Introduction
Thyroid cancer, a common malignancy of head and
neck, has a high incidence of 56 cases per 100,000 persons that,
ranks first in systemic endocrine tumors, and its incidence in
females is higher than that in males (1,2). In
recent years, due to the deterioration of the environment and the
accelerated pace of life, the incidence of thyroid cancer has
increased posing a great threat to human life (3).
The tumor cells of thyroid cancer are derived from
thyroid epithelial cells, and thyroid cancer has a high incidence
and less obvious clinical symptoms in the early stage, so its early
diagnosis is also increasingly important (4). At present, the thyroid nodule is often
detected by FNA, isotope scanning and ultrasound in clinical
practice (5). Ultrasound detection
has the advantages of low price, non-invasiveness, simple operation
and good resolution and commonly used in the examination of thyroid
lesion clinically (6). It also
provides detailed data and description on the size, location and
morphology of the nodule during the examination of the thyroid
nodule, and explores some clinically untouched nodules, which has a
certain value in the early diagnosis of thyroid cancer (7). According to the research report of Niu
et al (8), ultrasound can
find the smallest thyroid nodule with a diameter of 1 mm, and show
the structure, envelope and calcification of the nodule with a
diameter of 2 mm in detail. However, the polypathia of some nodules
leads to the overlapping of ultrasound images, which causes
ultrasound to have certain limitations and deficiencies for the
diagnosis of benign and malignant small thyroid nodules. Because of
its diagnostic safety, minimal invasiveness and good accuracy, FNA
is currently considered to be the most effective method for the
clinical diagnosis of thyroid malignancies in addition to
pathological examination (9). At
present, there are 6 classification criteria for FNA in the
diagnosis of thyroid cancer, including undiagnosed, benign lesion,
follicular lesion, follicular neoplasm, possibly malignancy and
malignant lesion. However, the difference in the operation
technique and experience in the diagnosis leads to missed
diagnosis, misdiagnosis, and differences in the diagnosis results
and pathological examination (10,11).
At present, there are few studies on FNA combined
with ultrasound in the diagnosis of thyroid cancer, which was
therefore explored in this study, in order to find a more accurate
method for the diagnosis of thyroid cancer and provide a more
accurate diagnostic reference.
Patients and methods
Basic information
A retrospective analysis was performed on 165
thyroid nodule patients in Liaocheng People's Hospital (Liaocheng,
China) from July 2014 to July 2017, and all patients underwent
ultrasound and FNA examinations. The average age was 35.9±8.7
years. The patients evaluated in this study were thyroid tumor
patients including patients with malignant and benign tumors. There
were 147 patients with thyroid malignant tumors, including 119
patients with papillary carcinoma, 14 patients with follicular
carcinoma, 8 patients with undifferentiated carcinoma and 6
patients with medullary carcinoma. Another 18 patients had thyroid
benign tumors, including 13 patients with nodular goiter, 3
patients with tumor nodules and 2 patients with cysts. Group A
consisted of 67 patients with a thyroid nodule diameter of ≤1 cm,
including 60 patients with malignant nodules and 7 patients with
benign nodules, and group B consisted of 98 patients with a thyroid
nodule diameter of >1 cm, including 87 patients with malignant
nodules and 11 patients with benign nodules. There were no
significant differences in sex, age and BMI between the two groups
(P>0.05) (Table I).
 | Table I.Comparison of general data between two
groups of patients [n (%)]. |
Table I.
Comparison of general data between two
groups of patients [n (%)].
| Factors | Group A (n=67) | Group B (n=98) | χ2
value | P-value |
|---|
| Sex |
|
| 0.061 | 0.805 |
| Male | 22 (32.84) | 34 (34.69) |
|
|
|
Female | 45 (67.16) | 64 (65.31) |
|
|
| Age |
|
| 0.039 | 0.844 |
| ≤40 | 27 (40.30) | 41 (41.84) |
|
|
|
>40 | 40 (59.70) | 57 (58.16) |
|
|
| BMI
(kg/m2) |
|
| 0.002 | 0.965 |
| ≤22 | 31 (46.27) | 45 (45.92) |
|
|
|
>22 | 36 (53.73) | 53 (54.08) |
|
|
| Malignant typing |
|
| 0.651 | 0.885 |
| Papillary
carcinoma | 48 (71.64) | 71 (72.45) |
|
|
|
Follicular carcinoma | 5 (7.46) | 9 (9.18) |
|
|
| Undifferentiated
carcinoma | 4 (5.97) | 4 (4.08) |
|
|
| Medullary
carcinoma | 3 (4.48) | 3 (3.06) |
|
|
| Benign typing |
|
| 0.144 | 0.931 |
| Nodular
goiter | 5 (7.46) | 8 (8.16) |
|
|
| Tumor
nodule | 1 (1.49) | 2 (2.04) |
|
|
| Cyst | 1 (1.49) | 1 (1.02) |
|
|
| Family history |
|
| 0.009 | 0.923 |
| Yes | 49 (73.13) | 71 (72.45) |
|
|
| No | 18 (26.87) | 27 (27.55) |
|
|
Inclusion and exclusion criteria
Groups A and B included patients diagnosed with
malignant or benign thyroid nodules by pathology. These patients
were aged 25 to 45 years with stable diseases and vital signs.
