Introduction
Oral squamous cell carcinoma (OSCC) accounts for
>90% of primary oral malignancies worldwide (1). A combination of different genetic
features and environmental factors contributes to the oncogenesis
of OSCC (2). Although treatment
methods, including chemotherapy, radiotherapy and surgery, have
advanced, the 5-year overall survival rate of patients with OSCC
remains ~50% (3). Locoregional
recurrence, metastatic disease and second primary tumors are the
main factors contributing to the poor survival rate of patients
with OSCC (4).
OSCCs are often ulcerated with a large number of
lymphocyte infiltration. An improved understanding of the tumor
immune microenvironment, including number, location and function of
infiltrating lymphocytes is crucial in order to examine and test
immunotherapeutic strategies, which may prolong the survival time
of patients with OSCC (5).
Tumor-infiltrating lymphocytes (TILs) are considered to be the host
immune response to tumor cells (6).
To date, a number of studies have reported an association between
the TILs subset and patient prognosis in various types of cancer
(6,7). Tumor infiltration by CD8+ T
cells, including cytotoxic T cells (CTLs), has been indicated to be
associated with an improved prognosis in various types of malignant
tumors (7). In turn, increasing
evidence has demonstrated that tumor-infiltrating forkhead box P3
(FoxP3)+ immunosuppressive regulatory T cells (Tregs)
are associated with poor prognosis, and suppressed function on host
antitumor immunity (8). The ratio of
cytotoxic CD8+ T cells and FoxP3+ Tregs in
the tumor microenvironment has been indicated to be a prognostic
factor in in various types of cancer (9–11).
However, further investigations on the role of TILs in OSCC are
required.
C-X-C motif chemokine ligand 12 (CXCL12) serves
multiple tumor promoting functions via its cognate receptor C-X-C
motif chemokine receptor (CXCR)4 present in cancer cells; either
directly, by enhancing tumor growth, migration and invasiveness, or
indirectly, by recruiting endothelial progenitors required for
tumor angiogenesis (12,13). In addition, CXCL12 promotes tumor
immunosuppression by recruiting specific immune cell populations
(13). Therefore, it may be
hypothesized that the expression levels of CXCL12 in OSCC are
associated with tumor progression and immune suppression. To
examine this hypothesis, the present study investigated the
association among clinicopathological parameters of OSCC and
CXCL12, densities of CD8+ T cells and FoxP3+
T cells. In addition, the present study examined whether CXCL12
expression can influence CD8+ T cells or
FoxP3+ T cells distribution in patients with OSCC.
Patients and methods
Patients and sample collection
The present study was performed on a retrospective
cohort of 45 Chinese patients with primary OSCC. A total of 24
patients were male and 21 were female, and the median age was 61
(range, 37–81 years). Paraffin-embedded tissue specimens, including
OSCC tissue and adjacent non-cancerous tissue, were collected from
the West China College of Stomatology, Sichuan University between
January 2011 and December 2011. All patients underwent radical
surgery with neck dissection without receiving any preoperative
radiotherapy and chemotherapy. All patients signed informed consent
forms prior to the present study. Data from patient follow-up and
clinicopathological characteristics were collected from the
database of West China College of Stomatology and telephone
interviews. Clinical staging was established according to the
American Joint Committee on Cancer Staging Manual (2009) (14). The present study was approved by the
Institutional Review Board of West China Hospital of Stomatology of
Sichuan University.
Immunohistochemistry
Formalin-fixed at 4°C for 24 h, paraffin-embedded
tissues, obtained from the Department of Pathology, West China
Hospital of Stomatology, were consecutively cut into 5-µm sections
and transferred onto silanized glass slides. Immunohistochemistry
for CXCL12, CD8 and FoxP3 was performed using standard procedures
(8,9). Briefly, 5-µm tissue sections were
dewaxed and rehydrated using xylene and graded alcohol washes. The
slides were heated to 121°C for 2 min for antigen retrieval in
citrate buffer (pH 6.0). Following serial blocking with 3% hydrogen
peroxide and 5% normal goat serum (cat. no., ZLI-9022; OriGene
Technologies, Inc.) at 37°C for 20 min, the sections were incubated
with primary monoclonal antibody against CD8 (dilution, 1:100;
clone C8/144B; Dako), CXCL12 (dilution, 1:400; cat. no. ab9797;
Abcam) or FoxP3 (dilution 1:100; cat. no. ab20034; Abcam) for 16 h
at 4°C. The sections were then incubated with biotinylated goat
anti-mouse immunoglobulin and peroxidase-conjugated streptavidin
(dilution, 1:100; cat. no., cat. no., ab64255; Abcam) at 37°C for
30 min. The enzyme substrate was 3,3′-diaminobenzidine
tetrahydrochloride. Tissue section were analyzed using a light
microscope. Negative controls were performed with PBS instead of
the primary antibody.
Evaluation of immunohistochemistry
results
For CXCL12 expression, the respective score was
calculated according to a visual grading scale based on the
percentage of positive cells and the intensity of staining. The
percentage scale was as follows: 0, <5; 1, 5–25; 2, 25–50; 3,
50–75; and 4, >75%. The intensity scale was as follows: 0, none;
1, weak staining; 2, moderate staining; and 3, strong staining.
Five representative fields of view were evaluated (magnification,
×400). The final weighted score was calculated for each case by
multiplying the two scores: <1, negative; ≥1, positive (15). The patients were divided into high
and low expression CXCL12 groups according to the median
values.
For CD8+ T and FoxP3+ T cells,
tissue sections were examined microscopically (magnification,
×400), five high-power fields of each case with the most abundant
TILs were selected for image capturing at an area of 0.0625
mm2, and the numbers of CD8+ T and
FoxP3+ T cells in each field were counted in the same
five areas of serial sections. The mean value represented the
number of lymphocyte infiltration, as described previously
(16).
