Introduction
Chronic lymphocytic leukemia (CLL) is the most
common type of leukemia in adults and the median age of diagnosis
is 70 years (1). The clinical course
and response to treatment for CLL is heterogeneous; a patient with
an indolent form of CLL (stages 0–II) may survive for years without
treatment, while an aggressive form of CLL (stages III–IV) may be
fatal within a short time period (2). The indications for treatment initiation
include disease-associated symptoms, including fatigue, night
sweats and fever without infection, in addition to threatened-organ
function, progressive bulky disease, progressive anemia and
progressive thrombocytopenia (3).
Only progressive CLL requires treatment (4). Certain gene mutations, including Notch
homolog 1, translocation-associated (Drosophila) (NOTCH1)
and splicing factor 3 subunit B1 (SF3B1) mutations are known
biomarkers for CLL prognosis (4).
The first comprehensive analysis of CLL using
whole-genome sequencing revealed that NOTCH1 and myeloid
differentiation primary response 88 (MYD88) somatic mutations
potentially affect gene function (5). The NOTCH1 gene encodes a trans membrane
protein that is involved in the growth, differentiation and
self-renewal of cells. In addition, NOTCH1 maintains stem cells and
regulates apoptosis in numerous tissues during normal embryonic and
postnatal development (4). The NOTCH
receptors, including NOTCH1, NOTCH2, NOTCH3, NOTCH4, are a family
of membrane proteins expressed by various tissue cells that serve
as cell surface receptors and transcription regulators (6).
The NOTCH signaling pathway in CLL cells serves a
role in survival and resistance to apoptosis (4). The most common mutation of NOTCH1 is
C.7544-7545delCT, which accounts for ~80% of all NOTCH1 mutations
(4). This mutation is identified in
~10% of patients with CLL during diagnosis (7). This mutation frequently occurs in
patients without immunoglobulin heavy-chain variable region (IGHV)
mutations and with trisomy (8). The
C.7544-7545delCT NOTCH1 mutation is a 2-bp frame shift deletion
within exon 34 that produces a premature stop codon in the PEST
domain, a peptide sequence rich in proline, glutamic acid, serine
and threonine, which acts as a signal for protein degradation and
typically limits the intensity and duration of NOTCH1 signaling
(8). The presence of this mutation
has been associated with an intermediate risk of CLL and
transformation to high grade lymphoma (8).
The splicing of mRNA is catalyzed by the
spliceosome, which includes a set of small ribonucleoproteins,
including U1, U2, U4, U5 and U6, in addition to multiple splicing
factors (9). The SF3B1, a central
component of the U2 spliceosome, serves an important role in the
excision of pre-mRNA introns and the production of mature mRNA.
Mutations that inactivate the SF3B1gene result in defective
splicing of various mRNAs and defective protein synthesis (4). Mutations of SF3B1 have been identified
in 10–14% of patients with CLL, particularly in patients without
IGHV mutation. The presence of SF3B1 mutations in CLL is associated
with lower overall survival rates (8). Furthermore, higher rates of SF3B1
mutation have been revealed in patients with chemo-refractory CLL
(8).
Murine double minute 2 (MDM2) protein is a negative
regulator of the tumor suppressor gene p53, by binding to it and
inhibiting its transactivation (10). The human MDM2gene is located on
chromosome 12q14.3-q15.1. This gene has two promoters; P1, a
constitutive promoter, and P2, an alternative promoter (11). The polymorphism of del1518
(rs3730485), which is a 40-bp insertion/deletion (Ins/Del) in the
MDM2 promoter P1 region, affects promoter activity (11).
Myeloid differentiation primary response 88 (MYD88)
is a critical adaptor molecule of toll-like receptors and
interleukine-1 receptors. This adaptor molecule induces the
secretion of 5- to 150-fold higher levels of interleukin-1 receptor
antagonist, interleukin-6 and chemokine (C-C motif) ligands 2, 3
and 4, which has been observed in 3–8% of patients with CLL
(5,8). The MYD88 c.794T>C gene mutation
leads to the replacement of leucine by proline (L265P) (12). In CLL, this mutation results in
constitutive MYD88-interleukin-1 receptor associated kinase
signaling even in the absence of ligand-receptor binding and leads
to constitutive nuclear factor-κB activity. The MYD88 L265P
mutation has been exclusively identified in CLL with mutated IGHV,
which supports the hypothesis that the gene is a novel
proto-oncogene (5).
The aim of the present study was to detect the
frequency of NOTCH1 (c.7544_7545 del CT), SF3B1 (c.2098A>G),
MDM2 (40-bp Ins/Del) and MYD88 (L265P) mutations in patients with
CLL from a population of Western Iran compared with healthy
individuals. In addition, the current study aimed to identify the
association of these mutations with the disease stage.
Materials and methods
Sample collection
This case-control study involved 100 patients with
CLL (67 males and 33 females) with a mean age of 61.6±11.1 years
and 105 healthy controls (75 males and 30 females) with a mean age
of 56.6±7.5 years, who were enrolled at Kermanshah University of
Medical Sciences (Kermanshah, Iran). Samples were collected from
February 2017 to July 2017. The inclusion criteria included the
availability of biological samples and patients of Kurdish
ethnicity. The demographic, hematologic, clinical and
histopathological parameters of the patients were collected from
their medical records. The ethnic background of all patients and
controls was Kurdish.
