Introduction
Lung cancer is a type of malignant tumor that causes
considerable mortality and morbidity worldwide (1). Out of all lung cancer cases, >85%
are non-small cell lung cancer (NSCLC) (2). Surgical intervention, chemotherapy and
radiation therapy are the traditional therapies for early-stage
lung cancer; however, all these treatments are accompanied by
undesirable adverse reactions. In recent years, molecular targeted
therapies, which specifically target carcinoma cells, and
reportedly have minimal adverse effects compared with conventional
treatments, have become a research focus (3). Currently, a large amount of molecular
therapies targeting diverse receptor tyrosine kinases (RTKs), which
have been demonstrated to be frequently mutated and to promote
tumorigenesis by regulating cell proliferation and survival, are
widely used in patients with NSCLC (4). Numerous types of RTKs, including
epidermal growth factor receptor (EGFR), hepatocyte growth factor
receptor (c-Met), ALK receptor tyrosine kinase (ALK) and BRAF,
which have been reported to be frequently mutated in patients with
NSCLC, have been used as targets in clinical therapy (5–10).
However, despite all these therapies, the majority of patients with
NSCLC still exhibit a poor 5-year survival rate of 15.9% (11). Therefore, there is an urgent need to
identify biomarkers with better prognostic and diagnostic
potential.
The cleavage polyadenylation specificity factor
(CPSF) complex is a core component of 3′-end processing and is
involved in regulating mRNA maturation and alternative splicing, as
well as internal introns, by modulating the cleavage and
polyadenylation of mRNAs (12). The
multi-subunit CPSF complex is composed of CPSF1 (also known as
CPSF160), CPSF2 (also known as CPSF100), CPSF3 (the cleavage
endonuclease, also known as CPSF73), CPSF4 (also known as CPSF30),
factor interacting with poly(A) polymerase α and CPSF1 (FIP1L1;
also known as FIP1) and WD repeat domain 33 (12). There are several studies regarding
the function of the CPSF complex in cancer, particularly in lung
cancer; however, CPSF1 promotes cell proliferation in human ovarian
cancer (13). Decreased CPSF2
expression promotes invasion and an increased cancer stem cell
population, and CPSF2 may be a novel prognostic marker for
papillary thyroid carcinoma (14,15).
Suppression of CPSF4 inhibits the proliferation of lung
adenocarcinoma (LUAD) cells and is associated with overall survival
(OS) (16–19). FIP1L1 is generated via gene fusion
with platelet-derived growth factor receptor a, which is recognized
as an important diagnostic marker of hematological malignancies,
including chronic eosinophilic leukemia, hypereosinophilic syndrome
and systemic mastocytosis, and occasionally atypical chronic
myelogenous leukemia (20).
Therefore, it was hypothesized that potential diagnostic and
prognostic biomarkers could exist within the CPSF complex.
The Cancer Genome Atlas (TCGA; http://portal.gdc.cancer.gov) is an open-access
database that is widely used globally and provides a reliable tool
for the analysis of numerous types of useful clinicopathological
data. In addition, TCGA data is overseen by the National Cancer
Institute's Center for Cancer Genomics (21). Genetic and clinicopathological data
of >1,000 patients with primary LUAD and lung squamous cell
carcinoma (LUSC) are recorded in the TCGA Lung Cancer Cohort
(22).
In the present study, promising biomarkers for NSCLC
were identified via bioinformatics data mining. The results of the
present study demonstrated that CPSF3 of the CPSF complex was
overexpressed in NSCLC, and its overexpression was associated with
OS and recurrence-free survival (RFS) of patients with LUAD. CPSF3
may also serve as a diagnostic biomarker for LUAD and LUSC.
Additionally, CPSF3 may promote the proliferation and lymph node
metastasis of LUAD. The mechanism of CPSF3 overexpression may be
connected to its DNA copy number variants and DNA
hypermethylation.
Materials and methods
TCGA Lung Cancer Cohort
TCGA Lung Cancer Cohort data, (http://tcga.cancer.gov/dataportal; accessed June
2016), which include the LUAD cohort, comprising 706 primary LUAD
tissues and normal lung tissues, and the LUSC cohort, comprising
554 primary LUSC tissues and normal lung tissues, were downloaded
from the University of California Santa Cruz Xena Browser
(https://xenabrowser.net). Excel 2016 (Microsoft
Corporation) was used for further data processing. From the
cohorts, 520 primary LUAD cases and 506 primary LUSC cases with
existing RNA-seq and intact clinical parameters were selected for
further analysis. In addition, DNA methylation data (‘Illumina 450k
methylation’) and CNA data (‘gene-level GISTIC2-processed’) were
downloaded from this database to detect the possible mechanisms of
abnormal expression of CPSF3 in LUAD.
Cancer cell line encyclopedia
(CCLE)
CCLE (https://portals.broadinstitute.org/ccle/about) is a
database containing genomic data, including copy number, mRNA
expression, reverse-phase protein microarray and reduced
representation bisulfite sequencing, from >1,100 cell lines.
LUAD cell line data (based on The Global Bioresource Center;
http://www.atcc.org) were downloaded to examine the
association between CPSF3 expression and its DNA methylation.
Statistical analysis
GraphPad Prism version 5.0 (GraphPad Software, Inc.)
or SPSS version 16.0 (SPSS, Inc.) were used for data analysis.
Unless specifically mentioned, all values are presented as the mean
± SD. Two-group independent sample comparisons were performed using
a Student's t-test (two-tailed) when the two groups had equal
variances, while Welch's t-test was used for unequal variances.
Multi-group samples statistics were analyzed via one-way ANOVA if
the variances were equal; if not, Welch's ANOVA was performed.
Bonferroni post hoc tests were performed for all ANOVAs. Samples
from TCGA Lung Cancer Cohort were divided into two groups,
according to median values. OS and RFS curves were plotted using
the Kaplan-Meier method, and OS and RFS differences were assessed
using the log-rank test. Receiver operating characteristic (ROC)
curves were constructed using CPSF3 expression data, and the area
under the curve (AUC) was estimated to investigate the feasibility
of distinguishing LUAD from LUSC. Pearson correlation analysis was
used to evaluate the correlations among CPSF3 mRNA expression and
CPSF3 DNA methylation and DNA copy number variants (CNAs).
P<0.05 was considered to indicate a statistically significant
difference.
Results
CPSF complex is significantly elevated
in NSCLC tissues compared with normal lung tissues (NTL)
Expression levels of CPSF complex components were
individually assessed in the TCGA LUAD and LUSC cohorts. The
results indicated that all CPSF complex components were
significantly overexpressed in LUAD (Fig. 1) and LUSC (Fig. 2) tissues compared with NTL.
