Introduction
Adenoid cystic carcinoma (ACC) is a malignant
neoplasm of the epithelium, which occurs in the major and minor
salivary glands (1). In 1859,
Billroth used the term ‘cylindroma’ to describe the standard
histology of salivary gland tumors, however, this was replaced by
the term ‘ACC’ in 1953 (2,3).
ACC is a relatively rare tumor, accounting for
<1% of all head and neck malignancies and 7.5–10% of all
salivary gland neoplasms (3–6).
Laryngeal localization of ACC, which is most
frequently hypoglottic, is relatively rare, occurring in 0.07–0.25%
of all laryngeal tumors (5,7,8). ACC
tumors arise from submucosal minor salivary glands, in which
laryngotracheal mucosa is sparse (5,9). The
majority of the minor salivary glands are located in the subglottis
(60%), however, they are also identified in the supraglottis, false
vocal cords, aryepiglottic folds and caudal aspect of the
epiglottis (5,7,10). Tumors
of the minor salivary glands are usually malignant and ACC presents
the most common tumor type (5,7). These
tumors most frequently occur in the oral cavity, particularly in
the hard palate, however, tumors are less common in the nasal
cavity, paranasal sinuses, pharynx and larynx (5,11), due to
the distribution of minor salivary glands in these regions. ACC
most commonly occurs in patients aged between 50 and 60 years old
with no gender predilection (11).
Laryngeal ACC is characterized as a slowly-growing tumor with
symptoms that are dependent on the location of the tumor. For
example, certain patients present with dyspnea, while patients with
lesions that involve the true vocal cords present with hoarseness
and dysphagia that is associated with ear pain (12). Distant metastasis is observed in
35–50% of ACC cases and most commonly occurs in the lungs (2). Diagnostic modalities include physical
examination with fiberoscopy and computed tomography of the neck
and chest in order to identify lung metastases, which are extremely
common (13). At present, surgery
followed by radiotherapy is the standard treatment for ACC
(10). Approximately 50% of ACC
patients experience recurrence within 5 years of diagnosis,
however, ACC exhibits a fairly good prognosis, with a 5-year