All individuals agreed to participate in the study
and informed written consent was obtained from each individual for
use of their blood specimens, in accordance with the principles of
the Helsinki II declaration. All methods and the examination of
blood samples were carried out in accordance with the approved
guidelines.
Genotyping
Genomic DNA was extracted from EDTA-treated whole
blood by using the phenol-chloroform method, as described
previously (13).
NOTCH1 genotyping
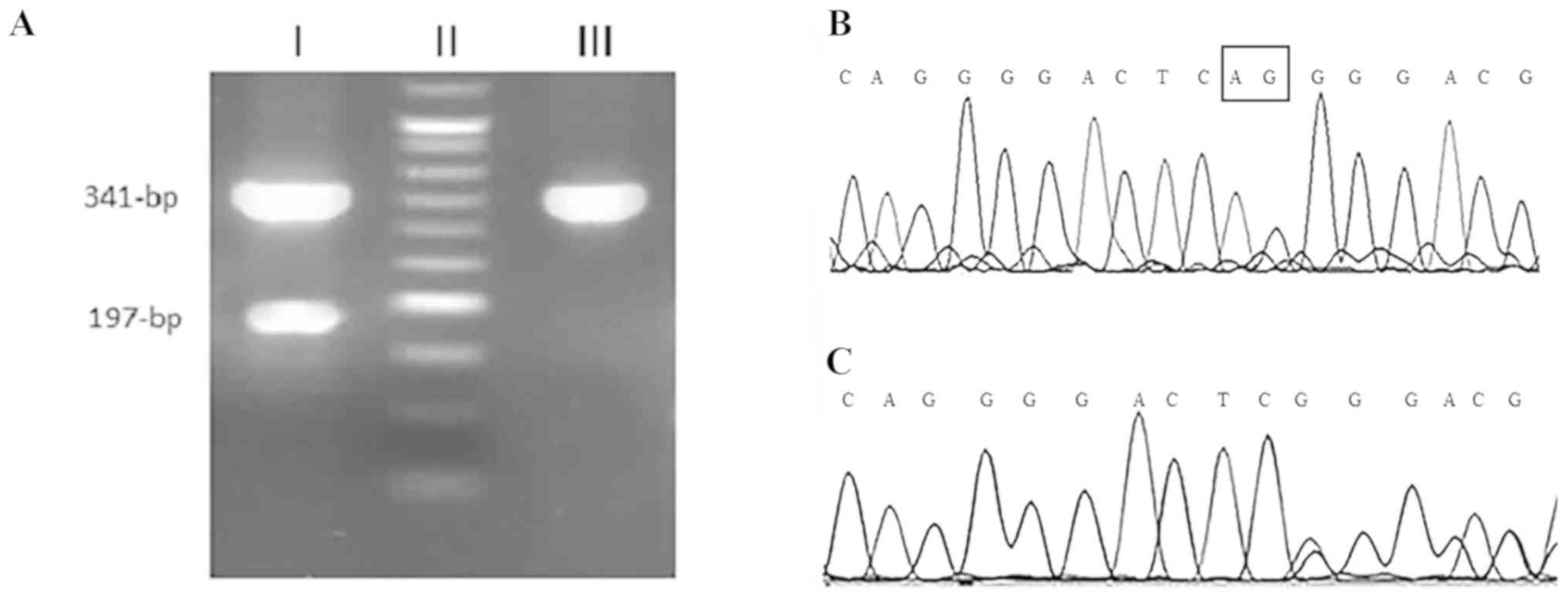
The detection of the 2-bp deletion in NOTCH1
(c.7544_7545delCT) was performed using an allele
specific-polymerase chain reaction (AS-PCR) method. Using two
external primers as the internal PCR control, a fragment with
341-bp was amplified for both wild and mutant alleles. The PCR
reaction was performed with a total volume of 25 µl containing 100
ng of genomic DNA, 1X PCR buffer, 200 nM of each dNTP, 1.75 nM
MgCl2, 1unit of Taq DNA polymerase (SinaClon Bioscience
Co., Karaj, Iran), and 200 nM each of the forward, reverse and
deletion detection primers (Table
I). The PCR thermocycling conditions were as follows: Initial
denaturation at 94°C for 5 min; 35 cycles of 94°C for 30 sec, 60°C
for 30 sec, 72°C for 30 sec; and a final elongation at 72°C for 7
min. The PCR products were visualized by electrophoresis on a 2.5%
agarose gel with the GelRed stain (Kawsar Biotech Co., Tehran,
Iran). A third primer was specific for detecting a 2-bp deletion
and only amplified the mutant allele with 197-bp (7). The internal primers amplified a 341-bp
fragment from both mutant and wild-type alleles, while the deletion
detection primer produced a 197-bpfragment only in cases with
mutated allele. The presence of NOTCH1 mutation was confirmed by
genomic DNA sequencing (Fig. 1).
 | Table I.Primer sequences used for genotyping
of NOTCH1 and SF3B1 genes. |
Table I.