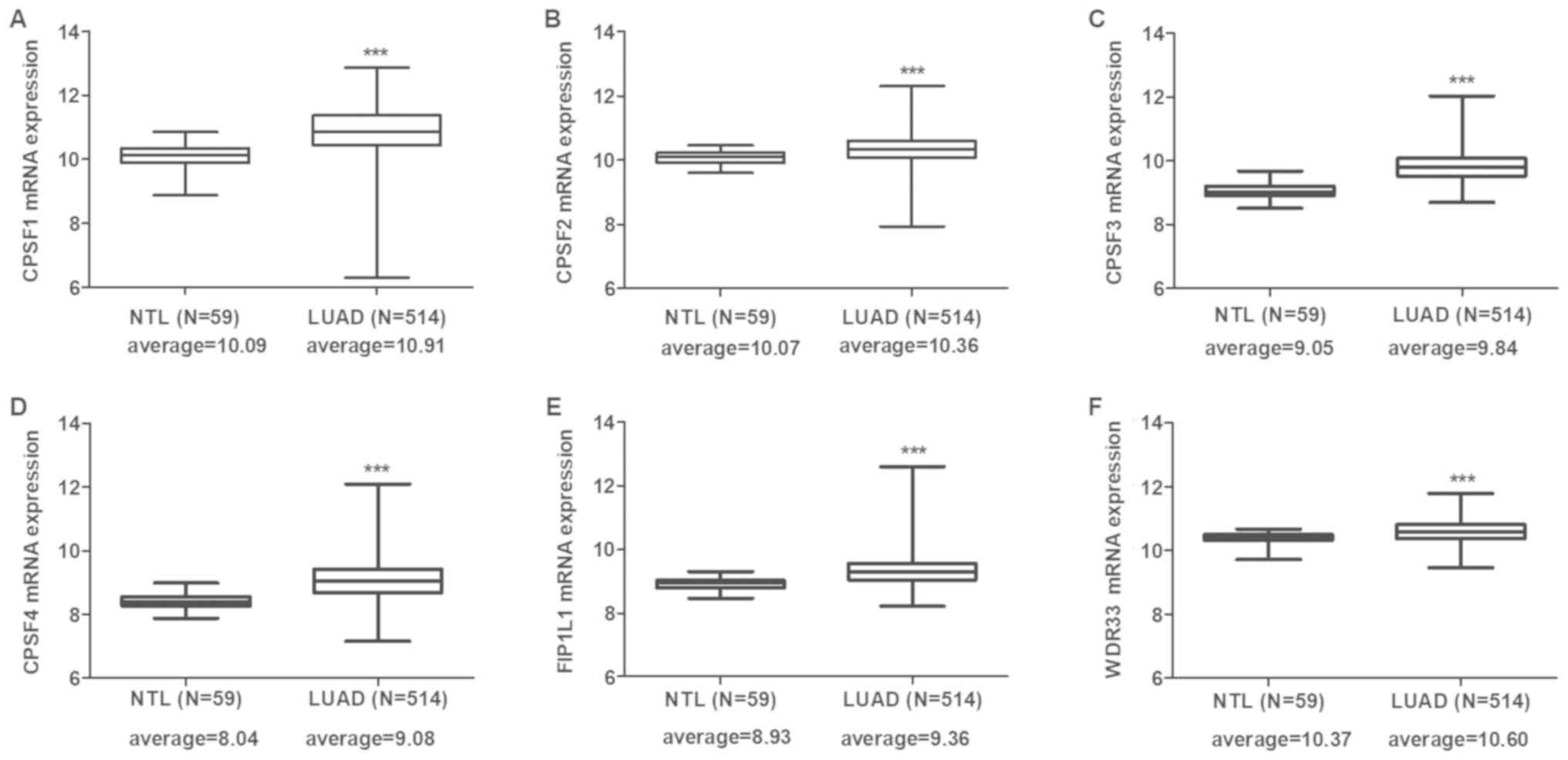 | Figure 1.CPSF complex component mRNA expression
in The Cancer Genome Atlas-LUAD tissues. CPSF complex components,
including (A) CPSF1, (B) CPSF2, (C) CPSF3, (D) CPSF4, (E) FIP1L1
and (F) WDR33, were significantly overexpressed in LUAD tissues
compared with in NTL. ***P<0.0001. CPSF, cleavage
polyadenylation specificity factor; NTL, normal lung tissue; LUAD,
lung adenocarcinoma; FIP1L1, factor interacting with poly(A)
polymerase α and CPSF1; WDR33, WD repeat domain 33. |
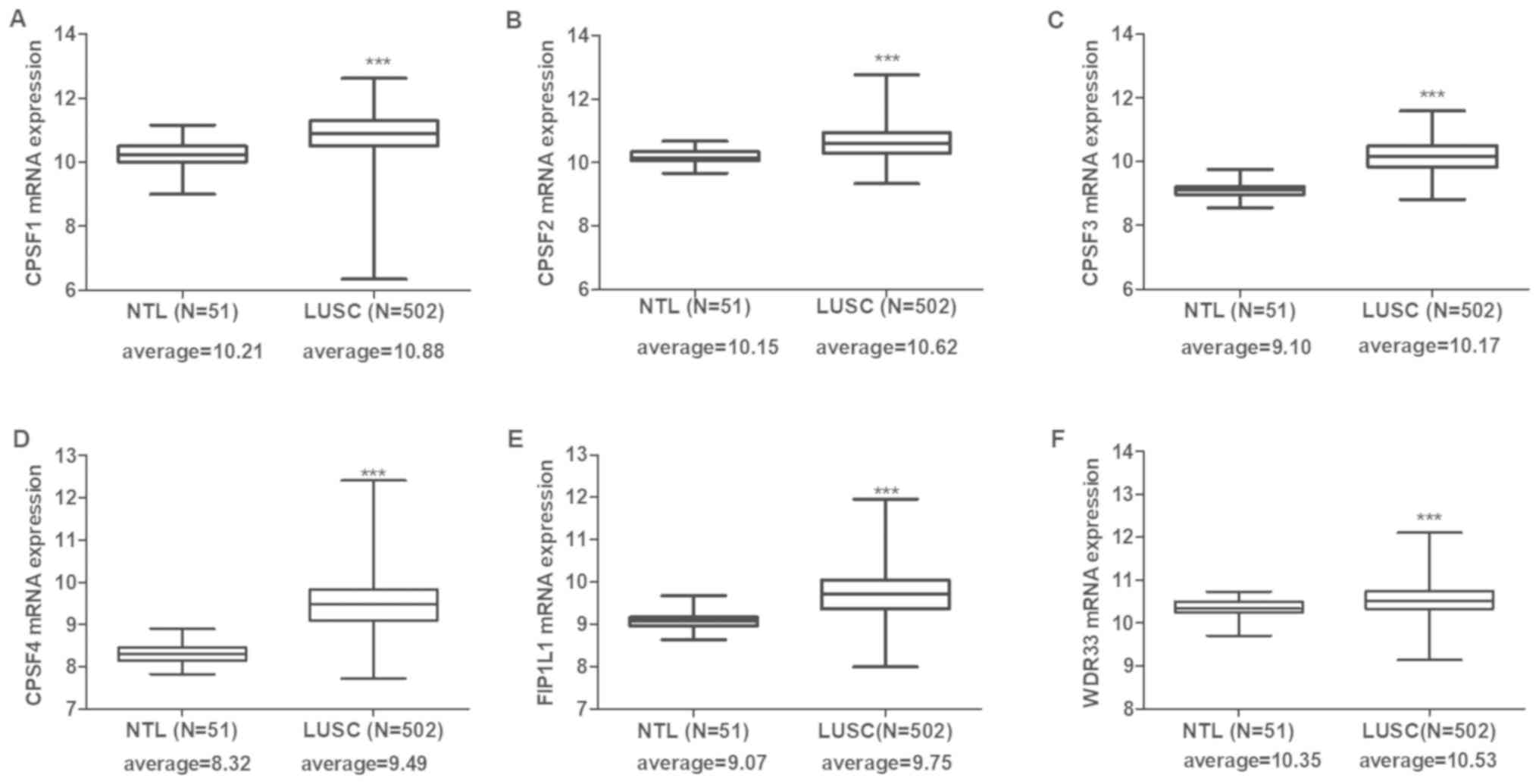 | Figure 2.CPSF complex component mRNA expression
in The Cancer Genome Atlas-LUSC tissues. All CPSF complex
components, including (A) CPSF1, (B) CPSF2, (C) CPSF3, (D) CPSF4,
(E) FIP1L1 and (F) WDR33, were significantly overexpressed in LUSC
tissues compared with in NTL. ***P<0.0001. CPSF, cleavage
polyadenylation specificity factor; NTL, normal lung tissue; LUSC,
lung squamous cell carcinoma; FIP1L1, factor interacting with
poly(A) polymerase α and CPSF1; WDR33, WD repeat domain 33. |
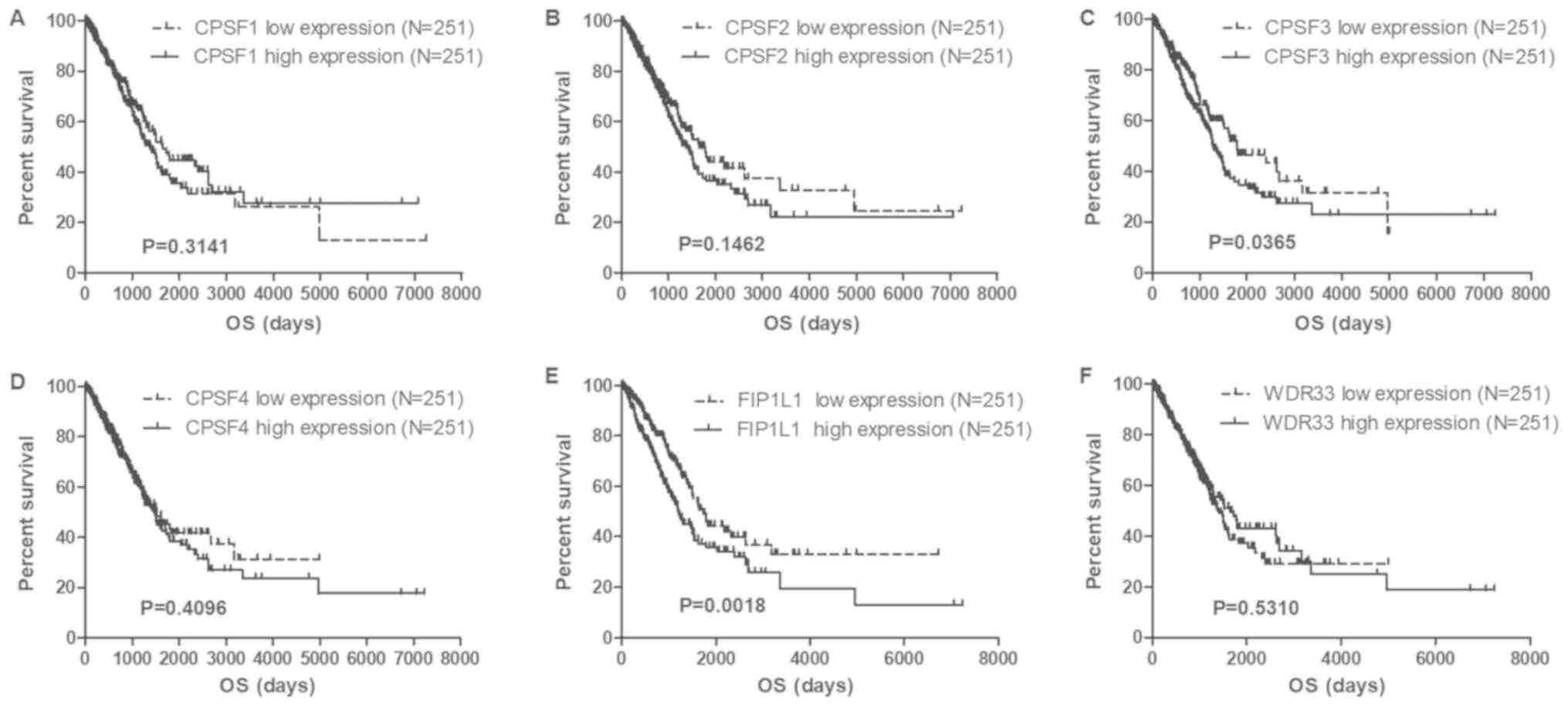
CPSF3 is the only component associated
with lung cancer OS and RFS in the CPSF complex
To identify potential prognostic biomarkers in the
CPSF complex, the associations among the CPSF complex components
and OS and RFS in the TCGA Lung Cancer Cohort were assessed. The
results of the present study demonstrated that overexpression of
CPSF3 and FIP1L1 in patients with LUAD was associated with
decreased survival times compared with patients with low expression
levels of CPSF3 and FIP1L1 (Fig. 3).
In patients with LUSC, no CPSF complex components were
significantly associated with OS (Fig.
4). Additionally, analysis of the association between the CPSF
complex component proteins and RFS was investigated. Patients with
LUAD with high CPSF2 and CPSF3 had shorter RFS than those in the
low expression groups (Fig. 5),
whereas expression of the components had no effect on RFS of
patients with LUSC (Fig. 6). Taken
together, CPSF3 was the only CSPF complex component that affected
OS and RFS, and it may thus function as a promising prognostic
biomarker for NSCLC. Therefore, CPSF3 was considered as a potential
biomarker and focused on in further research.
