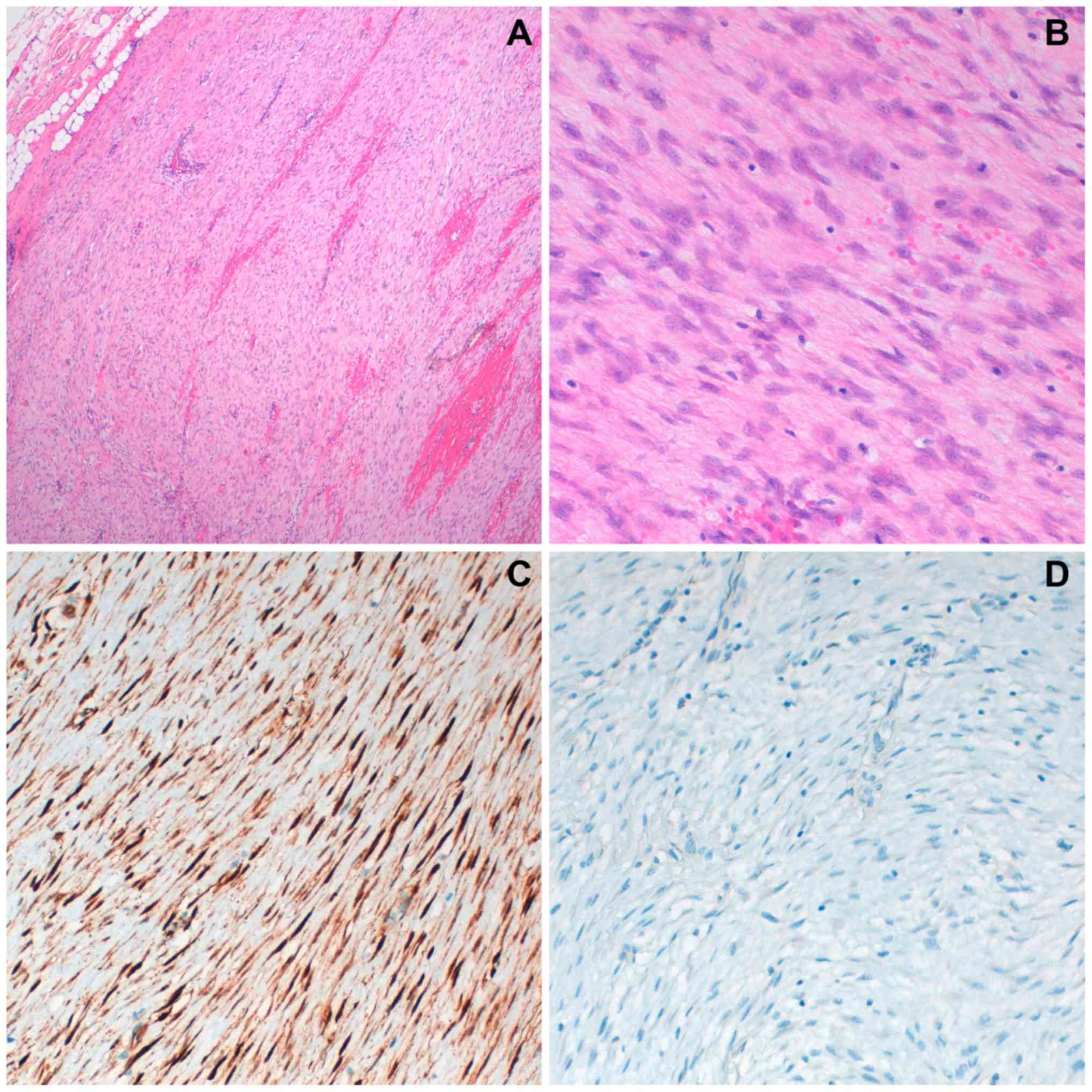
The histologic evaluation was similar to the
previous biopsy (Fig. 3A and B).
Immunohistochemistry with β-catenin and estrogen-receptors was
reevaluated in the surgical specimen. Nuclear expression of
β-catenin was detected (Fig. 3C) and
estrogen-receptors immunostaining were negative (Fig. 3D).