Primer sequences used for genotyping
of NOTCH1 and SF3B1 genes.
| Mutation | Gene | Primer sequence
(5′-3′) | Product size,
bp | Detection
method |
|---|
|
c.7544_7545delCT | NOTCH1 | Forward primer:
CACACTATTCTGCCCCAGGA | 341 | AS-PCR |
|
|
| Reverse primer:
AAAGGAAGCCGGGGTCTC | 197 |
|
|
|
| Deletion detection
primer: ACTGGTCAGGGGACTCGG |
|
|
| rs559063155 | SF3B1 |
Finternal:
GATGTGTTGAACTGCACCCTT | 92 | AS-PCR |
|
|
|
Rinternal:
CAGGCCCATACTAACTGTCC |
|
|
|
|
| Ft:
AGCACTGATGGTCCGAACTGT |
|
|
|
|
| Fc:
AGCACTGATGGTCCGAACTGC |
|
|
|
|
| Rcommon:
GACAGGCTATGGTTCATGTT | 199 |
|
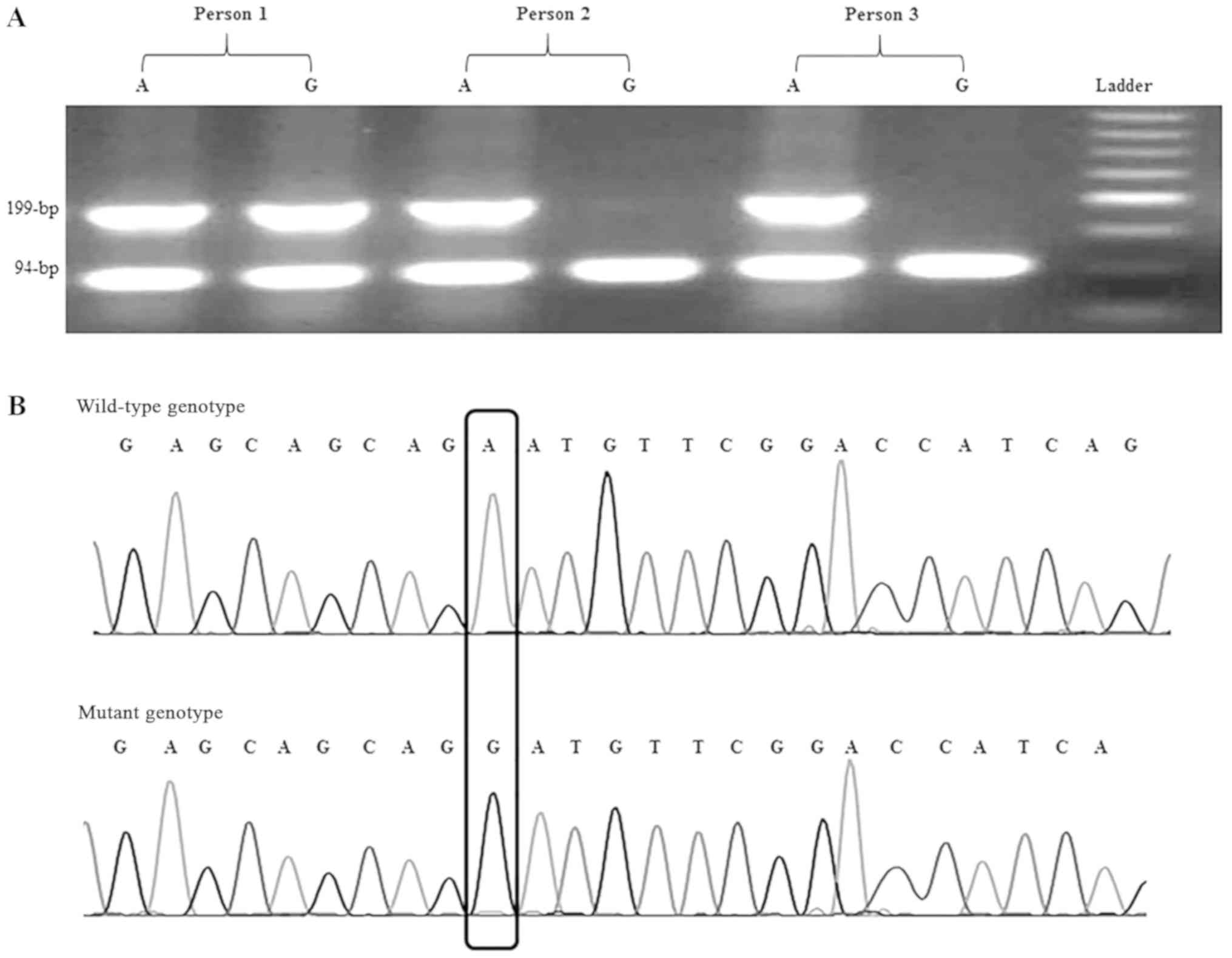
SF3B1 genotyping
The SF3B1c.2098A>G polymorphism was recognized
using a designed AS-PCR method. Five primers were designed; two
primers were used as the internal PCR control that amplified a
94-bpproduct and three primers, including Rcommon, Ft
(for detection of the ‘T’ allele) and Fc (for detection of the ‘C’
allele), amplified the 199-bp product (Fig. 2). The primer sequences are presented
in Table I. PCR reaction was carried
out with a total volume of 25 µl containing 100 ng of genomic DNA,
1X PCR buffer, 200 nM of each dNTPs, 1.75 nM MgCl2, 1
unit of Taq DNA polymerase (SinaClon Bioscience Co.), 200 nM of
each of the internal forward and reverse primers, and 400 nM of
Rcommon, Ft or Fc primers. The PCR cycling conditions
were as follows: initial denaturation at 94°C for 5 min; 35 cycles
of 94°C for 30 sec, 58°C for 30 sec, 72°C for 30 sec; and a final
elongation at 72°C for 7 min. The PCR products were visualized by
electrophoresis on a 2% agarose gel with the GelRed stain (Kawsar
Biotech Co.).