 | Figure 4.Association between CPSF complex
components and OS in TCGA-LUSC patients. Kaplan-Meier analysis of
OS time of TCGA-LUSC Cohort patients. The patients were divided
into high and low expression groups depending on the average
expression level of each gene. CPSF complex components, including
(A) CPSF1, (B) CPSF2, (C) CPSF3, (D) CPSF4, (E) FIP1L1 and (F)
WDR33, exhibited no connection with OS in LUSC. TCGA, The Cancer
Genome Atlas; LUSC, lung squamous cell carcinoma; CPSF, cleavage
polyadenylation specificity factor; OS, overall survival; FIP1L1,
factor interacting with poly(A) polymerase α and CPSF1; WDR33, WD
repeat domain 33. |
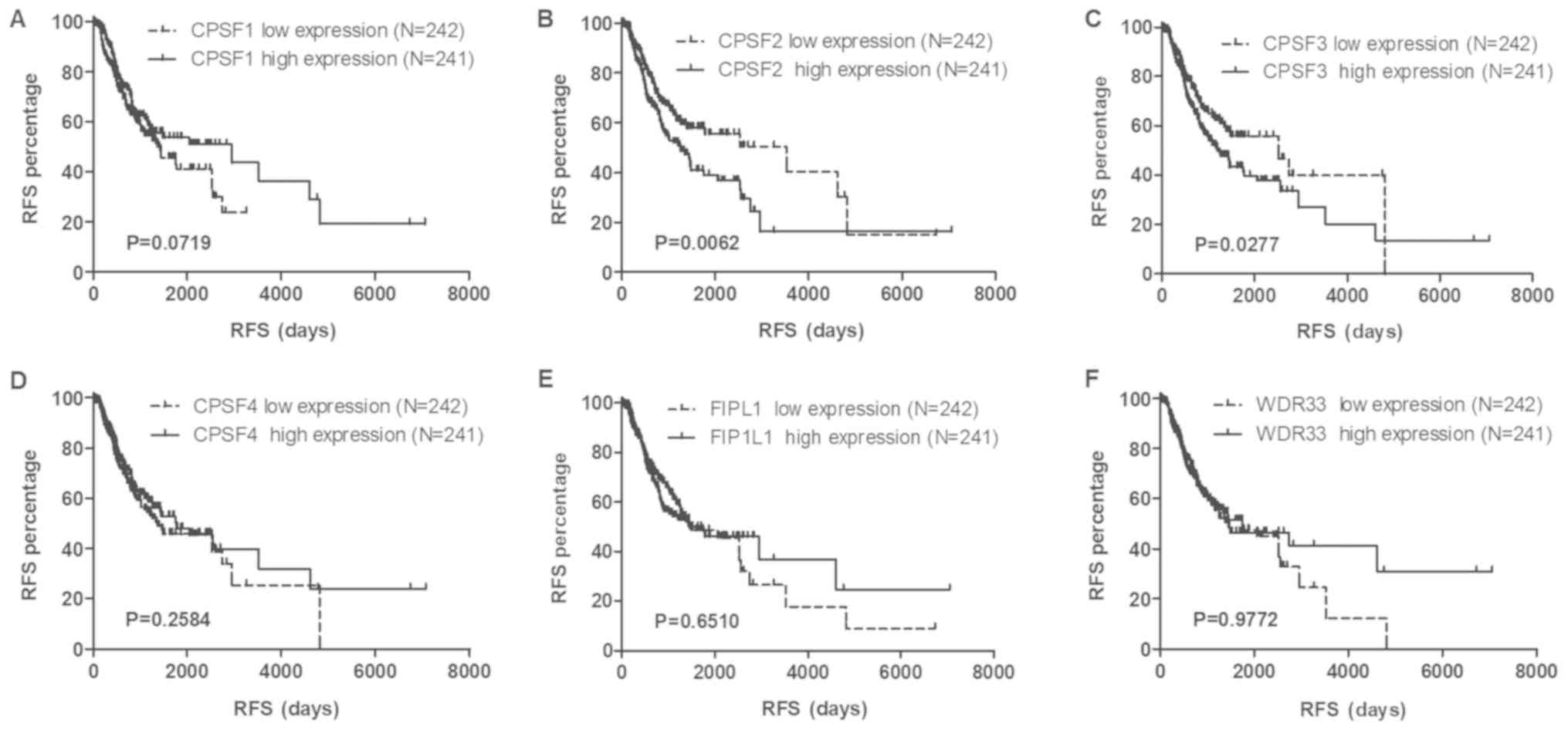 | Figure 5.Association of CPSF complex components
and RFS in TCGA-LUAD patients. Kaplan-Meier analysis of the RFS of
TCGA-LUAD patients. The patients were stratified depending on the
average expression level of (A) CPSF1, (B) CPSF2, (C) CPSF3, (D)
CPSF4, (E) FIP1L1 and (F) WDR33. High expression levels of CPSF2
and CPSF3 were associated with the RFS of patients with LUAD.
Overexpression of CPSF1, CPSF4, FIP1L1 and WDR33 had no influence
on RFS. TCGA, The Cancer Genome Atlas; LUAD, lung adenocarcinoma;
CPSF, cleavage polyadenylation specificity factor; RFS,
recurrence-free survival; FIP1L1, factor interacting with poly(A)
polymerase α and CPSF1; WDR33, WD repeat domain 33. |
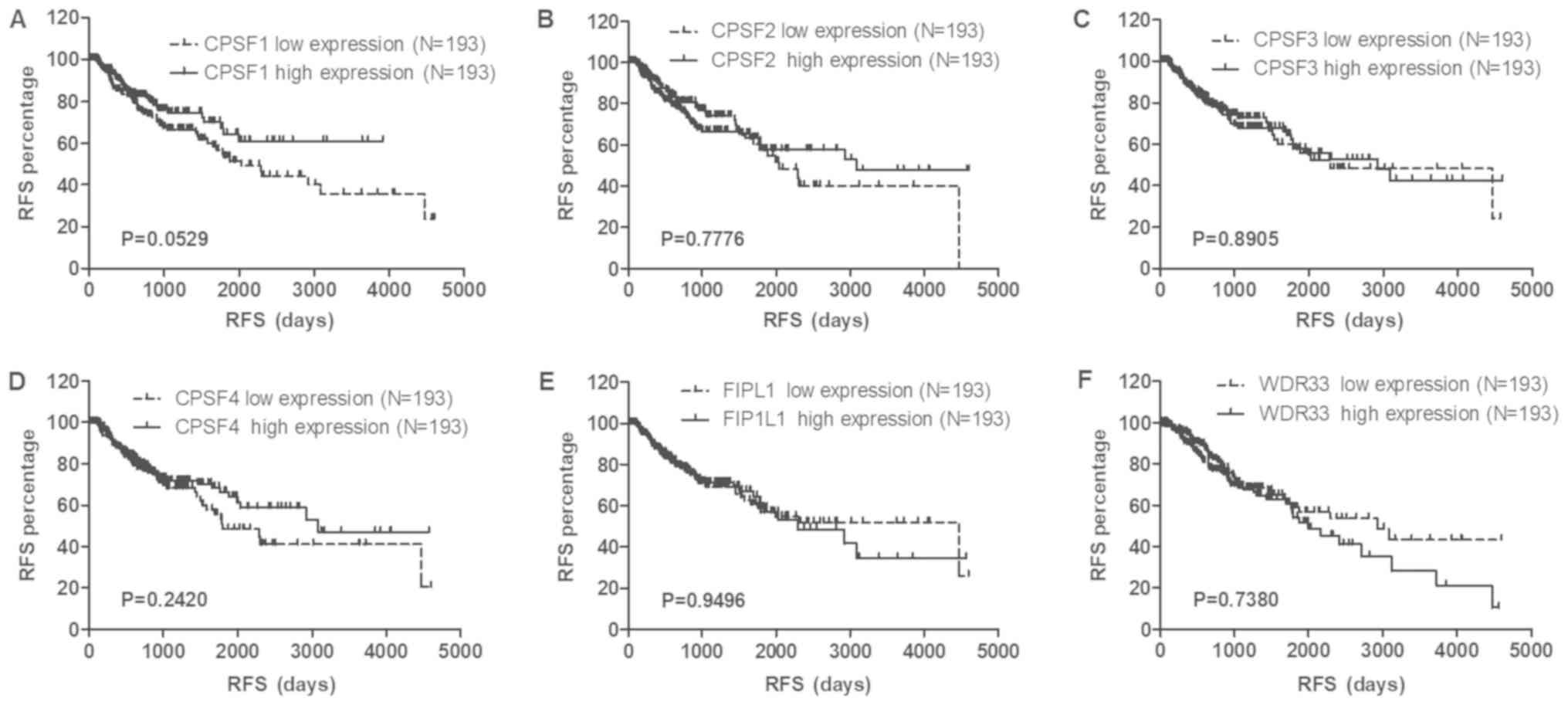 | Figure 6.Association between CPSF complex
expression and RFS in TCGA-LUSC patients. Kaplan-Meier analysis of
the RFS of TCGA-LUSC patients. The patients were stratified
depending on the average expression level of each gene. CPSF
complex members, including (A) CPSF1, (B) CPSF2, (C) CPSF3, (D)
CPSF4, (E) FIP1L1 and (F) WDR33, exhibited no connection with RFS
in LUSC. TCGA, The Cancer Genome Atlas; LUSC, lung squamous cell
carcinoma; CPSF, cleavage polyadenylation specificity factor; RFS,
recurrence-free survival; FIP1L1, factor interacting with poly(A)
polymerase α and CPSF1; WDR33, WD repeat domain 33. |
CPSF3 serves as a biomarker to
distinguish between histological subtypes of NSCLC
To further test whether CPSF3 could serve as a
biomarker to distinguish between LUAD and LUSC, CPSF3 expression
status of patients with LUAD and LUSC in the TCGA Lung Cancer
Cohort was compared. As shown in Fig.