Statistical analysis
The data was presented as mean ± standard deviation.
For CXCL12 expression and TILs densities, five areas were measured
and the mean score of the five areas was collected for further
analyses. Associations among clinicopathological features, CXCL12
expression and densities of TILs were evaluated using the
χ2 test. The variables were dichotomized via median
splits. Survival curves were plotted using the Kaplan-Meier method,
and significant differences in the overall survival rate were
assessed using a log-rank test. The correlation between variables
was calculated by linear regression. P<0.05 was considered to
indicate a statistically significant difference. All statistical
analyses were performed using SPSS version 19.0 (IBM Corp.).
Results
Characteristics of patients with OSCC
included in the present study
Between January 2011 and December 2011, a total of
45 specimens were collected from 45 pathologically confirmed
patients with OSCC. Out of these patients, 24 were male, 29 had
advanced disease, 14 exhibited poor differentiation and 19
exhibited positive lymph node metastasis.
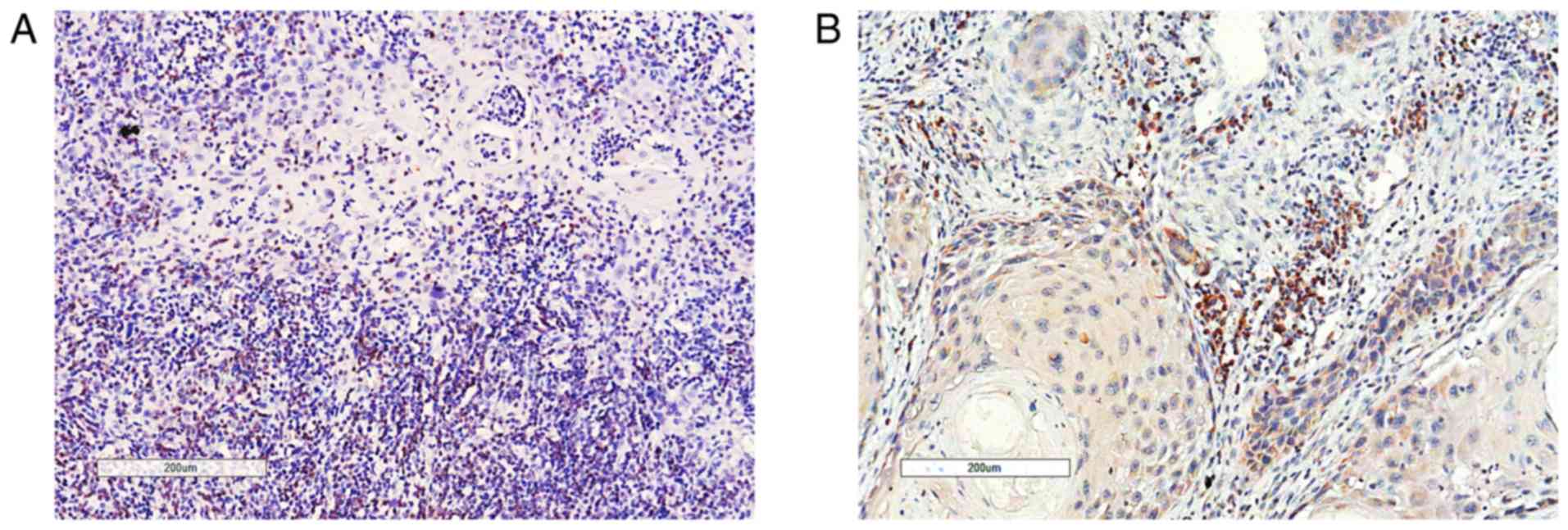
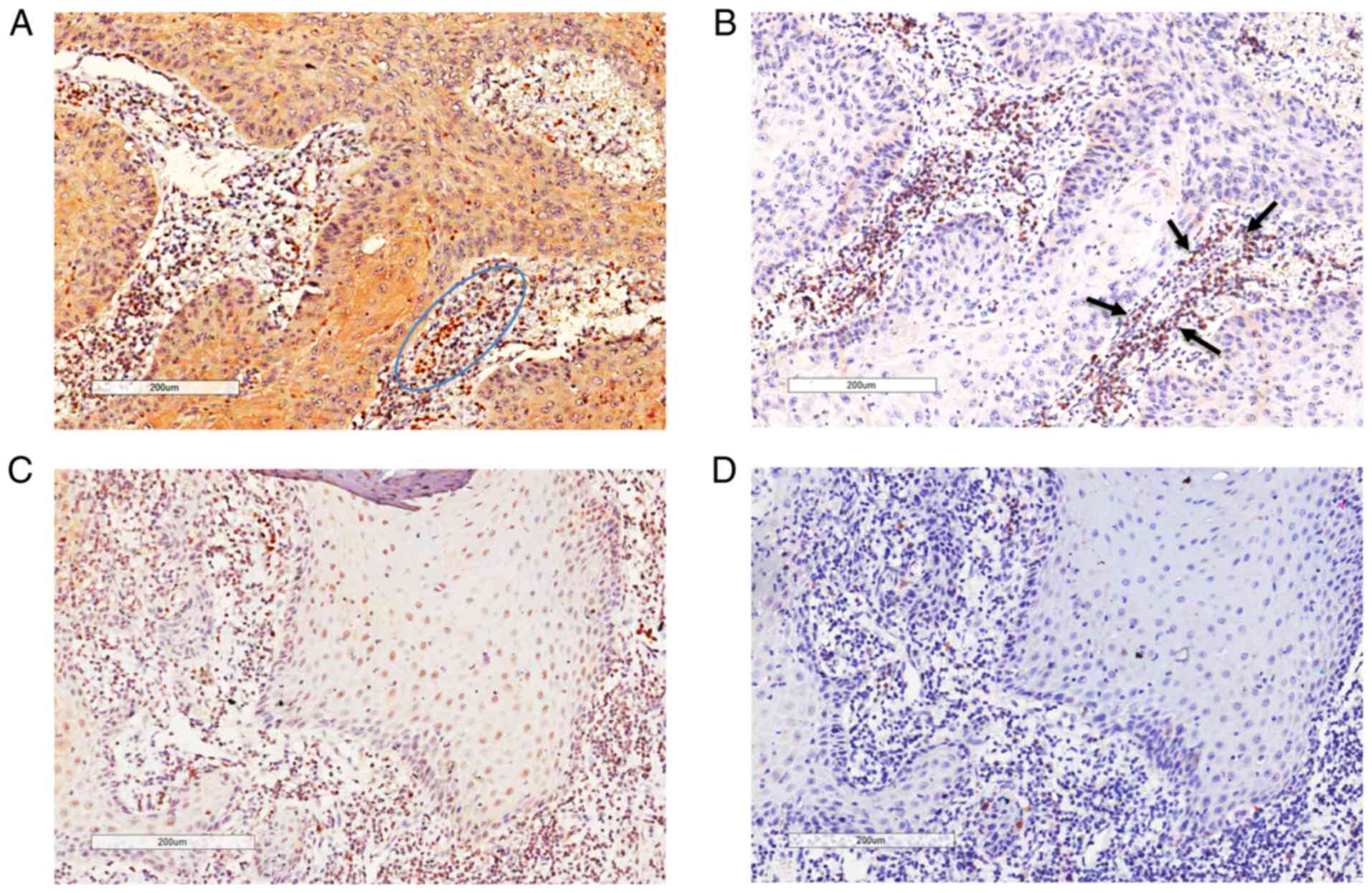
General features of TILs in OSCC
TILs were distributed in the cancer cell nests and