Validation of AS-PCR products of
NOTCH1 and SF3B1 genes by Sanger sequencing
To verify the obtained genotypes, Sanger sequencing
was employed as a reference method. For this purpose, certain
samples from each genotype were amplified as aforementioned and
subjected to sequencing. The results of Sanger sequencing were
detected using Chromas software 2.1 (Technelysium Pty. Ltd,
Helensvale, Queensland, Australia).
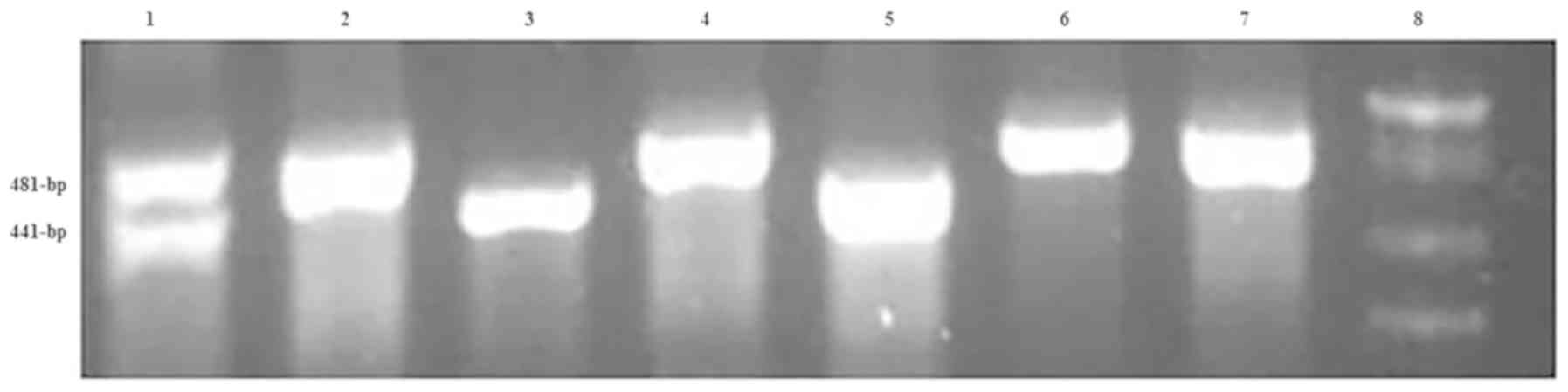
MDM2 genotyping
The MDM2 40-bp Ins/Del was amplified using Taq DNA
polymerase (SinaClon Bioscience Co.) and detected with the
following primers: MDM2 forward, 5′-GTGCGCAGCCTATCACTTATC-3′ and
reverse, 5′-ACTCACCTACTTTCCCACAGA-3′. The thermocycling conditions
were as follows: Initial denaturation at 94°C for 5 min; 35 cycles
of 94°C for 30 sec, 58°C for 30 sec, 72°C for 30 sec; and a final
elongation at 72°C for 10 min. The PCR products were visualized by
electrophoresis on a 2.5% agarose gel with GelRed stain (Kawsar
Biotech Co.). The PCR product of the insertion allele was a 481-bp
fragment, while in the presence of the deletion allele, the PCR
product was a 441-bp fragment (Fig.
3).
MYD88 genotyping
The MYD88 L265P mutation was amplified using Taq DNA
polymerase (SinaClon Bioscience Co.) and detected with the
following primers: MYD88 forward, 5′-CTGGCAAGAGAATGAGGGAATGT-3′ and
reverse, 5′-AGGAGGCAGGGCA-3′. The thermocycling conditions were the
same those used for MDM2 detection, except the annealing
temperature was 56°C for 30 sec. The PCR products were visualized
by electrophoresis on a 2% agarose gel with GelRed stain (Kawsar
Biotech Co.). The 489-bp fragment PCR product was digested with the
restriction enzyme BsiEI. In the presence of wild type
allele, the PCR product remained intact, while the mutated allele
was digested into 200-bp and 289-bp fragments (14).