7A, the average expression level of CPSF3 among 502 patients
with LUSC was higher than that of 512 patients with LUAD. ROC
analysis further demonstrated that CPSF3 expression could be a
single significant parameter to discriminate between LUAD and LUSC,
with an AUC of 0.7014 (Fig. 7B). To
further explore the clinical implications of CPSF3, associations
among CPSF3 expression and different molecular subtypes were
investigated within different types of adenocarcinoma classified
according to the genotypes of BRAF, erb-b2 receptor tyrosine kinase
4 (ERBB4), EGFR, echinoderm microtubule associated protein like 4,
KRAS and serine/threonine kinase 11, and ALK translocation, in the
TCGA-LUAD cohort. There was no difference in CPSF3 between the wild
type and mutant samples categorized by any of the aforementioned
genes of interest (Fig. 7C-H).
Overall, CPSF3 was shown to be a novel and efficient diagnostic
biomarker for distinguishing between LUAD and LUSC in NSCLC.
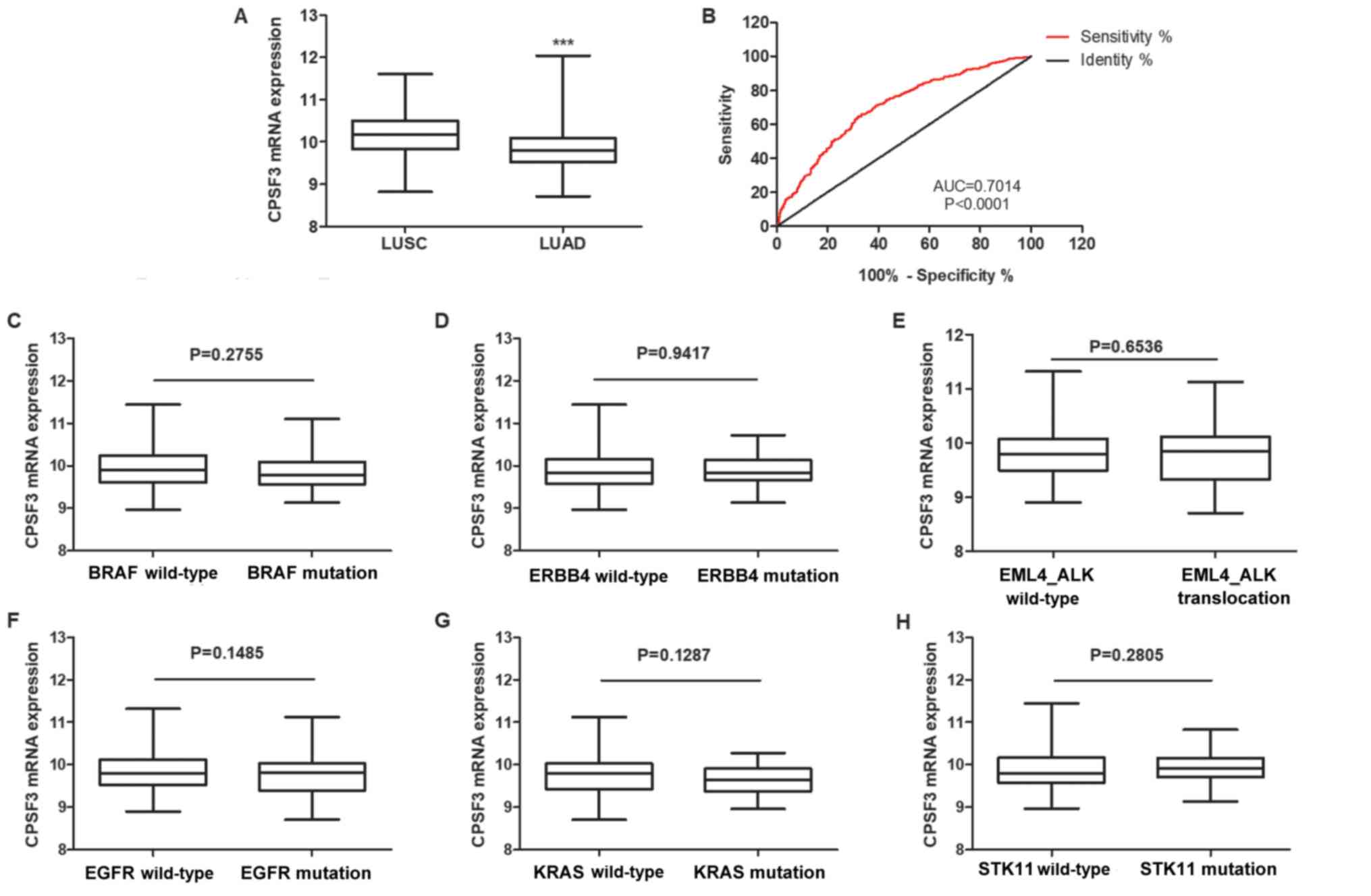 | Figure 7.CPSF3 functions as a biomarker to
distinguish between the histological subtypes of non-small cell
lung cancer. (A) Expression levels of CPSF3 were markedly higher in
patients with LUSC than in patients with LUAD. (B) Receiver
operating characteristic curve analysis revealed the potential use
of CPSF3 expression to discriminate between patients with LUAD and
LUSC in the TCGA Cohort. Comparison of the relative expression of
CPSF3 between two groups of patients with LUAD in the TCGA Cohort,
classified by molecular subtype based on (C) BRAF, (D) ERBB4, (E)
ALK, (F) EGFR, (G) KRAS and (H) STK11 mutations, respectively. None
of the mutations were identified to be associated with CPSF3
expression. ***P<0.0001. TCGA, The Cancer Genome Atlas; CPSF3,
cleavage polyadenylation specific factor 3; LUSC, lung squamous
cell carcinoma; LUAD, lung adenocarcinoma; AUC, area under the
curve; ERBB4, erb-b2 receptor tyrosine kinase 4; EML4, echinoderm
microtubule associated protein like 4; ALK, ALK receptor tyrosine
kinase; EGFR, epidermal growth factor receptor; STK11,
serine/threonine kinase 11. |
Association of CPSF3 expression with
clinicopathological features in LUAD
To explore the role of high CPSF3 expression in LUAD
progression, the association of clinicopathological features with
CPSF3 expression was evaluated. The present study revealed that
CPSF3 expression was associated with smoking history, tumor
diameter, lymph node metastasis, TNM stage and radiation therapy,
whereas there was no association with age, gender, distant
metastasis and targeted molecular therapy in the TCGA-LUAD Cohort
(Table I). Therefore, it was
hypothesized that CPSF3 may promote proliferation and metastasis,
and may be associated with radiation therapy.
 | Table I.Association of CPSF3 with
clinicopathological features in The Cancer Genome Atlas lung
adenocarcinoma patients. |
Table I.
