Introduction
As one of the most common malignant tumors in women,
ovarian cancer ranks the third in incidence rate among all
gynecologic tumors (1). The
statistical results by Oza et al (2) showed that 1.6 million patients were
newly diagnosed with ovarian cancer in 2015 globally. At present,
not only the incidence rate of ovarian cancer is on the increase
annually, but also an increasing number of young people are
susceptible to the disease (3). The
study conducted by Kuchenbaecker et al (4) indicated that ovarian cancer will be the
first among all gynecologic tumors in incidence rate by 2050.
As ovarian cancer has no significant signs in early
stage, most patients have developed mid-late stage ovarian cancer
at diagnosis, not only increasing the difficulty of treatment, but
also worsening the prognosis of patients (5). Postoperative five-year mortality rate
of patients with ovarian cancer is up to 72.8%, which is the
highest among those of gynecologic diseases, according to the
statistics by Bachmayr-Heyda et al (6). With the development of modern medical
technology, relatively stable research results in the treatment of
ovarian cancer have been achieved, and the survival rate after
surgery of patients has been on the increase year by year (7). However, the study conducted by
Lauby-Secretan et al (8)
proved that body weight is a key factor influencing the
postoperative prognosis of patients with tumors, but there has been
no report in literature on ovarian cancer so far. Therefore, by
studying the postoperative conditions of ovarian cancer patients
with different body weights, this study provides reference and
guidance for future clinical treatment of ovarian cancer.
Patients and methods
General data
A total of 362 patients who were diagnosed with
ovarian cancer by biopsy in the Department of Pathology of Shanxi
Dayi Hospital Affiliated to Shanxi Medical University (Taiyuan,
China) from April 2012 to July 2017 were selected as research
subjects and analyzed retrospectively. The patients were aged
between 35 and 55 years, with an average age of 44.78±9.17 years.
Inclusion criteria were: i) patients diagnosed with ovarian cancer
through biopsy in the Department of Pathology of Shanxi Dayi
Hospital, ii) patients aged 35–55 years, iii) patients who
underwent surgeries in the hospital after diagnosis of the disease,
iv) patients whose medical records were complete and v) patients
who co-operated with the instructions of our medical staff.
Exclusion criteria were: i) patients complicated with other
cardiovascular and cerebrovascular diseases, ii) patients
associated with other tumors, iii) patients with surgical
tolerance, iv) patients who were sensitive to drugs, v) pregnant
patients, vi) patients who had been bedridden for a long time, vii)
patients with physical disability and viii) patients who were
transferred to other hospitals halfway.
Methods
All the patients underwent ovarian tumor resections
in Shanxi Dayi Hospital Affiliated to Shanxi Medical University
after definite diagnosis and also received nursing care and
treatments in the Shanxi Dayi Hospital. According to body fat
health standard (8), the patients
were divided into the obesity group [body mass index (BMI) ≥28],
the overweight group (≥24 BMI <28), the normal body weight group
(1 ≥8.5 BMI <24) and the low body weight group (BMI <18.5).
Conditions of postoperative recovery and complications of patients
in each group during hospitalization were recorded, and the
prognosis of the patients was followed up for one year by means of
telephone, e-mail or hospital re-examination. The follow-up period
ended on May 30, 2018, and the events for termination of the
follow-up period included the death of patients or loss to follow
up, and the life conditions and survival of patients after
discharge were recorded.
The study was approved by the Ethics Committee of
Shanxi Dayi Hospital Affiliated to Shanxi Medical University.
Signed informed consents were obtained from the patients the
guardians.
Observation indexes
Clinical data, surgical time, intraoperative blood
loss amount, intraoperative blood transfusion amount, time of
postoperative passage of gas, length of stay, complications,
prognosis and survival rate were factors analyzed.
Statistical analysis
Statistical Product and Service Solutions (SPSS)
22.0 software (IBM Corp., Armonk, NY, USA) was employed for the
analysis and processing of the data, measurement data were
expressed by rate, and the comparison between two groups were
analyzed using the Chi-square test. Enumeration data were expressed
by mean ± standard deviation, and comparisons between two groups
were evaluated using the paired t-test. Comparisons among multiple
groups were conducted using analysis of variance and the LSD post
hoc test. The Kaplan-Meier method was used to calculate the
survival rate, and comparisons of survival rates were assessed by
log-rank test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Comparison of clinical data of
patients
The patients were divided into the obesity group
(n=64), the overweight group (n=124), the normal body weight group
(n=108) and the low body weight group (n=66) based on their BMI.