Discussion
The relation between the mutation of the APC
gene and the consequent phenotype is important to establish an
appropriate surveillance in a Family Risk Consulting, with a
regular program of colonoscopy and upper gastrointestinal endoscopy
to attempt evaluation of other FAP related lesions and also to
prevent the development of life threatening conditions such as
other neoplasms and the development of fibromatosis after surgical
procedures.
We describe a peculiar case of bilateral breast
fibromatosis after the placement of breast silicone prosthetics in
a woman diagnosed with classic FAP (≥100 tubular adenomas in the
colorectal specimen) with a nonsense mutation (c.935C>A) at
codon 935 in exon 15 of APC gene. She also had antecedents
of thyroidectomy for a pT1 cribriform-morular papillary thyroid
carcinoma.
Thyroid carcinoma was identified after the diagnosis
of germinal mutation, at the age of 16 years old. The search of
extra-colonic manifestations allowed the identification of a single
and rather small CMV-PTC, at an early age. CMV-PTC is a rare
variant of thyroid carcinoma (0.1–0.2% of all papillary carcinomas)
almost always associated with FAP (15). It affects female patients at 35 years'
age or younger, being exceptional in pediatric patients, and
sometimes preceding the colon manifestations (15). Characteristically presents distinctive
morphological features with a cribriform and morular architecture,
lack of nuclear atypia, mitosis or necrosis, and strong nuclear and
cytoplasmic expression for β-catenin, that allows the diagnosis,
and harbors germline mutations in the APC gene (exon 15), in
more than 85% of patients. The majority of these germline mutations
are found before codon 1220 and outside the mutation cluster region
(codons 1286 to 1513) (16) and the
overall prognosis of this variant is similar to that of classical
variant of PTC.
The surge of bilateral breast fibromatosis was not
anticipated, as this patient's mutation, located in exon 15
(c.935C>A), is seldom associated to fibromatosis; although
recent studies demonstrated that fibromatosis can develop
irrespective of the APC gene mutations site (1). In a genetic context of FAP, the surgical
trauma of the colocation of breast implants, the continuous trauma
of the prosthetics, seems to be concurrent factors for the
development of bilateral fibromatosis, with an aggressive course
and a rapid relapse.
All fibromatosis tumors, either superficial
(fascial) or deep (muscle-aponeurotic), have a morphological
similar pattern, corresponding to a proliferation of relatively
monomorphic population of fibroblasts and myofibroblasts, almost
without mitotic figures, arranged in long fascicles with dense
collagen, with nuclear expression of β-catenin in about 67–80% of
cases (4). Cytokeratin's expression,
CD34 and S100 protein are negative (5). Some of the cases are positive for
estrogen-receptors and may express smooth muscle actin and calponin
(4). As breast fibromatosis is very
rare (5,8) the histological differential diagnosis is
challenging (7), mainly in core
biopsies.
The differential diagnosis includes nodular
fasciitis, neurofibroma, fibroadenoma, phyllodes tumor and
low-grade fibromatosis-like spindle cell metaplastic carcinoma of
breast (5). MRI is particularly
important in the evaluation of margins and the eventual chest wall
involvement, helping to plan surgery, but it does not assists in
the differential diagnosis (5). MRI
can also be used for assessing the response to medical treatments
(5).
The clinical behavior may be indolent or progressive
and there is no histological discriminator to predict the clinical
behavior of fibromatosis.
In FAP patients' colon reducing risk surgery is
effective being this patient controlled and well at present, but
regarding fibromatosis, the best therapeutic approach is
controversial in all locations (4,17–19).
Surgery, radiotherapy, anti-inflammatory drugs,
hormone therapy, doxorubicin (DOX) or tyrosine kinase inhibitors
(TKI) and a wait and watch approach have been used.
Previously, radical surgical resection with negative
margins and radiotherapy were the first-line treatments (4,17,19). According to some authors, the clinical
indolent or progressive behavior of fibromatosis could require
different surgical approaches and different importance on negative
margins (4,17). Surgery may be a problematic solution,
because the growth factors released could lead to the activation of
β-catenin, acting as a tumor enhancer factor for fibromatosis
(17).
Radiotherapy has been used in extra-abdominal
fibromatosis, as an adjuvant therapy after surgery or as the
primary treatment in cases of non-resectable fibromatosis, with
controversial results (4,17).
