Introduction
Esophageal carcinoma (EC) is one of the most fatal
and prevalent human malignancies worldwide, that due to its rapidly
increasing incidence, it has gained worldwide attention (1). Esophageal squamous cell carcinoma
(ESCC) is the most lethal pathological type, accounting for ~90% of
total EC cases, and China alone contributes to more than half of
the global ESCC cases (2). At
present, surgery is the main treatment for EC, but the 5-year
survival rate after simple surgery is 31–55% (3). Most patients have lymph node
involvement and distant metastases after esophagectomy and the
5-year survival rate of ESCC patients with metastasis is only 5–47%
(4–6). Moreover, locoregional recurrence and
distant metastasis are the most common cause of treatment failure
(7). The most common recurrence
sites include the anastomosis and regional lymph nodes, which lead
to a relatively poorer prognosis (8,9). The
overall 2-year post-recurrence survival rate is 12.6%, and the
median postoperative survival is 6 months for patients with
postoperative recurrence of ESCC (10). Significant difficulty is often
encountered in identifying the appropriate treatment method from
the limited available treatment options for recurrence following
resection.
Recent advances in radiation techniques and
chemotherapy may lead to the improvement of the treatment outcomes
of postoperatively recurrent ESCC. Three-dimensional conformal
radiotherapy (3D-CRT)-based concurrent chemoradiotherapy (CCRT) has
been reportedly effective against the recurrence of ESCC after
radical surgery (9). 3D-CRT for
lymph node stations near ESCC with involved-field irradiation may
deliver considerable doses of incidental nodal irradiation and
promote the elimination of subclinical lesions (11). Intensity-modulated radiotherapy
(IMRT), a more advanced form of 3D-CRT, is a high-precision
conformal technique that allows physicians to modulate the
intensity of the radiation and apply high-radiation doses to the
tumor (12). Postoperative
precautionary IMRT has high local control rate and acceptable
side-effects on thoracic ESCC (13).
In this study, we evaluated the survival of ESCC patients that
received IMRT for the treatment of postoperative recurrence and
evaluated the prognostic factors affecting survival.
Patients and methods
Acquisition of clinical data
A total of 137 ESCC patients, who received IMRT for
postoperative locoregional recurrence at The First Affiliated
Hospital of Nanjing Medical University (Nanjing, China) from August
2003 to January 2018, were retrospectively studied. Locoregional
recurrence was defined as anastomotic or lymph node recurrence and
was confirmed by enhanced computed tomography (CT) and biopsy under
endoscopy, respectively. All patients were diagnosed with ESCC by
postoperative pathology and distant metastasis was ruled out by
imaging. The study was approved by the Ethics Committee of The
First Affiliated Hospital of Nanjing Medical University. Patients
who participated in this research had complete clinical data.
Signed informed consents were obtained from the patients or their
guardians.
Clinical data of postoperative tumor recurrence were
collected including sex and age, previous treatment (neoadjuvant
therapy, postoperative radiotherapy (PORT), and/or chemotherapy),
grades of differentiation, primary esophageal tumor location, TNM
staging, number and diameter of metastatic lymph nodes, recurrence
sites, CCRT, death from recurrence, gross tumor volume (GTV), and
survival time after recurrence.
Treatment and follow-up
assessment
IMRT was performed according to the standard program
in our Department. Briefly, patients were fixed in position with a
thermoplastic immobilizer. For treatment simulation and planning
purposes, CT scanning images were obtained to determine the
radiation treatment plan and target volume. The CT scan range
included the full mediastinum, lower neck, and upper abdomen, with
a layer spacing of 5 mm. The images were transmitted to the IMRT
treatment planning system and the attending physician's outline of
the GTV was reviewed by the chief physician. The GTV included
positive lymph nodes based on CT and positron emission tomography
(PET), including swollen lymph nodes identified by physical
examination and positive lymph nodes shown by PET-CT. The clinical
target volume (CTV) was defined as the GTV plus a 1–1.5 cm radial
margin, including high-risk regional lymph nodes. The planning
target volume (PTV) contained a 0.5-cm extension on the basis of
the CTV. The reference dose point was located at the central part
of the GTV and was optimized using a dose volume histogram with a
95% isodose curve covering the PTV. The treatment plan was reviewed
and confirmed by the chief physician. In this study, the median
dose of radiation therapy was 62.2 Gy (range, 40–80 Gy). The X-ray
irradiation energy was 6 MV administered 5 times/week with a test
dose of 2 Gy each time. The maximum doses to the endangered organs,
the lungs, and spine were V20≤25%, V30≤20%,
and ≤45 Gy, respectively.