Age, course of illness, pathological staging and metastasis of
lymph nodes were compared among the 4 groups of patients, and no
significant differences were noted, indicating that the 4 groups
were comparable (Table I).
 | Table I.Comparison of clinical data of the 4
groups of patients. |
Table I.
Comparison of clinical data of the 4
groups of patients.
| Variables | Obesity group
(n=64) | Overweight group
(n=124) | Normal body weight
group (n=108) | Low body weight group
(n=66) | f value | P-value |
|---|
| Age (years) | 45.27±8.16 | 44.68±9.07 | 43.54±8.57 | 44.17±7.04 | 0.66 | 0.58 |
| Course of illness
(days) | 17.84±5.76 | 18.34±4.07 | 19.27±5.88 | 18.07±6.04 | 1.25 | 0.29 |
| Pathological
staging |
|
|
|
| 0.58 | 0.61 |
| Stage
I–II | 21 (32.81) | 37 (29.84) | 33 (30.56) | 23 (34.85) |
|
|
| Stage
III–IV | 43 (67.19) | 87 (70.16) | 75 (69.44) | 43 (65.15) |
|
|
| Metastasis of lymph
nodes |
|
|
|
| 0.41 | 0.69 |
| Yes | 18 (28.13) | 34 (27.42) | 29 (26.85) | 18 (26.85) |
|
|
| No | 46 (71.88) | 90 (72.58) | 79 (73.15) | 48 (73.15) |
|
|
Comparison of surgical conditions
Comparison in surgical time in the 4 groups of
patients were performed, indicating that the surgical time of the
normal body weight group was 145.37±27.68 min, which was the
shortest, and that of the the obesity group (214.33±27.84 min) was
the longest (P<0.05), followed by that of the overweight group
(184.37±29.33 min) (P<0.05). In terms of intraoperative blood
loss amount, the obesity group had the highest blood loss, up to
342.17±42.37 ml, followed by the overweight group (284.68±50.27 ml)
(P<0.05), and the normal group had the lowest blood loss
(197.64±33.84 ml) (P<0.05). Similarly, among patients in the 4
groups, the obesity group had the highest intraoperative blood