Patients who underwent ultrasonography and FNA were included.
Patients with non-thyroid nodules, patients with unstable diseases,
patients who had undergone radiotherapy and chemotherapy, patients
complicated with other tumors, patients with severe loss of liver
and kidney function, patients with cognitive and communication
disorders and patients who did not cooperate with the examination
were excluded. All subjects and their family members signed an
informed consent form and cooperate with medical staff to complete
relevant medical treatment. The study was approved by the Ethics
Committee of Liaocheng People's Hospital.
Experimental instruments and
materials
Ultrasound diagnosis was performed using the SIEMEAS
Acuson sequoia 512 color Doppler ultrasound diagnostic instrument
manufactured by GE Healthcare Life Sciences configured with the
LA523 high-frequency linear array probe (12 MHz). Lidocaine (2%)
for puncture and anesthesia was purchased from Changtian Pharma
Co., Ltd.; SFDA approval no. H20057825. The biopsy puncture needle
(23 Gx8 cm) was purchased from C. R. Bard.
Methods
During the ultrasound examination, the patient was
placed in a supine position with the neck raised to fully expose
it. The thyroid was scanned thoroughly and versatilely, and the
size, location, morphology and calcification of the nodule,
peripheral and internal blood flow, tissue changes, and changes in
surrounding lymph nodes were recorded. After the ultrasound
examination, the FNA detection was performed. Before the puncture,
the patient was placed in the supine position with head
overextension to fully expose the head and neck, then the routine
disinfection and drape were performed. Two percent lidocaine was
used for local anesthesia and a #7 needle was used for the negative
pressure puncture of the thyroid nodule, in order to obtain the
biopsy tissues. After that, the negative pressure was quickly
eliminated, the needle was removed and the tissues were sent for
examination. The FNA and the ultrasound results were compared with
the results of the pathological examination that were used as the
gold standard, and the diagnostic values of FNA, ultrasound and FNA
combined with ultrasound for thyroid cancer were evaluated.
According to relevant studies (12,13),
sensitivity, specificity, diagnostic coincidence rate, negative
predictive value and positive predictive value were used in this
study to evaluate the diagnostic values of FNA, ultrasound and FNA
combined with ultrasound for thyroid cancer.
Statistical analysis
The statistical software SPSS 19.0 (IBM Corp.,
Armonk, NY, USA) was used to analyze and process the research data.
χ2 test was used for the comparison of enumeration data between
groups. For frequencies <5, a Fisher's exact test was used. At
P<0.05 the difference was considered statistically
significant.