Intravenous or oral chemotherapy, CCRT, continuous
chemoradiotherapy, radiotherapy alone or chemotherapy dose were
taken into account according to the patient's age, general
condition, Karnofsky Performance Status (KPS) score, treatment
tolerance and compliance. Follow-up data included physical
examinations, such as clinical evaluations and CT scans every 3
months. Tumor-related deaths were documented.
Statistical analysis
Statistical analysis was performed using IBM SPSS
19.0 software (IBM Corp.). Quantitative data were expressed as the
mean ± standard deviation (SD) or median (interquartile range),
while qualitative data were expressed as numbers and percentages.
The mean/median survival times with 95% CIs at different levels
were assessed by the Kaplan-Meier method (14). Univariate analyses using Kaplan-Meier
survival curves and log-rank tests were performed to assess whether
there was a significant association between demographic and
clinical features, such as sex, age, postoperative treatment, and
degree of differentiation, and death after recurrence. Statistical
significance was determined using the conventional P<0.05
criterion. For multivariate analysis, the statistically significant
results from the Kaplan-Meier method were subjected to Cox
regression analysis (15), which was
used to analyze the effect of multiple variables on survival
time.
Results
Patient characteristics
The clinical and pathological characteristics of the
patients are presented in Tables I
and II. Between 2003 and 2018, a
total of 109 male and 28 female patients were included, with an
average age of 62.22±6.56 years (range, 44–82 years). Ninety-seven
patients (70.8%) were ≥60 years of age. A total of 43.8% of
patients received PORT and/or chemotherapy or neoadjuvant therapy.
Based on TNM staging, 38 (27.7%), 53 (38.7%), and 46 (33.6%)
patients had stage I, II, and III ESCC, respectively. The locations
of the primary ESCCs removed by radical resection included the
upper, middle, and lower thoracic esophagus in 14 (10.2%), 67
(48.9%), and 56 (40.9%) patients, respectively. There were 21
(15.3%), 58 (42.3%), 36 (26.3%), 3 (2.2%), 17 (12.4%), and 2 (1.5%)
recurrences in the anastomotic, supraclavicular, mediastinal, tumor
bed, polyregional, and abdominal regions, respectively. Ninety-four
patients underwent CCRT. The median GTV of radiation was 27.06
cm3 with interquartile range (14.03, 70.48)
cm3. The analysis showed that the average survival time
after recurrence was 18.83±14.71 months. Of the 137 patients who
underwent IMRT, 84 (61.3%) died. As shown in Table III, the 2-year survival rates of
patients with anastomotic, supraclavicular, and mediastinal lymph
node recurrence were 36.4, 41.4, and 37.5%, respectively. The
2-year survival rates of patients with 0, 1, and 2–6 lymph node
recurrences were 38.9, 50.8, and 19.7%, respectively, and the
2-year survival rates for patients with and without CCRT were 41.2
and 34.9%, respectively.
 | Table I.Patient characteristics (qualitative
variables). |
Table I.