overall survival rate of 70% (14).
To the best of our knowledge, in the last 15 years a
total of 81 cases of ACC of the larynx have been reported in the
literature (Table I). In this study,
a case of laryngeal ACC in a 70-year-old man, which was a candidate
for total laryngectomy with bilateral neck dissection and adjuvant
radiotherapy, is presented.
 | Table I.Previous case reports of adenoid
cystic carcinoma arising in the larynx reported in the English
language literature over the last 15 years. |
Table I.
Previous case reports of adenoid
cystic carcinoma arising in the larynx reported in the English
language literature over the last 15 years.
| First author/s,
year | Case(s), n | Primary tumor
localization | Recurrence sites
(local-regional/ distant metastases) | Survival | Ref. |
|---|
| Javadi et
al, 2002 | 1 | Subglottis | ND | ND | (1) |
| Saraydaroglu et
al, 2011 | 1 |
Supraglottis-glottis | ND | ND | (5) |
| Ganly et al,
2006 | 12 | Larynx | ND | ND | (7) |
| Lee et al,
2003 | 1 | Larynx | ND | ND | (15) |
| Del Negro et
al, 2007 | 1 | Subglottis | ND | ND | (16) |
| Amit et al,
2014 | 6 | Larynx | ND | NED - Follow-up
period 3–288 months (median, 64 months) | (17) |
| Qian et al,
2014 | 1 | Supraglottis | Regional recurrence
[supraglottis, glottis and subglottis (1 cm)] | NED-42 months
follow-up | (18) |
| Misiukiewicz et
al, 2013 | 1 | Transglottic | Distant metastases
(pulmonary metastases at 54 months) | Alive, 112 months
follow-up | (19) |
|
| 1 | Glottis | None | NED - 60 months
follow-up |
|
| Testa et al,
2013 | 1 |
Glottis-subglottis | ND | NED - 36 months
follow-up | (20) |
| Murray et
al, 2010 | 1 | Larynx | Lung metastasis and
splenic lesion | ND | (21) |
| Zvrko and
Golubović, 2009 | 1 | Subglottis | ND | NED - 6 months
follow-up | (22) |
| Wang et al,
2009 | 1 | Subglottis | ND | NED - 6 months
follow-up | (23) |
| Zeng et al,
2009 | 10 |
Supraglottis/Subglottis | ND | ND | (24) |
| Maukarbel et
al, 2008 | 15 | Supraglottis (2;
13.3%), glottis (1; 6.6%), subglottis (9; 60%) and transglottis (3;
20%) | Distant metastases
(7), local/distant (2), local residual (1), none (3)
and regional (2) | 6 patients alive (1