Results
Analysis of partial ultrasound images
and FNA image
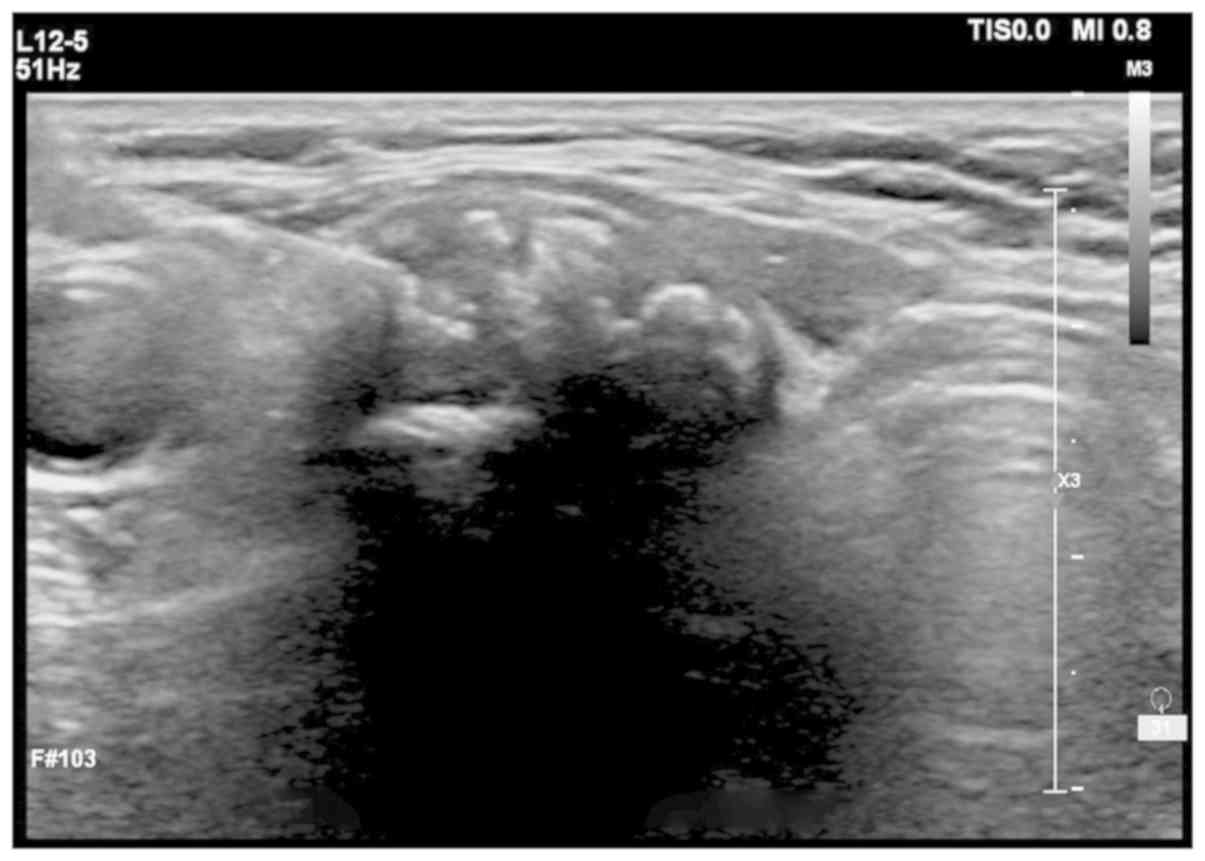
Ultrasound images: Fig.
1 shows low echo nodule of 1.4×1.3×1.1 cm detected by
ultrasound, with unclear boundary, heterogeneous internal echoes
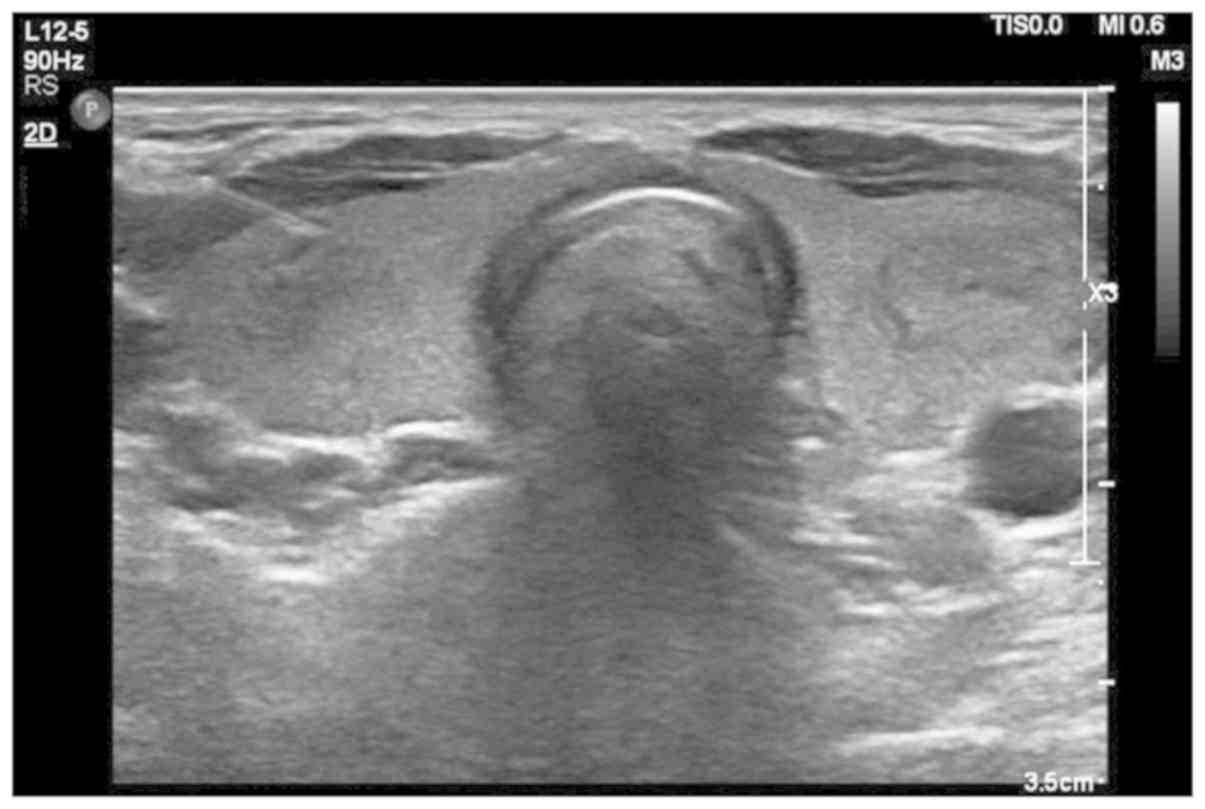
and multiple dotted high-echoes. Fig.
2 shows medium and low echo nodules detected by ultrasound,