Statistical analysis
The allelic frequencies were calculated using the
chromosome counting method (15).
The frequencies of genotypes and alleles in patients were compared
with controls using a chi-square test. Odds ratio (OR) values were
calculated as estimates of relative risk for disease and 95%
confidence intervals (CIs) were obtained. All statistical analysis
was performed using SPSS 22.0 software (IBM Corp., Armonk, NY,
USA). P<0.05 was considered to indicate a statistically
significant difference.
Results
Characteristics of patients
Table II presents
the hematological and clinicopathological characteristics of the
patients with CLL. The disease stages of 86 patients were available
and according to the Rai classification (16) these stages were as follows: 25
patients (29.1%) with stage 0; 15 patients (17.4%) with stage I; 8
patients with stage II (9.3%); 21 patients (24.4%) with stage III;
and 17 patients (19.8%) with stage IV.
| Table II.Characteristics of patients with
CLL. |
Table II.
Characteristics of patients with
CLL.
|
Characteristics | Mean ± standard
deviation (range) | n (%) |
|---|
| Sex |
|
|
|
Male |
| 67 (67.0) |
|
Female |
| 33 (33.0) |
| Age, years | 61.6±11.1
(31–84) |
|
| Duration of CLL,
months | 55.8±34.8
(1–144) |
|
| WBC,
count/mm3 | 43.8±42.5
(2–236) |
|
| Platelet,
count/mm3 | 173.5±69.9
(60–477) |
|
| Hb, g/dl | 12.5±2.1
(7–17) |
|
| LDH, IU/l | 383.3±152.9
(50–980) |
|
| Stage |
|
|
| 0 |
| 25 (29.1) |
| I |
| 15 (17.4) |
| II |
| 8 (9.3) |
|
III |
| 21 (24.4) |
| IV |
| 17 (19.8) |
NOTCH1 mutation
Table III presents
the frequencies of the NOTCH1, SF3B1, MDM2 and MYD88 mutations
among the patients with CLL and the healthy individuals. As
indicated in Table III, the NOTCH1
mutation was detected in 10% of patients (8 males and 2 females).
However, this mutation was not identified in healthy controls.
Table IV presents the distribution
of the NOTCH1 mutation according to the disease stage. A
significantly higher percentage of NOTCH1 mutation was identified
in patients with stage III CLL (high risk; 62.5%) compared with
stages 0–II (very low to moderate risk; 37.5%), with a 4.69-fold
increase (95% CI, 1.0–21.9; P=0.049; Table IV). The disease stage of two
patients with NOTCH1 mutation was not available from the patient's
records.
| Table III.Frequency of NOTCH1, SF3B1, MDM2 and
MYD88 mutations in patients with CLL and controls. |
Table III.
Frequency of NOTCH1, SF3B1, MDM2 and
MYD88 mutations in patients with CLL and controls.
| Mutation | Patients with CLL,
n (%) | Controls, n
(%) | χ2
(P-value) | OR (95%CI),
P-value |
|---|
| NOTCH1 |
|
|
|
|
|
Wild-type | 90 (90.0) | 100 (100.0) |
|
|
|
Mutant | 10 (10.0) | 0 (0.0) | 11.04 (0.001) |
|
| SF3B1 |
|
|
|
|
|
Wild-type | 88 (88.0) | 103 (98.1) | 8.2 (0.004) | 7.02 (1.53–32.23),
0.012 |
|
Mutant | 12 (12.0) | 2
(1.9) |
|
|
| MDM2 mutation |
|
|
|
|
|
Ins/Ins | 52 (52.5) | 51 (51.5) |
|
|
|
Ins/Del | 39 (39.4) | 34 (34.3) | 0.15 (0.70) |
|
|
Del/Del | 8 (8.1) | 14 (14.1) | 1.45 (0.22) |
|
| MYD88 |
|
|
|
|
| TT
(wild-type) | 100 (100.0) | 105 (100.0) |
|
|
| TC | 0 (0.0) | 0 (0.0) |
|
|
| CC | 0 (0.0) | 0 (0.0) |
|
|
| Table IV.Distribution of NOTCH1 mutation
according to the disease stage. |
Table IV.
Distribution of NOTCH1 mutation
according to the disease stage.
|
| NOTCH1 |
|
|
|---|
|
|
|
|
|
|---|
| Stage | Wild-type, n
(%) | Mutant, n (%) | χ2
(P-value) | OR (95% CI),
P-value |
|---|
| Very low to
moderate risk (stages 0–II) | 45 (57.7) | 3 (37.5) |
|
|
| High risk (stage
III) | 16 (20.5) | 5 (62.5) | 4.39 (0.036) | 4.69 (1.0–21.9),
0.049 |
| Very high risk
(stage IV) | 17 (21.8) | 0 (0.0) | 1.11 (0.29) |
|
SF3B1 mutation
The SF3B1 mutation was observed in 12 patients (12%;
9 males and 3 females) and in 2 controls (1.9%; both male), which
indicates a significant difference (P=0.012; Table III). No significant difference was
identified in the frequency of SF3B1 mutation according to the
disease stage.