Patient characteristics (qualitative
variables).
| Characteristics | No. of patients | Constituent ratio
(%) |
|---|
| Sex |
|
Males | 109 | 79.6 |
|
Females | 28 | 20.4 |
| Age (years) |
|
<60 | 40 | 29.2 |
| ≥60 | 97 | 70.8 |
| Postoperative
therapy |
| No | 77 | 56.2 |
|
Radiotherapy | 11 | 8.0 |
|
Chemotherapy | 34 | 24.8 |
|
Radiotherapy and
chemotherapy | 13 | 9.5 |
|
Neoadjuvant therapy | 2 | 1.5 |
| Differentiation
grades |
| Poor | 56 | 40.9 |
|
Moderate | 76 | 55.5 |
| Well | 3 | 2.2 |
|
Unknown | 2 | 1.5 |
| Primary tumor
location |
|
Upper | 14 | 10.2 |
|
Middle | 67 | 48.9 |
|
Lower | 56 | 40.9 |
| TNM staging |
| I | 38 | 27.7 |
| II | 53 | 38.7 |
| III | 46 | 33.6 |
| No. of lymph
nodes |
|
None | 24 | 17.5 |
| 1 | 63 | 46.0 |
|
2–6 | 15 | 10.9 |
|
Fusion | 35 | 25.5 |
| Recurrence
sites |
|
Anastomotic | 21 | 15.3 |
|
Supraclavicular lymph
nodes | 58 | 42.3 |
|
Mediastinal lymph nodes | 36 | 26.3 |
| Tumor
bed | 3 |
2.2 |
|
Polyregional lymph nodes | 17 | 12.4 |
|
Abdominal lymph nodes | 2 | 1.5 |
| CCRT |
|
Yes | 94 | 68.6 |
| No | 43 | 31.4 |
| Death |
|
Yes | 84 | 61.3 |
| No | 53 | 38.7 |
| Table II.Patient characteristics (quantitative
variables). |
Table II.
Patient characteristics (quantitative
variables).
|
Characteristics | Values | Range |
|---|
| Age (years) | 62.22±6.56 | 44–82 |
| Lymph node diameter
(cm) |
2.73±1.88 |
0-7.9 |
| GTV
(cm3) | 27.06 (14.03,
70.48) | 1.73–385.6 |
| Survival time after
recurrence (months) | 18.83±14.71 | 2–81 |
| Table III.Kaplan-Meier analysis of risk factors
related to death after tumor recurrence. |
Table III.
Kaplan-Meier analysis of risk factors
related to death after tumor recurrence.
|
Characteristics | Median (95%
CI) | P-value
(log-rank) | 1-year survival
rate (%) | 2-year survival
rate (%) | 3-year survival
rate (%) | 5-year survival
rate (%) |
|---|
| Sex |
