Introduction
Cystatins are a superfamily of cysteine proteinase
inhibitors found in animals and plants. Cystatin-C, a secreted
molecule of the cystatin family, is composed of 120 amino acids and
has a molecular weight of 13,260 Da. Cystatin-C is increased in
patients with cancer and is suggested to be a better renal
functional marker than creatinine. In pediatric patients with
cancer, cystatin-C is a suitable marker for monitoring renal
function during chemotherapy (1). The
importance of the accurate assessment of renal function in patients
with cancer is increasing, and the prediction of the glomerular
filtration rate with combined evaluation of cystatin-C and
creatinine is being tested for anticancer agents, such as cisplatin
(2). By contrast, a low level of
cystatin-C is associated with atherosclerosis and aortic aneurysm.
Additionally, it has been suggested that cystatin-C adversely
affects metabolic factors, in particular abdominal obesity, and
thus contributes to the development of metabolic syndrome (3).
Cathepsin B is a lysosomal cysteine protease in
normal tissues, and an important matrix protease in cancers,
including lung cancer, colon cancer and hepatocellular carcinoma
(4). Activated cathepsin B is
considered to be involved in cancer invasion and the destruction of
the basement membrane, by degrading collagen, laminin and
proteoglycans. Cathepsin B is regulated by cysteine protease
inhibitors, such as stefin A, stefin B and cystatin-C. In
colorectal cancer, cathepsin B expression may contribute to early
stage invasion and systemic metastasis, without the effect of
cystatin-C (5). It has been reported
that non-malignant colorectal tissues do not express cystatin-C,
whilst cancer tissues expressed high levels of both cystatin-C and
cysteine proteinase inhibitors (6).
In a previous study of esophageal cancer, the intensity of
cystatin-C immunostaining in cancer tissue was increased compared
with the adjacent normal esophageal tissues. In addition, the mRNA
expression levels of cystatin-C were increased in cancerous tissue
compared with normal tissue (7). In
prostate cancer, a significant reduction in the immunohistochemical
expression of cystatin-C in non-neuroendocrine prostate cancer has
been reported (8). However, there was
strong expression of cystatin-C in neuroendocrine-like cells
compared with benign prostate tissues, suggesting a strong
connection between cystatin-C expression and neuroendocrine
differentiation (8). In breast
cancer, an imbalance between cathepsin B and cystatin-C expression
has been reported in the early stages of cancer progression.
However, no correlation between cathepsin B and cystatin-C
expression levels in histological classification, tumor size, lymph
node metastasis and hormonal receptor status was observed (9). Generally, an increase in the ratio of
cathepsins to cystatins contributes to tumor invasiveness and
metastasis (10). However, data are
conflicting regarding the role of cystatins in cancer invasion and
metastasis. High levels of cystatin-B and -C predict poor survival
of patients with colorectal cancer, and increased cystatin-F showed
a strong correlation with liver metastasis in colorectal cancer
(11). Additionally, high levels of
cystatin-A exhibited a strong correlation with tumor size and
increased mitotic activity in breast cancer (12).
Extracellular levels of stefins and cystatin-C are
also associated with cancer progression. In hepatocellular
carcinoma, increased serum stefin A levels correlated with tumor
size and number (13), and increased
serum cystatin-C levels correlated with tumor stage in melanoma
(14). In colorectal cancer, a
correlation between high levels of extracellular cystatin-C and
poor survival was observed (15). In
elderly patients with lung cancer, serum cystatin-C levels
increased in an age-dependent manner between 65 and ≥75 years
(16). In serum samples from patients
with breast cancer, high cystatin-C levels were found in larger
sized tumors, in older patients and in post-menopausal women.
Significantly lower levels of cathepsin X and H were found in
patients with inflammatory breast cancer, and a trend was also
observed for cathepsin B and cystatin-C (17).
The present study aimed to evaluate circulating
cystatin-C as a biomarker at different clinical time points in
patients with breast cancer over a long-term follow-up period. In
addition, the excretory rate of circulating cystatin-C was
investigated by comparing the blood and tissue expression levels of
cystatin-C. To the best of our knowledge, the present study is the
first to simultaneously assess the expression levels of cystatin-C
in tissue and serum samples from patients with breast cancer at
different time points of clinical progress.
Materials and methods
Collection of blood and tissues
Blood samples from healthy volunteers (40 males and
40 females) were obtained at Inha University Hospital (Incheon,
Korea), subsequent to obtaining approval if no laboratory and
imaging abnormalities were observed following check-up in 2003.
Blood samples from 34 female patients with breast cancer were
obtained at 205 different time points of initial diagnosis state,
during chemotherapy period and off-chemotherapy state between
January 1999 and January 2003, and stored at −80°C. Heparinized
vacuum tubes and needles (BD Biosciences, Franklin Lakes, NJ, USA)
were used to avoid platelet damage and venous occlusion, as in
clinical sample setting. Following surgical excision (29 specimens)
or biopsy (23 specimens) between January 1992 and December 2002,
specimens were fixed in 10% formalin and embedded in paraffin.
Approval for the present study was obtained from the Institutional
Review Board of Severance Hospital (Seoul, Korea) and Inha
University Hospital (IRB 4-2009-0256 and 10–617, respectively) and
samples were used subsequent to obtaining consent from volunteers
and patients.
Determination of the normal range of
serum cystatin-C
Using 40 healthy male and 40 healthy female
volunteer blood samples, the normal cut-off point of cystatin-C was
determined. The cut-off point was determined using the mean ± 2
standard deviations. The serum cystatin-C level was determined as
positive when the blood value of the patient was higher than the
cut-off value (18).
Immunohistochemistry
Sections (4-µm) were stained by the horseradish
peroxidase (HRP) labeling method. The specimens were deparaffinized
and immersed in a solution of 0.1% hydrogen peroxide in methanol to
eliminate endogenous peroxidase activity. The antibody used was
rabbit anti-human cystatin-C polyclonal antibody (cat. no. ab68290;
Abcam, Cambridge, MA, USA) with a 1:2,000 dilution. In total, a
maximum of 500 cancer cells were counted. Positive staining was
defined as the presence of cytoplasmic immunoreactivity in a
minimum of 10% of cancer cells.
