Introduction
Chronic obstructive pulmonary disease (COPD) is a
common and chronic respiratory disease. The main feature of COPD is
an incomplete irreversible airflow limitation, which is present in
the progressive development of the disease. Furthermore, COPD is
associated with an inflammatory reaction to harmful gases or
particles in the lungs. A previous study has revealed that the
incidence rate of COPD increases annually (1), and is expected to become one of the
world's top three causes of pathogenic-associated mortality by 2020
(2). The latest epidemiological
survey data revealed that the incidence rate of COPD among people
aged ≥40 in China has risen to 9.9% (3). This disease is a major threat to the
health of China's residents, and is also ranked the top disease
burden in China (4). A number of the
symptoms of COPD can be controlled through drug treatments;
however, there is no effective treatment available that can delay
or reverse the disease course (5).
Therefore, it is of vital importance for a novel effective
treatment to be developed.
Ulinastatin is a type of broad-spectrum protease
inhibitor (6). It has the ability to
inhibit the activity of glycohydrolase, lipid hydrolase and
protease through numerous pathways, as well as to restrain the
excessive release of inflammatory mediators, including TNF-α, IL-6
and IL-8, thus reducing the tissue damage (6). A number of studies have revealed that
ulinastatin may have the ability to prevent the development of
acute lung injury, by inhibiting the release of inflammatory
mediators (7–9); therefore, it is widely used in the
clinical treatment of acute lung injury (10). The occurrence and development of COPD
is closely associated with the inflammatory reaction, and the
symptoms of the majority of patients are unable to be alleviated
during the acute exacerbation of COPD. Ulinastatin has not been
previously used in a study on its effects in COPD; therefore, this
study used COPD rat models. The rats were given ulinastatin
treatment, to determine whether it has a protective effect on lung
injury in COPD.
The high mobility group box protein 1 (HMGB1) is
distributed in the nuclei and cytoplasm of numerous different types
of cells (11). In 1999, Wang et
al (12) revealed for the first
time, to the best of our knowledge, that HMGB1 is involved in
sepsis, and can be considered an important inflammatory mediator. A
number of previous studies revealed that ulinastatin could inhibit
the release of the inflammatory mediator HMGB1 (8,13,14), and, therefore, it could be associated
with COPD due to the high expression of HMGB1 in COPD (15). Toll-like receptor 4 (TLR4) is the
receptor for HMGB1; the pro-inflammatory role of HMGB1 is closely
associated with the TLR4 signal transduction pathway (16,17). When
the HMGB1/TLR4 signaling pathway is activated, HMGB1 binds to and
activates TLR4. The activated TLR4 then binds with the TLR4
receptor on myeloid differentiation factor 88 (MyD88) with the aid
of MD-2. MyD88 activates IRAK through its death domain, which then
activates tumor necrosis factor receptor-associated factor (TRAF6)
(18). TRAF6 can activate the nuclear
factor κB (NF-κB) signaling pathway, mediated by the downstream
associated factors. This causes the upregulation of lectin-type
oxidized LDL receptor 1 (LOX-1), mediating the inflammatory
response (18). A previous study
revealed that knocking out the TLR4 gene using small interfering
RNA could alleviate the inflammatory reaction induced by HMGB1
(19). In the present study, the
expression of key molecules associated with the HMGB1/TLR4
signaling pathway was evaluated in lung tissues of COPD rats, in
response to treatment with ulinastatin. The mechanism of action of
this drug was partially explored, in order to provide a theoretical
basis for the effect of ulinastatin in the clinical treatment of
COPD.
Materials and methods
Instruments and reagents
Lipopolysaccharide (LPS) was purchased from
Sigma-Aldrich (Merck KGaA, Darmstadt, Germany); mortar and grinding
rods were purchased from Jiangsu Shunhe Teaching Instrument Co.,
Ltd. (Jiangsu, China); ulinastatin was purchased from Guangdong
Techpool Bio-Pharma Co., Ltd. (Guangzhou, China); the RNA
extraction reagent TRIzol® was purchased from Invitrogen
(Thermo Fisher Scientific, Inc., Waltham, MA, USA), reverse
transcription kit (cat no. 6110A), the fluorescence RT-qPCR kit
(cat no. 639676) was purchased from Takara Biotechnology Co., Ltd.
(Dalian, China); all primers were synthesized by Shanghai Shenggong
Biological Engineering Technology Service, Ltd. (Shanghai, China);
chloroform, isopropanol, DEPC water, anhydrous ethanol, agarose
were purchased from Shanghai Shenggong Biological Engineering
Technology Service, Ltd.; Nanodrop2000 Protein Nucleic Acid
Analyzer was purchased from Thermo Fisher Scientific, Inc.; the
agarose gel electrophoresis imaging system was purchased from
Biometra GmbH (Göttingen, Germany); the ViiA™ 7 fluorescent RT-qPCR
machine was purchased from Applied Biosystems (Thermo Fisher
Scientific, Inc.); the flexiVent animal lung function instrument
was purchased from SCIREQ Inc. (Montreal, Canada); the RIPA cell
lysate (cat no. 20101ES60) and PMSF were purchased from Shanghai
Biyuntian Bio-technology Co., Ltd. (Shanghai, China); S-18KS
handheld microelectromotive tissue homogenizer was purchased from
Leptute Scientific Instruments (Beijing) Co., Ltd. (Beijing,
China); the total protein extraction kit was purchased from
BestBio, Co. (Shanghai, China); the Coomassie Brilliant Blue
protein determination kit was purchased from Shanghai Majorbio
Bio-pharm Technology Co., Ltd. (Shanghai, China); the
SDS-polyacrylamide, PBST solution, vertical electrophoresis
apparatus and GIS-2020D gel image analysis system were purchased
from Sigma-Aldrich; superSignal™ chemiluminescence substrate was
purchased from Thermo Fisher Scientific, Inc.; nitrocellulose
membrane, developer, fixer and film were purchased from China Lucky
Film Group Corporation (Baoding, Hebei, China); TLR4 (cat no.