Association of CPSF3 with
clinicopathological features in The Cancer Genome Atlas lung
adenocarcinoma patients.
| Variable | N | CPSF3 (mean ±
SE) | t-value | P-value |
|---|
| Sex |
|
|
|
|
|
Female | 277 | 9.805±0.4380 | 1.804 | 0.0717 |
| Male | 237 | 9.876±0.4555 |
|
|
| Age, years |
|
|
|
|
|
<65 | 220 | 9.871±0.4691 | 1.693 | 0.0911 |
| ≥65 | 275 | 9.876±0.4252 |
|
|
| Smoking history |
|
|
|
|
|
Smoked | 75 | 9.700±0.4516 | 2.937 | 0.0035a |
| Never
smoked | 425 | 9.766±0.3928 |
|
|
| Tumor diameter,
cm |
|
|
|
|
| ≤3 | 169 | 9.876±0.4677 | 2.638 | 0.0086a |
|
>3 | 342 | 9.766±0.3928 |
|
|
| Lymph node
metastasis |
|
|
|
|
| No | 330 | 9.805±0.4598 | 2.763 | 0.0059a |
|
Yes | 172 | 9.766±0.4188 |
|
|
| Distant
metastasis |
|
|
|
|
| M0 | 346 | 9.853±0.4440 | 1.611 | 0.1079 |
| M1 | 25 | 9.921±0.4796 |
|
|
| TNM stage |
|
|
|
|
| I | 425 | 9.792±0.4115 | 4.178 | 0.0062a |
| II | 122 | 9.820±0.4917 |
|
|
|
III | 84 |
9.961±0.4288b |
|
|
| IV | 25 |
9.979±0.4837b |
|
|
| Radiation
therapy |
|
|
|
|
|
Yes | 60 | 9.812±0.4398 | 2.742 | 0.0063a |
| No | 397 | 9.981±0.4847 |
|
|
| Molecular
therapy |
|
|
|
|
| No | 303 | 9.804±0.4477 | 1.946 | 0.0523 |
|
Yes | 152 | 9.891±0.4482 |
|
|
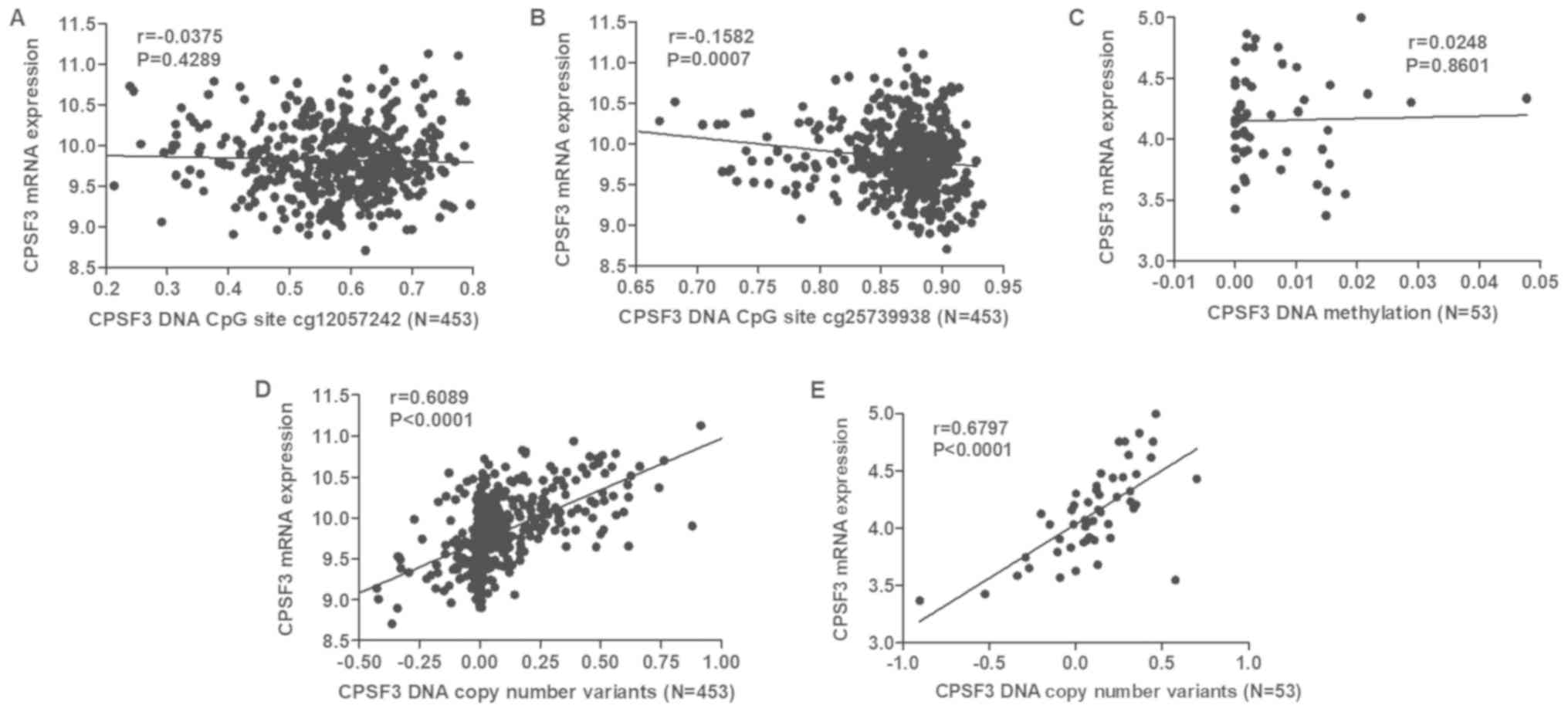
DNA methylation and DNA CNAs are
correlated with CPSF3 expression in LUAD
DNA methylation is one of the most common factors
associated with abnormal gene expression. By analyzing CPSF3 DNA
methylation and RNA-seq data in the TCGA-LUAD Cohort, two CPSF3 DNA
methylation CpG sites (cg12057242 and cg25739938) were identified
to be differentially methylated in TCGA-LUAD tissues compared with
normal lung tissues (Table II). The
correlation between the two differentially expressed DNA CpG sites
and RNA expression was assessed, demonstrating that cg25739938
exhibited a negative correlation with CPSF3 expression (Fig. 8A and B). However, the same analysis
conducted in 53 LUAD cell lines from CCLE indicated there was no
correlation between CPSF3 expression and methylation (Fig. 8C). DNA CNAs are another mechanism
that leads to aberrant RNA expression. Therefore, the association
between CPSF3 DNA CNAs and RNA expression was further analyzed. The
results demonstrated that CPSF3 CNAs were positively correlated
with CPSF3 mRNA expression in TCGA-LUAD samples (Fig. 8D) and CCLE-LUAD cell lines (Fig. 8E).
| Table II.CPSF3 DNA methylation CpG sites
analysis in The Cancer Genome Atlas-LUAD. |
Table II.