ELISA assay
A sandwich ELISA was used to measure cystatin-C,
cancer antigen (CA) 15-3 and CA125 levels, according to the
manufacturer's instructions. In brief, murine polyclonal antibody
specific for cystatin-C (RD 191009100; dilution, 1:400; BioVendor,
Brno, Czech Republic), and monoclonal antibodies specific for
CA15-3 (cat. no. IS-F3329; LSBio, Seattle, WA, USA) and CA125 (cat.
no. CA239T; Calbiotech, Inc., El Cajon, CA, USA) were used to coat
the 96-well microplates. Each standard and sample was added to the
plate and incubated for 1 h at room temperature. Following washing
to remove unbound proteins, enzyme-linked antibodies specific for
cystatin-C, CA15-3 and CA125 were added to the wells. Absorbance
was measured at 450 nm and the detection limit of cystatin-C was
0.25 ng/ml. A standard curve was constructed by plotting absorbance
values vs. the cystatin-C, CA15-3 and CA125 concentrations of the
standards, and the concentrations of the test samples were
determined using this standard curve. All samples were run in
triplicate. The intra- and inter-assay variations of cystatin-C
were 3.4 and 6.9%, respectively. Dilutional linearity was 98%. The
upper normal range were 25 U/ml for CA15-3 and 35 IU/ml for
CA125.
Statistical analysis
The statistical analysis and graphing were performed
using SPSS software, version 20 (IBM Corp., Armonk, NY, USA) and
GraphPad Prism version 5 (GraphPad Software, Inc., La Jolla, CA,
USA). The differences between the groups were analyzed using
one-way analysis of variance (Wilcoxon rank-sum test and paired
t-test) and the post-hoc test was performed by Turkey test.
Correlation between variables was estimated using the Spearman's
rank correlation coefficient. P<0.05 was considered to indicate
a statistically significant difference.
Results
Volunteers and patients with breast
cancer
The median age of the healthy male and female
volunteers was 41 (range, 25–66 years) and 35 years (range, 21–56
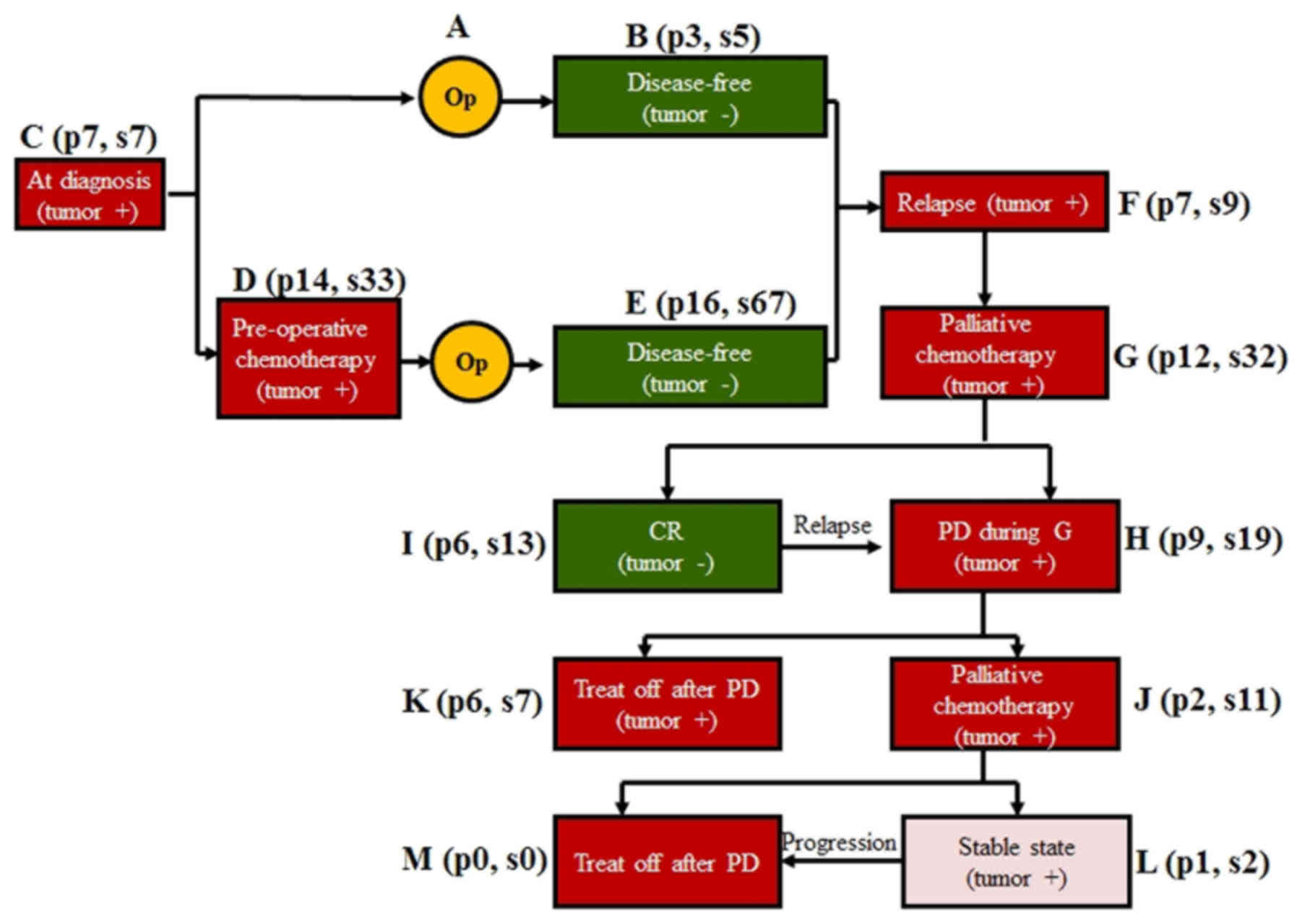
years), respectively. A total of 205 samples were obtained from 34
patients with breast cancer (median age, 45 years; range, 32–65
years) in 12 different disease states during long-term follow-up
and treatment (Fig. 1). Blood was
also obtained prior to surgery in 7 patients with prostate cancer
and 13 patients with colon cancer.