ab13556), MyD88 (cat no. ab2064), TRAF-6 (cat no. ab33915), LOX-1
(cat no. ab60178), HMGB1 (cat no. ab18256), GAPDH (cat no. ab8245)
and Horseradish Peroxidase (HRP)-conjugated rabbit anti-mouse IgG
secondary antibody (ab6728) were purchased from Abcam (Cambridge,
MA, USA).
Preparation of the animal models
A total of 30 healthy, specific-pathogen-free, male
adult Sprague-Dawley® rats with a weight range of
180–200 g, 2–3 months of age were provided by the Guangdong Medical
Lab Animal Center (Foshan, China). The rats were housed at a
temperature of 20–25°C, a humidity of 50–65% a 12 h light/dark
cycle and given free access to food and water. The rats were fed
adaptively for one week, and randomly divided into three groups: A
control group, a model group and an experimental group, with each
group containing 10 rats. The method of establishing a COPD rat
model was as follows: At days 1 and 14, the rats were injected with
0.2 ml (200 µg) LPS solution (1 g/l) in the trachea through a
tracheal intubation under a 10% chloral hydrate anesthesia
(according to a 3 ml/Kg dose). Rats were then vertically rotated in
order to uniformly distribute the LPS in the lung. Following on,
the rats were placed in a homemade glass box in the morning of days
2–13 and days 15–28, where they continuously inhaled cigarette
smoke for 1 h/day. The rats in the control group were injected with
the same volume of saline through the trachea, but did not inhale
any cigarette smoke. The rats in the model group received
conventional treatments available for COPD, including expelling
phlegm, improving ventilation and antibiotic regimens, whereas rats
in the experimental group received 100,000 U/each time of
ulinastatin intravenously twice a day for seven days. Upon
completion, the lung function was detected using the small animal
lung function detector. Following this, the rats were sacrificed
after one week, and the lung tissues were removed and stored at
−80°C for subsequent experiments. The experimental program in this
study was examined and ethically approved by the Laboratory Animal
Ethics Committee.
RNA extraction and RT-qPCR
analysis
Total RNA in the lung tissue was extracted using a
TRIzol® kit. The lung tissue was ground up in a mortar
in a liquid nitrogen environment, then 1 ml TRIzol® was
added, followed by 200 µl chloroform to extract the layers. The
supernatant was transferred to another 1.5 ml EP tube, to which 1
ml isopropanol was added to precipitate the RNA. Using 1 ml of 70%
ethanol, the RNA was washed twice and then dissolved in DEPC water.
The RNA purity and content detected using a protein nucleic acid
detector (Coomassie Brilliant Blue protein determination kit).
Subsequently, 1% agarose gel electrophoresis was conducted to
identify the integrity of the RNA. Following this, 1 µg RNA was
used to synthesize cDNA via RT, using a Reverse Transcription kit
(fluorescence RT-qPCR kit), according to the manufacturer's
protocol.
In the reverse transcription reaction system a total
volume of 10 µl reaction mixture was used, including 1 µg total
RNA, 2 µl of 5× reverse transcriptase buffer, 0.5 µl oligo (dT) and
Random Primer Mix, 0.5 µl RT Enzyme Mix, 0.5 µl RNase inhibitor,
and supplemental ddH2O to bring the total volume up to
10 µl. The reaction conditions were as follows: 37°C for 15 min and
98°C for 5 min. The cDNA produced was stored at −20°C for later
use. The cDNA was then used as a template, the fluorescence RT-qPCR
reaction system was set as follows: 5 µl of 2× SYBR®
Green Mixture, 0.5 µl cDNA, 0.5 µl Primer F (10 µM), 0.5 µl Primer
R (10 µM) and 4 µl ddH2O. The reaction conditions were
set as follows: Pre-denaturing at 95°C for 10 min, 40 PCR cycles of
denaturing at 95°C for 15 sec, and annealing and extension at 60°C
for 60 sec. The reactions were processed in a ViiA™ 7 fluorescence
RT-qPCR instrument using the 2−∆∆Cq method (20). Overall, three parallel samples were
set as replicates for each experiment, with GAPDH as the internal
control gene. The sequences of the specific primers are depicted in
Table I.
 | Table I.Forward and reverse upstream primers
used in the present study. |
Table I.