| 0.160 |
|
|
|
|
|
Male | 28.48 (22.13,
34.82) |
| 65.1 | 34.9 | 25.3 | 13.5 |
|
Female | 36.85 (23.58,
50.12) |
| 68.0 | 57.7 | 43.2 | – |
| Age (years) |
| 0.169 |
|
|
|
|
|
<60 | 27.90 (17.33,
38.48) |
| 50.2 | 30.4 | – | 15.2 |
|
≥60 | 30.46 (24.24,
36.68) |
| 75.5 | 42.6 | 28.2 | – |
| Diameter of nodes
(cm) |
| 0.184 |
|
|
|
|
| <2.6
(n=66) | 29.76 (22.52,
37.00) |
| 73.7 | 43.3 | 29.5 | 11.1 |
| ≥2.6
(n=71) | 29.00 (20.96,
37.03) |
| 62.9 | 35.0 | – | 18.2 |
| GTV
(cm3) |
| 0.013 |
|
|
|
|
| <27
(n=68) | 35.76 (27.44,
44.09) |
| 72.7 | 51.5 | 37.1 | 25.9 |
| ≥27
(n=69) | 22.48 (16.98,
27.98) |
| 63.7 | 26.9 | 17.9 |
0.0 |
| Postoperative
therapy |
| 0.286 |
|
|
|
|
| No | 32.40 (25.24,
39.55) |
| 71.0 | 47.1 | 37.7 | 16.2 |
|
Radiotherapy | 21.69 (16.36,
27.02) |
| – | 35.1 | – | – |
|
Chemotherapy | 25.41 (15.51,
35.31) |
| 56.8 | 27.1 | 17.0 | – |
|
Radiotherapy and
chemotherapy | 16.00 (10.08,
21.92) |
| 38.5 | – | – | – |
| Grades of
differentiation |
| 0.689 |
|
|
|
|
|
Poorly | 30.48 (21.75,
39.20) |
| 65.3 | 44.0 | 30.0 | 20.0 |
|
Moderately | 29.90 (21.93,
37.87) |
| 69.6 | 39.7 | 31.2 | 12.5 |
|
Well | 18.67 (15.82,
21.51) |
| 66.7 | – | – | – |
| Primary tumor
location |
| 0.162 |
|
|
|
|
|
Upper | 29.82 (17.60,
42.04) |
| 71.4 | 53.6 | – | – |
|
Middle | 30.85 (23.18,
38.52) |
| 75.2 | 43.7 | 28.1 | 14.1 |
|
Lower | 26.70 (18.86,
34.55) |
| 58.9 | 29.1 | – | – |
| TNM staging |
| 0.222 |
|
|
|
|
| I | 24.64 (18.24,
31.04) |
| 71.1 | 37.8 | 21.6 | – |
| II | 32.70 (24.67,
40.74) |
| 74.4 | 49.2 | – | 13.1 |
|
III | 27.60 (17.78,
37.43) |
| 57.7 | 27.4 | – | – |
| Location of lymph
nodes |
| 0.073 |
|
|
|
|
| No | 23.86 (16.12,
31.59) |
| 62.5 | 38.9 | 15.6 | – |
|
Supraclavicular lymph
nodes | 31.55 (23.61,
39.48) |
| 69.4 | 40.9 | – | 18.2 |
|
Mediastinal lymph nodes | 37.85 (24.05,
51.66) |
| 74.0 | 53.2 | 39.9 | – |