Normal range of cystatin-C
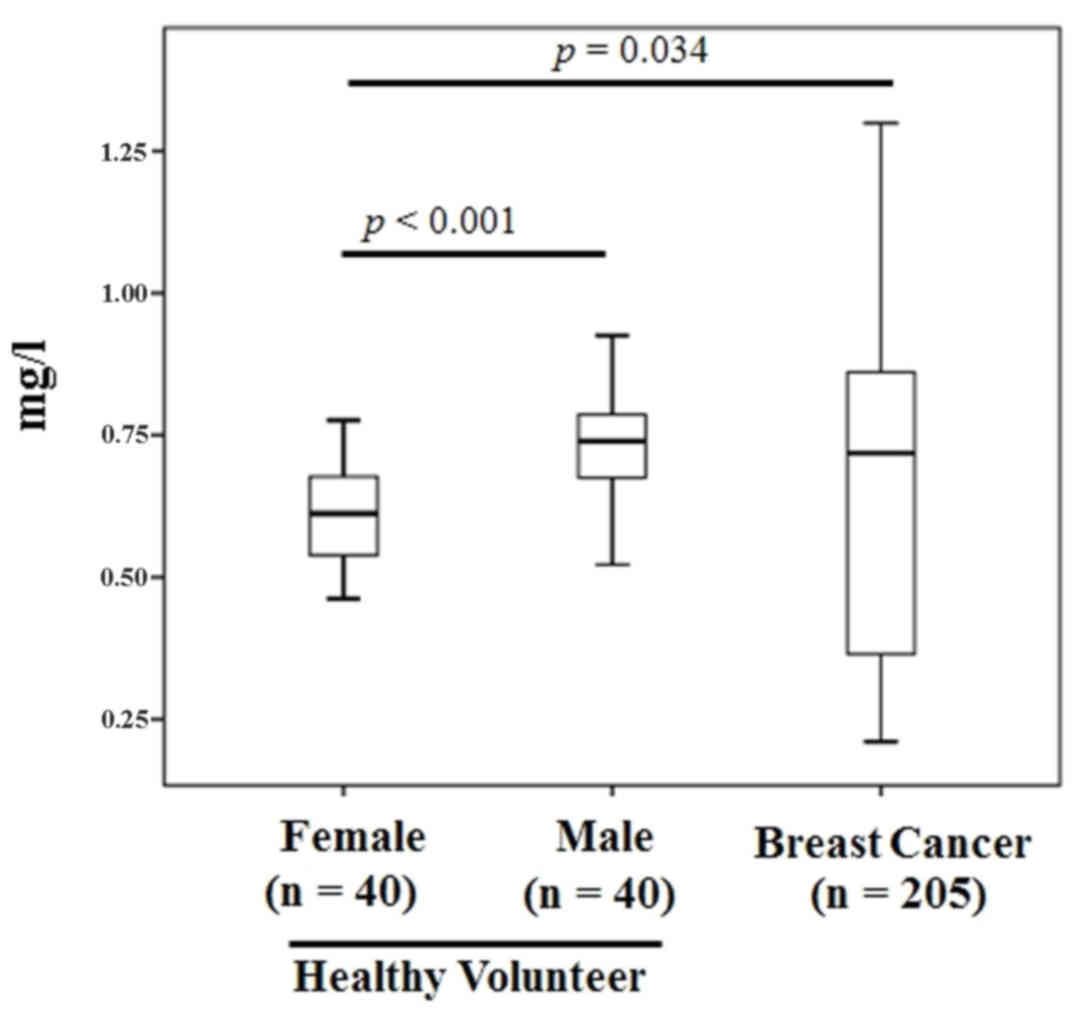
The mean levels of cystatin-C in healthy female and
male volunteers were 0.61±0.09 and 0.73±0.09 mg/l, respectively.
The levels were increased in men compared with women (P<0.001)
and in patients with breast cancer compared with female volunteers
(P=0.034) (Fig. 2). Using a cut-off
point of the mean ± 2 standard deviations, the cut-off point was
0.91 mg/l in men and 0.79 mg/l in women. There was no evidence of
an effect of age in men or women (Table
I). The positivity rate was 46% in patients (38/83) and 40% in
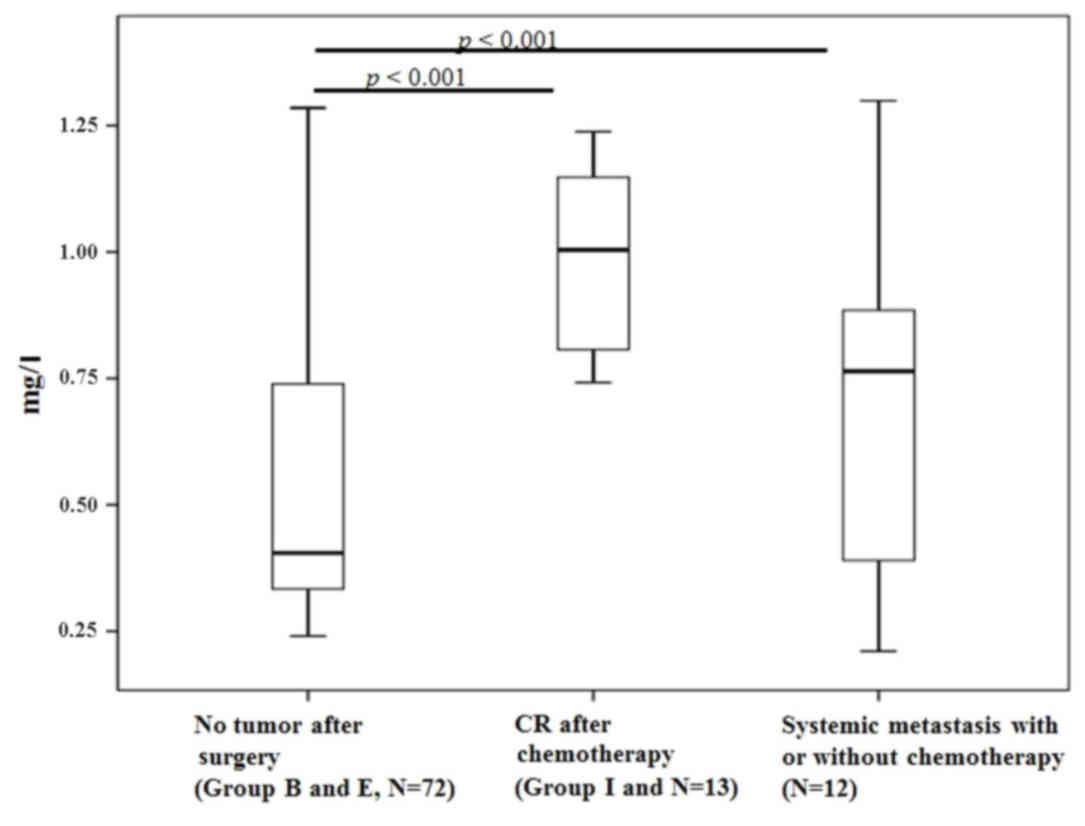
samples collected from the different time points (82/205; Table II). Blood cystatin-C levels were
lowest following surgery compared with patients with systemic
metastasis (P<0.001; Fig. 3). The
sensitivity, specificity and accuracy rate of the ELISA was 53.6,
63.6 and 53.9%, respectively (Table
III). Among the 7 patients with prostate cancer, only 1 patient
(14.2%) showed cystatin-C positivity by ELISA. In the 13 patients
with resectable colon cancer, no patients exhibited cystatin-C
positivity in the blood.