A total of 3 patients with stage II or III CLL were
identified to exhibit both the NOTCH1 and SF3B1 mutations. In these
patients, the wild-type genotype of MDM2 insertion/insertion (II)
was observed.
MDM2 insertion/deletion mutation
The MDM2 insertion/deletion (ID) genotype was
detected in 39.4% of patients and 34.3% of controls (P=0.70). The
MDM2 deletion/deletion (DD) genotype was identified in 8.1% of
patients and 14.1% of controls (P=0.22; Table III). The various genotypes of MDM2
were not associated with the disease stage. Four patients who
possessed the NOTCH1 mutation and MDM2 II or MDM2 ID had stage III
CLL, and two patients with the NOTCH1 mutation and MDM2 II or MDM2
ID had stage 0 CLL. In addition, 6 patients were identified to
exhibit the SF3B1 mutation and MDM2 ID, however these patients had
various stages of CLL. This suggests the concomitant presence of
NOTCH1 and MDM2 mutations or the combined presence of SF3B1 and
MDM2 mutations does not have an influence on the disease stage. The
MYD88 L265P mutation was not detected in the patients or the
controls.
Discussion
Associations have been reported between the presence
of NOTCH1mutations and poor survival, resistance to treatment and
disease progression in aggressive clinical phases of CLL (4). The predominant NOTCH1 mutation, a frame
shift mutation, results in enhanced stability of NOTCH1 protein and
the accumulation of an active isoform of NOTCH1 (4). The NOTCH1 C.7544-7545delCT is the most
common mutation that occurs in ~80% of CLL cases (4). The present study detected the NOTCH1
C.7544-7545 delCT mutation in 10% of patients with CLL, which is in
agreement with a previous study that also reported the presence of
this mutation in ~10% of patients with CLL (7). In addition, Fabbri et al
(17) have reported the presence of
this mutation in 8.3% of patients with CLL. Furthermore, in the
current study, the presence of this mutation was associated with a
4.39-fold risk of stage III CLL. The presence of NOTCH1 mutation
has previously been reported in patients with CLL with
intermediate-risk (8).
The NOTCH1 C.7544-7545 delCT mutation results in the
removal of the C-terminal PEST domain which is associated with an
accumulation of constitutively active NOTCH1 protein and the
constitutive activation of NOTCH1 signaling, which contributes to
apoptosis resistance and increased survival of CLL cells (5,18). This
suggests that the NOTCH1 delCT mutation and the activation of NOTCH
signaling is associated with the pathogenesis of the severe
clinical form of CLL, however this needs to be confirmed by further
studies. Among patients with CLL, a significantly shorter survival
time has been revealed in patients with the NOTCH1 delCT mutation
compared with patients without this mutation (7,19). All
the patients involved in our study were alive at the end of the
study but due to the low number of individuals and the low median
duration of the disease (55.8 months), a comparison between the
survival of patients with and without NOTCH1 mutation was not
possible.
The current study detected the SF3B1 mutation in 12%
of patients and 1.9% of controls. An association was not identified
between this mutation and the stage of CLL. Mutations that
inactivate the SF3B1 gene result in defective splicing of various
mRNAs and subsequent defective protein synthesis (4). In a cohort of patients with CLL from
the phase 3 United Kingdom Leukaemia Research Fund Chronic
Lymphocytic Leukemia 4 trial, NOTCH1 and SF3B1 mutations were
revealed in 10 and 17% of patients, respectively (20). In this trial, NOTCH1 mutations were
associated with reduced overall and progression-free survival time.
In addition, SF3B1mutations were associated with reduced overall
survival time. Two initial studies that reported the association of
CLL with mutated SF3B were conducted using case cohorts.
Wang et al (21) and Queseda
et al (22) revealed that the
SF3B1 mutation was associated with poor clinical outcome. Both
studies reported that the SF3B1 mutation provided prognostic
information independent from other known CLL prognostic markers.
Additionally, Te Raa et al (23) proposed an explanation for the poor
prognosis associated with SF3B1 mutations. The current study
identified that 3 out of the 10 patients (30%) with both NOTCH1 and
SF3B1 mutations had stage II or III CLL. However, a study by Sutton
et al demonstrated that only 1 patient out of 106 possessed
both mutations (24).
In the present study, the polymorphism of MDM2 40-bp
Ins/Del was not associated with CLL risk and disease stage. In a
study among an Iranian population, the MDM2 40-bp Del mutation was
identified to increase the risk of breast cancer (25). However, a recent meta-analysis did
not reveal a significant association between the MDM2 40-bp Ins/Del
polymorphism and overall cancer risk (11).
In the current study, the MYD88 L265P mutation was
not detected in all studied individuals. The MYD88 L265P mutation
has been demonstrated to be strongly associated with lymphoblastic
lymphoma (26). However, this
mutation was identified in only 2% of patients with CLL in a study
based in Mexico (26). In another
study, the absence of MYD88 mutation was detected in a large cohort
of patients with CLL (24). It has
been indicated that the MYD88 mutation occurs exclusively in
mutated IGHV genes, but not in unmutated IGHV genes (5,24,27–29).