|
Polyregional lymph nodes | 13.40 (8.42,
18.39) |
| 53.3 | – | – | – |
| No. of lymph
nodes |
| 0.025 |
|
|
|
|
|
None | 23.86 (16.12,
31.59) |
| 62.5 | 38.9 | 15.6 | – |
| 1 | 38.74 (29.28,
31.59) |
| 77.3 | 50.8 | 38.1 | – |
|
2–6 | 25.56 (10.70,
40.42) |
| 63.2 | 19.7 | – | – |
|
Fusion | 21.66 (13.72,
29.60) |
| 54.0 | – | – |
0.0 |
| Recurrence
sites |
| 0.838 |
|
|
|
|
|
Anastomotic | 23.25 (15.39,
31.12) |
| 61.9 | 36.4 | 14.5 | – |
|
Supraclavicular lymph
nodes | 32.03 (23.82,
40.24) |
| 71.1 | 41.4 | – | 18.4 |
|
Mediastinal lymph nodes | 29.44 (18.19,
40.70) |
| 58.5 | 37.5 | 28.2 | – |
|
Polyregional lymph nodes | 18.45 (13.33,
23.57) |
| 70.1 | – | – | – |
| CCRT |
| 0.513 |
|
|
|
|
| No | 30.63 (20.81,
40.45) |
| 55.3 | 34.9 | – | – |
|
Yes | 28.78 (22.46,
35.10) |
| 74.5 | 41.2 | 28.5 |
7.9 |
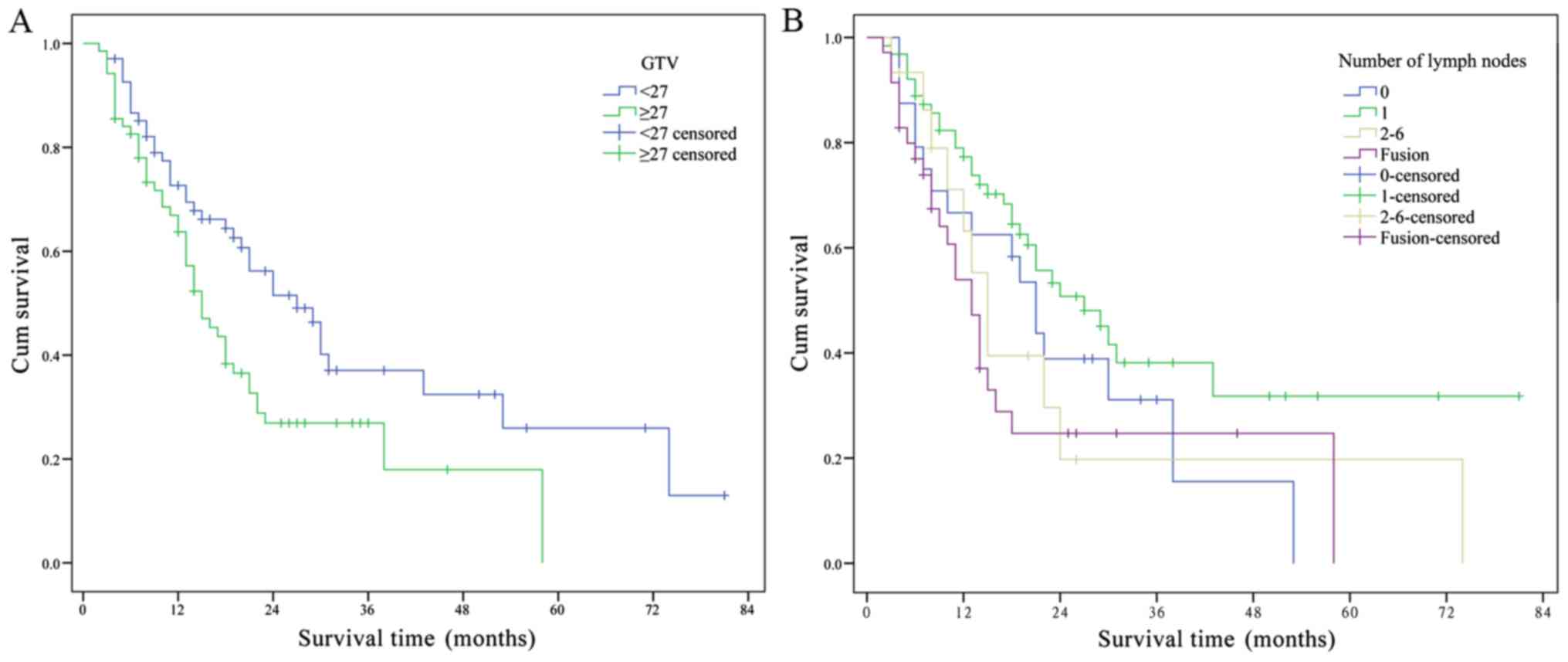
Univariate analysis showed that the GTV of radiation
(<27 vs. ≥27 cm3) and the number of lymph nodes were
significantly related to survival. Other factors, such as
differentiation grade and recurrence site, were not related to
survival (Table III, Fig. 1). The 1-, 2-, 3-, and 5-year survival
rates of patients with GTV<27 cm3 were 72.7, 51.5,
37.1, and 25.9%, respectively, and with GTV≥27 cm3 were
63.7, 26.9, 17.9, and 0%, respectively. Multivariate regression
analysis with a Cox model showed that the GTV of radiation was a
significant independent prognostic factor and was significantly
related to the risk of death after recurrence [HR (95% CI), 1.746
(1.112–2.741); P=0.016] (Table IV).
According to the results, the risk of death for patients with
GTV≥27 cm3 was 1.746 times that for patients with
GTV<27 cm3, with a statistically significant
difference.
| Table IV.Multivariate regression model
analysis of risk factors related to death after tumor
recurrence. |
Table IV.