Forward and reverse upstream primers
used in the present study.
| Protein | Upstream primers,
F | Upstream primers,
R |
|---|
| TLR4 |
CGCTTTCAGCTTTGCCTTCA |
CTCCAGAAGATGTGCCTCCC |
| MyD88 |
GCTGACTTGGAGCCTGATTCT |
ATGGGTGGGTGGGAGTAAA |
| TRAF-6 |
AGAGGAATCACTTGGCACGG | TCTGCGTTTCCATTT
TGGCG |
| LOX-1 |
CCTCACCTGGAAGCTAAACG |
CCTGCTCTTTGGATTTCTCG |
| HMGB1 |
ATGGGCAAAGGAGATCCTA |
ATTCATCATCATCATCTTCT |
| GAPDH |
CTGAGCACTCTCCCTCACAATTC |
GTGCAGCGAACTTTATTGATGGT |
Protein extraction and western blot
analysis
The obtained lung tissues were added to 400 µl RIPA
cell lysate containing Phenylmethanesulfonyl fluoride (PMSF) (PMSF:
RIPA=1:1,000) and homogenized in a homogenizer. After being placed
on ice for 30 min, the samples were centrifuged at 13,400 × g, and
centrifuge at 30°C for 4 min. The supernatant was collected to
obtain total lung tissue proteins. The proteins were quantified
with a BCA Protein Quantitation kit, and the total protein was
stored at −80°C for later use. After the 6–12% gradient SDS-PAGE
was prepared, 40 µg protein samples were loaded for electrophoretic
separation (100 V, 4 h). The protein gels were then placed into a
transferring electrophoresis chamber, and transferred at 100 V for
1.5 h with the added transferring buffer. The transferred membranes
were blocked for 2 h on a shaker at room temperature, in PBST
containing 5% skim-milk powder. After rinsing with PBST three
times, the membranes were incubated at 4°C on a shaker with the
primary antibody (1:500 dilution) solution. Following this, PBST
was used to rinse the membranes for 30 min; then diluted secondary
antibody (diluted 1:10,000) was added, which was diluted with PBST
containing 2.5% skimmed milk powder, and incubated at room
temperature in a shaker for 60 min. After using PBST to rinse
another three times, the nitrocellulose membranes were evenly
applied with the chemiluminescence reagent, and underwent exposure
in a darkroom. The films were developed in developing reagent for 2
min, rinsed, and then fixed in a fixing reagent for 2 min. The
films were further rinsed and hung to dry. The GIS-2020D Gel
Imaging Analysis System was used to analyze the optical density of
the protein bands of TLR4, MyD88, TRAF-6, LOX-1, HMGB1 and GAPDH.
The relative protein expression intensity was defined as the
optical density of the protein bands of TLR4, MyD88, TRAF-6, LOX-1
and HMGB1 compared with that of GAPDH.
Statistical analysis
SPSS 20.0 statistical software (IBM Corp., Armonk,
NY, USA) was used for statistical analysis. Measured data were
expressed as the mean ± standard deviation. The counted data were
expressed as the number of cases or percentage. The comparison
between the control group, model group and experimental group was
performed using the ANOVA. The comparison between the groups was
performed using the Student-Newman-Keuls test. Pearson correlation
analysis was used to analyze the correlation between the two sets
of data that matched the normal distribution. Spearman correlation
analysis was used to analyze the correlation between two sets of
data that did not follow the normal distribution. P<0.05 was
considered to indicate a statistically significant difference.
Results
Effect of ulinastatin on lung
function
As depicted in Table
II, the rat lung function indexes, FEV and forced vital
capacity (FVC) were significantly lower in the model group compared
with in the control group (P<0.05). In the experimental group,
FEV and FVC were significantly increased compared with in the model
group (P<0.05).
| Table II.Comparison of inspection results of
rat lung function among the groups. |
Table II.
Comparison of inspection results of
rat lung function among the groups.
| Group | FEV0.3
(ml) | FVC (ml) |
FEV0.3/FVC (%) | PEF
(ml.s−1) |
|---|
| Control group | 5.56±0.31 | 6.68±0.43 | 90.10±2.78 | 36.78±3.89 |
| Model group |
3.89±0.32a |
4.71±0.39a |
74.24±2.31a |
26.16±3.12a |
| Experimental
group |
5.07±0.41a,b |
6.11±0.45a,b |
83.26±2.56a,b |
32.48±3.26a,b |
mRNA and protein expression of TLR4,
MYD88, TRAF-6, LOX-1 and HMGB1 in lung tissues
The mRNA expression levels of TLR4, MyD88, TRAF-6,
LOX-1 and HMGB1 were evaluated in the lung tissues of rats from
each group. As depicted in the Table
III, the mRNA expression levels of all genes were significantly
increased in the model group compared with in the control group
(P<0.05). In rats from the experimental group with ulinastatin
treatment, the mRNA levels are significantly lower when compared
with in the model group (P<0.05); however, they are
significantly higher when compared with in the control group
(P<0.05).
| Table III.Expression of specific mRNAs in rat
lung tissues. |
Table III.