 | Table I.Comparison of blood cystatin-C levels
by ages in healthy volunteers. |
Table I.
Comparison of blood cystatin-C levels
by ages in healthy volunteers.
|
| Age, years |
|---|
|
|
|
|---|
| Sex | 21–30 | 31–40 | 41–50 | 51–60 | 61–70 | Total |
|---|
| Male |
| Number,
n | 10 | 10 | 13 | 5 | 2 | 40 |
| Mean ±
SD | 0.67±0.10 | 0.76±0.07 | 0.78±0.09 | 0.71±0.04 | 0.66±0.02 | 0.73±0.09 |
|
Median | 0.68 | 0.77 | 0.77 | 0.71 | 0.66 | 0.74 |
| Female |
| Number,
n | 12 | 16 | 10 | 2 | 0 | 40 |
| Mean ±
SD | 0.60±0.09 | 0.65±0.09 | 0.55±0.07 | 0.67±0.03 | – | 0.61±0.09 |
|
Median | 0.61 | 0.65 | 0.55 | 0.67 | – | 0.61 |
| Table II.Comparison of blood cystatin-C
positivity at 12 different clinical time points. |
Table II.
Comparison of blood cystatin-C
positivity at 12 different clinical time points.
| Tumor state | Patient group | Number of patients,
n | Cystatin-C-positive
patients, positive/total (%) | Cystatin-C-positive
samples, n (%) Positive/total |
|---|
| Presence of
tumor |
| 25 |
|
|
| At
diagnosis | Group C | 7 | 3/7 (43) | 3/7 (43) |
| During
pre-operative chemotherapy | Group D | 8 | 8/14 (57) | 14/33 (42) |
| At first
relapse | Group F | 3 | 1/7 (14) | 1/9 (11) |
| During
1st line palliative chemotherapy | Group G | 5 | 5/12 (42) | 16/32 (50) |
| At PD
after 1st line chemotherapy | Group H | 1 | 6/9 (67) | 10/19 (53) |
| Treat-off
after 1st line chemotherapy | Group K | 1 | 2/6 (33) | 2/7 (29) |
| During
2nd line palliative chemotherapy | Group J | 0 | 2/2 (100) | 11/11 (100) |
| SD
after 2nd line chemotherapy | Group L | 0 | 0/1 (0) | 0/2 (0) |
| PD
after 2nd line palliative chemotherapy | Group M | 0 | 0/0 (0) | 0/0 (0) |
| Absence of
tumor |
| 9 |
|
|
| After
initial surgery | Group B | 3 | 0/3 (0) | 0/5 (0) |
| After
surgery and neoadjuvant chemotherapy | Group E | 4 | 6/16 (38) | 15/67 (22) |
| At CR
after 1st line chemotherapy | Group I | 2 | 5/6 (83) | 10/13 (77) |
| Table III.Comparison of accuracy of cystatin-C
ELISA based on tumor status. |
Table III.
Comparison of accuracy of cystatin-C
ELISA based on tumor status.
|
| Cystatin-C
expression, n (%) |
|---|
|
|
|
|---|
| Tumor status | Positive | Negative | Total, n (%) |
|---|
| Present | 22 (31.7) | 19 (30.2) | 41 (65.1) |
| Absent | 8 (12.7) | 14 (22.2) | 22 (34.9) |
| Total | 30 (47.6) | 33 (52.4) | 63 (100.0) |
Detection of cystatin-C by
immunohistochemistry in patients with breast cancer
Immunohistochemical analysis was conducted at 3
different clinical time points (29 specimens at diagnosis, 21
specimens following pre-operative chemotherapy and 2 specimens at
relapse), including 2 patients with bilateral breast cancer. The
positivity rate was 41.4% (12/29) at diagnosis, 66.7% (14/21)
following pre-operative chemotherapy, and 100% (2/2) following
relapse. In 6 patients it was possible to compare cystatin-C
expression between pre- and post-chemotherapy samples. The
concordance rate was 66.7% (Table
IV). In the 2 patients who relapsed, 1 patient showed
cystatin-C expression in both the primary and relapsed tumors. The
other patient showed no expression in the pre- or post-chemotherapy
samples, while cystatin-C expression was detected in the relapsed
tumor. In the 2 patients with bilateral breast cancer, 1 patient
exhibited simultaneous cystatin-C expression from both breast
tumors, while the second showed discordance in cystatin-C
expression in both breast cancers.
| Table IV.Comparison of cystatin-C expression
by immunohistochemistry at diagnosis (pre-chemotherapy) and
following surgery (post-chemotherapy). |
Table IV.
Comparison of cystatin-C expression
by immunohistochemistry at diagnosis (pre-chemotherapy) and
following surgery (post-chemotherapy).
|
| Cystatin-C
expression |
|---|
|
|
|
|---|
| Patient number | Pre-chemotherapy
(at diagnosis) | Post-chemotherapy
(following surgery) |
|---|
| 1 | Positive | Positive |
| 2 | Negative | Negative |
| 3 | Negative | Positive |
| 4 | Negative | Negative |
| 5 | Negative | Negative |
| 6 | Negative | Positive |
Comparison of paired-tissue
immunohistochemistry and blood ELISA positivity
In 16 patients, tissue immunohistochemistry and
blood ELISA were compared, resulting in a concordance rate of 38%.