Systemic treatment regimens became more frequent in
the last years (4,17). The most commonly used are nonsteroidal
anti-inflammatory drugs like sulindac and indomethacin (4,17).
Antiestrogen, most often tamoxifen, and anthracycline-containing
regimes appear to be associated with higher response rates than TKI
(17,19). Some studies suggest that tamoxifen
combination with anti-inflammatory drugs is more effective than
tamoxifen alone (17). Regarding TKI,
imatinib and sorafenib have been tested, with better responses for
sorafenib (4,17). Other drugs, like DOX and vinca
alkaloids are reserved for rapidly progressive disease (4,17).
A treatment algorithm has been suggested by Bonvalot
et al (17) and by the
Consensus on sporadic desmoid-type fibromatosis, according with the
indolent or progressive behavior of the fibromatosis (20).
In the present case, a wait and watch approach was
initially used and the contraceptive subdermal implant was removed.
After 1 month, the tumor continued to grow according to MRI
evaluation. The estrogen-receptors immunostaining was negative, but
a relative recent review (21) found
that approximately half of the patients respond to tamoxifen,
irrespective of the estrogen receptor status. Thus, tamoxifen
treatment was initiated, after carefully weighing this therapy with
the patient.
As the tumor continued to progress (Fig. 1C), one year after the diagnosis,
another treatment strategy was advised and surgical excision with a
thoracic wall reconstruction was performed. The relapsing tumor on
right thoracic wall, one year after, was again approached by
surgical excision. Currently the patient remains in surveillance 24
months after this surgery, without evidence of recurrence.
In conclusion, this is the first case reported in
the literature of a patient with classic FAP and with antecedents
of a cribriform-morular papillary thyroid carcinoma that developed
an aggressive breast bilateral fibromatosis after breast silicone
prosthetics. The knowledge of the relationship between the mutation
of the APC gene and the consequent phenotype is important to
establish appropriate surveillance protocols in FAP patients and to
prevent the development of life threatening conditions.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SS made substantial contributions to conception and
design, acquisition of data, analysis and interpretation of data,
was involved in drafting the manuscript and agree to be accountable
for all aspects of the work in ensuring that questions related to
the accuracy or integrity of any part of the work are appropriately
investigated and resolved. RA and FC provided clinical data and
contribute to the general discussion. PL contributed with familial
and genetic data and to the general discussion. AC analyzed the
data and participated in the discussion. AF analyzed the data,
participated in the discussion and did the paper's review. SA made
substantial contributions to conception and design, acquisition of
data, analysis and interpretation of data, was involved in drafting
the manuscript and in revising it critically, gave final approval
of the version to be published, agree to be accountable for all
aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved. Also, she got the funding for
publication and supervised the research group. All authors approved
the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Consent for publication
Informed consent was obtained from the patient in
this clinical case to authorize its publication.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
FAP
|
familial adenomatous polyposis
|
|
APC
|
adenomatous polyposis coli
|
|
CMV-PTC
|
cribriform-morular morphologic variant
of papillary thyroid carcinoma
|
|
MRI
|
magnetic resonance imaging
|
|
DGGE
|
denaturing gradient gel
electrophoresis
|
|
PTT
|
protein truncation test
|
|
DOX
|
doxorubicin
|
|
TKI
|
tyrosine kinase inhibitors
|
References
|
1
|
Calvert GT, Monument MJ, Burt RW, Jones KB
and Randall RL: Extra-abdominal desmoid tumors associated with
familial adenomatous polyposis. Sarcoma. 2012:7265372012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Plawski A, Banasiewicz T, Borun P,
Kubaszewski L, Krokowicz P, Skrzypczak-Zielinska M and Lubinski J:
Familial adenomatous polyposis of the colon. Hered Cancer Clin
Pract. 11:152013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Colaco RJ, Menasce LP, Ranson M, Sobrinho
Simoes M, Cameselle Teijeiro J, Vinjamuri S and Yap BK: A clinical
case report of cribriform-morular variant of papillary thyroid
carcinoma with neuroendocrine differentiation and aggressive
behaviour in a patient with familial adenomatous polyposis coli.