with an echo halo on the edge and regular shape, therefore
suspected of papillary thyroid carcinoma.
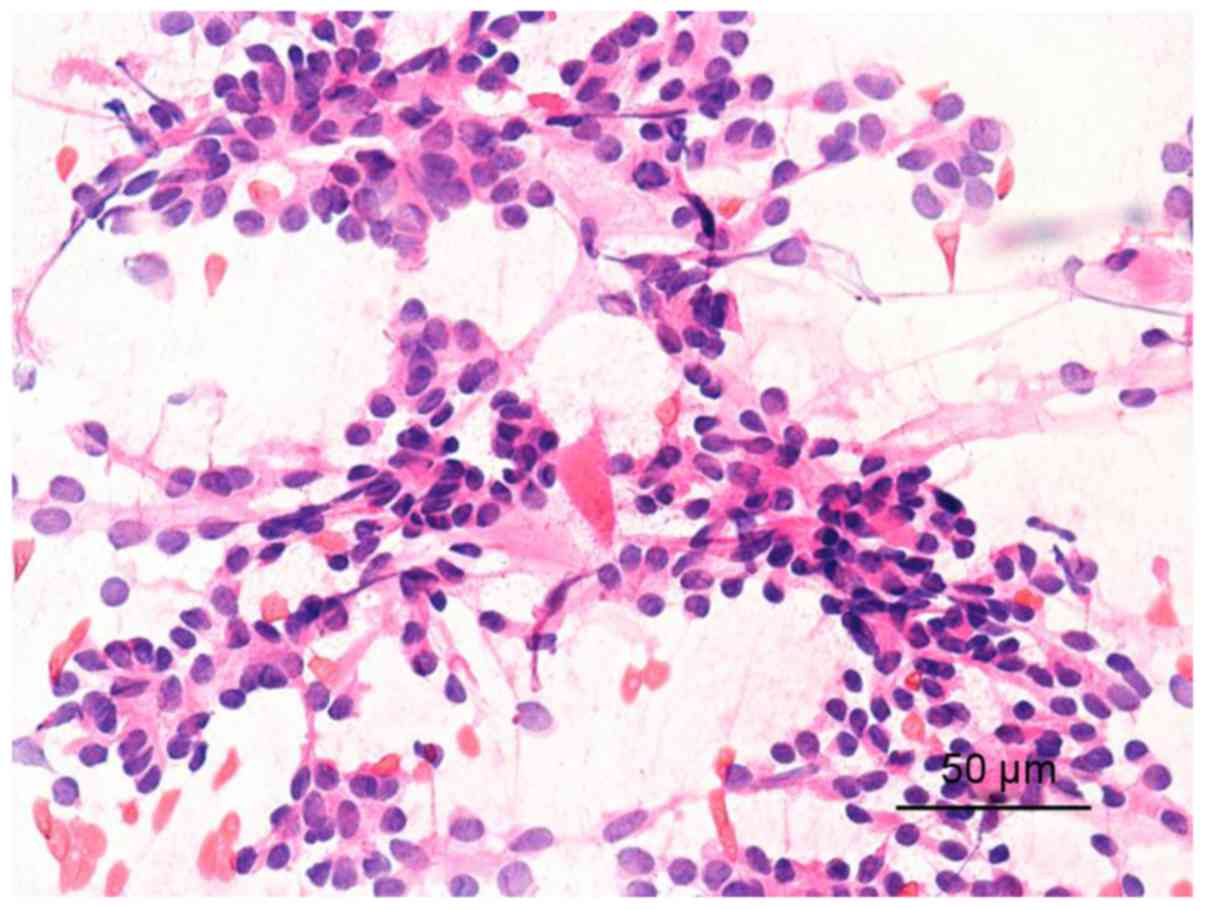
FNA image: Fig. 3
shows follicular epithelium. The cells were various in size and
crowded, with the nucleus being ground glass-like. Therefore, it
was considered as papillary thyroid carcinoma.