Expression of specific mRNAs in rat
lung tissues.
| Group | N | TLR4 | MyD88 | TRAF-6 | LOX-1 | HMGB1 |
|---|
| Control group | 10 | 1.00±0.20 | 1.00±0.18 | 1.00±0.21 | 1.00±0.22 | 1.00±0.19 |
| Model group | 10 |
2.78±0.31a |
2.67±0.28a |
2.34±0.41a |
1.89±0.29a |
3.31±0.35a |
| Experimental
group | 10 |
1.67±0.26a,b |
1.98±0.25a,b |
1.85±0.36a,b |
1.38±0.37a,b |
2.01±0.29a,b |
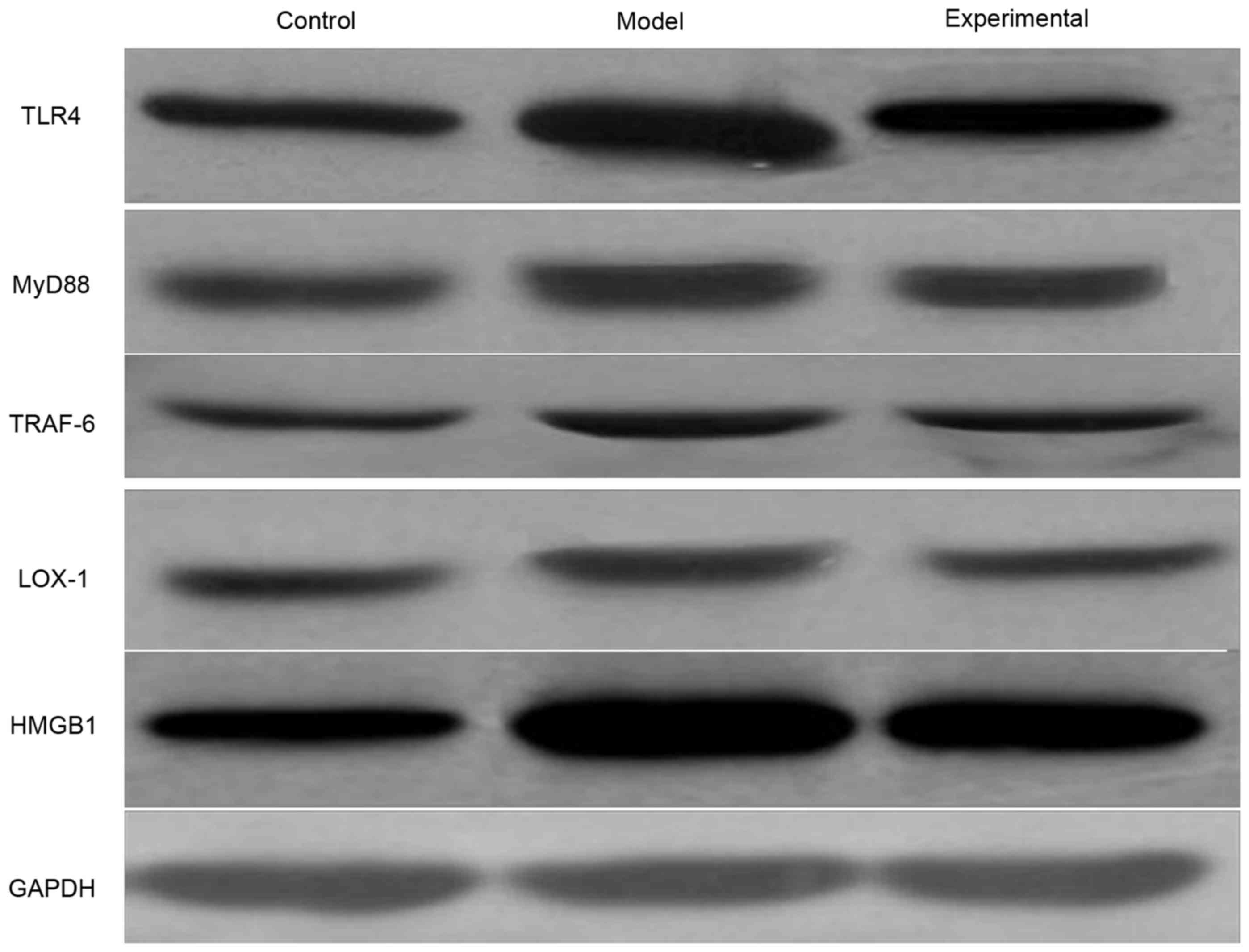
The western blot analyzes reveal a variation of
protein expression levels similar to that of the mRNA expression
levels (Fig. 1, Table IV). The protein expression levels of
TLR4, MyD88, TRAF-6, LOX-1 and HMGB1 were greater in the model
group compared with in the control group (P<0.05). In the lung
tissue of rats that received the ulinastatin treatment, the protein
expression levels were significantly lower (P<0.05) compared
with in the model rats, but remained higher in comparison with the
control rats (P<0.05).
| Table IV.Expression of certain proteins in the
rat lung tissues. |
Table IV.