Multivariate regression model
analysis of risk factors related to death after tumor
recurrence.
|
|
|
| 95.0% CI for
HR |
|---|
|
|
|
|
|
|---|
| Factors | P-value | HR | Lower | Upper |
|---|
| GTV | 0.016 | 1.746 | 1.112 | 2.741 |
| No. of lymph
nodes | 0.813 | 1.068 | 0.616 | 1.853 |
Discussion
Currently, surgery is the primary treatment for
ESCC. However, the overall recurrence rate of ESCC patients after
radical resection ranges from 34 to 79%, while the rate of
locoregional recurrence is 21–68% (16,17).
Evidence has indicated that the number of lymph nodes involved and
the depth of primary tumor invasion may help in evaluating the
recurrence risk in ESCC patients following curative surgery
(17). EC guidelines for the
national comprehensive cancer network (NCCN) suggest that some
patients with local recurrence after surgery can tolerate CCRT
(18,19). Approximately 28% of patients with
ESCC achieved long-term survival with the use of CRT for lymph node
recurrence after curative resection (20). Current radiation techniques using
3D-CRT with enhanced accuracy using daily image guidance have
improved the accuracy of irradiation (21). The incidental irradiation doses with
involved-field irradiation have significantly impacted the control
of micro-metastasis and may contribute to the elimination of
subclinical ESCC lesions (11). It
has been reported that the tolerance to 3D-CRT combined with
chemotherapy is better than that of the simple 3D-CRT, which is a
feasible technology and can improve the overall survival (OS) rate
of patients with recurrent ESCC mediastinal lymph node metastasis
after surgery (22). In the present
study, ESCC patients with anastomotic or lymph node recurrence
received IMRT or IMRT-based CCRT and the factors affecting their
survival were investigated.
Previous studies have indicated that the number and
regions of lymph node recurrences after ESCC are also important
factors influencing the efficacy of salvage chemoradiotherapy
(23). Jingu et al reported
that the median OS rates of single and multiple recurrent regions
after EC surgery were 39.0 and 6.5 months, respectively, after
radiotherapy and chemotherapy, and the number of recurrent lesions
was a significant prognostic factor (23). Miyata et al reported that the
OS rate of patients with ≥4 recurrent lymph nodes after ESCC
surgery was significantly lower than that in patients with <4
recurrent lymph nodes (24). Chen
et al reported 5-year OS rates for 1–2, 3–6, and ≥7
recurrent lymph nodes after ESCC resection of 33, 17, and 12%,
respectively, and patients with more recurrent lymph nodes had
worse prognoses (25). In the
current study, although Kaplan-Meier analysis showed that the
number of lymph nodes was a risk factor related to death after
tumor recurrence, multivariate regression model analyses showed
that the number of lymph nodes was not an independent prognostic
factor.
The risk factor GTV of radiation was a significant
independent prognostic factor for survival after recurrence in
patients receiving IMRT treatment. The GTVs were contoured as
visible tumors on CT scans (26).
Most of the lymphatic recurrences after surgery among patients
diagnosed with ESCC would have been covered by the proposed PORT
CTV (21). The GTV has been
demonstrated to be an independent prognostic factor for survival in
multiple cancers treated with radiation therapy (27,28). Ma
et al reported that the GTV of radiation (≥5 vs. <5
cm3) was an important independent prognostic factor in
patients with recurrent ESCC (22).
However, this study confirmed that GTV of radiation (<27 vs. ≥27
cm3) is an important independent prognostic factor for
the risk of death after recurrence treated by IMRT.
This study has several limitations. Its
retrospective design may have a potential bias. In addition,
because of the different doses and schedule used in this study, the
optimal treatment for locoregional recurrence has not been
determined.