Comparison of diagnostic values of
ultrasound, FNA and ultrasound combined with FNA in group A
In group A, the sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of
ultrasound in the diagnosis of thyroid cancer were 86.67, 28.57,
80.60, 91.23 and 25%, respectively, those of FNA were 93.33, 71.43,
91.04, 96.55 and 55.56%, respectively, and those of FNA combined
with ultrasound were 100, 28.57, 92.54, 95.6 and 100%,
respectively. Ultrasound combined with FNA had higher sensitivity
than ultrasound and FNA alone, higher accuracy than ultrasound
alone and lower missed diagnosis rate than ultrasound and FNA
alone, with statistically significant differences (P<0.05)
(Tables II and III).
| Table II.Comparison of diagnostic values of
ultrasound and ultrasound combined with FNA in group A [n (%)]. |
Table II.
Comparison of diagnostic values of
ultrasound and ultrasound combined with FNA in group A [n (%)].
| Diagnosis | Ultrasound | Ultrasound combined
with FNA | χ2
value | P-value |
|---|
| Sensitivity | 52 (86.67) | 60 (100.00) | 8.571 | 0.003 |
|
| 8 (13.33) | 0 |
|
|
| Specificity | 2 (28.57) | 2 (28.57) | – | – |
|
| 5 (71.43) | 5 (71.43) |
|
|
| Accuracy rate | 54 (80.60) | 62 (92.54) | 4.107 | 0.043 |
|
| 13 (19.40) | 5 (7.46) |
|
|
| Positive predictive
value | 52 (91.23) | 60 (92.31) | 0.047 | 0.828 |
|
| 5 (8.77) | 6 (7.69) |
|
|
| Negative predictive
value | 2 (25.00) | 2 (100.00) | 4.800 | 0.109 |
|
| 6 (75.00) | 0 |
|
|
| Table III.Comparison of diagnostic values of
FNA and ultrasound combined with FNA in group A [n (%)]. |
Table III.
Comparison of diagnostic values of
FNA and ultrasound combined with FNA in group A [n (%)].
| Diagnosis | FNA | Ultrasound combined
with FNA | χ2
value | P-value |
|---|
| Sensitivity | 56 (93.33) | 60 (100.00) | 4.138 | 0.042 |
|
| 4 (6.67) | 0 |
|
|
| Specificity | 5 (71.43) | 2 (28.57) | 2.571 | 0.109 |
|
| 2 (28.57) | 5 (71.43) |
|
|
| Accuracy | 61 (91.04) | 62 (92.54) | 0.099 | 0.753 |
|
| 6 (8.95) | 5 (7.46) |
|
|
| Positive predictive
value | 56 (96.55) | 60 (92.31) | 1.029 | 0.311 |
|
| 2 (3.45) | 5 (7.69) |
|
|
| Negative predictive
value | 5 (55.56) | 2 (100.00) | 1.397 | 0.491 |
|
| 4 (44.44) | 0 |
|
|
Comparison of diagnostic values of
ultrasound, FNA and ultrasound combined with FNA in group B
In group B, the sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of
ultrasound in the diagnosis of thyroid cancer were 96.55, 72.73,
93.88, 96.55 and 72.73%, respectively, those of FNA were 100,
54.55, 94.90, 94.57 and 100%, respectively, and those of FNA
combined with ultrasound were 100, 63.64, 97.96, 95.92 and 100%,
respectively, without statistically significant differences in
those between FNA, ultrasound and FNA combined with ultrasound
(P>0.05) (Tables IV and V).
| Table IV.Comparison of diagnostic values of
ultrasound and ultrasound combined with FNA in group B [n (%)]. |
Table IV.