transfusion, up to 427.68±50.72 ml, followed by the overweight
group (354.73±33.86) (P<0.05), and the lowest blood transfusion
was detected in the normal group (197.64±33.84) (P<0.05)
(Table II).
| Table II.Comparison in surgical conditions
among the 4 groups of patients. |
Table II.
Comparison in surgical conditions
among the 4 groups of patients.
| Variables | Obesity group
(n=64) | Overweight group
(n=124) | Normal body weight
group (n=108) | Low body weight group
(n=66) | f value | P-value |
|---|
| Surgical time
(min) | 214.33±27.84 |
184.37±29.33a |
145.37±27.68a,b |
172.14±30.57a–c | 79.17 | <0.01 |
| Intraoperative blood
loss amount (ml) | 342.17±42.37 |
284.68±50.27a |
197.64±33.84a,b |
263.17±45.07a–c | 253.30 | <0.01 |
| Intraoperative blood
transfusion amount (ml) | 427.68±50.72 |
354.73±33.86a |
247.36±45.23a,b |
321.76±39.27a–c | 274.03 | <0.01 |
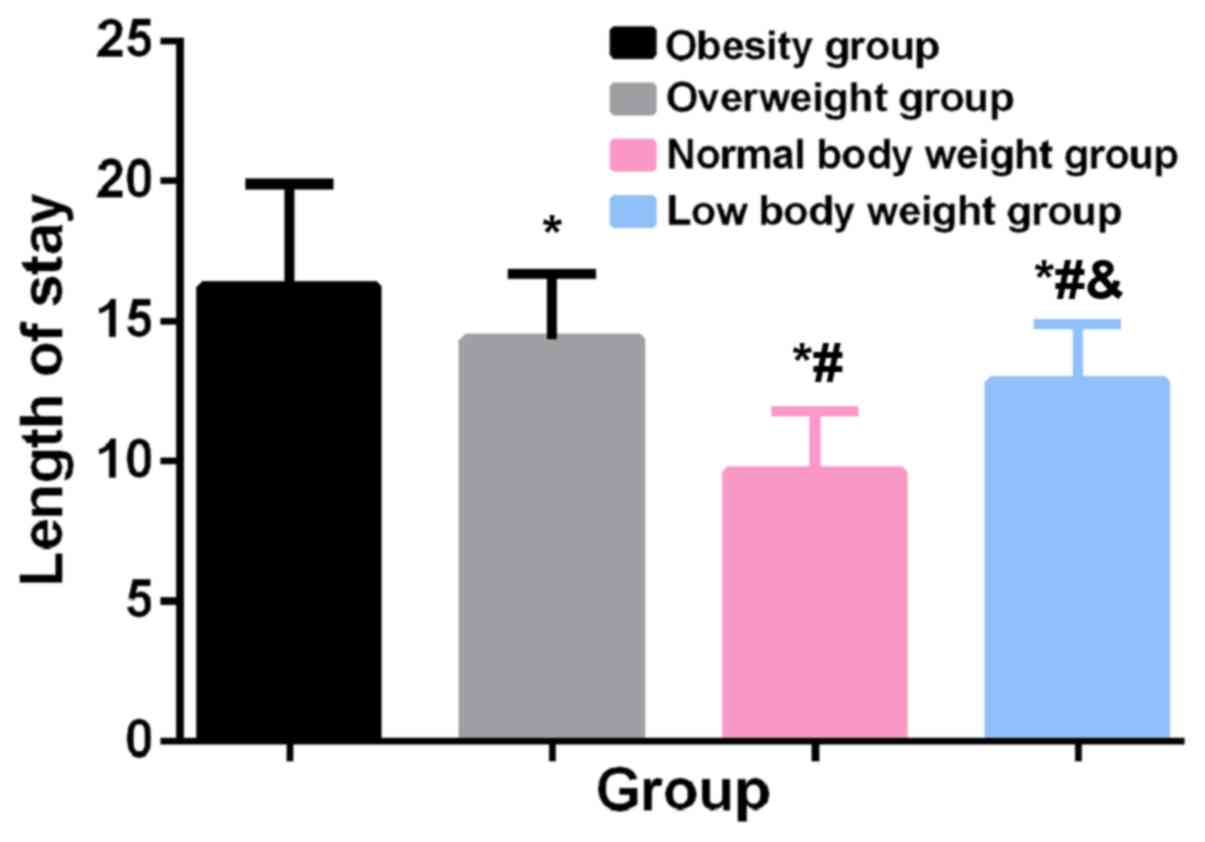
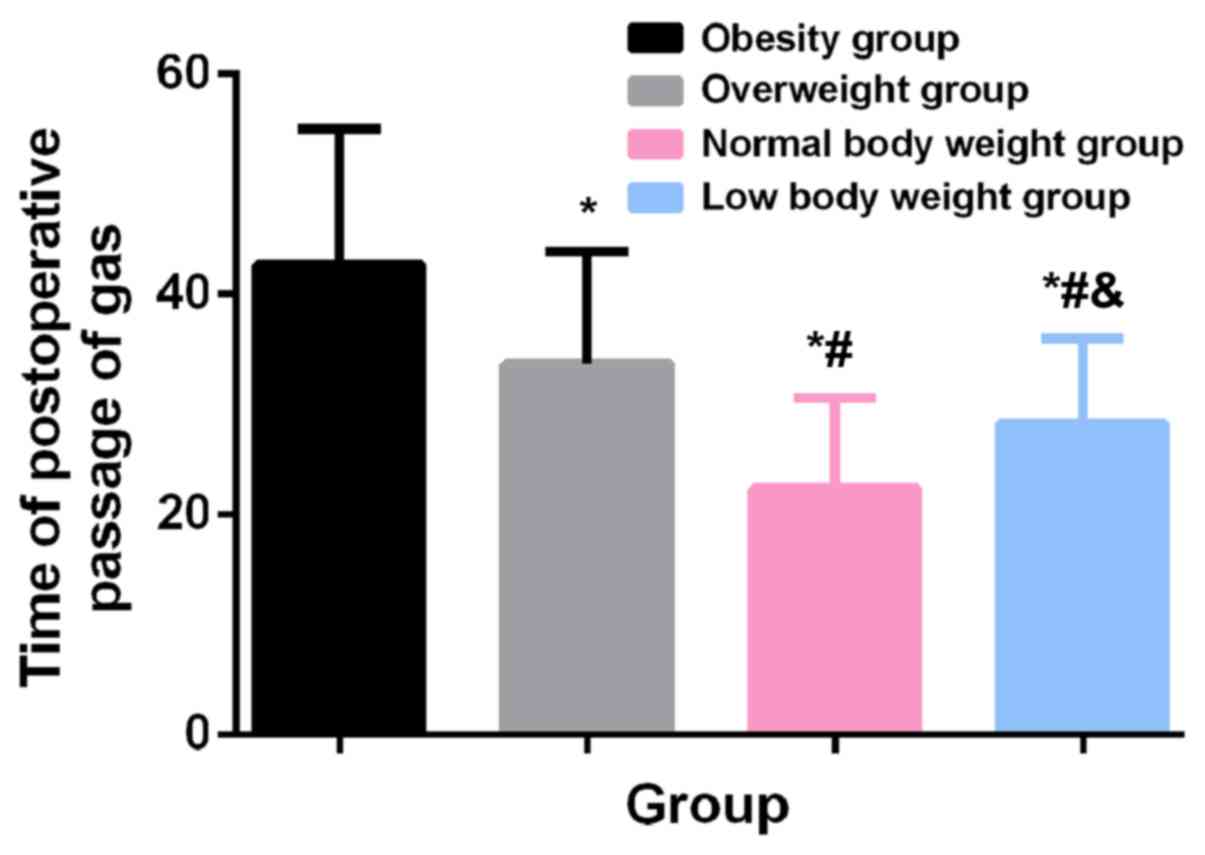
Postoperative conditions
The lengths of stay of patients in the 4 groups were
compared, and the results showed that the length of stay in the
obesity group was 16.24±3.67 days, which was the longest, followed
by those in the overweight group (14.37±2.33 days), the low body
weight group (12.86±2.07 days), and the normal group (9.63±2.15
days), which was the shortest (P<0.05). The time of
postoperative passage of gas in the 4 groups was in the same order
as above, i.e., the obesity group had the longest time of
postoperative passage of gas (42.68±12.33 h), followed by the
overweight group, the low body weight group and the normal body
weight group (P<0.05) (Figs. 1
and 2).
Complications
A total of 32 patients in the obesity group, 38
patients in the overweight group, 5 patients in the normal body
weight group and 9 patients in the low body weight group had