in the stroma of the tumor-host interface. The majority of
FoxP3+ T cells were located in the stroma (Fig. 1B). However, CD8+ T cells
infiltrated not only the stroma of the tumor-host interface but
also the cancer cell nests (Fig.
1A). CD8+ TILs and FoxP3+ TILs were
present in every case, with an average number of 111.9 and 50.4 per
0.0625 mm2, respectively (Table I). The median value of the
CD8+/FoxP3+ ratio was 2.07, ranging between
0.1 and 20 (data not shown).
 | Table I.Expressions levels of FoxP3 and CD8
in TILs in oral squamous cell carcinoma. |
Table I.
Expressions levels of FoxP3 and CD8
in TILs in oral squamous cell carcinoma.
| Variables | FoxP3+
TIL | CD8+
TIL |
|---|
| Number of patients,
n | 45 (100%) | 45 (100%) |
| Average number per
0.0625 mm2, n | 50.4 | 111.9 |
| Range | 9–99 | 7–259 |
| Location | Stroma | Stroma |
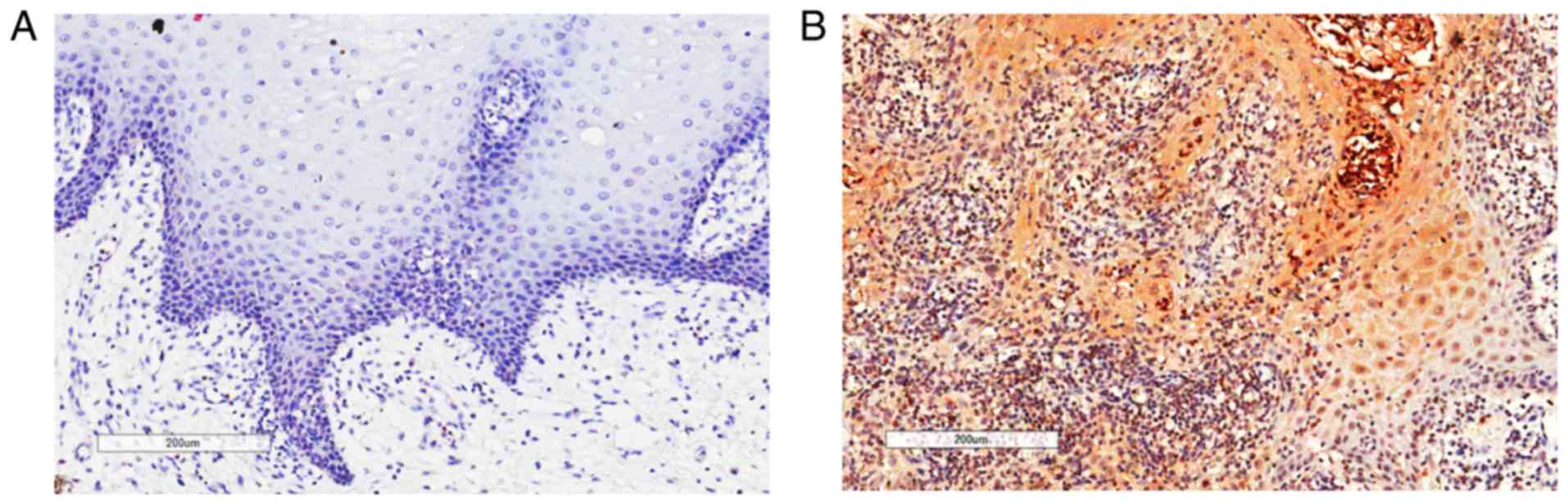
Expression levels of CXCL12 in OSCC
cells
Among the available specimens, 11 specimens included
OSCC tissues and adjacent non-cancerous tissues (epithelia and
stroma). The non-cancerous tissues were collected from 0.5–1 cm
apart from the margin. These samples were selected to compare
CXCL12 expression between tumor adjacent tissues and OSCC tissues.