Therefore, it may be that the patients in the current study
predominantly possessed unmutated IGHV genes. The high frequency of
patients with NOTCH1 mutation in the present study supports this
hypothesis, as the NOTCH1 mutation is mostly detected in patients
with unmutated IGHV genes (5).
In summary, the current study established the
frequency of NOTCH1, SF3B1, MDM2 and MYD88 mutations in patients
from Western Iran with CLL. A high frequency of NOTCH1 delCT and
SF3B1 mutations among patients with CLL were reported. In addition,
the present study identified an association between NOTCH1 mutation
and aggressive clinical stages of CLL. However, the low sample size
is a limitation of the study that may affect the association
between the combined presence of two or three mutations and CLL
stage. Detection of the NOTCH1 mutation as a biomarker for the
incidence and severity of CLL may improve patient management and
treatment.
Acknowledgements
Not applicable.
Funding
The study was supported by the National Institute
for Medical Research Development (grant no. 943793).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
ZoR designed the study, wrote the manuscript and
approved the final version to be published. MA collected the
samples and interpreted the results. YM, ZA, ZH, ZiR and MAK
collected the samples and performed experiments. MM, FB and KY
performed the experiments. All authors have reviewed the final
version of the manuscript and approved it for publication.
Ethical approval and consent to
participate
The study was approved by the Ethics Committee of
Kermanshah University of Medical Sciences (Kermanshah, Iran). All
individuals agreed to participate in the study and informed written
consent was obtained from each individual for use of their blood
specimens, in accordance with the principles of the Helsinki II
declaration.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Parikh SA, Rabe KG, Kay NE, Call TG, Ding
W, Schwager SM, Bowen DA, Conte M, Jelinek DF, Slager SL and
Shanafelt TD: Chronic lymphocytic leukemia in young (≤55 years)
patients: A comprehensive analysis of prognostic factors and
outcomes. Haematologica. 99:140–147. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shanafelt TD, Rabe KG, Kay NE, Zent CS,
Jelinek DF, Reinalda MS, Schwager SM, Bowen DA, Slager SL, Hanson
CA and Call TG: Age at diagnosis and the utility of prognostic
testing in patients with chronic lymphocytic leukemia. Cancer.
116:4777–4787. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ghia P and Hallek M: Management of chronic
lymphocytic leukemia. Haematologica. 99:965–972. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shahjahani M, Mohammadiasl J, Noroozi F,
Seghatoleslami M, Shahrabi S, Saba F and Saki N: Molecular basis of
chronic lymphocytic leukemia diagnosis and prognosis. Cell Oncol
(Dordr). 38:93–109. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Puente XS, Pinyol M, Quesada V, Conde L,
Ordóñez GR, Villamor N, Escaramis G, Jares P, Beà S, González-Díaz
M, et al: Whole-genome sequencing identifies recurrent mutations in
chronic lymphocytic leukaemia. Nature. 475:101–105. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gianfelici V: Activation of the NOTCH1
pathway in chronic lymphocytic leukemia. Haematologica. 97:328–330.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sportoletti P, Baldoni S, Del Papa B,
Aureli P, Dorillo E, Ruggeri L, Plebani S, Amico V, Di Tommaso A,
Rosati E, et al: A revised NOTCH1 mutation frequency still impacts
survival while the allele burden predicts early progression in
chronic lymphocytic leukemia. Leukemia. 28:436–439. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Landau DA and Wu CJ: Chronic lymphocytic
leukemia: Molecular heterogeneity revealed by high-throughput
genomics. Genome Med. 5:472013. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wan Y and Wu CJ: SF3B1 mutations in
chronic lymphocytic leukemia. Blood. 121:4627–4634. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dong HJ, Fang C, Fan L, Zhu DX, Wang DM,
Zhu HY, Zhuang Y, Miao KR, Liu P, Xu W and Li JY: MDM2 promoter
SNP309 is associated with an increased susceptibility to chronic
lymphocytic leukemia and correlates with MDM2 mRNA expression in
Chinese patients with CLL. Int J Cancer. 130:2054–2061. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hua W, Zhang A, Duan P, Zhu J, Zhao Y, He
J and Zhang Z: MDM2 promoter del1518 polymorphism and cancer risk:
Evidence from 22,931 subjects. Onco Targets Ther. 10:3773–3780.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang CZ, Lin J, Qian J, Shao R, Xue D,
Qian W, Xiao GF, Deng ZQ, Yang J, Li Y and Chen XX: Development of
high-resolution melting analysis for the detection of the MYD88
L265P mutation. Clin Biochem. 46:385–387. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rahimi Z, Vaisi-Raygani A, Mozafari H,
Kharrazi H, Rezaei M and Nagel RL: Prevalence of factor V Leiden
(G1691A) and prothrombin (G20210A) among Kurdish population from
Western Iran. J Thromb Thrombolysis. 25:280–283. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Argentou N, Vassilopoulos G, Ioannou M,
Germenis A and Speletas M: Rapid detection of MYD88-L265P mutation
by PCR-RFLP in B-cell lymphoproliferative disorders. Leukemia.