complications. Postoperative complications of the patients mainly
included bleeding, infection of incision, urinary retention,
intestinal obstruction, pulmonary infection, diarrhea, and venous
thrombosis. All the complications were the most serious in the
obesity group. The comparison results indicated that the incidence
rates of complications in the obesity group, overweight group, low
body weight group and the normal body weight group were 50.00,
30.65, 13.64 and 4.63%, respectively (P<0.05) (Table III).
| Table III.Comparison of complications among the
4 groups of patients. |
Table III.
Comparison of complications among the
4 groups of patients.
| Compications
experienced | Obesity group
(n=64) | Overweight group
(n=124) | Normal body weight
group (n=108) | Low body weight group
(n=66) | f value | P-value |
|---|
| Bleeding | 17 (26.56) | 12 (9.68) | 4 (3.70) | 5 (7.58) |
|
|
| Infection of
incision | 9 (14.06) | 4 (3.23) | 1 (0.93) | 2 (3.03) |
|
|
| Urinary
retention | 7 (10.94) | 3 (2.42) | 2 (1.85) | 2 (3.03) |
|
|
| Intestinal
obstruction | 12 (18.75) | 8 (6.45) | 0 (0) | 3 (4.55) |
|
|
| Pulmonary
infection | 7 (10.94) | 3 (2.42) | 0 (0) | 0 (0) |
|
|
| Diarrhea | 11 (17.19) | 6 (4.84) | 1 (0.93) | 3 (4.55) |
|
|
| Venous
thrombosis | 3 (4.69) | 1 (0.81) | 0 (0) | 0 (0) |
|
|
| Others | 8 (12.50) | 8 (6.45) | 2 (1.85) | 3 (4.55) |
|
|
| Incidence rates of
complications (%) | 50.00 | 30.65a | 4.63a,b | 13.64a–c | 67.82 | <0.01 |
Prognosis and survival rate
Among the 362 patients, 354 patients were
successfully followed up, with a success rate of follow-up of
97.79%. There were 3 cases in the obesity group, 3 cases in the
overweight group, 1 case in the normal body weight group and 2
cases in the low body weight group who were lost to follow-up.