The main reason of discordance between tissue and serum expression
of cytostatin-C came from low serum positivity in samples showing
tissue cytostatin-C positivity (3/11, 27%). Additionally, the
specificity rate was 60%. This indicates that in the early stages
of breast cancer, the secretion rate of cystatin-C from the tumor
mass into the blood is quite low (Table
V).
| Table V.Comparison of cystatin-C expression
between paired tissue (immunohistochemistry) and blood (ELISA). |
Table V.
Comparison of cystatin-C expression
between paired tissue (immunohistochemistry) and blood (ELISA).
| Cystatin-C
expression on immunohistochemistry/ELISA | Patients, n |
|---|
|
Positive/positive | 3 |
|
Positive/negative | 8 |
|
Negative/positive | 2 |
|
Negative/negative | 3 |
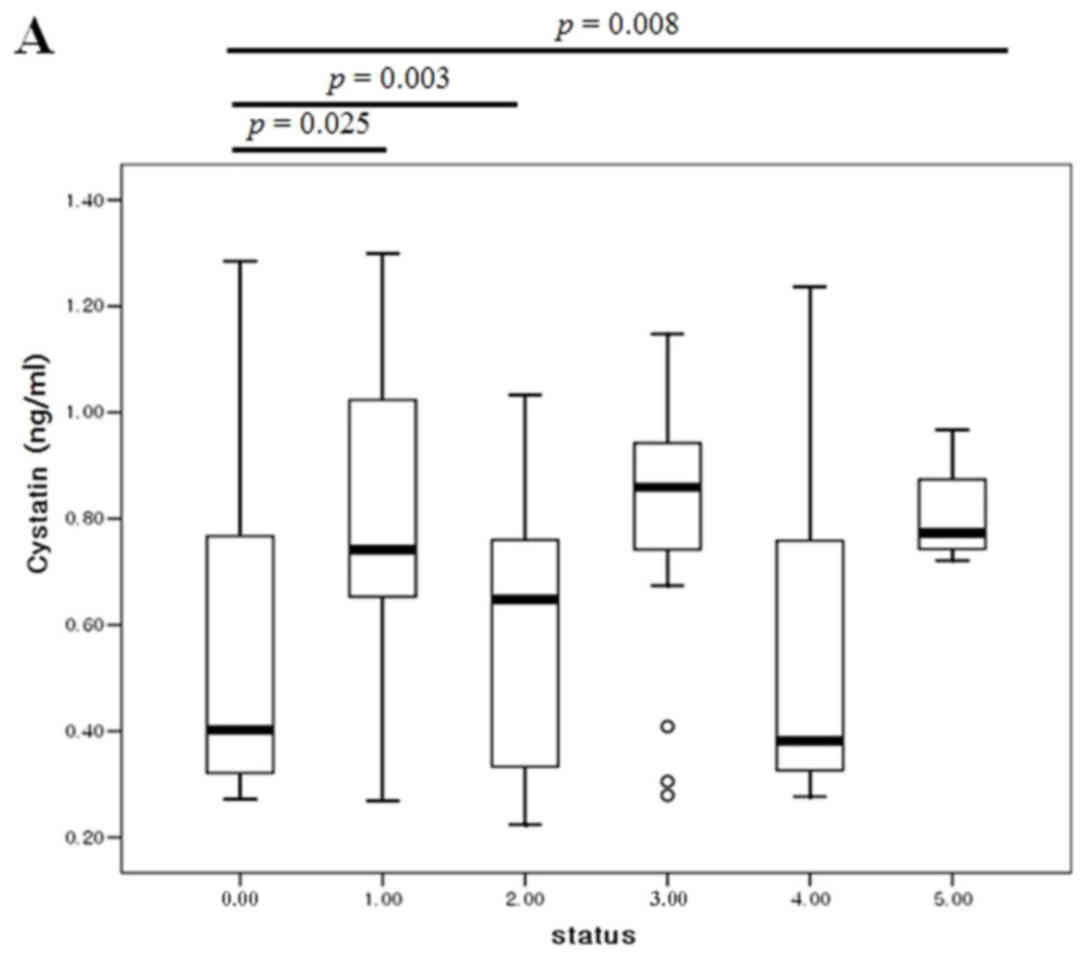
Comparison of serum positivity based
on the clinical status of cancer
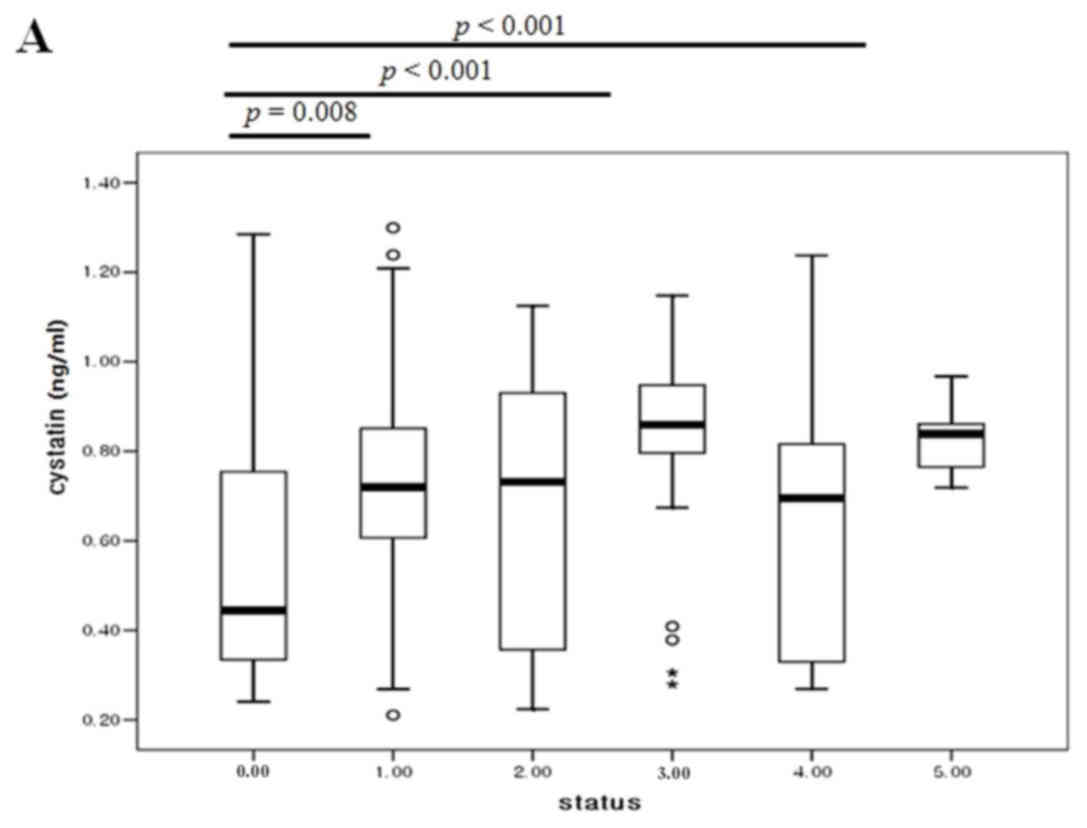
The blood cystatin-C levels were then compared with
the number of metastases from immediate post-operative samples (no
residual tumor), up to 5 tumor metastases. The cystatin-C levels
were lowest following surgery and increased as the number of
metastases increased (Fig. 4A). In 6
patients, the blood cystatin-C levels from both pre- and
post-operative samples were compared. Whilst no patients showed
positivity for cystatin-C expression, the expression levels
exhibited a reducing trend following surgery (P=0.13; Fig. 4B).