CPSF3 DNA methylation CpG sites
analysis in The Cancer Genome Atlas-LUAD.
| CpG site | Tissue | CpG methylation
(mean ± SE) | t-value | P-value |
|---|
| cg23889771 | NTL | 0.0700±0.0196 | 0.0107 | 0.9915 |
|
| LUAD | 0.0700±0.0110 |
|
|
| cg24873957 | NTL | 0.0837±0.0137 | 0.5146 | 0.6071 |
|
| LUAD | 0.0825±0.0124 |
|
|
| cg20361001 | NTL | 0.0388±0.0083 | 0.3778 | 0.7058 |
|
| LUAD | 0.0040±0.0108 |
|
|
| cg20093808 | NTL | 0.0276±0.0067 | 0.0731 | 0.9417 |
|
| LUAD | 0.0274±0.0092 |
|
|
| cg07814910 | NTL | 0.0801±0.0187 | 0.3878 | 0.6983 |
|
| LUAD | 0.0792±0.0128 |
|
|
| cg20549545 | NTL | 0.0864±0.0178 | 1.826 | 0.0685 |
|
| LUAD | 0.0916±0.0139 |
|
|
| cg08937729 | NTL | 0.0948±0.0213 | 0.1190 | 0.9054 |
|
| LUAD | 0.0944±0.0173 |
|
|
| cg07179925 | NTL | 0.0288±0.0134 | 1.171 | 0.2421 |
|
| LUAD | 0.0268±0.0090 |
|
|
| cg00024812 | NTL | 0.0601±0.0152 | 1.133 | 0.2578 |
|
| LUAD | 0.0573±0.0133 |
|
|
| cg26306976 | NTL | 0.0795±0.0482 | 0.6744 | 0.5004 |
|
| LUAD | 0.7806±0.1175 |
|
|
| cg07974891 | NTL | 0.6744±0.0430 | 0.2672 | 0.7894 |
|
| LUAD | 0.6685±0.1237 |
|
|
| cg18666330 | NTL | 0.8918±0.0274 | 1.260 | 0.2083 |
|
| LUAD | 0.8856±0.0261 |
|
|
| cg12057242 | NTL | 0.5333±0.0448 | 2.207 | 0.0278a |
|
| LUAD | 0.5772±0.1117 |
|
|
| cg25739938 | NTL | 0.8485±0.8658 | 2.137 | 0.0331a |
|
| LUAD | 0.8658±0.0445 |
|
|
| cg18794882 | NTL | 0.8378±0.0475 | 1.774 | 0.0767 |
|
| LUAD | 0.8187±0.0595 |
|
|
Discussion
Previously, a number of promising potential
biomarkers have been identified in a series of secondary analyses
using TCGA data. For example, DNA methylation of SOX30 is
correlated with myelodysplastic syndrome progression, and has been
reported to act as a potential predictive and prognostic biomarker
in acute myeloid leukemia (23).
Higher FOS expression is associated with a better outcome in breast
cancer datasets (24). Using public
data from TCGA, a 22-gene signature that demonstrated the best
predictive value for assessing the clinical benefit of
postoperative chemoradiotherapy was established (25).
Compound gene analysis is a more effective way of
elucidating novel biomarkers and assessing the interactions among
individual genes. Targeting one of these genes may lead to a large
feedback effect. CPSF complex components have been demonstrated to
regulate the cleavage and polyadenylation of mRNAs during the mRNA
maturation and alternative splicing processes (12). However, there are few reports
regarding the role of CPSF4 in lung cancer (16–19),
and, to the best of our knowledge, no reports on the other
components. Therefore, TCGA data was utilized to elucidate
potential prognostic and diagnostic biomarkers within the complex
in the present study.
In the present study, CPSF complex components were
first evaluated in terms of their expression levels in NSCLC using
TCGA data, as biomarkers must be differentially expressed between
cancer tissue and normal tissue. The results of the present study
indicated that expression of all CPSF complex components was
increased in NSCLC. A promising biomarker should affect prognosis
and recurrence, and may therefore serve as a predictor. The
associations of CPSF complex expression with OS and RFS were
assessed, which demonstrated that CPSF3 was the only component that
affected OS and RFS in LUAD. Additionally, there is only one
previous report regarding the role of CPSF3 in cancer (26), and, to the best of our knowledge, no
reports regarding the role of CPSF3 in lung cancer; therefore, the
present study focused on CPSF3 for further research, as it appeared
to be a potentially promising biomarker. Further ROC curve analysis
demonstrated that CPSF3 may serve as a diagnostic biomarker for
NSCLC to distinguish between LUAD and LUSC.
A previous study in prostate cancer demonstrated
that knockdown of CPSF3 by a specific siRNA induces apoptosis
(26), which verified that CPSF3 is
associated with the proliferation of malignant carcinoma. To
further assess the role of CPSF3 in LUAD, the association between
clinicopathological features and CPSF3 was assessed. The present
study revealed that CPSF3 expression was associated with smoking
history, tumor diameter, lymph node metastasis, TNM stage and
radiation therapy; thus, CPSF3 may affect LUAD proliferation and
metastasis, consistent with the results of the aforementioned study
in prostate cancer (26).
The mechanism of gene dysregulation in NSCLC is
complex. Among all the mechanisms, genetic and epigenetic
alterations, including DNA amplification, DNA methylation and
somatic mutations, commonly lead to abnormal gene expression
accompanied by anomalous cancer cell behavior. For instance,
heteroclite sulfatase 2 methylation acts as a prognostic marker for
lung cancer survival (27). ERBB2
amplification results in erlotinib resistance in EGFR-L858R mutated
tyrosine kinase inhibitor-naïve LUAD (28). c-Met overexpression, HER-2 gene
amplification and spectrin β non-erythrocytic 1-ALK gene fusion
have been reported to coexist in LUAD, and this may become a novel
biomarker for cancer that is refractory to crizotinib, chemotherapy
and radiotherapy, and poor prognosis (29). Promoter methylation of cadherin 13 is
strongly associated with LUAD and may function as a promising
diagnostic biomarker for LUAD (30).
Thus, the present study assessed whether DNA CNA and abnormal DNA
methylation were the mechanism underlying the aberrant mRNA
expression of CPSF3, similar to the aforementioned gene. In the
present study, DNA methylation levels in TCGA LUAD tissues were
compared with levels in normal lung tissues, which revealed two
differentially expressed CpG sites. Further correlation analysis
confirmed that cg25739938 was negatively correlated with CPSF3
expression, while cg12057242 in TCGA-LUAD Cohort patients and in
LUAD cell lines has no correlation with CPSF3 expression. The
aforementioned results suggested that the hypermethylation of
cg25739938 may be the potential mechanism affecting CPSF3 mRNA
expression in LUAD. Furthermore, the DNA amplification status of
CPSF3 was detected. The results demonstrated that DNA CNAs were
closely associated with increased CPSF3 expression, in TCGA LUAD
Cohort patients and 53 LUAD cell lines. Overall, the dysregulation
of CPSF3 may be caused by DNA methylation and DNA CNAs.
In summary, the present study is the first to
elucidate the potential role of the CPSF complex, particularly
CPSF3, in proliferation and migration in lung cancer. As the
present study was conducted via bioinformatics analysis,
experimental studies regarding the role of CPSF3 in LUAD will be
performed in order to verify the results of the present study. In
conclusion, aberrant CPSF3 expression may be regulated by DNA CNAs,
and it may function as a promising prognostic and diagnostic
biomarker for LUAD.
Acknowledgements
Not applicable.
Funding
This study was funded by the National Nature Science
Foundation of China (grant no. 81401391) and the National Nature
Science Foundation of Guangdong Province (grant no.
2015A030313452).
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable request.
Data were obtained from The Cancer Genome Atlas (TCGA; http://portal.gdc.cancer.gov), CCLE (https://portals.broadinstitute.org/ccle/about); The
Global Bioresource Center (http://www.atcc.org) and the University of California
Santa Cruz Xena Browser (https://xenabrowser.net).