28:447–449. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jafari Y, Rahimi Z, Vaisi-Raygani A and
Rezaei M: Interaction of eNOS polymorphism with MTHFR variants
increase the risk of diabetic nephropathy and its progression in
type 2 diabetes mellitus patients. Mol Cell Biochem. 353:23–34.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li PP, Feng LL, Chen N, Ge XL, Lv X, Lu K,
Ding M, Yuan D and Wang X: Metadherin contributes to the
pathogenesis of chronic lymphocytic leukemia partially through
Wnt/β-catenin pathway. Med Oncol. 32:4792015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fabbri G, Rasi S, Rossi D, Trifonov V,
Khiabanian H, Ma J, Grunn A, Fangazio M, Capello D, Monti S, et al:
Analysis of the chronic lymphocytic leukemia coding genome: Role of
NOTCH1 mutational activation. J Exp Med. 208:1389–1401. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bilous NI, Abramenko IV, Chumak AA, Dyagil
IS and Martіna ZV: Detection of NOTCH1 c.7541_7542delCT mutation in
chronic lymphocytic leukemia using conventional and real-time
polymerase chain reaction. Exp Oncol. 38:112–116. 2016.PubMed/NCBI
|
|
19
|
Dal Bo M, Pozzo F, Bomben R, Degan M,
Marconi D, Zucchetto A, Rossi D, Pozzato G, Zauli G, Gaidano G, et
al: ARHGDIA, a mutant TP53-associated Rho GDP dissociation
inhibitor, is over-expressed in gene expression profiles of TP53
disrupted chronic lymphocytic leukaemia cells. Br J Haematol.
161:596–599. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oscier DG, Rose-Zerilli MJ, Winkelmann N,
Gonzalez de Castro D, Gomez B, Forster J, Parker H, Parker A,
Gardiner A, Collins A, et al: The clinical significance of NOTCH1
and SF3B1 mutations in the UK LRF CLL4 trial. Blood. 121:468–475.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang L, Lawrence MS, Wan Y, Stojanov P,
Sougnez C, Stevenson K, Werner L, Sivachenko A, DeLuca DS, Zhang L,
et al: SF3B1 and other novel cancer genes in chronic lymphocytic
leukemia. N Engl J Med. 365:2497–2506. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Quesada V, Conde L, Villamor N, Ordóñez
GR, Jares P, Bassaganyas L, Ramsay AJ, Beà S, Pinyol M,
Martínez-Trillos A, et al: Exome sequencing identifies recurrent
mutations of the splicing factor SF3B1 gene in chronic lymphocytic
leukemia. Nat Genet. 44:47–52. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Te Raa GD, Derks IA, Navrkalova V,
Skowronska A, Moerland PD, van Laar J, Oldreive C, Monsuur H,
Trbusek M, Malcikova J, et al: The impact of SF3B1 mutations in CLL
on the DNA-damage response. Leukemia. 29:1133–1142. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sutton LA, Young E, Baliakas P,
Hadzidimitriou A, Moysiadis T, Plevova K, Rossi D, Kminkova J,
Stalika E, Pedersen LB, et al: Different spectra of recurrent gene
mutations in subsets of chronic lymphocytic leukemia harboring
stereotyped B-cell receptors. Haematologica. 101:959–967. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hashemi M, Omrani M, Eskandari-Nasab E,
Hasani SS, Mashhadi MA and Taheri M: A 40-bp insertion/deletion
polymorphism of Murine Double Minute2 (MDM2) increased the risk of
breast cancer in Zahedan, Southeast Iran. Iran Biomed J.
18:245–249. 2014.PubMed/NCBI
|
|
26
|
Insuasti-Beltran G, Gale JM, Wilson CS,
Foucar K and Czuchlewski DR: Significance of MYD88 L265P mutation
status in the subclassification of low-grade B-cell
lymphoma/leukemia. Arch Pathol Lab Med. 139:1035–1041. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Baliakas P, Hadzidimitriou A, Sutton LA,
Rossi D, Minga E, Villamor N, Larrayoz M, Kminkova J,
Agathangelidis A, Davis Z, et al: Recurrent mutations refine
prognosis in chronic lymphocytic leukemia. Leukemia. 29:329–336.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jeromin S, Weissmann S, Haferlach C,
Dicker F, Bayer K, Grossmann V, Alpermann T, Roller A, Kohlmann A,
Haferlach T, et al: SF3B1 mutations correlated to cytogenetics and
mutations in NOTCH1, FBXW7, MYD88, XPO1 and TP53 in 1160 untreated
CLL patients. Leukemia. 28:108–117. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Rossi D, Rasi S, Spina V, Bruscaggin A,
Monti S, Ciardullo C, Deambrogi C, Khiabanian H, Serra R, Bertoni
F, et al: Integrated mutational and cytogenetic analysis identifies
new prognostic subgroups in chronic lymphocytic leukemia. Blood.
121:1403–1412. 2013. View Article : Google Scholar : PubMed/NCBI
|