NED), 9 patients succumbed (7 from their disease. 6.9 years
follow-up (range, 1.3–22.3 years) | (25) |
| Aydin et al,
2008 | 1 | Subglottis | None | NED - 6 years | (26) |
| Messaoudi et
al, 2007 | 1 | Subglottis | None | NED - 6 months | (27) |
| Khan et al,
2006 | 1 | Subglottis | ND | ND | (28) |
| Pino Rivero et
al, 2006 | 1 | Larynx | Pulmonary
metastases | NED - 1 year | (29) |
| Natarajan et
al, 2004 | 1 | Larynx | ND | ND | (30) |
| Adachi et
al, 2003 | 1 | Larynx | Choroidal/optic
disc metastasis | ND | (31) |
| Dexemple et
al, 2003 | 2 | Larynx | ND | ND | (32) |
| Mahlstedt et
al, 2002 | 6 | Larynx | ND | ND | (33) |
| Issing et
al, 2002 | 3 | Larynx | ND | ND | (34) |
| Altaf, 2001 | 1 | Larynx | ND | ND | (35) |
| Szmeja et
al, 2001 | 1 | Larynx | ND | ND | (36) |
| Lucioni et
al, 2015 | 8 | Supraglottis
(2), transglottis (1) and subglottis (5) | Regional metastases
(2) | NED - 41 months
median follow-up (range, 14–301 months) | (37) |
Case report
In May 2012, a 70-year-old man presented to the
Department of Otolaryngology-Head and Neck Surgery at ‘Federico II’
University (Naples, Italy) with ear pain, dysphonia, a 1-year
history of dysphagia and a 1-month history of dyspnea. The patient
was a former smoker (80 cigarettes/day for 50 years) and had
previously been diagnosed with diabetes mellitus and chronic renal
failure, which had been managed with dialysis for 10 years.
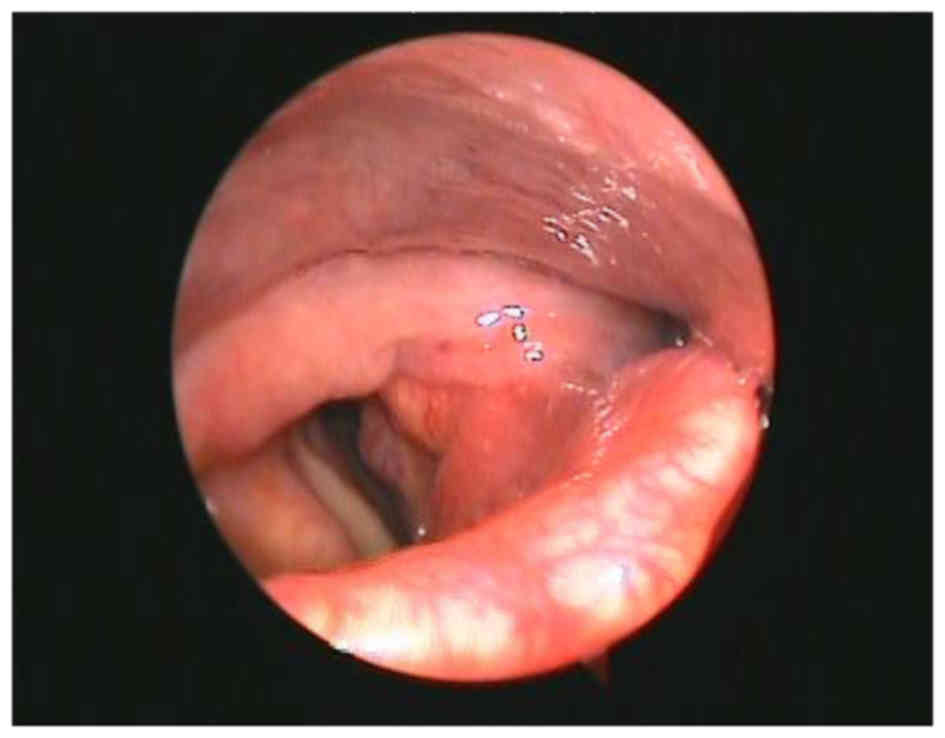
Laryngoscopy revealed a bulging mass in the left
true vocal cord and left ventricle, which extended to the
subglottic area with lack of mobility of the left larynx (Fig. 1). In the neck, left lymph nodes were
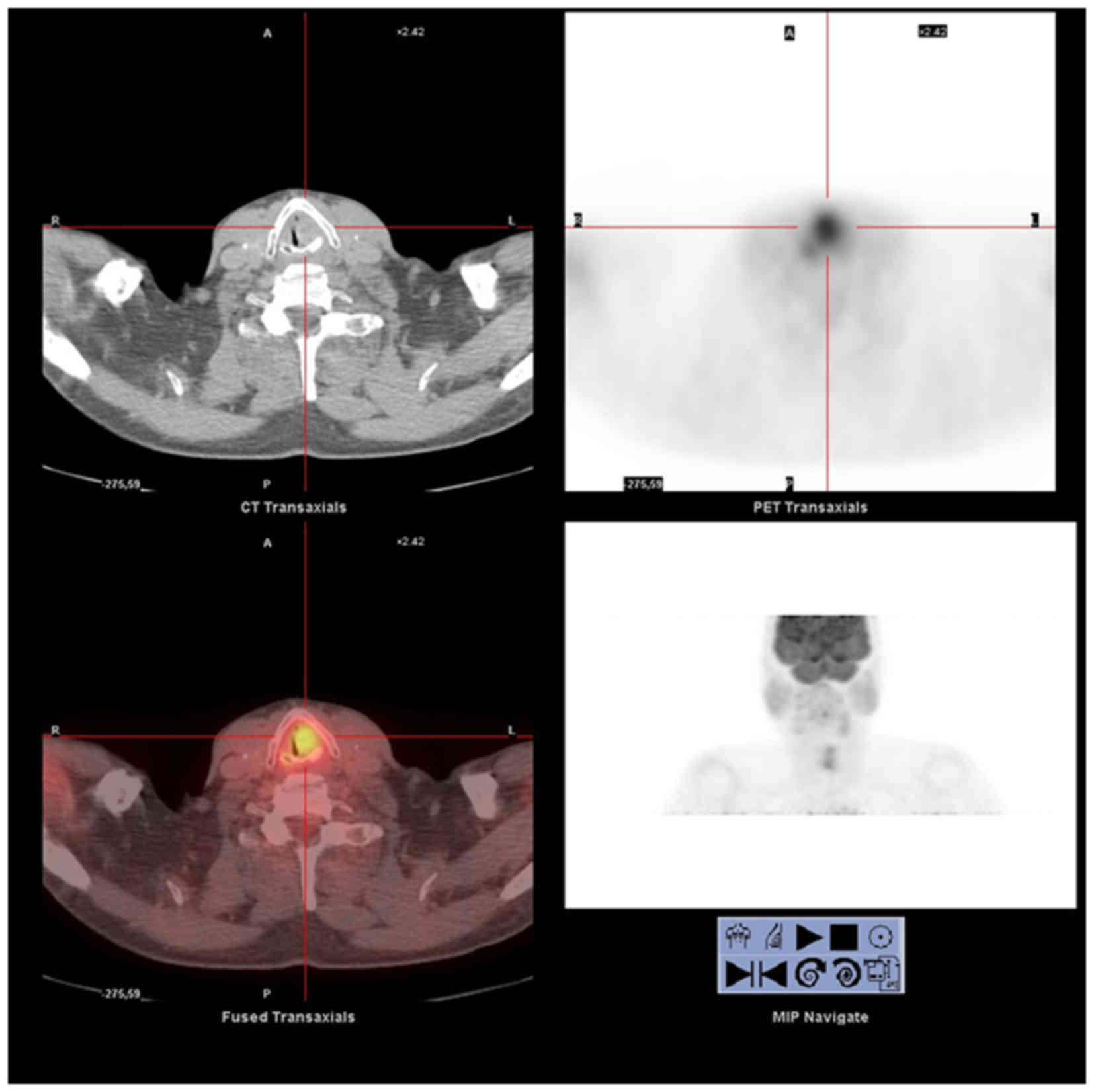
palpable (level III). Total body positron emission
tomography-computed tomography (PET-CT) with contrast medium
revealed hyperaccumulation of tracer in the left laryngeal region
(standardized uptake volume, 7.9) (Fig.
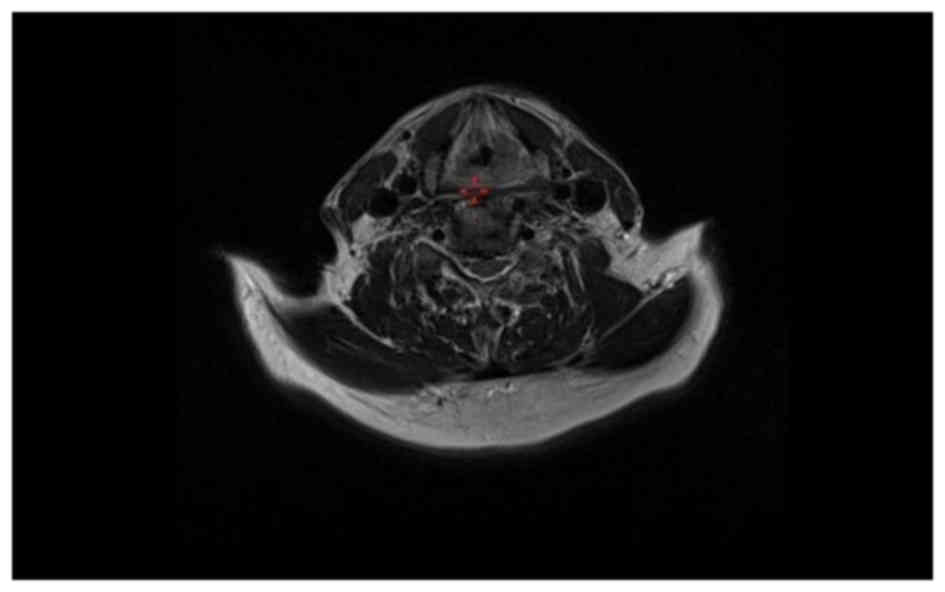
2). Magnetic resonance imaging (MRI) of the neck with contrast
medium revealed asymmetric reduction of the laryngeal glottic plane
and the presence of a solid, inhomogeneous lesion with evidence of
increased perfusion predominantly in the left true vocal cord
(28×37 mm).