Comparison of serum positivity among
cystatin-C, CA15-3 and CA125 in breast cancer
In 92 samples with different states of systemic
metastasis, we simultaneously compared the cystatin-C, CA15-3 and
CA125 levels with the numbers of tumor metastases. As the number of
metastasis increased, CA15-3 (P<0.001), CA125 (P=0.001) and
cystatin-C (P=0.035) showed dynamic alterations compared to
post-operative (no tumor) state (Fig.
5). The accuracy rates of cystatin-C, CA15-3 and CA125 were
50.0, 67.4 and 59.8%, respectively. With tumor presence, the
concordance rate between cystatin-C and CA15-3, and cystatin-C and
CA125 were 66.7 and 53.6%, respectively. Without tumor presence,
the concordance rates between cystatin-C and CA15-3, and cystatin-C
and CA125 were 87.0 and 69.6%, respectively (Table VI).
| Table VI.Comparison of serum positivity among
cystatin-C, CA15-3 and CA125. |
Table VI.
Comparison of serum positivity among
cystatin-C, CA15-3 and CA125.
| A, Tumor
presence |
|---|
|
|---|
| Expression | Total |
|---|
| Total | 69 |
| Cystatin-C (+) | 33 |
| Cystatin-C (−) | 59 |
| CA15-3 (+) | 41 |
| CA15-3 (−) | 28 |
| CA125 (+) | 36 |
| CA125 (−) | 33 |
| Cystatin-C
(+)/CA15-3 (+) | 23 |
| Cystatin-C
(−)/CA15-3 (+) | 18 |
| Cystatin-C
(+)/CA15-3 (−) | 5 |
| Cystatin-C
(−)/CA15-3 (−) | 23 |
| Cystatin-C
(+)/CA125 (+) | 16 |
| Cystatin-C
(−)/CA125 (+) | 20 |
| Cystatin-C
(+)/CA125 (−) | 12 |
| Cystatin-C
(−)/CA125 (−) | 21 |
|
| B, Tumor
absence |
|
|
Expression | Total |
|
| Total | 23 |
| Cystatin-C (+) | 5 |
| Cystatin-C (−) | 18 |
| CA15-3 (+) | 2 |
| CA15-3 (−) | 21 |
| CA125 (+) | 4 |
| CA125 (−) | 19 |
| Cystatin-C
(+)/CA15-3 (+) | 2 |
| Cystatin-C
(−)/CA15-3 (+) | 0 |
| Cystatin-C
(+)/CA15-3 (−) | 3 |
| Cystatin-C
(−)/CA15-3 (−) | 18 |
| Cystatin-C
(+)/CA125 (+) | 1 |
| Cystatin-C
(−)/CA125 (+) | 3 |
| Cystatin-C
(+)/CA125 (−) | 4 |
| Cystatin-C
(−)/CA125 (−) | 15 |
Discussion
Cystatin-C is a non-glycosylated low molecular
weight basic protein and is the product of a housekeeping gene,
CST-3 (19). Cystatin-C is
constitutively produced by all human nucleated cells. Blood
cystatin-C levels are independent of age, body mass index (20) and sex (15) in healthy individuals (20); however, the levels show a weak
association with age due to a reduced glomerular filtration rate in
elderly individuals (21). Finney
et al (20) reported no
difference in cystatin-C levels by age, but the median age of the
control group in their study was 40 years (range, 19–59 years),
while Norlund et al (21)
reported an age dependency in older individuals. The present study
tested blood cystatin-C levels in healthy Korean volunteers (age
range, 21–56 years), which indicated that there was no
age-dependence in males or females. However, the levels were
increased in males compared with in females, potentially due to a
difference in age. The median age of the men was 41 years (range,
25–66 years) and in the women was 35 years (range, 21–56 years).
Ohara et al (16) reported age
dependence in cystatin-C levels in elderly patients with lung
cancer aged >75 years old compared with those aged <65 years
old (16). In patients with colon
cancer, the cystatin-C levels were 1.4-fold increased in all stages
of cancer compared with healthy individuals (15). In breast cancer, inflammatory cancer
type and increased tumor size exhibited high expression levels of
cystatin-C (17). Although the
control group was not age-matched with the patient group in the
present study, patients with breast cancer exhibited increased
levels of cystatin-C compared with healthy volunteers. Due to the
availability of 205 blood samples from 34 patients with breast
cancer at 12 different clinical time points, the cystatin-C
positive rate was evaluated at the different time points. This
demonstrated the tumor mass dependence of cystatin-C level, by the
observation of the lowest serum positivity following surgery, where
there is no tumor. However, despite the increased cystatin-C levels
in patients with cancer, the sensitivity of the blood test was only
53.6% and the accuracy was 53.9%, suggesting a low secretion
capacity from the tumor mass.