Comparison of diagnostic values of
ultrasound and ultrasound combined with FNA in group B [n (%)].
| Diagnosis | Ultrasound | Ultrasound combined
with FNA | χ2
value | P-value |
|---|
| Sensitivity | 84 (96.55) | 87 (100.00) | 3.053 | 0.081 |
|
| 3 (3.45) | 0 |
|
|
| Specificity | 8 (72.73) | 7 (63.64) | 0.210 | 0.647 |
|
| 3 (27.28) | 4 (36.37) |
|
|
| Accuracy | 92 (93.88) | 94 (97.96) | 0.422 | 0.516 |
|
| 6 (6.12) | 2 (2.04) |
|
|
| Positive predictive
value | 84 (96.55) | 87 (95.61) | 0.106 | 0.745 |
|
| 3 (3.45) | 4 (4.39) |
|
|
| Negative predictive
value | 8 (72.73) | 7 (100.00) | 2.291 | 0.245 |
|
| 3 (27.27) | 0 |
|
|
| Table V.Comparison of diagnostic values of
FNA and ultrasound combined with FNA in group B [n (%)]. |
Table V.
Comparison of diagnostic values of
FNA and ultrasound combined with FNA in group B [n (%)].
| Diagnosis | FNA | Ultrasound combined
with FNA | χ2
value | P-value |
|---|
| Sensitivity | 87 (100.00) | 87 (100.00) | – | – |
|
| 0 | 0 |
|
|
| Specificity | 6 (54.55) | 7 (63.64) | 0.188 | 0.665 |
|
| 5 (45.45) | 4 (36.37) |
|
|
| Accuracy | 93 (94.90) | 94 (97.96) | 0.117 | 0.733 |
|
| 5 (5.10) | 2 (2.04) |
|
|
| Positive predictive
value | 87 (94.57) | 87 (95.92) | 0.106 | 0.745 |
|
| 5 (5.43) | 4 (4.08) |
|
|
| Negative predictive
value | 6 (100.00) | 7 (100.00) | – | – |
|
| 0 | 0 |
|
|
Discussion
As the most common thyroid malignant tumor, thyroid
cancer accounts for ~1% of systemic malignant tumors and occurs in
patients at any age, with a higher incidence in females than in
males (14). In most cases, thyroid
cancer occurs on one side of the thyroid gland and is a single
tumor (11). In clinical practice,
the early clinical manifestations of thyroid cancer are similar to
those of benign thyroid nodules, which are mainly lumps in the
thyroid, difficult breathing, swallowing obstruction and
hoarseness, so thyroid cancer is easily misdiagnosed as a benign
nodule. Therefore, the malignant lesion should be detected and
excluded for each thyroid nodule patient (15,16). The
most common pathological type of thyroid cancer is papillary
adenocarcinoma that accounts for ~70%, followed by follicular
adenocarcinoma, medullary carcinoma and undifferentiated carcinoma
(17). At present, the key to the
treatment of thyroid cancer remains how to make the early diagnosis
and intervention therapy (18).
Ultrasound, which is commonly used in clinical practice, is an
auxiliary diagnostic method of thyroid cancer, but the ultrasound
images of thyroid cancer are overlapping and diverse, so ultrasound
has a high misdiagnosis rate of atypical and early thyroid cancers
(19). Simple to operate and
relatively safe, FNA has higher sensitivity and accuracy and is
currently considered to be effective for detecting thyroid cancer
worldwide (20). However, the
diagnosis of some nodules by FNA such as follicular adenocarcinomas
is unclear (21). Therefore, in this
study, the diagnostic value of FNA combined with ultrasound for
thyroid cancer was explored, in order to provide a more accurate
diagnostic method of thyroid cancer.
In this study, the diagnostic values of ultrasound,
FNA and ultrasound combined with FNA for patients with a thyroid
nodule ≤1 cm were first analyzed. The results showed that
ultrasound combined with FNA had higher sensitivity than ultrasound
and FNA alone, higher accuracy than ultrasound alone (P<0.05).