Expression of certain proteins in the
rat lung tissues.
| Group | N | TLR4 | MyD88 | TRAF-6 | LOX-1 | HMGB1 |
|---|
| Control group | 10 | 0.82±0.11 | 0.56±0.12 | 0.58±0.14 | 0.51±0.09 | 0.79±0.14 |
| Model group | 10 |
1.21±0.12a |
0.73±0.11a |
0.76±0.13a |
0.95±0.10a |
1.36±0.15a |
| Experimental
group | 10 |
0.93±0.10a,b |
0.61±0.10a,b |
0.62±0.10a,b |
0.72±0.11a,b |
1.04±0.13a,b |
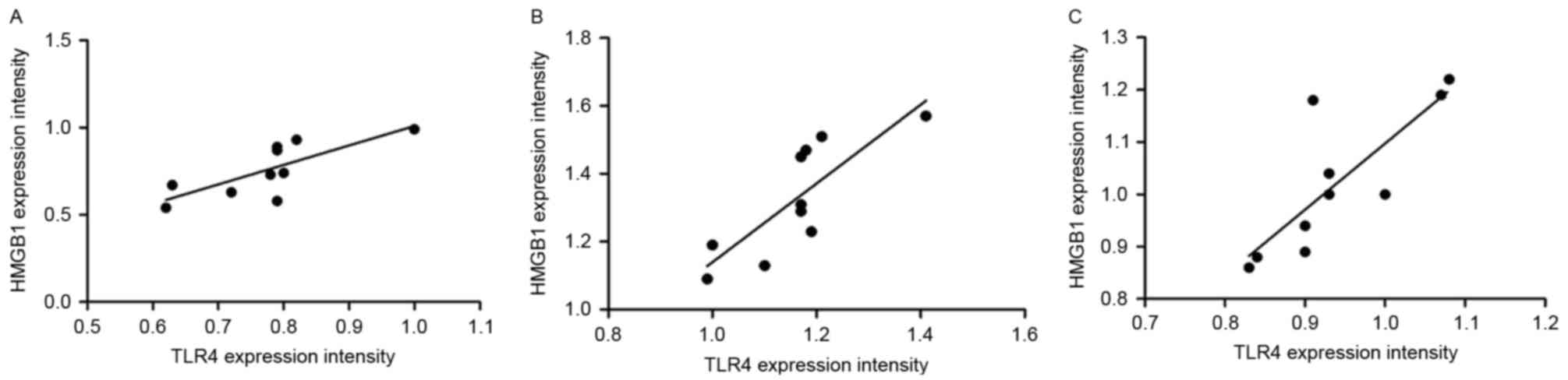
Correlation between the protein
expression levels of TLR4 and HMGB1 in the rat lung tissues
Pearson's correlation analysis was conducted to
analyze the correlation between TLR4 and HMGB1 protein expression
levels in the lung tissue of the rats (Fig. 2). The results revealed that TLR4 and
HMGB1 expression levels exhibit positive correlations in the
control group (r=0.764, P=0.010), model group (r=0.814, P=0.004)
and experimental group (r=0.805, P=0.005).
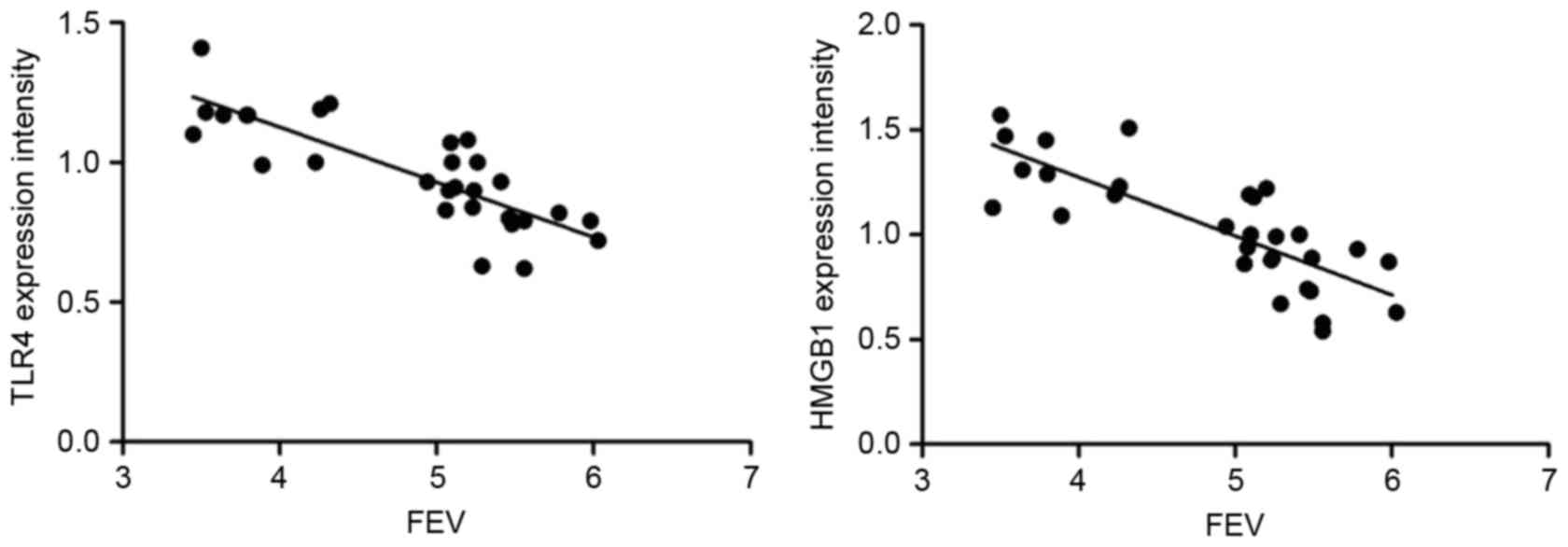
Correlation between TLR4 and HMGB1
expression levels and the lung function of rats
Spearman's correlation analysis was conducted to
analyze the correlation between the rat lung function index FEV,
and TLR4 and HMGB1 protein expression levels (Fig. 3). The results reveal that there is a
significant negative correlation between FEV, and TLR4 (r=−0.845,
P<0.001) and HMGB1 expression levels (r=−0.820, P<0.001).