The present study demonstrated that, in these specimens, CXCL12
could not be detected in adjacent non-cancerous tissues (Fig. 2A). CXCL12 expression in OSCC cells
was observed in 68.9% (31/45) of OSCC cases. Cytoplasmic and
intracellular staining patterns were observed in OSCC tissues
(Fig. 2B).
Association among TILs density in the
tumor microenvironment and clinicopathological features/survival of
patients with OSCC
Associations among clinicopathological features and
TILs density are summarized in Table
II. An increased number of FoxP3+ TILs was
associated with tumor recurrence (P=0.022) in patients with OSCC.
There was no significant association identified among the density
of CD8+ TILs and any of the clinicopathological features
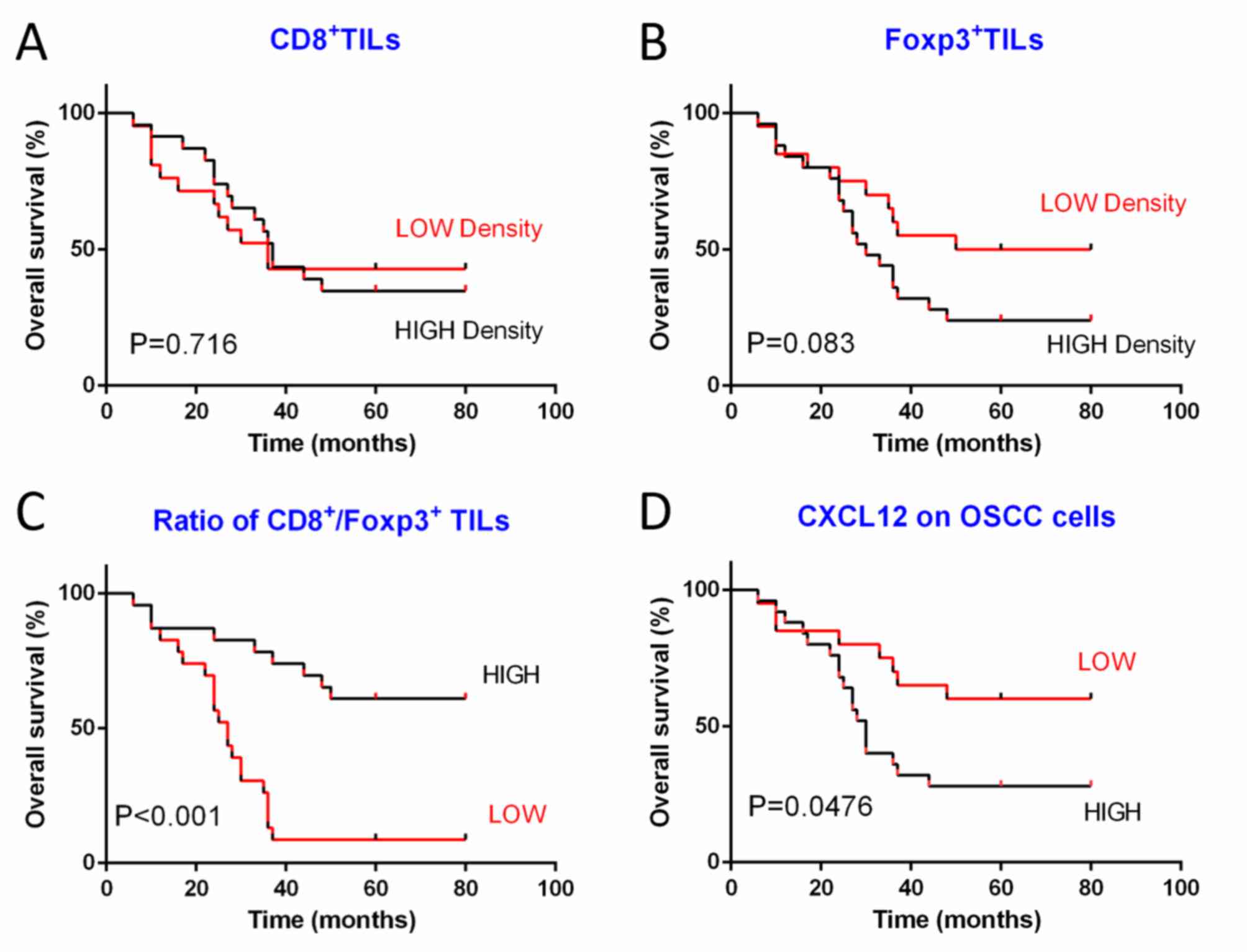
of patients with OSCC examined in the present study. Furthermore,
neither the density of CD8+ TILs nor the density of
FoxP3+ TILs were associated with patient survival
(Fig. 3A and B). However, the ratio
of these two types of TILs was suggested to be more important
compared with their densities when evaluating the
clinicopathological features and survival of patients (9). In particular, a low
CD8+/FoxP3+ ratio was significantly
associated with poor differentiation (P=0.034), advanced stage
tumors (P=0.015) and tumor recurrence (P=0.002). In addition, low
CD8+/FoxP3+ TILs ratios were associated with
a poor 5-year overall survival rate (P<0.001; Fig. 3C).
| Table II.Associations between
clinicopathological parameters of patients with oral squamous cell
carcinoma and densities of TILs. |
Table II.