This lesion laterally destroyed the paraglottic
space, upward interesting the ipsilateral false vocal cord and
anteriorly reaching the anterior commissure; posteriorly and
inferiorly it was associated with mixed structural alteration
mainly thickening of the left arytenoid cartilage, especially in
his vocal process, and the posterosuperior and lateral portion of
the cricoid cartilage, which exhibited moderate and uniform
contrast enhancement suggesting infiltrative growth into nearby
structures (Fig. 3). In addition,
neck MRI revealed an enlarged left cervical lymph node, measuring
1.8 cm in diameter. Clinical staging was T3N1M0 (stage III,
according to the Union for International Cancer Control/American
Joint Committee on Cancer staging system) (38).
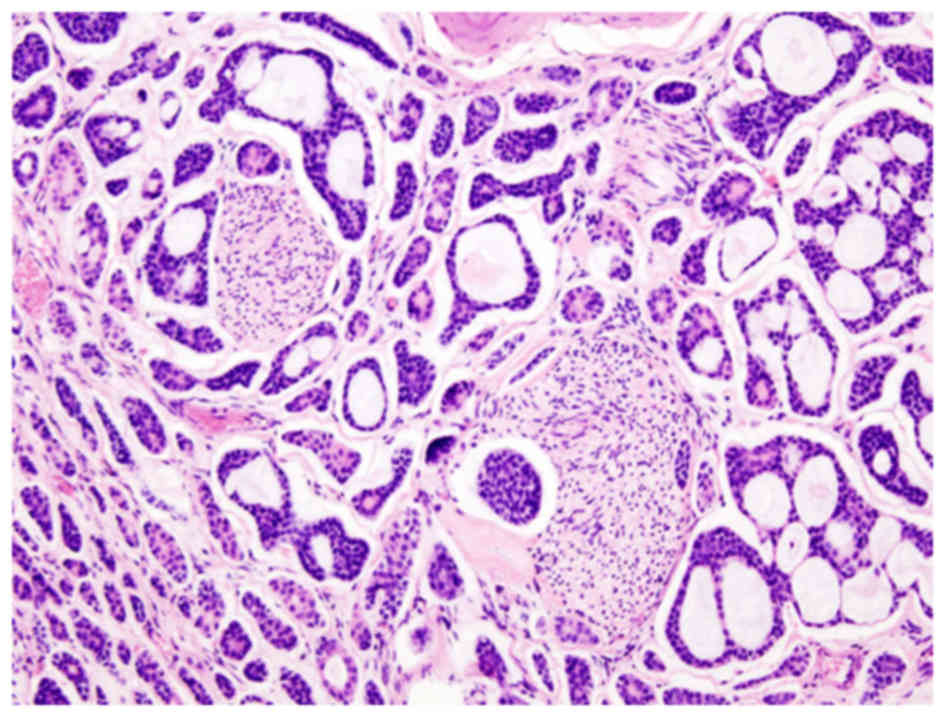
Biopsy of the tumor mass by direct microlaryngoscopy
in suspension revealed a cellular neoplasm with prominent
cribriform architecture, which was composed of small, bland
hyperchromatic cells with a high nuclear-to-cytoplasmic ratio. The
neoplastic cells surrounding the pseudoglandular spaces were filled
with basement membrane-like material and mucin (Fig. 4).
Subsequently, the patient underwent total
laryngectomy with bilateral selective neck dissection (levels
II–IV, left side; levels II–III, right side).
Tissue sections (3–5 µm) from each specimen were
mounted on glass slides and dried overnight at 37°C. All sections
were deparaffinized in xylene, rehydrated through a graded alcohol
series and washed in phosphate-buffered saline. Tissue sections
were processed using the standard
streptavidin-biotin-immunoperoxidase method (Dako LSAB2 Universal
Kit; Dako, Carpinteria, CA, USA). Rabbit polyclonal anti-human
c-kit antibody (CD117; catalog no. 34–8800; Dako) at 1:50 dilution
was used according to the manufacturer's protocols. Hematoxylin and
eosin (Sigma-Aldrich; Merck KGaA, Damrstadt, Germany) stain was
used as the final chromogen. Histological examination identified
the presence of ACC, which exhibited focal solid areas and
infiltration of the cartilage and fibroadipose perilaryngeal
tissues with perineural invasion. All dissected neck lymph nodes
were free of metastases. Immunohistochemical analysis of ACC cells
revealed positivity for the c-kit protein. Subsequently, the tumor
was pathologically staged as ACC T3N0M0 (stage III).