One-year mortality rate of the obesity group was 35.94%,
significantly higher than those of the other three groups
(P<0.05). The 1-year mortality rate of the overweight group was
28.23%, followed by those of the low body weight group (24.24%) and
the normal body weight group (12.04%) (P<0.05). The differences
were statistically significant (Table
IV).
| Table IV.Prognosis and survival rates of
patients in the 4 groups. |
Table IV.
Prognosis and survival rates of
patients in the 4 groups.
| Time period | Obesity group
(n=61) | Overweight group
(n=121) | Normal body weight
group (n=107) | Low body weight
group (n=64) | f value | P-value |
|---|
| First month | 59 (96.72) | 117 (96.69) | 105 (98.13) | 62 (96.88) |
|
|
| Sixth month | 50 (81.97) | 101 (83.47) | 99 (92.52) | 56 (87.50) |
|
|
| Twelfth month | 41 (67.21) | 89 (73.55) | 95 (88.79) | 50 (78.13) |
|
|
| Total mortality
rate (%) | 35.94 | 28.23a | 12.04a,b | 24.24a–c | 56.21 | <0.01 |
Discussion
Due to high incidence rate and high mortality rate,
ovarian cancer has become a vital issue in clinical gynecology, and
it is urgent to make a breakthrough in this field (9). Currently, cytoreductive surgery is the
most effective measure to treat tumors (10). However, because of the special body
structure of females, ovarian lesions generally involve large areas
and are difficult to identify, and cytoreductive surgery cannot
thoroughly kill all cancer cells in patients, very easily resulting
in the recurrence and deterioration of ovarian cancer (11). Therefore, ovarian resection remains
the major procedure for clinical treatment of ovarian cancer
(12). Although the surgical
technique has become relatively mature, the prognosis of patients
with ovarian cancer is not satisfactory. Numerous studies have
evidenced that the prognosis of patients with ovarian cancer is
closely associated with many factors, of which BMI is highly
representative (13–15). As modern society develops rapidly,
living conditions have been increasingly improved, and obesity has
become one of the problems affecting most individuals. Due to high
BMI, obese patients are very vulnerable to diabetes and
cardiovascular disease (16). There
have been very few studies worldwide on the influence of BMI on
patients with ovarian cancer. Therefore, this study, by means of
analyzing the survival and postoperative complications of patients
with different BMIs who underwent ovarian cancer resection, aimed
to evaluate the influence of BMI on ovarian cancer resection, so as
to provide reliable reference for clinical treatment of such
patients in the future.
The results of this experiment demonstrated that the
obesity group ranked the first in terms of surgical time,
intraoperative blood loss amount, blood transfusion amount, length
of stay and complications (P<0.05), and its mortality rate was
the highest (P<0.05), followed by the overweight group, the low
body weight group and the normal body weight group. Ovarian cancer
resection is a traumatic surgery involving large areas, and
patients with extremely high BMI have more subcutaneous fat and
thicker fat layer, which not only affect field of view and
operation of the surgeon during surgeries, but also improve the
difficulty of suturing due to large fat tension in the suture
incision, thus resulting in the longest surgical time, and the
largest amount of intraoperative blood loss and blood transfusion
in the obesity group. In addition, because of excessively thick fat
layer which affects the healing of the incision, patients are more
susceptible to fat liquefaction and infection of incision (17). Moreover, obese patients tend to sweat
more, making it is difficult to keep the incision dry, which
results in the infection of incision. In addition, ovarian cancer
resection can damage vesical plexus of patients very easily, thus
lowering sensitivity of the bladder. Moreover, the bladder may be
displaced as it loses support after removal of the ovary, and the
accumulated urine cannot be discharged, thereby resulting in
urinary retention (18). Due to
accumulation of subcutaneous fats, internal organs of obese
patients are surrounded by a large amount of adipose tissues, which
will affect various functions of the patients to a certain extent
and retard the recovery of tissues in the body, thus resulting in
urinary retention, diarrhea and other complications in patients
with ovarian cancer. In addition, the accumulation of subcutaneous
fats can extremely easily lead to abdominal distention, backward
extension of thoracic vertebrae, lumbar lordosis and other
dislocations in patients, which compress the normal movements of
the ribs and chest, making patients more vulnerable to shortness of
breath and respiratory arrest after surgeries (19). Moreover, lungs cannot be stably
supplied with nutrients, and are therefore more susceptible to
infection. The accumulation of adipose tissues in obese patients
also affects normal blood supply of the vessels, thus causing blood
cell blockage and accelerating the formation of venous thrombosis
and embolus. The study by Tremaroli et al (20) also proved that patients with high BMI
have worse prognosis after gastrointestinal surgery, which confirms
the results of this experiment.