Discussion
Currently, it is generally considered that COPD is
characterized by chronic inflammation in the airway, lung
parenchyma and pulmonary vascular vessels (21). The activated inflammatory cells have
the ability to release numerous inflammatory mediators, which can
damage the lung tissue structure and/or promote an inflammatory
reaction (22). Therefore, the
release of inflammatory mediators serves an important role in the
occurrence and development of COPD; in addition,
protease/anti-protease imbalance serves an important role in the
pathogenesis of COPD (23). Previous
studies have revealed that ulinastatin, a type of broad-spectrum
protease inhibitor, can reduce tissue damage by inhibiting the
release of inflammatory mediators, as observed in acute kidney
injury (24), acute pancreatitis
(25) and acute lung injury (7,26);
however, there are very limited reports on the treatment of COPD
with ulinastatin. Therefore, in the present study COPD rat models
were established, and underwent ulinastatin treatment, to determine
whether ulinastatin had an effect on COPD; which may eventually
lead to the elucidation of the underlying disease mechanism.
Pulmonary function tests are the most commonly used
clinical indicators to assess COPD lesions, and can confirm the
nature and extent of lung injury; FEV, FEV/FVC and peak expiratory
flow (PEF) are important clinical indicators of lung function, and
can be used to monitor the extent of COPD, and thus guide the
selection of treatment (27,28). The present study used the pulmonary
function test indicators to evaluate the efficacy of ulinastatin.
The results revealed that after the treatment with ulinastatin, the
FEV0.3, FVC, FEV0.3/FVC and PEF indexes in the experimental group
were significantly higher than those in the model group; this
suggests that the rat lung function had improved to a certain
extent, and, therefore, that ulinastatin had a protective effect on
the lungs of COPD rats. Ulinastatin exerts its inhibitory effect on
the activity of various proteases, and carbohydrate and lipid
hydrolases, while simultaneously inhibiting the production of
oxygen free radicals, thus reducing the oxidative damage to and
inflammatory reactions of lung tissues. As HMGB1 is an important
cytokine for initiating and maintaining inflammatory reactions, the
expressions of HMGB1 and TLR4 signaling pathway-associated
molecules, TLR4, MyD88, TRAF-6 and LOX-1, were detected. The
results revealed that, compared with in the control group, the mRNA
and protein expression levels of TLR4, MyD88, TRAF-6, LOX-1 and
HMGB1 were significantly higher in the model group, suggesting that
the HMGB1/TLR4 signaling pathway is involved in the occurrence of
COPD. After the treatment with ulinastatin, the expression levels
of TLR4, MyD88, TRAF-6, LOX-1 and HMGB1 mRNA and protein were
significantly decreased in the experimental group, compared with in
the model group, and FEV exhibited a significant negative
correlation with TLR4 and HMGB1 expression levels. These suggests
that the protective effect of ulinastatin on the lung of the COPD
rat is associated with inhibiting the expression of molecules
associated with the HMGB1/TLR4 signaling pathway. In a previous
study, Ko et al (29) reported
that HMGB1 was associated with the occurrence of COPD, and that the
serum expression level of HMGB1 had a significant negative
correlation with the FEV1/FVC ratio. Kanazawa et al
(30) revealed that the HMGB1 content
in the epithelial lining fluid of patients with COPD was notably
higher than in the healthy control population. The study by Gangemi
et al (15) demonstrated that
the content of the inflammatory factor HMGB1 in the peripheral
blood of patients with COPD was notably elevated. In the present
study, the HMGB1 expression in the lung tissues of the COPD model
rats was significantly higher than in the control group, indicating
that HMGB1 may participate in promoting the onset of COPD. The data
are consistent with the studies conducted by Kanazawa et al
(30) and Gangemi et al
(15). Furthermore, the study by Li
et al (31) determined that,
compared with in the healthy control population, TRL4 expression in
the bronchoalveolar lavage fluid of patients with COPD was
significantly high. In the present study, HMGB1 expression was
significantly higher in the lung tissues of the COPD model rats,
compared with in the control rats, indicating that TLR4
participates in the onset of COPD; these results were similar to
those reported by Li et al (31).
Simvastatin is closely associated with the treatment
mechanism of COPD and the inhibition of TLR4 expression (32), and isothiocyanate serves an
anti-inflammatory role in the treatment of COPD by inhibiting the
expression of molecules associated with the TLR4/MyD88 signaling
pathway (33); however, there are no
associated reports on the treatment of COPD rat with ulinastatin,
to the best of our knowledge.
The pathogenesis of COPD is complex, along with the
treatment mechanism of ulinastatin in COPD (34,35). In
the present study, the focus was on the HMGB1/TLR4 signaling
pathway, and the conclusion is that the protective effect of
ulinastatin on the lungs of COPD rats may be associated with
changes in the HMGB1/TLR4 signaling pathway; however, what it
discloses is only the tip of the iceberg in its complex action
mechanism. For the better application of ulinastatin in the
clinical treatment of COPD, further exploration of the mechanism of
action is required.
