Introduction
Cardiac fibroma is a rare benign primary tumor of
the heart, which has been reported as the second most common benign
cardiac tumor following rhabdomyoma in the pediatric population
(1). Fibroma accounts for between 12
and 16% of primary cardiac tumors in children (2). Signs and symptoms are nonspecific,
including arrhythmias, dyspnea, cyanosis, chest-pain and sudden
mortality (3). However, a number of
patients with cardiac fibroma are asymptomatic (4). The prevalence of cardiac fibroma is rare
in the adult population (5). Cardiac
fibromas generally are surgically resected, and patients with large
tumors that cause heart failure require heart transplantation
(2). Asymptomatic tumors require a
long-term follow-up or surgical resection as a preventive measure
to avoid complications (6).
Echocardiography is the initial diagnostic modality for evaluating
cardiac fibroma, and computed tomography (CT) or magnetic resonance
imaging (MRI) can be as supplementary diagnostic techniques. The
present case report describes an adult with cardiac fibroma arising
from the left ventricle.
Case report
A 43-year-old man presented with cough and shortness
of breath, which continued for 2 months. The individual was
admitted to the First People's Hospital of Chengdu (Chengdu, China)
in June 2015, and a presumptive diagnosis of bronchitis was reached
based on the aforementioned symptoms. Informed consent was obtained
from the patient for publication of the present case report.
Following relevant, standard treatment for bronchitis
(chemotherapeutics and intravenous infusion therapy), the cough
symptoms improved, however, the shortness of breath remained, and
the patient complained of a slight chest pain. These symptoms had
no association with regular activities such as walking.
Electrocardiogram indicated normal sinus rhythm, and physical
examination revealed normal blood pressure and regular pulse.
Subsequently, echocardiography was performed, and revealed a large
mass located in the left ventricular lateral wall. The patient was
transferred to the West China Hospital, Sichuan University
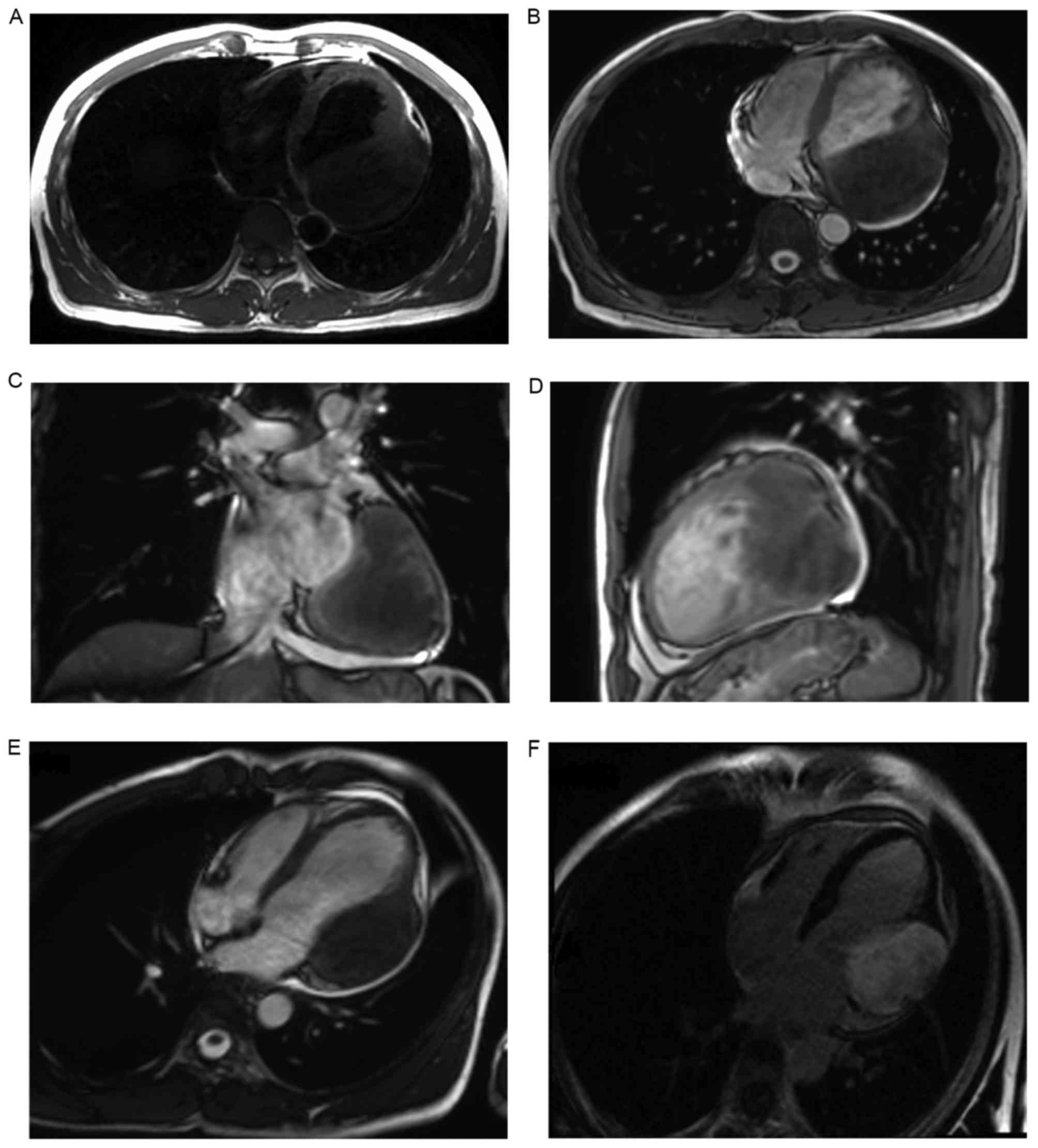
(Chengdu, China) for further investigation. Cardiac magnetic
resonance imaging (MRI) indicated a large mass located in the