In this experiment, postoperative complications of
patients suffering from ovarian cancer with different BMI were
compared, research subjects were selected in strict accordance with
inclusion and exclusion criteria, and comparison and analysis were
performed using statistical analysis methods. However, due to the
limited conditions, the experiment still had deficiencies. For
example, a small cardinal number of research subjects and short
prognosis follow-up time may cause changes in the prognosis and
survival of patients. We will follow up the prognosis of patients
for a longer time and constantly improve and perfect the experiment
to obtain the most accurate results.
In conclusion, for patients with ovarian cancer,
obesity can raise the risks of postoperative complications and
worsen their prognosis. In clinical practice, therefore, various
indexes of tumor patients with high BMI should be monitored more
strictly after surgeries.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
HL drafted the manuscript. HL analyzed and
interpreted clinical data, surgical time, intraoperative blood loss
amount, intraoperative blood transfusion amount, time of
postoperative passage of gas, length of stay. SW analyzed
complications, prognosis and survival rate. Both authors read and
approved the final study.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Shanxi Dayi Hospital Affiliated to Shanxi Medical University
(Taiyuan, China). Signed informed consents were obtained from the
patients the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jacobs IJ, Menon U, Ryan A, Gentry-Maharaj
A, Burnell M, Kalsi JK, Amso NN, Apostolidou S, Benjamin E,
Cruickshank D, et al: Ovarian cancer screening and mortality in the
UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A
randomised controlled trial. Lancet. 387:945–956. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Oza AM, Cibula D, Benzaquen AO, Poole C,
Mathijssen RH, Sonke GS, Colombo N, Špaček J, Vuylsteke P, Hirte H,
et al: Olaparib combined with chemotherapy for recurrent
platinum-sensitive ovarian cancer: A randomised phase 2 trial.
Lancet Oncol. 16:87–97. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hamanishi J, Mandai M, Ikeda T, Minami M,
Kawaguchi A, Murayama T, Kanai M, Mori Y, Matsumoto S, Chikuma S,
et al: Safety and antitumor activity of anti-PD-1 antibody,
nivolumab, in patients with platinum-resistant ovarian cancer. J
Clin Oncol. 33:4015–4022. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kuchenbaecker KB, Ramus SJ, Tyrer J, Lee
A, Shen HC, Beesley J, Lawrenson K, McGuffog L, Healey S, Lee JM,
et al EMBRACE; GEMO Study Collaborators; Breast Cancer Family
Registry; HEBON; KConFab Investigators; Australian Cancer Study
(Ovarian Cancer Investigators); Australian Ovarian Cancer Study
Group; Consortium of Investigators of Modifiers of BRCA1BRCA2, :
Identification of six new susceptibility loci for invasive
epithelial ovarian cancer. Nat Genet. 47:164–171. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Falconer H, Yin L, Grönberg H and Altman
D: Ovarian cancer risk after salpingectomy: A nationwide
population-based study. J Natl Cancer Inst. 107:4102015. View Article : Google Scholar
|
|
6
|
Bachmayr-Heyda A, Reiner AT, Auer K,
Sukhbaatar N, Aust S, Bachleitner-Hofmann T, Mesteri I, Grunt TW,
Zeillinger R and Pils D: Correlation of circular RNA abundance with
proliferation - exemplified with colorectal and ovarian cancer,
idiopathic lung fibrosis, and normal human tissues. Sci Rep.
5:80572015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kim G, Ison G, McKee AE, Zhang H, Tang S,
Gwise T, Sridhara R, Lee E, Tzou A, Philip R, et al: FDA approval
summary: Olaparib monotherapy in patients with deleterious germline
BRCA-mutated advanced ovarian cancer treated with three or more
lines of chemotherapy. Clin Cancer Res. 21:4257–4261. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lauby-Secretan B, Scoccianti C, Loomis D,
Grosse Y, Bianchini F and Straif K; International Agency for
Research on Cancer handbook working group, : Body fatness and
cancer - viewpoint of the IARC working group. N Engl J Med.