Acknowledgements
The authors would like to thank Dr. Daijiao Yi
(Department of Respiratory Medicine, The Second People's Hospotial
of Hunan Province, Hunan, China) for their help with animal feeding
and specimen processing and Dr. Zhuolan Chen (The Medical
Ultrasound, Hunan Children's Hosptial, Hunan, China) for her help
in data collection.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WL was responsible for the acquisition of data in
animal experiments and drafting the manuscript. WZ was responsible
for the statistical analysis, writing and revision of the paper. ZL
was responsible for analysis and interpretation of data in animal
experiments and revising the manuscript. SC was responsible for the
design and modification of experimental protocols, statistical
analysis and thesis revision.
Ethics approval and consent to
participate
The experimental program in this study was examined
and ethically approved by the Institute Research Ethics Committee
at Hunan Provincial People's Hospital (Changsha, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
TLR4
|
toll-like receptor 4
|
|
COPD
|
chronic obstructive pulmonary
disease
|
|
FEV
|
forced expiratory volume/sec
|
|
HMGB1
|
high mobility group box protein 1
|
|
MyD88
|
myeloid differentiation factor 88
|
|
TRAF-6
|
TNF receptor-associated factor 6
|
|
LOX-1
|
lectin-type oxidized LDL receptor
1
|
|
LPS
|
lipopolysaccharide
|
|
RT-qPCR
|
reverse transcription-quantitative
polymerase chain reaction
|
|
RT
|
reverse transcriptase
|
|
FVC
|
forced vital capacity
|
|
PEF
|
peak expiratory flow
|
References
|
1
|
Doucet M, Rochette L and Hamel D:
Incidence, prevalence, and mortality trends in chronic obstructive
pulmonary disease over 2001 to 2011: A public health point of view
of the burden. Can Respir J. 2016:75182872016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pauwels RA and Rabe KF: Burden and
clinical features of chronic obstructive pulmonary disease (COPD).
Lancet. 364:613–620. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bao H, Fang L and Wang L: Prevalence of
chronic obstructive pulmonary disease among community population
aged ≥40 in China: A meta-analysis on studies published between
1990 and 2014. Zhonghua Liu Xing Bing Xue Za Zhi. 37:119–124.
2016.(In Chinese). PubMed/NCBI
|
|
4
|
Zhong N, Wang C, Yao W, Chen P, Kang J,
Huang S, Chen B, Wang C, Ni D, Zhou Y, et al: Prevalence of chronic
obstructive pulmonary disease in China: A large, population-based
survey. Am J Respir Crit Care Med. 176:753–760. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vestbo J, Hurd SS, Agusti AG, Jones PW,
Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ,
Nishimura M, et al: Global strategy for the diagnosis, management,
and prevention of chronic obstructive pulmonary disease: GOLD
executive summary. Am J Respir Crit Care Med. 187:347–365. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fang Y, Xu P, Gu C, Fu XJ, Yu WR and Yao
M: Ulinastatin improves pulmonary function in severe burn-induced
acute lung injury by attenuating inflammatory response. J Trauma.
71:1297–1304. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li W, Qiu X, Jiang H, Zhi Y, Fu J and Liu
J: Ulinastatin inhibits the inflammation of LPS-induced acute lung
injury in mice via regulation of AMPK/NF-κB pathway. Int
Immunopharmacol. 29:560–567. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang SY, Li ZJ, Wang X, Li WF and Lin ZF:
Effect of ulinastatin on HMGB1 expression in rats with acute lung
injury induced by sepsis. Genet Mol Res. 14:4344–4353. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang Y, Qiu X, Zhou G, Liu Z, Chang N and
Jia C: Early effects of ulinastatin by aerosol inhalation on
rabbits with lipopolysaccharide-induced acute lung injury. Zhonghua
Shao Shang Za Zhi. 30:203–207. 2014.(In Chinese). PubMed/NCBI
|
|
10
|
Wang N, Liu X, Zheng X, Cao H, Wei G, Zhu
Y, Fan S, Zhou H and Zheng J: Ulinastatin is a novel candidate drug
for sepsis and secondary acute lung injury, evidence from an
optimized CLP rat model. Int Immunopharmacol. 17:799–807. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dange RB, Agarwal D, Teruyama R and
Francis J: Toll-like receptor 4 inhibition within the
paraventricular nucleus attenuates blood pressure and inflammatory
response in a genetic model of hypertension. J Neuroinflammation.
12:312015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang H, Bloom O, Zhang M, Vishnubhakat JM,
Ombrellino M, Che J, Frazier A, Yang H, Ivanova S, Borovikova L, et
al: HMG-1 as a late mediator of endotoxin lethality in mice.
Science. 285:248–251. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li J, Hu C, Yao Y and Yang H: Effects of
ulinastatin on immune function of spleen in severely burned rats
and its mechanism. Zhonghua Shao Shang Za Zhi. 32:266–271. 2016.(In
Chinese). PubMed/NCBI
|
|
14
|
Tong Y, Tang Z, Yang T, Yang Y, Yang L,
Shen W and Chen W: Ulinastatin preconditioning attenuates
inflammatory reaction of hepatic ischemia reperfusion injury in
rats via high mobility group box 1(HMGB1) inhibition. Int J Med
Sci. 11:337–343. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gangemi S, Casciaro M, Trapani G,
Quartuccio S, Navarra M, Pioggia G and Imbalzano E: Association
between HMGB1 and COPD: A systematic review. Mediators Inflamm.