The patient was administered adjuvant radiotherapy
(66 Gy) for 6 weeks according to recent guidelines (39). Follow-up examinations were performed
every 6 months and follow-up 2 years after surgery revealed no
evidence of locoregional recurrence or distant metastases.
Discussion
ACC of the larynx most commonly occurs in patients
aged between 40 and 60 years-old (5,11,15). However, in the present case, ACC of
the larynx was diagnosed in a 70-year-old patient. In the last 15
years, a total of 81 laryngeal ACCs have been reported and
well-documented in the English literature (Table I). ACC is the predominant histological
type among malignancies of the minor salivary glands, with a
frequency of 10–20%, representing only 2–4% of all head and neck
malignancies. ACC of the larynx is incredibly rare (0.07–0.25% of
all laryngeal tumours, 1% of all ACC) as there are few salivary
glands in the mucosa of laryngeal-tracheal tract (5). These tumors are predominantly subglottic
(64%), such as in the present case. Moreover, their prevalence is
25% for the supra-glottic region, 5% for the glottic region and 6%
for the trans-glottic area. This pattern of distribution in the
anatomical laryngeal subsites is due to their origin from
submucosal glands, which are more frequently found in the
subglottic region of the larynx (1,5,7,1). These tumors grow slowly with
perineural diffusion (37). So the
evolution prognosis of this disease is caused by lung, bone and
brain metastases or by local recurrence (20,37).
ACC of the larynx develops in a similar manner to
ACC of other head and neck sites. It is considered a slowly growing
but highly invasive cancer with a high recurrence rate.
In the laryngeal region, symptoms depend on the
tumor location. Patients with subglottic cancer show dyspnea,
whereas common symptoms of glottis implications are dyspnea and a
hoarse voice. Subglottic tumors are rare and associated with
stridor and airway obstruction (12).
In the present clinical case, an initial glottic and supraglottic
lesion infiltrating the left true vocal cord and left ventricle
caused hoarseness (due to vocal cord compromise) and dysphagia
associated with ear pain for 1 year (10), and subsequently, the major extension
of the lesion to the subglottic region resulted in dyspnea (due to
airway obstruction) over the last month.
In the present case, physical and radiological
examinations identified an enlarged left cervical lymph node, 1.8
cm in diameter with no evidence of distant metastasis. Previously
it has been reported that nodal metastasis is a common cause of
treatment failure in ACC patients (16), however, metastasis to the cervical
lymph nodes is rare in ACC, occurring in 10–20% of patients with
head and neck ACC (38). Notably, the
metastasis rates of ACC located in the base of the tongue (19.2%),
mobile tongue (17.6%) and mouth floor (15.3%) are higher than that
of ACC of the larynx (15). In
addition, clinical investigations have shown that the incidence of
ACC with distant metastasis ranges from 35 to 50%, and leads to
5-year survival rates ranging from 12–17% following surgery
(12). The lungs are the most common
site of distant metastasis from ACC (15).
We recommend that neck dissection is performed in
all ACC patients with pre-operative evidence of nodal metastases,
as indicated by physical examination and imaging studies including
CT, MRI and/or PET-CT, since occult cervical metastases of head and
neck ACC occurs in 10–20% of cases (38).
The prognostic factors of ACC are dependent on tumor
site, tumor stage and microscopic tumor pattern. Other prognostic
factors are an age >60 years, a solid histological subtype, an
advanced clinical stage and the presence of perineural invasion
(5,40).
In the patient of the present case, the ACC tumor
was mainly localized to the glottis and supraglottic area, causing
hoarseness and dysphagia; however, major extension of the lesion to
the subglottic region resulted in dyspnea leading to a late
diagnosis. In the larynx, tumor occurrence in the minor salivary
glands is rare, accounting for <1% laryngeal tumors (5). The tumors arise from submucosal minor
salivary glands, which exhibit a distinct anatomical distribution
in the larynx. The majority of minor salivary glands are
concentrated in the subglottis, however, they may also be
identified in the supraglottis in the false vocal cords,
aryepiglottic folds and caudal aspect of the epiglottis (5). The anatomical site in which laryngeal
submucosal minor salivary glands are located explains the evolution
of the symptoms in the present clinical case.
The patient in the present case was initially
diagnosed with clinical stage III (cT3N1M0) disease, as tumor
extension to the vocal cords with emilaryngeal lack of mobility
(T3) and a metastatic omolateral lymph node (N1) were observed with
no evidence of distant metastases (M0) (5). Tumor staging was postoperatively
confirmed as T3N0M0 since all dissected neck lymph nodes were free
of metastases.
According to the World Health Organization
Classification of Tumors (41), ACC
may be divided into three microscopic grades: Tubular
(well-differentiated/grade I), which exhibits the best prognosis;
cribriform (moderately-differentiated/grade II), which is the most
common; and solid (poorly-differentiated/grade III), which is the
least common with the worst prognosis (5,16,17). ACC tumors often exhibit a mixture of
the three histological growth patterns and thus, tumors are
classified according to the predominant pattern (42). The tumor in the present case exhibited
a classic cribriform pattern and thus was defined as low-grade
(grade II).