375:794–798. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lu Y, Day FR, Gustafsson S, Buchkovich ML,
Na J, Bataille V, Cousminer DL, Dastani Z, Drong AW, Esko T, et al:
New loci for body fat percentage reveal link between adiposity and
cardiometabolic disease risk. Nat Commun. 7:104952016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rebbeck TR, Mitra N, Wan F, Sinilnikova
OM, Healey S, McGuffog L, Mazoyer S, Chenevix-Trench G, Easton DF,
Antoniou AC, et al CIMBA Consortium, : Association of type and
location of BRCA1 and BRCA2 mutations with risk of breast and
ovarian cancer. JAMA. 313:1347–1361. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Walker JL, Powell CB, Chen LM, Carter J,
Bae Jump VL, Parker LP, Borowsky ME and Gibb RK: Society of
Gynecologic Oncology recommendations for the prevention of ovarian
cancer. Cancer. 121:2108–2120. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang F, Zhou J, Xie X, Hu J, Chen L, Hu Q,
Guo H and Yu C: Involvement of SRPK1 in cisplatin resistance
related to long non-coding RNA UCA1 in human ovarian cancer cells.
Neoplasma. 62:432–438. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hareyama H, Hada K, Goto K, Watanabe S,
Hakoyama M, Oku K, Hayakashi Y, Hirayama E and Okuyama K:
Prevalence, classification, and risk factors for postoperative
lower extremity lymphedema in women with gynecologic malignancies:
A retrospective study. Int J Gynecol Cancer. 25:751–757. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
McDermott FD, Heeney A, Kelly ME, Steele
RJ, Carlson GL and Winter DC: Systematic review of preoperative,
intraoperative and postoperative risk factors for colorectal
anastomotic leaks. Br J Surg. 102:462–479. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang WW, Liu KJ, Hu GL and Liang WJ:
Preoperative platelet/lymphocyte ratio is a superior prognostic
factor compared to other systemic inflammatory response markers in
ovarian cancer patients. Tumour Biol. 36:8831–8837. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shungin D, Winkler TW, Croteau-Chonka DC,
Ferreira T, Locke AE, Mägi R, Strawbridge RJ, Pers TH, Fischer K,
Justice AE, et al ADIPOGen Consortium; CARDIOGRAMplusC4D
Consortium; CKDGen Consortium; GEFOS Consortium; GENIE Consortium;
GLGC; ICBP; International Endogene Consortium; LifeLines Cohort
Study; MAGIC Investigators; MuTHER Consortium; PAGE Consortium;
ReproGen Consortium, : New genetic loci link adipose and insulin
biology to body fat distribution. Nature. 518:187–196. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yu H, Di J, Bao Y, Zhang P, Zhang L, Tu Y,
Han X and Jia W: Visceral fat area as a new predictor of short-term
diabetes remission after Roux-en-Y gastric bypass surgery in
Chinese patients with a body mass index less than 35
kg/m2. Surg Obes Relat Dis. 11:6–11. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Osborn DJ, Kaufman MR, Mock S, Guan MJ,
Dmochowski RR and Reynolds WS: Urinary retention rates after
intravesical onabotulinumtoxinA injection for idiopathic overactive
bladder in clinical practice and predictors of this outcome.
Neurourol Urodyn. 34:675–678. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Schafer AL, Li X, Schwartz AV, Tufts LS,
Wheeler AL, Grunfeld C, Stewart L, Rogers SJ, Carter JT, Posselt
AM, et al: Changes in vertebral bone marrow fat and bone mass after
gastric bypass surgery: A pilot study. Bone. 74:140–145. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tremaroli V, Karlsson F, Werling M,
Ståhlman M, Kovatcheva-Datchary P, Olbers T, Fändriks L, le Roux
CW, Nielsen J and Bäckhed F: Roux-en-Y gastric bypass and vertical
banded gastroplasty induce long-term changes on the human gut
microbiome contributing to fat mass regulation. Cell Metab.
22:228–238. 2015. View Article : Google Scholar : PubMed/NCBI
|