There is a study (22) showing that
preoperative ultrasound combined with ultrasound-guided lymph node
puncture biopsy can detect approximately >50% of breast cancer
patients with axillary lymph node metastasis, which indicates the
diagnostic value of ultrasound combined with puncture biopsy, and
supports our conclusion. Then, the diagnostic values of ultrasound,
FNA and ultrasound combined with FNA for patients with a thyroid
nodule >1 cm were analyzed. The results showed that in group B
(>1 cm group), there were no statistically significant
differences in the sensitivity, specificity, accuracy, positive
predictive value and negative predictive value between FNA,
ultrasound and FNA combined with ultrasound (P>0.05). These
findings show that for large nodules, ultrasound, FNA and
ultrasound combined with FNA are not much different, but ultrasound
is relatively more convenient and economical. There is a study
(23) showing that the accuracy of
FNA is 100.0% in the diagnosis of medullary thyroid carcinoma with
a diameter >1 cm and 66.6% in the diagnosis of medullary
microcarcinoma with a diameter <1 cm, which is similar to our
findings. We concluded that the accuracy of ultrasound and FNA is
affected by the size of the nodule, and the smaller the nodule is,
the lower the accuracy of diagnosis is, which are also consistent
with the findings of Shrestha et al (24). However, it has been reported
(25) that the sensitivity of
thyroid FNA affected by operational techniques and diagnostic
experience is difficult to be calculated accurately. Therefore, our
experimental results have yet to be further verified.
In summary, FNA combined with ultrasound can
significantly improve the sensitivity and accuracy in the diagnosis
of the thyroid nodule in the ≤1 cm group, while ultrasound, FNA and
ultrasound combined with FNA all have higher sensitivity and
accuracy in the diagnosis of the thyroid nodule in the >1 cm
group, without significant differences. Therefore, it can be
considered that ultrasound combined with FNA has a higher
diagnostic value for the determination of most benign and malignant
thyroid nodules, and can be used as a preferred solution for the
clinical diagnosis of thyroid cancer.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JL wrote the manuscript. JL and QW collected and
interpreted the data. JL, QW and LW were mainly devoted to surgery.
JW and DW analyzed the FNA results. ZX, YL and QZ were responsible
for and the ultrasound results. All the authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Liaocheng People's Hospital (Liaocheng, China). The signed informed
consents were obtained from the patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Giordano D, Valcavi R, Thompson GB,
Pedroni C, Renna L, Gradoni P and Barbieri V: Complications of
central neck dissection in patients with papillary thyroid
carcinoma: Results of a study on 1087 patients and review of the
literature. Thyroid. 22:911–917. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lee HS, Park C, Kim SW, Song JW, Chun BK,
Park TJ, Hong JC and Lee KD: Primary tumour characteristics predict
the invasiveness of lymph node metastases in papillary thyroid
carcinoma patients. J Laryngol Otol. 130:302–308. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
James BC, Mitchell JM, Jeon HD, Vasilottos
N, Grogan RH and Aschebrook-Kilfoy B: An update in international
trends in incidence rates of thyroid cancer, 1973–2007. Cancer
Causes Control. 29:465–473. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tang W, Huang C, Tang C, Xu J and Wang H:
Galectin-3 may serve as a potential marker for diagnosis and
prognosis in papillary thyroid carcinoma: A meta-analysis.
OncoTargets Ther. 9:455–460. 2016. View Article : Google Scholar
|
|
5
|
Archier A, Heimburger C, Guerin C, Morange
I, Palazzo FF, Henry JF, Schneegans O, Mundler O, Abdullah AE,
Sebag F, et al: (18)F-DOPA PET/CT in the diagnosis and localization
of persistent medullary thyroid carcinoma. Eur J Nucl Med Mol
Imaging. 43:1027–1033. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li F, Zhang J, Wang Y and Liu L: Clinical
value of elasticity imaging and contrast-enhanced ultrasound in the
diagnosis of papillary thyroid microcarcinoma. Oncol Lett.