Associations between
clinicopathological parameters of patients with oral squamous cell
carcinoma and densities of TILs.
|
|
| FoxP3+
TIL | CD8+
TIL | CD8/FoxP3
ratio |
|---|
|
|
|
|
|
|
|---|
| Variables | Number, n | Low | High | P-value | Low | High | P-value | Low | High | P-value |
|---|
| Age |
|
|
| 0.174 |
|
| 0.214 |
|
| 0.140 |
|
≤59 | 24 | 12 | 12 |
| 11 | 13 |
| 10 | 14 |
|
|
>59 | 21 | 8 | 13 |
| 11 | 10 |
| 12 | 9 |
|
| Sex |
|
|
| 0.231 |
|
| 0.232 |
|
| 0.178 |
|
Male | 24 | 11 | 13 |
| 12 | 12 |
| 13 | 11 |
|
|
Female | 21 | 9 | 12 |
| 10 | 11 |
| 9 | 12 |
|
| Tumor size |
|
|
| 0.165 |
|
| 0.233 |
|
| 0.142 |
| T1,
T2 | 19 | 7 | 12 |
| 9 | 10 |
| 11 | 8 |
|
| T3,
T4 | 26 | 13 | 13 |
| 13 | 13 |
| 11 | 15 |
|
| Lymph node
metastasis |
|
|
| 0.230 |
|
| 0.142 |
|
Positive | 19 | 8 | 11 |
| 11 | 8 |
| 12 | 7 | 0.065 |
|
Negative | 26 | 12 | 14 |
| 11 | 15 |
| 10 | 16 |
|
| Stage (14) |
|
|
| 0.125 |
|
| 0.132 |
|
| 0.015a |
| I,
II | 16 | 9 | 7 |
| 6 | 10 |
| 4 | 12 |
|
| III,
IV | 29 | 11 | 18 |
| 16 | 13 |
| 18 | 11 |
|
|
Differentiation |
|
|
| 0.095 |
|
| 0.251 |
|
| 0.034a |
|
Well-moderate | 31 | 16 | 15 |
| 15 | 16 |
| 12 | 19 |
|
|
Poor | 14 | 4 | 10 |
| 7 | 7 |
| 10 | 4 |
|
| Recurrence |
|
|
| 0.022a |
|
| 0.097 |
|
| 0.002a |
|
Yes | 24 | 7 | 17 |
| 14 | 10 |
| 17 | 7 |
|
| No | 21 | 13 | 8 |
| 8 | 13 |
| 5 | 16 |
|
Association between CXCL12 expression
and clinicopathological features/survival of patients with
OSCC
As indicated in Table
III, patients with poor differentiation (P=0.045), advanced
stage tumors (P<0.001) and tumor recurrence (P=0.011) tended to
exhibit a higher CXCL12 expression level. No significant
associations among CXCL12 expression and lymph node metastasis
(P=0.200) and tumor size (P=0.200) were identified. In addition,
high CXCL12 expression was associated with poor overall survival
(P=0.0476; Fig. 3D).
| Table III.Associations between CXCL12
expression and clinicopathological parameters of patients with oral
squamous cell carcinoma and density of TILs. |
Table III.
Associations between CXCL12
expression and clinicopathological parameters of patients with oral
squamous cell carcinoma and density of TILs.
|
|
| CXCL12 in tumor
cells |
|---|
|
|
|
|
|---|
| Variable | Number, n | Low score, n | High sore, n | P-value |
|---|
| Age |
|
|
| 0.056 |
|
≤59 | 24 | 13 | 11 |
|
|
>59 | 21 | 6 | 15 |
|
| Sex |
|
|
| 0.189 |
|
Male | 24 | 9 | 15 |
|
|
Female | 21 | 10 | 11 |
|
| Tumor size |
|
|
| 0.200 |
| T1,
T2 | 19 | 7 | 12 |
|
| T3,
T4 | 26 | 12 | 14 |
|
| Lymph node
metastasis |
|
|
| 0.200 |
|
Positive | 19 | 7 | 12 |
|
|
Negative | 26 | 12 | 14 |
|
| Stage (14) |
|
|
|
<0.001a |
| I,
II | 16 | 12 | 4 |
|
| III,
IV | 29 | 7 | 22 |
|
|
Differentiation |
|
|
| 0.045a |
|
Well-moderate | 31 | 16 | 15 |
|
|
Poor | 14 | 3 | 11 |
|
| Recurrence |
|
|
| 0.011a |
|
Yes | 24 | 6 | 18 |
|
| No | 21 | 13 | 8 |
|
| FoxP3+
TIL |
|
|
|
<0.001a |
|
Low | 20 | 15 | 5 |
|
|
High | 25 | 4 | 21 |
|
| CD8+
TIL |
|
|
| 0.095 |
|
Low | 22 | 7 | 15 |
|
|
High | 23 | 12 | 11 |
|
| CD8/FoxP3
ratio |
|
|
|
<0.001a |
|
Low | 22 | 2 | 20 |
|
|
High | 23 | 17 | 6 |
|
Association between CXCL12 expression
and TILs density
The density of FoxP3+ TILs exhibited a
significant positive association with the CXCL12 expression of
tumor cells (P<0.001). However, the density of CD8+
TILs was not identified to be associated with CXCL12 expression
(P=0.095). In addition, the ratio of
CD8+/FoxP3+ exhibited a significant negative
association with CXCL12 expression (P<0.001; Table III).