Generally, neoplastic ACC cells exhibit
myoepithelial and ductal differentiation, with positivity for p63,
S100 protein, smooth muscle actin and cytokeratins (43). Typically, the most peripheral cells of
the tumor nests and glands are arranged in a cribriform pattern and
exhibit myoepithelial differentiation that is accompanied by the
abundant production of extracellular matrix and basement membrane
components, such as laminin (43).
Loss of laminin or reduced expression may occur during
transformation to a more aggressive malignancy (3,44). In the
present case, immunochemistry revealed positivity for c-kit
protein, a class III transmembrane receptor tyrosine kinase. C-kit
is a proto-oncogene encoded by a gene located on the human
chromosome segment 4q11, which leads to activation of specific
intracellular signal transduction cascades that contribute to the
cellular growth and differentiation that subsequently confers a
worse prognosis (11). Thus, further
investigation is required to characterize c-kit functional pathways
in salivary gland tumors and to evaluate potential therapeutic
effects of small molecule inhibitors of c-kit, such as imatinib
mesylate (42). In ACC, c-kit
expression is limited to the inner epithelial cells, whereas
epidermal growth factor receptor (EGFR) is typically expressed in
myoepithelial cells. EGFR, which facilitates carcinogenesis in
humans via the blockade of apoptosis and promotion of angiogenesis,
may be modified by anti-EGFR agents, including cetuximab and
erlotinib. In addition, recent studies have reported that
cytogenetically, ACC is characterized by the tumor-type specific
translocation, t(6;9) (q22-23;p23-24), which has been identified as
the sole anomaly in certain cases. This traslocation results in the
fusion of the MYB proto-oncogene and the transcription factor gene
nuclear factor I-B (NFIB), leading to the formation of the MYB-NFIB
fusion oncogene, which is highly overexpressed in ACC; thus, it may
be considered a useful biomarker for the disease (3,11).
At present, surgery followed by radiotherapy is the
standard treatment for ACC due to the risk of perineural and
hematogenous spread. According to the literature, surgical excision
of the lesion is recommended due to the relative radioresistance of
these tumors. Surgical excision should be performed with bilateral
selective neck dissection in cases where frozen sections reveal
negative lymph nodes (no tumoral infiltration) (pN0) and with
radical neck dissection in cases whereby frozen sections reveal
positive lymph nodes (pN+) (39).
The patient in the present case underwent total
laryngectomy associated with bilateral selective neck dissection
(levels II–IV, left side; levels II–III, right side). Furthermore,
frozen biopsy sections revealed that negative lymph nodes were
negative for metastasis (pN0) and thus adjuvant radiotherapy (66
Gy) was administered according to recent guidelines (39).
Postoperative radiation is recommended in certain
cases, as radiotherapy has been demonstrated to result in tumor
regression and symptomatic relief (16). However, the use of chemotherapy for
ACC remains controversial. Certain studies have demonstrated
positive patient responses to chemotherapy and thus, it is
recommended as palliative therapy in advanced cases (5,17).
However, currently, the identification of molecular
abnormalities underlying ACC, such as those of c-kit and EGFR, is
paramount for the development of specific targeted therapies.
Previous case reports of ACC in the larynx during
the last 14 years are listed in Table
I (1,5,7,1).
After 2 years of post-operative follow-up, performed
every 6 months, the patient in the current study remained free of
locoregional recurrence and/or distant metastases.
In conclusion, ACC is a relatively rare tumor
comprising <1% of all malignancies of the head and neck area.
ACC of the larynx occurs more commonly in middle-aged or older
patients, evolving slowly and with patients mainly developing
dyspnea. In addition, it is considered a highly invasive cancer
with a high recurrence rate and an incidence of distant metastasis
ranging from 35 to 50%, resulting in a low long-term survival rate
(12). It has been well-documented
that the most common site of distant metastasis from ACC is the
lung. In localized ACC, the gold-standard therapy is surgery
followed by adjuvant radiotherapy. Novel therapeutic frontiers will
focus on the identification of molecular abnormalities underlying
ACC, such as c-kit and EGFR, to develop specific targeted
therapies.
References
|
1
|
Javadi M, Bafrouee FM, Mohseni M and
Asghari A: Laryngeal adenoid cystic carcinoma in a child: A case
report. Ear Nose Throat J. 81:34–35. 2002.PubMed/NCBI
|
|
2
|
Soares EC, Filho Carreiro FP, Costa FW,
Vieira AC and Alves AP: Adenoid cystic carcinoma of the tongue:
Case report and literature review. Med Oral Pathol Oral Cir Bucal.