In conclusion, our retrospective study showed that
the GTV of radiation is an independent prognostic factor in ESCC
patients with postoperative locoregional recurrence. Patients with
a GTV≥27 cm3 have a higher risk of death.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the National
Natural Science Foundation of China (nos. 81703028, 81472809,
81502653 and 81672983). We would like to thank everyone involved
for their support, and the patients who participated in this
study.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YS and XG performed the retrospective analyses and
wrote the manuscript. ZG and SL performed the statistical analysis
and revised the manuscript. XS and JL designed the study. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The First Affiliated Hospital of Nanjing Medical University
(Nanjing, China). Patients who participated in this research had
complete clinical data. Signed informed consents were obtained from
the patients or their guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
Statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zeng H, Zheng R, Zhang S, Zuo T, Xia C,
Zou X and Chen W: Esophageal cancer statistics in China, 2011:
Estimates based on 177 cancer registries. Thorac Cancer. 7:232–237.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yao J, Shen X, Li H, Xu J, Shao S, Huang
JX and Lin M: LncRNA- ECM is overexpressed in esophageal squamous
cell carcinoma and promotes tumor metastasis. Oncol Lett.
16:3935–3942. 2018.PubMed/NCBI
|
|
4
|
Kayani B, Zacharakis E, Ahmed K and Hanna
GB: Lymph node metastases and prognosis in oesophageal carcinoma -
a systematic review. Eur J Surg Oncol. 37:747–753. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bai Y, Lin H, Fang Z, Luo Q, Fang Y, Su Y,
Hu Q, Duan H, Chen F and Zhang ZY: Plasma microRNA-19a as a
potential biomarker for esophageal squamous cell carcinoma
diagnosis and prognosis. Biomarkers Med. 11:431–441. 2017.
View Article : Google Scholar
|
|
6
|
Wu SG, Zhang WW, He ZY, Sun JY, Chen YX
and Guo L: Sites of metastasis and overall survival in esophageal
cancer: A population-based study. Cancer Manag Res. 9:781–788.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kato H, Fukuchi M, Miyazaki T, Nakajima M,
Kimura H, Faried A, Sohda M, Fukai Y, Masuda N, Manda R, et al:
Classification of recurrent esophageal cancer after radical
esophagectomy with two- or three-field lymphadenectomy. Anticancer
Res. 25:3461–3467. 2005.PubMed/NCBI
|
|
8
|
Doki Y, Ishikawa O, Takachi K, Miyashiro
I, Sasaki Y, Ohigashi H, Murata K, Yamada T, Noura S, Eguchi H, et
al: Association of the primary tumor location with the site of
tumor recurrence after curative resection of thoracic esophageal
carcinoma. World J Surg. 29:700–707. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bao Y, Liu S, Zhou Q, Cai P, Anfossi S, Li
Q, Hu Y, Liu M, Fu J, Rong T, et al: Three-dimensional conformal
radiotherapy with concurrent chemotherapy for postoperative
recurrence of esophageal squamous cell carcinoma: Clinical efficacy
and failure pattern. Radiat Oncol. 8:2412013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hsu PK, Wang BY, Huang CS, Wu YC and Hsu
WH: Prognostic factors for post-recurrence survival in esophageal
squamous cell carcinoma patients with recurrence after resection. J
Gastrointest Surg. 15:558–565. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ji K, Zhao L, Yang C, Meng M and Wang P:
Three-dimensional conformal radiation for esophageal squamous cell
carcinoma with involved-field irradiation may deliver considerable
doses of incidental nodal irradiation. Radiat Oncol. 7:2002012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gupta T, Agarwal J, Jain S, Phurailatpam
R, Kannan S, Ghosh-Laskar S, Murthy V, Budrukkar A, Dinshaw K,
Prabhash K, et al: Three-dimensional conformal radiotherapy
(3D-CRT) versus intensity modulated radiation therapy (IMRT) in
squamous cell carcinoma of the head and neck: A randomized
controlled trial. Radiother Oncol. 104:343–348. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang W, Liu X, Xiao Z, Wang L, Zhang H,
Chen D, Zhou Z, Feng Q, Hui Z, Liang J, et al: Efficacy of
intensity-modulated radiotherapy for resected thoracic esophageal
squamous cell carcinoma. Thorac Cancer. 6:597–604. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jager KJ, van Dijk PC, Zoccali C and
Dekker FW: The analysis of survival data: The Kaplan-Meier method.