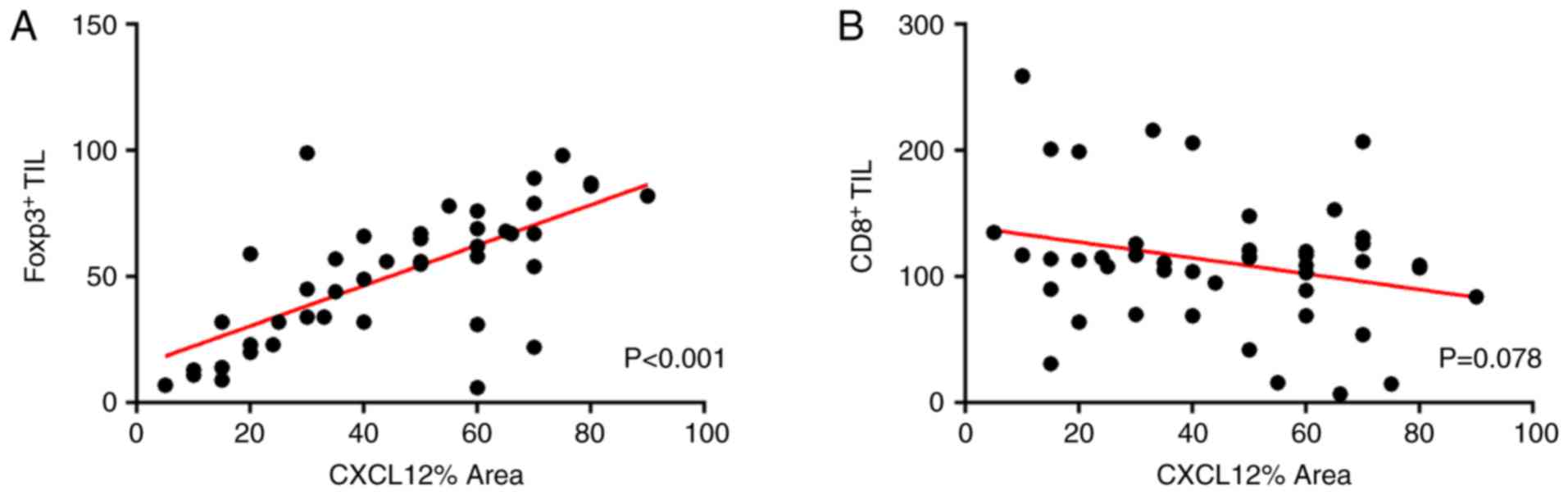
To investigate the association between TILs and
CXCL12 expression, a linear regression test was performed. The
results indicated a correlation between CXCL12 percentage area and
the density of FoxP3+ TILs (R2=0.481,
P<0.001; Fig. 4A). By contrast,
the CD8+ TILs were not identified to be significantly
correlated with CXCL12 percentage area (R2=0.070,
P=0.078; Fig. 4B). Further
observations revealed that the higher the expression level of
CXCL12, the larger the number of FoxP3+ T-cells
infiltrating in the tumor microenvironment (Fig. 5A and B). Conversely,
FoxP3+ T-cells hardly infiltrated in the region with low
CXCL12 expression (Fig. 5A and
B).
Discussion
CXCL12 was initially known as a chemotactic factor
for T cells and monocytes, and as a growth factor for B cell
progenitor cells. In recent years, there has been an increasing
number of studies focusing on the pathological characteristics of
CXCL12 in the tumor microenvironment (12,13).
Particularly, attention has been drawn to the tumor
microenvironment suppressing the effectiveness of immune responses
by trafficking and retaining these immunosuppressive cells
(17). However, further studies are
required regarding the role of CXCL12 in OSCC. In the present
study, the expression levels of CXCL12 were investigated as a novel
prognostic factors in the treatment of OSCC. High expression levels
of CXCL12 may contribute to a high recurrence rate and a low 5-year
overall survival rate. The results of a previous study are in
accordance with the results of the present study. In particular,
Clatot et al (18)
investigated 71 patients with primary head and neck squamous cell
carcinoma, and revealed that CXCL12 expression is significantly
associated with metastatic evolution and overall survival.
TILs in the tumor microenvironment may reflect tumor
biology and predict prognosis. However, further examination is
required to investigate whether lymphocyte infiltration at the
primary tumor site represents a beneficial antitumor immune
response in the tumor microenvironment, or whether it is implicated
as a poor prognostic factor, promoting tumor progression by
releasing regulatory cytokines (19,20).
CTLs belong to the CD8 population, a major subpopulation which has
been suggested to aid in the promotion of immune mediated tumor
regression and serve as a response indicator in chemotherapy in a
number of types of cancer (7,9). A
number of studies have indicated that decreased numbers of nest and
stromal CD8+ T cells were associated with lower survival
time in patients with OSCC (5,21). The
present study reported that the density of CD8+ TILs was
not associated with the overall survival or any of the
clinicopathological features of OSCC. Therefore, taking the
aforementioned into consideration, it is controversial to regard
CD8+ TILs as an independent prognostic factor.
The development and function of Tregs depends on the
expression of FoxP3, which has been reported as the master
regulator (22). Tumor cells have
the ability to recruit Tregs to the tumor microenvironment to
inhibit antitumor immunity in patients with cancer. It has been
reported that a population of FoxP3+ regulatory T cells
serves as a predicting factor for survival in colon cancer
(22). In the present study,
FoxP3+ TILs were significantly associated with tumor
recurrence. Furthermore, it was indicated that a high density of
FoxP3+ TILs in OSCC tissue is associated with poor
survival, however this result was not significant (P=0.083). The
number of FoxP3+ TILs tended to be sparse in early stage
OSCC and in well-differentiated OSCC. Conversely, in the present
study, expression levels of FoxP3+ TILs were higher in
advanced stage OSCC and poorly-differentiated OSCC. This finding
may indicate that FoxP3+ TILs may serve an important
role in suppressing an antitumor immune response in advanced OSCC
compared to early OSCC. However, another study revealed that higher
peripheral blood levels of this subset were associated with
improved survival in patients with oropharyngeal cancer (5). Another study on tumor infiltration
suggested that high expression levels of FoxP3 infiltration are
associated with an increased survival rate in patients with head
and neck cancer (23).