Due to the low blood positivity rate,
immunohistochemical analysis of cystatin-C was conducted to
investigate the expression levels of cystatin-C in primary breast
cancer. The expression levels were evaluated at 3 different time
points (at diagnosis, following pre-operative chemotherapy and at
relapse), resulting in a positivity rate of 54.0%, which was
similar to the blood positivity. The positivity rate increased from
diagnosis to relapse, suggesting an association between tumor
progression and cystatin-C expression. In addition, synchronicity
was investigated in 6 paired samples by comparing samples taken at
diagnosis, before chemotherapy, with samples taken following
chemotherapy and surgery, which resulted in a concordance rate of
66.7%. Two initially negative patients exhibited cystatin-C
expression following chemotherapy. This may be due to tumor
heterogeneity from the small biopsy specimen or cystatin-C
induction subsequent to chemotherapy. In previous studies, no
differences in cystatin-C levels were observed in samples from
prior to and subsequent to chemotherapy (median age, 57 years)
(22), while transient increments
(20–40%) were detected following chemotherapy (within 10 days of
chemotherapy) in esophageal cancer (median age, 60 years) (23). This requires further confirmation
through the investigation of an increased number of cases.
As the positivity rate was similar in blood and
tissue levels, tissue expression and blood levels were then
compared in 16 patients. The concordance rate was only 38%, which
mostly resulted from the low blood positivity (27%) in the tissue
positive cases. This suggests that the blood cystatin-C levels are
associated with tumor volume; however, secreted cystatin-C levels
in the blood are quite low in early breast cancer. Laurent-Matha
et al (24) reported the
amount of cystatin-C in the extracellular environment is reduced
when the cell is transfected with cathepsin D. In addition,
cathepsin D secreted by breast cancer cells extensively cleaved
cystatin-C, which may reduce the cystatin-C levels in the blood
(24).
To investigate the association between tumor volume
and blood cystatin-C levels, the cystatin-C levels were compared
with the number of metastases. Cystatin-C was observed to be at the
lowest levels subsequent to surgery, when the tumor had been
removed, with the levels increasing as the number of metastases
increases. As in the immunohistochemical analysis, paired
comparisons were performed between cystatin-C levels prior and
subsequent to surgery in 6 patients. Whilst these patients did not
show serum positivity, the absolute blood levels of cystatin-C
decreased subsequent to surgery compared with the time of
diagnosis, suggesting levels are dependent upon the tumor volume.
Similarly in ovarian cancer, cystatin-C has been reported to
increase only in patients with cancer, not in healthy individuals
and patients with benign ovarian disease (25). By contrast, cystatin-C levels were low
in prostate cancer specimens compared with benign tissues. Wegiel
et al (26) observed an
inverse correlation between the expression of cystatin-C and matrix
metalloproteinase 2. Similarly, the present study did not find any
patients with prostate cancer to be cystatin-C positive, suggesting
a functional specificity of cystatin-C in different types of
cancer, due to the presence of different co-functioning molecules.
Cystatin-C is a TGF-β receptor antagonist in addition to a
cystatin-C-mediated feedback loop that inhibits TGF-β signaling
(27). By inhibiting oncogenic TGF-β
signaling, cystatin-C is effective in preventing breast cancer
angiogenesis and progression (28).
As a cysteine protease inhibitor, it was reported
that cystatin-C reduces cancer invasion and metastasis (25). Cystatin-C was increased in cancer
tissues from ovarian cancer, non-small cell lung cancer and in
blood samples from patients with hepatocellular carcinoma,
melanoma, breast cancer and colon cancer. By contrast, cystatin-C
mRNA levels did not change in pancreatic, head and neck cancer.
Using laser-capture microdissection technology, breast cancer cells
were reported to show increased expression levels of cystatin-C,
with this correlating with increased tumor size (29). However, the increased cystatin-C
expression relative to cathepsin B (9) and cathepsin D (24) expression was reduced. Cathepsin X and
H were significantly lower in inflammatory breast cancer compared
with cystatin-C levels (17). This
imbalance between cysteine protease and proteinase inhibitors may
be associated with the ability of cancer interstitial tissues to
detach, which is important in cancer invasion and metastasis
(9). High levels of stefin B and
cystatin-C were associated with poor prognosis, whether as a result
of primary activation or secondary feedback loop activation
(15). To investigate whether the
elevated levels of cystatin-C were associated with tumor mass, we
then compared dynamic alterations in cystatin-C levels based on
tumor volume with known tumor markers in breast cancer, such as
CA15-3 and CA125. Cystatin-C showed a plateau in the blood levels
as the tumor mass increased, while CA15-3 showed continuous
increases in the blood level with tumor mass increases. The
concordance rates of cystatin-C and CA15-3, cystatin-C and CA125
were low (66.7 and 53.6%) when tumors were present compared with
when tumors were absent (87.0 and 69.6%). This indicates that a
minimum of one-third of breast cancer showed molecular tumor
heterogeneity in the expression of cystatin-C and CA15-3.
In conclusion, elevated blood cystatin-C levels were
detected in 40% of breast cancer cases, with this being tumor
volume-dependent. However, the concordance rate between levels in
tissue and blood samples was low, suggesting tumor heterogeneity in
cystatin-C expression or co-acting pathway activation, such as
cathepsin D. As one-third of breast cancer cases expressed
cystatin-C without CA15-3 elevation, cystatin-C may represent a
good tumor-monitoring marker in breast cancer.
References
|
1
|
Lankisch P, Wessalowski R, Maisonneuve P,
Haghgu M, Hermsen D and Kramm CM: Serum cystatic C is a suitable
marker for routine monitoring of renal function in pediatric cancer
patients, especially of very young age. Pediatr Blood Cancer.
46:767–772. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chew-Harris JS, Florkowski CM, George PM
and Endre ZH: Comparative performances of the new chronic kidney
disease epidemiology equations incorporating cystatin-C for use in
cancer patients. Asia Pac J Clin Oncol. 11:142–151. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Magnusson M, Hedblad B, Engström G,
Persson M, Nilsson P and Melander O: High and Cancer Study. J Int
Med. 274:192–199. 2013. View Article : Google Scholar
|
|
4
|
Sheahan K, Shuja S and Murnane MJ:
Cysteine protease activities and tumor development in human
colorectal carcinoma. Cancer Res. 49:3809–3814. 1989.PubMed/NCBI
|
|
5
|
Hirai K, Yokoyama M, Asano G and Tanaka S:
Expression of cathepsin B and cystatin-C in human colorectal
cancer. Human Pathol. 30:680–686. 1999. View Article : Google Scholar
|
|
6
|
Saleh Y, Sebzda T, Warwas M, Kopec W,
Ziólkowska J and Siewinski M: Expression of cystatin c in human
colorectal cancer tissues. J Exp Ther Oncol. 5:49–53.