lateral wall of the left ventricle. The mass was regular and well
defined, with a size of 10×7×7 cm. Fig.
1A-D are MRI images captured of the T1 transaxial section, T2
transaxial section, T2 coronal section and T2 sagittal section,
respectively. The mass was T1 iso-intense compared with cardiac
muscle (Fig. 1A) and T2 hypo-intense
compared with cardiac muscle (Fig.
1B-D). Myocardial first-pass perfusion images indicated a lack
of enhancement in the mass compared to the myocardial wall
(Fig. 1E). By contrast, in delayed
phase perfusion images, the mass showed heterogeneous enhancement
(Fig. 1F). In addition, MRI
functional analysis reported no abnormality in cardiac
function.
The patient underwent surgical excision of the tumor
under standard cardiopulmonary bypass, and median sternotomy was
performed. Under cardioplegic arrest and aortic cross clamping, the
left ventricle was opened through the posterior wall. The tumor
mass was fully resected, including a part of the lateral wall. The
resultant defect was reinforced with a polytetrafluoroethylene
patch. Histopathological examination conducted by the Pathology
Department of West China Hospital, Sichuan University confirmed the
mass to be a fibroma. The patient had a good postoperative recovery
and was discharged on day 9 post-surgery. Follow-up
echocardiography was performed every 3 months post-surgery, there
is no evidence of recurrence and the patient remains
asymptomatic.
Discussion
Cardiac tumors may be primary or secondary tumors
(4). Primary cardiac tumors are rare,
with a prevalence of <0.03% according to postmortem studies
(1). Cardiac fibromas arise from
heart fibroblasts, and these tumors are mainly located in the
ventricles or interventricular septum (4). Cardiac fibromas generally have no
capsules. Fibromas are able to interdigitate with ventricular
muscle at the tumor border and replace functioning muscle mass,
which may result in intractable congestive heart failure (2,6). Clinical
symptoms and signs of cardiac tumors vary depending on tumor
location and size (7). Cardiac tumors
may be associated with certain symptoms, including chest pain,
cardiomegaly, arrhythmias and even sudden mortality. In some cases,
cardiac tumors may be asymptomatic (1,8).