Therefore, the balance between the CD8+
TILs and FoxP3+ TILs is significant. In the present
study, the CD8+/FoxP3+ ratio was revealed to
be the strongest prognostic indicator and was associated with poor
differentiation, advanced stage tumors, tumor recurrence and poor
survival rates. A previous study demonstrated that the
CD8+/C-C motif chemokine receptor 4+ T-cells
ratio was the most significant prognostic factor among all
TIL-associated variables (6).
Additionally, various types of immune cells can be attracted to the
tumor environment via CXCL12 (24,25).
Thus, the present study investigated the
associations among CXCL12 expression and FoxP3+ TILs and
CD8+ TILs in OSCC. Notably, the present study revealed
that FoxP3+ TIL counts and CXCL12 percentage area
exhibited a significant correlation. However, no significant
correlation was detected for CD8+ TILs and CXCL12
percentage area. In addition, the present study identified that
some stroma cells with high CXCL12 expression were surrounded by
numerous FoxP3+ TILs, which may support the result of a
correlation between FoxP3+ TIL counts and CXCL12
percentage area. Therefore, the present study demonstrated that
CXCL12 may contribute to tumor immunosuppression by recruiting
FoxP3+ T-cell populations in OSCC. The chemokine CXCL12
is a well-known T-cell chemoattractant that selectively binds its
receptors CXCR4 and CXCR7. Activation of Tregs upregulates CXCR4 or
CXCR7 expression and drives them to migrate to the tumor
microenvironment in a CXCL12-dependent manner (24). A recent study indicated that
inhibition of CXCL12 expression may increase the number of
tumor-infiltrating lymphocytes and overcome resistance to
anti-programmed cell death protein 1 treatment (26). Additionally, CXCL12 and CXCR4 may
attract the myeloid-derived suppressor cells into the tumor
microenvironment in ovarian cancer (25).
In conclusion, the present study indicated that some
clinicopathological parameters, including tumor differentiation,
tumor stage and overall survival, were significantly associated
with the CD8+/FoxP3+ ratio and CXCL12
expression. Overall, these findings supported the hypothesis that
high expression levels of CXCL12 may lead to FoxP3+
T-cells accumulation in the progression of OSCC. However, the
underlying mechanism of CXCL12 in recruiting FoxP3+ TILs
in OSCC remains unclear. In addition, considering the limited
sample size, the subgroup survival analysis of CXCL12 could not be
conducted. Therefore, further large and long-term studies are
required to validate and supplement the findings of the present
study. The present study indicated that CXCL12 is a potential
prognostic marker that may assist in the pathological analysis of
OSCC. Recently, immunotherapy has become an increasingly important
treatment strategy in tumor therapy. Specific blocking of CXCL12 is
expected to enhance the effects of immunotherapy for OSCC in the
future.
Acknowledgements
The authors would like to thank Professor Xiaoyu Li
and Dr Yu Chen from State Key Laboratory of Oral Diseases and
pathology department for their technical support and assistance in
experiments.
Funding
The present study was funded by the National Natural
Science Foundation of China (grant no. 81472532) and Graduate
Student's Research and Innovation Fund of Sichuan University (grant
no. 2018YJSY106).
Availability of data and materials
The datasets used or analysed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
BZ and CW participated in the design and conducted
the experiments, data analysis, and final drafting and writing of
the manuscript. ZZ, KY, YL and CL were involved in research design
and contributed to the drafting of the manuscript. LL was involved
in research design and drafting of the final manuscript. All
authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of West China Hospital of Stomatology of Sichuan
University. All patients signed informed consent forms prior to the
present study.
Patient consent for publication
Informed consent was obtained from all patients for
the publication of the present study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
McDowell JD: An overview of epidemiology
and common risk factors for oral squamous cell carcinoma.
Otolaryngol Clin North Am. 39:277–294. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Williams HK: Molecular pathogenesis of
oral squamous carcinoma. Mol Pathol. 53:165–172. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bernier J, Domenge C, Ozsahin M,
Matuszewska K, Lefèbvre JL, Greiner RH, Giralt J, Maingon P,
Rolland F, Bolla M, et al: Postoperative irradiation with or
without concomitant chemotherapy for locally advanced head and neck
cancer. N Engl J Med. 350:1945–1952. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Warnakulasuriya S: Global epidemiology of
oral and oropharyngeal cancer. Oral Oncol. 45:309–316. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wolf GT, Chepeha DB, Bellile E, Nguyen A,
Thomas D and McHugh J; University of Michigan Head and Neck SPORE
Program, : Tumor infiltrating lymphocytes (TIL) and prognosis in
oral cavity squamous carcinoma: A preliminary study. Oral Oncol.