2005.PubMed/NCBI
|
|
7
|
Zeng Q, Zhao Y, Yang Y, Zheng G, Wang G,
Zhang P, Cui Y, Su S and Li K: Expression of cystatin C in human
esophageal cancer. Tumori. 97:203–210. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jiborn T, Abrahamson M, Gadaleanu V,
Lundwall A and Bjartell A: Aberrant expression of cystatin C in
prostate cancer is associated with neuroendocrine differentiation.
BJU Int. 98:186–196. 2006. View Article : Google Scholar
|
|
9
|
Yano M, Hirai K, Naito Z, Yokoyama M,
Ishiwata T, Shiraki Y, Inokuchi M and Asano G: Expression of
cathepsin B and cystatin C in human breast cancer. Surg Today.
31:385–389. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sloane BF: Cathepsin B and cystatins:
Evidence for a role in cancer progression. Cancer Biol. 1:137–152.
1990.
|
|
11
|
Utsunomiya T, Hara Y, Kataoka A, Morita M,
Arakawa H, Mori M and Nishiyama S: Cystatin-like
metastasis-associated protein mRNA expression in human colorectal
cancer is associated with both liver metastasis and patient
survival. Clin Cancer Res. 8:2591–2594. 2002.PubMed/NCBI
|
|
12
|
Kuopio T, Kankaanranta A, Jalava P,
Kronqvist P, Kotkansalo T, Weber E and Collan Y: Cysteine
proteinase inhibitor cystatin A in breast cancer. Cancer Res.
58:432–436. 1998.PubMed/NCBI
|
|
13
|
Leto G, Tuminello FM, Pizzolanti G,
Montallo G, Soresi M and Gebbia N: Lysosomal cathepsins B and L and
stefin A blood levels in patients with hepatocellular carcinoma
and/or liver cirrhosis: Potential clinical implications. Oncology.
54:79–83. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kos J, Stabuc B, Schweiger A, Krasovec M,
Cimerman N, Kopitar-Jerala N and Vrhovec I: Cathepsin B, H, L and
their inhibitors stefin A and cystatin-C in sera of melanoma
patients. Clin Cancer Res. 3:1815–1822. 1997.PubMed/NCBI
|
|
15
|
Kos J, Krasovec M, Cimerman N, Nielsen HJ,
Christensen IJ and Brunner N: Custeine proteinase inhibitors
stefin-A, stefin-B, and cystatin-C in sera from patients with
colorectal cancer: Relation to prognosis. Clin Cancer Res.
6:505–511. 2000.PubMed/NCBI
|
|
16
|
Ohara G, Miyazaki K, Kurishima K,
Kagohashi K, Ishikawa H, Satoh H and Hizawa N: Serum levels of
cystatin-C in elderly lung cancer patients. Oncol Lett. 3:303–306.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Decock J, Obermajer N, Vozelj S, Hendricks
W, Paridaens R and Kos J: Cathepsin B, cathepsin H, cathepsin X and
cystatin C in sera of patients with early-stage and inflammatory
breast cancer. Int J Biol Markers. 23:161–168. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rha SY, Yang WI, Gong SJ, Kim JJ, Yoo NC,
Roh JK, Min JS, Lee KS, Kim BS and Chung HC: Correlation of tissue
and blood plasminogen activation system in breast cancer. Cancer
Lett. 150:137–145. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hwang SJ, Yang Q, Meigs JB, Pearce EN and
Fox CS: A genome-wide association for kidney function and
endocrine-related traits in the NHLBI's Framingham Heart Study. BMC
Med Genet. 8 Suppl 1:S102007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Finney H, Bates CJ and Price CP: Plasma
cystatin C determinations in healthy elderly population. Arch
Gerontol Geriatr. 29:75–94. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Norlund L, Grubb A, Fex G, Leksell H,
Nilsson JE, Schenck H and Hultberg B: The increase of plasma
homocysteine concentrations with age is partly due to the
deterioration of renal f unction as determined by plasma cystatin
C. Clin Chem Lab Med. 36:175–178. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Stabuc B, Vrhovec L, Stabuc-Silih M and
Cizej TE: Improved prediction of decreased creatinine clearance by
serum cystatin C: Use in cancer patients before and during
chemotherapy. Clin Chemis. 46:193–197. 2000.
|
|
23
|
Kume M, Yasui H, Yoshikawa Y, Horinouchi
M, Higashiguchi K, Kobayashi Y, Kuroda D, Hirano T, Hirai M and
Nakamura T: Transient elevation of serum cystatin C concentrations
during perioperative cisplatin-based chemotherapy in esophageal
cancer patients. Cancer Chemother Pharmacol. 69:1537–1544. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Laurent-Matha V, Huesgen PF, Masson O,
Derocq D, Prébois C, Gary-Bobo M, Lecaille F, Rebiére B, Meurice G,
Oréar C, et al: Proteolysis of cystatin-C by cathepsin D in the
breast cancer microenvironment. FASEB J. 26:5172–5181. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nishikawa H, Ozaki Y, Nakanishi T,
Blomgren K, Tada T, Arakawa A and Suzumori K: The role of cathepsin
B and cystatin C in the mechanisms of invasion by ovarian cancer.
Gynecol Oncol. 92:881–886. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wegiel B, Jiborn T, Abrahamson M,
Helczynski L, Otterbein L, Persson JL and Bjartell A: Cystatin C is
downregulated in prostate cancer and modulates invasion of prostate
cancer cells vis MAPK/Erk and androgen receptor pathways. PLos One.
4:e79532009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sokol JP and Schiemann WP: Cystatin C
antagonizes transforming growth factor beta signaling in normal and
cancer cells. Mol Cancer Res. 2:183–195. 2004.PubMed/NCBI
|
|
28
|
Tian M and Schiemann WP: Preclinical
efficacy of cystatin C to target the oncogenic activity of
transforming growth factor Beta in breast cancer. Transl Oncol.
2:174–183. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Vigneswaran N, Wu J, Muller S, Zacharias
W, Narendran S and Middleton L: Expression analysis of cystatin C
and M in laser-capture microdissectioned human breast cancer
cells-a preliminary study. Pathol Res Pract. 200:753–762. 2005.
View Article : Google Scholar : PubMed/NCBI
|