2015:1649132015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen Y, Huang XJ, Yu N, Xie Y, Zhang K,
Wen F, Liu H and Di Q: HMGB1 contributes to the expression of
P-glycoprotein in mouse epileptic brain through toll-like receptor
4 and receptor for advanced glycation end products. PLoS One.
10:e1409182015.
|
|
17
|
Li G, Wu X, Yang L, He Y, Liu Y, Jin X and
Yuan H: TLR4-mediated NF-κB signaling pathway mediates
HMGB1-induced pancreatic injury in mice with severe acute
pancreatitis. Int J Mol Med. 37:99–107. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cheng Y, Wang D, Wang B, Li H, Xiong J, Xu
S, Chen Q, Tao K, Yang X, Zhu Y and He S: HMGB1 translocation and
release mediate cigarette smoke-induced pulmonary inflammation in
mice through a TLR4/MyD88-dependent signaling pathway. Mol Biol
Cell. 28:201–209. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lai CH, Wang KC, Lee FT, Tsai HW, Ma CY,
Cheng TL, Chang BI, Yang YJ, Shi GY and Wu HL: Toll-like receptor 4
is essential in the development of abdominal aortic aneurysm. PLoS
One. 11:e1465652016.
|
|
20
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Reséndiz-Hernández JM and Falfán-Valencia
R: Genetic polymorphisms and their involvement in the regulation of
the inflammatory response in asthma and COPD. Adv Clin Exp Med.
27:125–133. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huckle AW, Fairclough LC and Todd I:
Prophylactic antibiotic use in COPD and the potential
anti-inflammatory activities of antibiotics. Respir Care.
63:609–619. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yamasaki K and Eeden S: Lung macrophage
phenotypes and functional responses: Role in the pathogenesis of
COPD. Int J Mol Sci. 19:pii: E582. 2018. View Article : Google Scholar
|
|
24
|
Wan X, Xie X, Gendoo Y, Chen X, Ji X and
Cao C: Ulinastatin administration is associated with a lower
incidence of acute kidney injury after cardiac surgery: A
propensity score matched study. Crit Care. 20:422016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhang C, Wang Y, Fu W, Zhang W, Wang T and
Qin H: A meta-analysis on the effect of ulinastatin on serum levels
of C-reactive protein, interleukin 6, and tumor necrosis factor
alpha in Asian patients with acute pancreatitis. Genet Test Mol
Biomarkers. 20:118–124. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sun R, Li Y, Chen W, Zhang F and Li T:
Total ginsenosides synergize with ulinastatin against septic acute
lung injury and acute respiratory distress syndrome. Int J Clin Exp
Pathol. 8:7385–7390. 2015.PubMed/NCBI
|
|
27
|
Yanagisawa S and Ichinose M: Definition
and diagnosis of asthma-COPD overlap (ACO). Allergol Int.
67:172–178. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Twigg MJ and Wright DJ: Community pharmacy
COPD services: What do researchers and policy makers need to know?
Integr Pharm Res Pract. 6:53–59. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ko HK, Hsu WH, Hsieh CC, Lien TC, Lee TS
and Kou YR: High expression of high-mobility group box 1 in the
blood and lungs is associated with the development of chronic
obstructive pulmonary disease in smokers. Respirology. 19:253–261.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kanazawa H, Tochino Y, Asai K, Ichimaru Y,
Watanabe T and Hirata K: Validity of HMGB1 measurement in
epithelial lining fluid in patients with COPD. Eur J Clin Invest.
42:419–426. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li H, Yang T, Li FY, Ning Q and Sun ZM:
TLR4 overexpression inhibits endothelial PAS domain-containing
protein 1 expression in the lower respiratory tract of patients
with chronic COPD. Cell Physiol Biochem. 39:685–692. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang S, Xiong L, Deng X, Ren W, Zhu C, Li
C and Zhou Q: Effects of simvastatin on airway inflammation and
airway mucus hypersecretion in rats with chronic obstructive
pulmonary disease. Zhonghua Yi Xue Za Zhi. 95:1726–1730. 2015.(In
Chinese). PubMed/NCBI
|
|
33
|
Zeng X, Liu X, Bao H, Zhang Y, Wang X, Shi
K and Pang Q: Effects of sulforaphane on Toll-like receptor
4/myeloid differentiation factor 88 pathway of monocyte-derived
macrophages from patients with chronic obstructive pulmonary
disease. Zhonghua Jie He He Hu Xi Za Zhi. 37:250–254. 2014.(In
Chinese). PubMed/NCBI
|
|
34
|
Wang J, Wu A and Wu Y: Endothelial
glycocalyx layer: A possible therapeutic target for acute lung
injury during lung resection. Biomed Res Int. 2017:59696572017.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Liu W and Chai JK: Influences of
ulinastatin on acute lung injury and time phase changes of
coagulation parameters in rats with burn-blast combined injuries.
Zhonghua Shao Shang Za Zhi. 34:32–39. 2018.(In Chinese). PubMed/NCBI
|