10:1371–1377. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Trimboli P, Nasrollah N, Amendola S, Rossi
F, Ramacciato G, Romanelli F, Aurello P, Crescenzi A, Laurenti O,
Condorelli E, et al: Should we use ultrasound features associated
with papillary thyroid cancer in diagnosing medullary thyroid
cancer? Endocr J. 59:503–508. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Niu LJ, Hao YZ and Zhou CW: Diagnostic
value of ultrasonography in thyroid lesions. Zhonghua Er Bi Yan Hou
Tou Jing Wai Ke Za Zhi. 41:415–418. 2006.(In Chinese). PubMed/NCBI
|
|
9
|
Hong YR, Luo ZY, Mo GQ, Wang P, Ye Q and
Huang PT: Role of contrast-enhanced ultrasound in the pre-operative
diagnosis of cervical lymph node metastasis in patients with
papillary thyroid carcinoma. Ultrasound Med Biol. 43:2567–2575.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Theoharis C, Adeniran AJ, Roman S, Sosa JA
and Chhieng D: The impact of implementing The Bethesda System for
reporting of thyroid FNA at an academic center. Diagn Cytopathol.
41:858–863. 2013.PubMed/NCBI
|
|
11
|
Renshaw AA and Gould EW: Why there is the
tendency to ‘overdiagnose’ the follicular variant of papillary
thyroid carcinoma. Am J Clin Pathol. 117:19–21. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ruilong Z, Daohai X, Li G, Xiaohong W,
Chunjie W and Lei T: Diagnostic value of 18F-FDG-PET/CT for the
evaluation of solitary pulmonary nodules: A systematic review and
meta-analysis. Nucl Med Commun. 38:67–75. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu X, Ouyang D, Li H, Zhang R, Lv Y, Yang
A and Xie C: Papillary thyroid cancer: Dual-energy spectral CT
quantitative parameters for preoperative diagnosis of metastasis to
the cervical lymph nodes. Radiology. 275:167–176. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sipos JA: Advances in ultrasound for the
diagnosis and management of thyroid cancer. Thyroid. 19:1363–1372.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Levy I, Barki Y and Tovi F: Giant cervical
cyst: Presenting symptom of an occult thyroid carcinoma. J Laryngol
Otol. 105:863–864. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vierhapper H, Niederle B, Bieglmayer C,
Kaserer K and Baumgartner-Parzer S: Early diagnosis and curative
therapy of medullary thyroid carcinoma by routine measurement of
serum calcitonin in patients with thyroid disorders. Thyroid.
15:1267–1272. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sheils O: Molecular classification and
biomarker discovery in papillary thyroid carcinoma. Expert Rev Mol
Diagn. 5:927–946. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Huang GQ, Liu Y, Cao DF, Gong Y, Su D,
Zhao JH and Wang L: Advances in tumor markers for the early
diagnosis of papillary thyroid carcinoma. Int J Pharm Pharm Sci.
8:472016. View Article : Google Scholar
|
|
19
|
Harshan M, Crapanzano JP, Aslan DL,
Vazquez MF and Saqi A: Papillary thyroid carcinoma with atypical
histiocytoid cells on fine-needle aspiration. Diagn Cytopathol.
37:244–250. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Trimboli P, Treglia G, Guidobaldi L,
Romanelli F, Nigri G, Valabrega S, Sadeghi R, Crescenzi A, Faquin
WC, Bongiovanni M, et al: Detection rate of FNA cytology in
medullary thyroid carcinoma: A meta-analysis. Clin Endocrinol
(Oxf). 82:280–285. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoon JH, Kim EK, Kwak JY and Moon HJ:
Effectiveness and limitations of core needle biopsy in the
diagnosis of thyroid nodules: Review of current literature. J
Pathol Transl Med. 49:230–235. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Houssami N, Ciatto S, Turner RM, Cody HS
III and Macaskill P: Preoperative ultrasound-guided needle biopsy
of axillary nodes in invasive breast cancer: Meta-analysis of its
accuracy and utility in staging the axilla. Ann Surg. 254:243–251.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yang GC, Fried K and Levine PH: Detection
of medullary thyroid microcarcinoma using ultrasound-guided fine
needle aspiration cytology. Cytopathology. 24:92–98. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shrestha M, Crothers BA and Burch HB: The
impact of thyroid nodule size on the risk of malignancy and
accuracy of fine-needle aspiration: A 10-year study from a single
institution. Thyroid. 22:1251–1256. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pitman MB, Abele J, Ali SZ, Duick D,
Elsheikh TM, Jeffrey RB, Powers CN, Randolph G, Renshaw A and
Scoutt L: Techniques for thyroid FNA: a synopsis of the National
Cancer Institute Thyroid Fine-Needle Aspiration State of the
Science Conference. Diagn Cytopathol. 36:407–424. 2008. View Article : Google Scholar : PubMed/NCBI
|