13:E475–E478. 2008.
|
|
3
|
Anupriya S, Mahesh P, Sharada P,
Swaminathan U, Nagamalini B and Hosthor SS: Immunohistochemical
analysis of laminin expression in adenoid cystic carcinoma. J Oral
Maxillofac Pathol. 18 Suppl 1:S26–S31. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sadeghi A, Tran LM, Mark R, Sidrys J and
Parker RG: Minor salivary gland tumors of the head and neck:
Treatment strategies and prognosis. Am J Clin Oncol. 16:3–8. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Saraydaroglu O, Coskun H and Kasap M:
Unique presentation of adenoid cystic carcinoma in postcricoid
region: A case report and review of the literature. Head Neck
Pathol. 5:413–415. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barrett AW and Speight PM: Perineural
invasion in adenoid cystic carcinoma of the salivary glands: A
valid prognostic indicator? Oral Oncol. 45:936–940. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ganly I, Patel SG, Coleman M, Ghossein R,
Carlson D and Shah JP: Malignant minor salivary gland tumors of the
larynx. Arch Otolaryngol Head Neck Surg. 132:767–770. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Serafini I, Lucioni M, Bittesini L, Dei
Tos AP and Della Libera D: Treatment of laryngeal adenoid cystic
carcinoma. Acta Otorhinolaryngol Ital. 11:13–24. 1991.(In Italian).
PubMed/NCBI
|
|
9
|
Bak-Pedersen K and Nielsen KO:
Subepithelial mucous glands in the adult human larynx. Studies on
number, distribution and density. Acta Otolaryngol. 102:341–352.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Karasmanis I, Goudakos JK, Vital I,
Zarampoukas T, Vital V and Markou K: Hybrid carcinoma of the
larynx: A case report (adenoid cystic and adenocarcinoma) and
review of the literature. Case Rep Otolaryngol.
2013:3854052013.PubMed/NCBI
|
|
11
|
Brill LB II, Kanner WA, Fehr A, Andrén Y,
Moskaluk CA, Löning T, Stenman G and Frierson HF Jr: Analysis of
MYB expression and MYB-NFIB gene fusions in adenoid cystic
carcinoma and other salivary neoplasms. Mod Pathol. 24:1169–1176.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li G, Chen J, Zhang S, Lin J, Kong F, Cai
F and Yang S: Adenoid cystic carcinoma of the larynx: A report of
two cases. Oncol Lett. 10:2303–2306. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Joshi VM, Wadhwa V and Mukherji SK:
Imaging in laryngeal cancers. Indian J Radiol Imaging. 22:209–226.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lin YC, Chen KC, Lin CH, Kuo KT, Ko JY and
Hong RL: Clinicopathological features of salivary and non-salivary
adenoid cystic carcinomas. Int J Oral Maxillofac Surg. 41:354–360.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee LA, Fang TJ, Li HY and Lee KF: Adenoid
cystic carcinoma of the supraglottis mimicking a laryngeal cyst.
Otolaryngol Head Neck Surg. 129:157–158. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Del Negro A, Ichihara E, Tincani AJ,
Altemani A and Martins AS: Laryngeal adenoid cystic carcinoma: Case
report. Sao Paulo Med J. 125:295–296. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Amit M, Na'ara S, Sharma K, Ramer N, Ramer
I, Agbetoba A, Glick J, Yang X, Lei D, Bjoerndal K, et al: Elective
neck dissection in patients with head and neck adenoid cystic
carcinoma: An international collaborative study. Ann Surg Oncol.
22:1353–1359. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qian X, Zhou H, Gu Y, Zhang Y and Gao X:
Supraglottic adenoid cystic carcinoma mimicking laryngeal
amyloidosis: A case report. Oncol Lett. 7:2154–2156. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Misiukiewicz KJ, Camille N, Tishler R,
Haddad R, Limaye S and Posner M: Organ preservation for adenoid
cystic carcinoma of the larynx. Oncologist. 18:579–583. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Testa D, Guerra G, Conzo G, Nunziata M,
D'Errico G, Siano M, Ilardi G, Vitale M, Riccitiello F and Motta G:
Glottic-Subglottic adenoid cystic carcinoma. A case report and
review of the literature. BMC Surgery. 13 Suppl 2:S482013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Murray BW, Lyons LC, Mancino AT and Huerta
S: A report of laryngeal adenocystic carcinoma metastatic to the
spleen and the role of splenectomy in the management of metastatic
disease: A case report. J Med Case Rep. 4:2072010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zvrko E and Golubović M: Laryngeal adenoid
cystic carcinoma. Acta Otorhinolaryngol Ital. 29:279–282.
2009.PubMed/NCBI
|
|
23
|
Wang HL, Xu L and Li FJ: Subglottic
adenoid cystic carcinoma mistaken for asthma. J Zhejiang Univ Sci
B. 10:707–710. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zeng Q, Tang PZ, Xu ZG, Qi YF, Wu XX and
Liu WS: Malignant minor salivary gland tumors of the larynx.