51:90–95. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Watanabe Y, Katou F, Ohtani H, Nakayama T,
Yoshie O and Hashimoto K: Tumor-infiltrating lymphocytes,
particularly the balance between CD8(+) T cells and CCR4(+)
regulatory T cells, affect the survival of patients with oral
squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 109:744–752. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Piersma SJ, Jordanova ES, van Poelgeest
MI, Kwappenberg KM, van der Hulst JM, Drijfhout JW, Melief CJ,
Kenter GG, Fleuren GJ, Offringa R and van der Burg SH: High number
of intraepithelial CD8+ tumor-infiltrating lymphocytes is
associated with the absence of lymph node metastases in patients
with large early-stage cervical cancer. Cancer Res. 67:354–361.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wolf D, Wolf AM, Rumpold H, Fiegl H,
Zeimet AG, Muller-Holzner E, Deibl M, Gastl G, Gunsilius E and
Marth C: The expression of the regulatory T cell-specific forkhead
box transcription factor FoxP3 is associated with poor prognosis in
ovarian cancer. Clin Cancer Res. 11:8326–8331. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sato E, Olson SH, Ahn J, Bundy B,
Nishikawa H, Qian F, Jungbluth AA, Frosina D, Gnjatic S, Ambrosone
C, et al: Intraepithelial CD8+ tumor-infiltrating lymphocytes and a
high CD8+/regulatory T cell ratio are associated with favorable
prognosis in ovarian cancer. Proc Natl Acad Sci USA.
102:18538–18543. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gao Q, Qiu SJ, Fan J, Zhou J, Wang XY,
Xiao YS, Xu Y, Li YW and Tang ZY: Intratumoral balance of
regulatory and cytotoxic T cells is associated with prognosis of
hepatocellular carcinoma after resection. J Clin Oncol.
25:2586–2593. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jordanova ES, Gorter A, Ayachi O, Prins F,
Durrant LG, Kenter GG, van der Burg SH and Fleuren GJ: Human
leukocyte antigen class I, MHC class I chain-related molecule A,
and CD8+/regulatory T-cell ratio: Which variable determines
survival of cervical cancer patients? Clin Cancer Res.
14:2028–2035. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kryczek I, Lange A, Mottram P, Alvarez X,
Cheng P, Hogan M, Moons L, Wei S, Zou L, Machelon V, et al: CXCL12
and vascular endothelial growth factor synergistically induce
neoangiogenesis in human ovarian cancers. Cancer Res. 65:465–472.
2005.PubMed/NCBI
|
|
13
|
Orimo A, Gupta PB, Sgroi DC,
Arenzana-Seisdedos F, Delaunay T, Naeem R, Carey VJ, Richardson AL
and Weinberg RA: Stromal fibroblasts present in invasive human
breast carcinomas promote tumor growth and angiogenesis through
elevated SDF-1/CXCL12 secretion. Cell. 121:335–348. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xia J, Chen N, Hong Y, Chen X, Tao X,
Cheng B and Huang Y: Expressions of CXCL12/CXCR4 in oral
premalignant and malignant lesions. Mediators Inflamm.
2012:5163952012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liu F, Lang R, Zhao J, Zhang X, Pringle
GA, Fan Y, Yin D, Gu F, Yao Z and Fu L: CD8+ cytotoxic T
cell and FOXP3+ regulatory T cell infiltration in
relation to breast cancer survival and molecular subtypes. Breast
Cancer Res Treat. 130:645–655. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rabinovich GA, Gabrilovich D and Sotomayor
EM: Immunosuppressive strategies that are mediated by tumor cells.
Annu Rev Immunol. 25:267–296. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Clatot F, Picquenot JM, Choussy O,
Gouérant S, Moldovan C, Schultheis D, Cornic M, François A, Blot E
and Laberge-Le-Couteulx S: Intratumoural level of SDF-1 correlates
with survival in head and neck squamous cell carcinoma. Oral Oncol.
47:1062–1068. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Strauss L, Bergmann C, Szczepanski M,
Gooding W, Johnson JT and Whiteside TL: A unique subset of
CD4+CD25highFoxp3+ T cells secreting interleukin-10 and
transforming growth factor-beta1 mediates suppression in the tumor
microenvironment. Clin Cancer Res. 13:4345–4354. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Whiteside TL: The tumor microenvironment
and its role in promoting tumor growth. Oncogene. 27:5904–5912.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nguyen N, Bellile E, Thomas D, McHugh J,
Rozek L, Virani S, Peterson L, Carey TE, Walline H, Moyer J, et al:
Tumor infiltrating lymphocytes and survival in patients with head
and neck squamous cell carcinoma. Head Neck. 38:1074–1084. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Halama N, Michel S, Kloor M, Zoernig I,
Benner A, Spille A, Pommerencke T, von Knebel DM, Folprecht G,
Luber B, et al: Localization and density of immune cells in the
invasive margin of human colorectal cancer liver metastases are
prognostic for response to chemotherapy. Cancer Res. 71:5670–5677.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Badoual C, Hans S, Rodriguez J, Peyrard S,
Klein C, Agueznay Nel H, Mosseri V, Laccourreye O, Bruneval P,
Fridman WH, et al: Prognostic value of tumor-infiltrating CD4+
T-cell subpopulations in head and neck cancers. Clin Cancer Res.
12:465–472. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zou L, Barnett B, Safah H, Larussa VF,
Evdemon-Hogan M, Mottram P, Wei S, David O, Curiel TJ and Zou W:
Bone marrow is a reservoir for CD4+CD25+ regulatory T cells that
traffic through CXCL12/CXCR4 signals. Cancer Res. 64:8451–8455.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Obermajer N, Muthuswamy R, Odunsi K,
Edwards RP and Kalinski P: PGE(2)-induced CXCL12 production and
CXCR4 expression controls the accumulation of human MDSCs in
ovarian cancer environment. Cancer Res. 71:7463–7470. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zboralski D, Hoehlig K, Eulberg D,
Frömming A and Vater A: increasing tumor-infiltrating T cells
through inhibition of CXCL12 with NOX-A12 synergizes with PD-1
blockade. Cancer Immunol Res. 5:950–956. 2017. View Article : Google Scholar : PubMed/NCBI
|