Thyroid Sci. 4:1–3. 2009.
|
|
4
|
Escobar C, Munker R, Thomas JO, Li BD and
Burton GV: Update on desmoid tumors. Ann Oncol. 23:562–569. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ebrahim L, Parry J and Taylor DB:
Fibromatosis of the breast: A pictorial review of the imaging and
histopathology findings. Clin Radiol. 69:1077–1083. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Balzer BL and Weiss SW: Do biomaterials
cause implant-associated mesenchymal tumors of the breast? Analysis
of 8 new cases and review of the literature. Hum Pathol.
40:1564–1570. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ünal B, Erdoğan G and Karaveli FŞ: Step by
step approach to rare breast lesions containing spindle cells.
Springerplus. 4:6782015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mátrai Z, Tóth L, Gulyás G, Szabó E,
Szentirmay Z and Kásler M: A desmoid tumor associated with a
ruptured silicone breast implant. Plast Reconstr Surg. 127:1e–4e.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jeong WS, Oh TS, Sim HB and Eom JS:
Desmoid tumor following augmentation mammoplasty with silicone
implants. Arch Plast Surg. 40:470–472. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Amourak S, Alaoui FF, Jayi S, Chaara H and
Melhouf MA: Desmoid fibromatosis of the breast: A case report on
and a review of the literature. Pan Afr Med J. 21:882015.(In
French). PubMed/NCBI
|
|
11
|
Abraham SC, Reynolds C, Lee JH, Montgomery
EA, Baisden BL, Krasinskas AM and Wu TT: Fibromatosis of the breast
and mutations involving the APC/beta-catenin pathway. Hum Pathol.
33:39–46. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Haggitt RC and Booth JL: Bilateral
fibromatosis of the breast in Gardner syndrome. Cancer. 25:161–166.
1970. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Filipe B, Baltazar C, Albuquerque C,
Fragoso S, Lage P, Vitoriano I, Mão de Ferro S, Claro I, Rodrigues
P, Fidalgo P, et al: APC or MUTYH mutations account for the
majority of clinically well-characterized families with FAP and
AFAP phenotype and patients with more than 30 adenomas. Clin Genet.
76:242–255. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Albuquerque C, Cravo M, Cruz C, Lage P,
Chaves P, Fidalgo P, Suspiro A and Nobre Leitão C: Genetic
characterisation of patients with multiple colonic polyps. J Med
Genet. 39:297–302. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Perea Del Pozo E, Ramirez Plaza C, Padillo
Ruiz J and Martos Martínez JM: Cribiform variant of papillary
thyroid cancer and familial adenomatous polyposis. Int J Surg Case
Rep. 16:192–194. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cao X, Eu KW, Seow-Choen F, Zao Y and
Cheah PY: APC mutation and phenotypic spectrum of Singapore
familial adenomatous polyposis patients. Eur J Hum Genet. 8:42–48.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bonvalot S, Desai A, Coppola S, Le Péchoux
C, Terrier P, Dômont J and Le Cesne A: The treatment of desmoid
tumors: A stepwise clinical approach. Ann Oncol. 23(Suppl 10):
x158–x166. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Roussin S, Mazouni C, Rimareix F, Honoré
C, Terrier P, Mir O, Dômont J, Le Péchoux C, Le Cesne A and
Bonvalot S: Toward a new strategy in desmoid of the breast? Eur J
Surg Oncol. 41:571–576. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bonvalot S, Ternès N, Fiore M, Bitsakou G,
Colombo C, Honoré C, Marrari A, Le Cesne A, Perrone F, Dunant A and
Gronchi A: Spontaneous regression of primary abdominal wall desmoid
tumors: More common than previously thought. Ann Surg Oncol.
20:4096–4102. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kasper B, Baumgarten C, Bonvalot S, Haas
R, Haller F, Hohenberger P, Moreau G, van der Graaf WT and Gronchi
A; Desmoid Working Group: Management of sporadic desmoid-type
fibromatosis: A European consensus approach based on patients' and
professionals' expertise-a sarcoma patients EuroNet and European
Organisation for research and treatment of cancer/soft tissue and
bone sarcoma group initiative. Eur J Cancer. 51:127–136. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bocale D, Rotelli MT, Cavallini A and
Altomare DF: Anti-oestrogen therapy in the treatment of desmoid
tumours: A systematic review. Colorectal Dis. 13:e388–e395. 2011.
View Article : Google Scholar : PubMed/NCBI
|