Zhongua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 44:40–43. 2009.(In
Chinese).
|
|
25
|
Maukarbel RV, Goldstein DP, O'Sullivan B,
Gullane PJ, Brown DH, Wang L and Irish JC: Adenoid cystic carcinoma
of the larynx: A 40-year experience. Head Neck. 30:919–924. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Aydin O, Ustündağ E, Işeri M and Erçin C:
Laringeal adenoid cystic carcinoma in an adolescent. Kulak Burun
Bogaz Ihtis Derg. 18:319–322. 2008.PubMed/NCBI
|
|
27
|
Messaouidi C, Larouk R, Baili S, Noui B,
Benchaoui M, Benkadri H and Belbekri F: Adenoid cystic carcinoma of
the larynx. A case report and review of the literature. Rev
Laryngol Otol Rhinol (Bord). 128:97–100. 2007.(In French).
PubMed/NCBI
|
|
28
|
Khan AR, Jan A, Nawaz G and Zaman N:
Adenoid cystic carcinoma of larynx. J Coll Physicians Surg Pak.
16:669–670. 2006.PubMed/NCBI
|
|
29
|
Pino Rivero V, Pantoja Hernández CG,
Palomino González A, Ramos Trinidad G, Romero Pardo G, García
Marcos M, Tamayo Pereda JM and Huelva Blasco A: Adenoid cystic
carcinoma of the larynx-hypopharynx. A case report and review of
the literature. An Otorrinolaringol Ibero Am. 33:339–345. 2006.(In
Spanish). PubMed/NCBI
|
|
30
|
Natarajan S, Greaves TS, Raza AS and Cobb
CJ: Fine-needle aspiration of an adenoid cystic carcinoma of the
larynx mimicking a thyroid mass. Diagn Cytopathol. 30:115–118.
2004. View
Article : Google Scholar : PubMed/NCBI
|
|
31
|
Adachi N, Tsuyama Y, Mizota A, Fujimoto N,
Suehiro S and Adachi-Usami E: Optic disc metastasis presenting as
an initial sign of recurrence of adenoid cystic carcinoma of the
larynx. Eye (Lond). 17:270–272. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dexemple P, Huth J, Rebufy M and Chabrol
A: Cystic adenoid carcinoma of the larynx: Two cases. Ann
Otolaryngol Chir Cervicofac. 120:244–248. 2003.(In French).
PubMed/NCBI
|
|
33
|
Mahlstedt K, Ussmüller J and Donath K:
Malignant sialogenic tumours of the larynx. J Laryngol Otol.
116:119–122. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Issing PR, Hemmanouil I, Wilkens L,
Karstens H and Lenarz T: Long term results in adenoidcystic
carcinoma. Laryngorhinootologie. 81:98–105. 2002.(In German).
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Altaf FJ: Histopathology of adenoid cystic
carcinoma of the larynx and adenocarcinoma hybrid. Saudi Med J.
22:920–923. 2001.PubMed/NCBI
|
|
36
|
Szmeja Z, Wierzbicka M, Szyfter W and
Woźniak A: A rare case of adenoid cystic carcinoma of the larynx.
Otolaryngol Pol. 55:203–206. 2001.(In Polish). PubMed/NCBI
|
|
37
|
Lucioni M, Bertolin A, Lionello M and
Rizzotto G: Terapia chirurgica nelle localizzazioni primitive
laringee e della giunzione laringotracheale. In: Il carcinoma
adenoido-cistico nel distretto cervico-facciale. Quaderni
monografici di aggiornamento A.O.O.I. - 2015. 195–206, (In
Italian).
|
|
38
|
Edge SB, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A III: Larynx AJCC Cancer Staging Manual. 7th
edition. Springer; New York: pp. 57–62. 2010
|
|
39
|
Pinto C, Maiello E, Moschetti I, Cinquini
M, Torri V, Pappagallo G and Gori S: Head Neck Tumors Guidelines.
In: AIOM Guidelines. Italian Association of Medical Oncology-AIOM.
2015.https://www.aiom.it5–Oct. 2015
|
|
40
|
Norberg-Spaak L, Dardick I and Ledin T:
Adenoid cystic carcinoma: use of cell proliferation, BCL-2
expression, histologic grade, and clinical stage as predictors of
clinical outcome. Head Neck. 22:489–97. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: World Health Organization Classification of
TumoursPathology and Genetics of Head and Neck Tumours. IARC Press;
Lyon: 2005
|
|
42
|
Kokemueller H, Eckardt A, Brachvogel P and
Hausamen JE: Adenoid cystic carcinoma of the head and neck - a 20
years experience. Int J Oral Maxillofac Surg. 33:25–31. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Salehinejad J, Mohtasham N, Bagherpour A,
Abbaszadeh-Bidokhty H and Ghazi A: Evaluation of c-kit protein
(CD117) expression in common salivary gland neoplasms. J Oral
Maxillofac Pathol. 18:177–182. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Mesolella M, Iengo M, Testa D, Di Lullo
AM, Salzano G and Salzano FA: Mucoepidermoid carcinoma of the base
of tongue. Acta Otorhinolaryngol Ital. 35:58–61. 2015.PubMed/NCBI
|