Echocardiography is non-invasive, fast and does not
involve the use of radiation. It is generally the initial
diagnostic modality for evaluating cardiac fibroma. Supplementary
diagnostic techniques include computed tomography (CT) or MRI. CT
and MRI can provide the location of the tumor, as well as
identifying its surrounding structures and hemodynamic effects. In
addition, MRI can provide additional functional data. Therefore,
cardiac MRI is the modality of choice for further evaluation of
cardiac fibroma (1,4).
In the present study, the cardiac MRI showed a
regular solid lesion, which was iso-intense relative to muscle on
T1-weighted and hypo-intense on T2-weighted images, which suggested
fibrosis (9). Diagnosis was confirmed
by histopathological evaluation of the specimen following surgical
resection.
Cardiac tumors, that are symptomatic, are treated by
surgical resection (3), and if
surgical resection is not possible, heart transplantation is
required (1). The type of surgical
intervention (a total or subtotal resection) depends on the
location of the tumor (1) with total
and subtotal resection reported exhibit good outcomes (10). Asymptomatic tumors require a long-term
follow-up or surgical resection as a preventive measure to avoid
complications (6). In the present
study, the patient presented with symptoms, and therefore surgery
was required. Following operation, the patient had a good recovery,
and echocardiography, which was performed 3 months following
surgical resection, indicated no recurrence.
In conclusion, cardiac fibroma is very rare in
adults. Echocardiogram, CT and cardiac MRI can provide valuable
findings. Surgical excision is a reliable and effective method for
treatment.
References
|
1
|
Ünsal H and Ekici E: Conservative
management of a left ventricle cardiac fibroma in an asymptomatic
child patient. Turk Kardiyol Dern Ars. 43:481–483. 2015.PubMed/NCBI
|
|
2
|
Uzun O, Wilson DG, Vujanic GM, Parsons JM
and De Giovanni JV: Cardiac tumours in children. Orphanet J Rare
Dis. 2:112007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Burke A and Tavora F: The 2015 WHO
classification of tumors of the heart and pericardium. J Thorac
Oncol. 11:441–452. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tao TY, Yahyavi-Firouz-Abadi N, Singh GK
and Bhalla S: Pediatric cardiac tumors: Clinical and imaging
features. Radiographics. 34:1031–1046. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cho SH, Fritz T, Cronin LJ and Cohle SD:
Primary cardiac fibroma in an adult. Case Rep Cardiol.
2015:7137022015.PubMed/NCBI
|
|
6
|
Stiller B, Hetzer R, Meyer R, Dittrich S,
Pees C, Alexi-Meskishvili V and Lange PE: Primary cardiac tumours:
When is surgery necessary? Eur J Cardiothorac Surg. 20:1002–1006.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bruce CJ: Cardiac tumours: Diagnosis and
management. Heart. 97:151–160. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Burke AP, Rosado-de-Christenson M,
Temleton PA and Virmani R: Cardiac fibroma: Clinicopathologic
correlates and surgical treatment. J Thorac Cardiovasc Surg.
108:862–870. 1994.PubMed/NCBI
|
|
9
|
Eric S, Ana S and Philippe D:
Inter-ventricular septal cardiac fibroma in an adult: MR and MDCT
features with pathologic correlation. Eur J Radiol Ext.
67:e103–e106. 2008. View Article : Google Scholar
|
|
10
|
Cho JM, Danielson GK, Puga FJ, Dearani JA,
McGregor CG, Tazelaar HD and Hagler DJ: Surgical resection of
ventricular cardiac fibromas: Early and late results. Ann Thorac
Surg. 76:1929–1934. 2003. View Article : Google Scholar : PubMed/NCBI
|