Kidney Int. 74:560–565. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ni A and Cai J: Tuning parameter selection
in Cox proportional hazards model with a diverging number of
parameters. Scand Stat Theory Appl. 45:557–570. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dresner SM and Griffin SM: Pattern of
recurrence following radical oesophagectomy with two-field
lymphadenectomy. Br J Surg. 87:1426–1433. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu Y, Chen Q, Yu X, Zhou X, Zheng X and
Mao W: Factors influencing the risk of recurrence in patients with
esophageal carcinoma treated with surgery: A single institution
analysis consisting of 1002 cases. Oncol Lett. 5:185–190. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nakamura T, Hayashi K, Ota M, Eguchi R,
Ide H, Takasaki K and Mitsuhashi N: Salvage esophagectomy after
definitive chemotherapy and radiotherapy for advanced esophageal
cancer. Am J Surg. 188:261–266. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nemoto K, Ariga H, Kakuto Y, Matsushita H,
Takeda K, Takahashi C, Takai Y, Yamada S and Hosoi Y: Radiation
therapy for loco-regionally recurrent esophageal cancer after
surgery. Radiother Oncol. 61:165–168. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kawamoto T, Nihei K, Sasai K and Karasawa
K: Clinical outcomes and prognostic factors of chemoradiotherapy
for postoperative lymph node recurrence of esophageal cancer. Jpn J
Clin Oncol. 48:259–264. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Liu Q, Cai XW, Wu B, Zhu ZF, Chen HQ and
Fu XL: Patterns of failure after radical surgery among patients
with thoracic esophageal squamous cell carcinoma: Implications for
the clinical target volume design of postoperative radiotherapy.
PLoS One. 9:e972252014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ma DY, Tan BX, Liu M, Li XF, Zhou YQ and
Lu Y: Concurrent three-dimensional conformal radiotherapy and
chemotherapy for postoperative recurrence of mediastinal lymph node
metastases in patients with esophageal squamous cell carcinoma: A
phase 2 single-institution study. Radiat Oncol. 9:282014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jingu K, Matsushita H, Takeda K, Umezawa
R, Takahashi C, Sugawara T, Kubozono M, Abe K, Tanabe T, Shirata Y,
et al: Long-term results of radiotherapy combined with nedaplatin
and 5-fluorouracil for postoperative loco-regional recurrent
esophageal cancer: Update on a phase II study. BMC Cancer.
12:5422012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Miyata H, Yamasaki M, Kurokawa Y,
Takiguchi S, Nakajima K, Fujiwara Y, Konishi K, Mori M and Doki Y:
Survival factors in patients with recurrence after curative
resection of esophageal squamous cell carcinomas. Ann Surg Oncol.
18:3353–3361. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chen XL, Chen TW, Fang ZJ, Zhang XM, Li
ZL, Li H, Tang HJ, Zhou L, Wang D and Zhang Z: Patterns of lymph
node recurrence after radical surgery impacting on survival of
patients with pT1-3N0M0 thoracic esophageal squamous cell
carcinoma. J Korean Med Sci. 29:217–223. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Huang Y, Chen S-W, Fan C-C, Ting L-L, Kuo
C-C and Chiou J-F: Clinical parameters for predicting
radiation-induced liver disease after intrahepatic reirradiation
for hepatocellular carcinoma. Radiat Oncol. 11:892016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Basaki K, Abe Y, Aoki M, Kondo H, Hatayama
Y and Nakaji S: Prognostic factors for survival in stage III
non-small-cell lung cancer treated with definitive radiation
therapy: Impact of tumor volume. Int J Radiat Oncol Biol Phys.
64:449–454. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhu D, Ma T, Niu Z, Zheng J, Han A, Zhao S
and Yu J: Prognostic significance of metabolic parameters measured
by (18)F-fluorodeoxyglucose positron emission tomography/computed
tomography in patients with small cell lung cancer. Lung Cancer.
73:332–337. 2011. View Article : Google Scholar : PubMed/NCBI
|