Authors' contributions
YN conceived and designed the study. WL performed
the bioinformatics analysis. XG helped design the project and wrote
the paper. XX analyzed the data, reviewed and checked the
manuscript. YZ proposed the concept of the study, analyzed and
interpreted the data, supervised the research throughout, managed
the project and funding and revised the article for important
intellectual content. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Thomas A, Liu SV, Subramaniam DS and
Giaccone G: Refining the treatment of NSCLC according to
histological and molecular subtypes. Nat Rev Clin Oncol.
12:511–526. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gadgeel SM, Ramalingam SS and Kalemkerian
GP: Treatment of lung cancer. Radiol Clin North Am. 50:961–974.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Daga A, Ansari A, Patel S, Mirza S, Rawal
R and Umrania V: Current drugs and drug targets in Non-small cell
lung cancer: Limitations and opportunities. Asian Pac J Cancer
Prev. 16:4147–4156. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Godin-Heymann N, Ulkus L, Brannigan BW,
McDermott U, Lamb J, Maheswaran S, Settleman J and Haber DA: The
T790M ‘gatekeeper’ mutation in EGFR mediates resistance to low
concentrations of an irreversible EGFR inhibitor. Mol Cancer Ther.
7:874–879. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Coate LE, John T, Tsao MS and Shepherd FA:
Molecular predictive and prognostic markers in non-small-cell lung
cancer. Lancet Oncol. 10:1001–1010. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yu HA, Sima CS, Huang J, Solomon SB,
Rimner A, Paik P, Pietanza MC, Azzoli CG, Rizvi NA, Krug LM, et al:
Local therapy with continued EGFR tyrosine kinase inhibitor therapy
as a treatment strategy in EGFR-mutant advanced lung cancers that
have developed acquired resistance to EGFR tyrosine kinase
inhibitors. J Thorac Oncol. 8:346–351. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Soucheray M, Capelletti M, Pulido I, Kuang
Y, Paweletz CP, Becker JH, Kikuchi E, Xu C, Patel TB, Al-Shahrour
F, et al: Intratumoral heterogeneity in EGFR-Mutant NSCLC results
in divergent resistance mechanisms in response to EGFR tyrosine
kinase inhibition. Cancer Res. 75:4372–4383. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ciuffreda L, Incani UC, Steelman LS,
Abrams SL, Falcone I, Curatolo AD, Chappell WH, Franklin RA, Vari
S, Cognetti F, et al: Signaling intermediates (MAPK and PI3K) as
therapeutic targets in NSCLC. Curr Pharm Des. 20:3944–3957. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schrank Z, Chhabra G, Lin L, Iderzorig T,
Osude C, Khan N, Kuckovic A, Singh S, Miller RJ and Puri N: Current
molecular-targeted therapies in NSCLC and their mechanism of
resistance. Cancers (Basel). 10(pii): E2242018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Goldstraw P, Ball D, Jett JR, Le Chevalier
T, Lim E, Nicholson AG and Shepherd FA: Non-small-cell lung cancer.
Lancet. 378:1727–1740. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Misra A and Green MR: From polyadenylation
to splicing: Dual role for mRNA 3′end formation factors. RNA Biol.
13:259–264. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang B, Liu Y, Liu D and Yang L:
Targeting cleavage and polyadenylation specific factor 1 via shRNA
inhibits cell proliferation in human ovarian cancer. J Biosci.
42:417–425. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nilubol N, Boufraqech M, Zhang L and
Kebebew E: Loss of CPSF2 expression is associated with increased
thyroid cancer cellular invasion and cancer stem cell population,
and more aggressive disease. J Clin Endocrinol Metab.
99:E1173–E1182. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sung TY, Kim M, Kim TY, Kim WG, Park Y,
Song DE, Park SY, Kwon H, Choi YM, Jang EK, et al: Negative
expression of CPSF2 predicts a poorer clinical outcome in patients
with papillary thyroid carcinoma. Thyroid. 25:1020–1025. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yi C, Wang Y, Zhang C, Xuan Y, Zhao S, Liu
T, Li W, Liao Y, Feng X, Hao J, et al: Cleavage and polyadenylation
specific factor 4 targets NF-κB/cyclooxygenase-2 signaling to
promote lung cancer growth and progression. Cancer Lett. 381:1–13.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chen W, Qin L, Wang S, Li M, Shi D, Tian
Y, Wang J, Fu L, Li Z, Guo W, et al: CPSF4 activates telomerase
reverse transcriptase and predicts poor prognosis in human lung
adenocarcinomas. Mol Oncol. 8:704–716. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tang Z, Yu W, Zhang C, Zhao S, Yu Z, Xiao
X, Tang R, Xuan Y, Yang W, Hao J, et al: CREB-binding protein
regulates lung cancer growth by targeting MAPK and CPSF4 signaling
pathway. Mol Oncol. 10:317–329. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen W, Guo W, Li M, Shi D, Tian Y, Li Z,
Wang J, Fu L, Xiao X, Liu QQ, et al: Upregulation of cleavage and
polyadenylation specific factor 4 in lung adenocarcinoma and its
critical role for cancer cell survival and proliferation. PLoS One.
8:e827282013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Appiah-Kubi K, Lan T, Wang Y, Qian H, Wu
M, Yao X, Wu Y and Chen Y: Platelet-derived growth factor receptors
(PDGFRs) fusion genes involvement in hematological malignancies.
Crit Rev Oncol Hematol. 109:20–34. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cancer Genome Atlas Research Network, ;
Weinstein JN, Collisson EA, Mills GB, Shaw KR, Ozenberger BA,
Ellrott K, Shmulevich I, Sander C and Stuart JM: The cancer genome
atlas Pan-cancer analysis project. Nat Genet. 45:1113–1120. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chang JT, Lee YM and Huang RS: The impact
of the Cancer Genome Atlas on lung cancer. Transl Res. 166:568–585.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhou JD, Wang YX, Zhang TJ, Li XX, Gu Y,
Zhang W, Ma JC, Lin J and Qian J: Identification and validation of
SRY-box containing gene family member SOX30 methylation as a
prognostic and predictive biomarker in myeloid malignancies. Clin
Epigenetics. 10:922018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fisler DA, Sikaria D, Yavorski JM, Tu YN
and Blanck G: Elucidating feed-forward apoptosis signatures in
breast cancer datasets: Higher FOS expression associated with a
better outcome. Oncol Lett. 16:2757–2763. 2018.PubMed/NCBI
|
|
25
|
Chen J, Fu G, Chen Y, Zhu G and Wang Z:
Gene-expression signature predicts survival benefit from
postoperative chemoradiotherapy in head and neck squamous cell
carcinoma. Oncol Lett. 16:2565–2578. 2018.PubMed/NCBI
|
|
26
|
Zhu Z, Yu YP, Shi Y, Nelson JB and Luo J:
CSR1 induces cell death through inactivation of CPSF3. Oncogene.
28:41–51. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tessema M, Yingling CM, Thomas CL, Klinge
DM, Bernauer AM, Liu Y, Dacic S, Siegfried JM, Dahlberg SE,
Schiller JH and Belinsky SA: SULF2 methylation is prognostic for
lung cancer survival and increases sensitivity to topoisomerase-I
inhibitors via induction of ISG15. Oncogene. 31:4107–4116. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Carney BJ, Rangachari D, VanderLaan PA,
Gowen K, Schrock AB, Ali SM and Costa DB: De novo ERBB2
amplification causing intrinsic resistance to erlotinib in
EGFR-L858R mutated TKI-naive lung adenocarcinoma. Lung Cancer.
114:108–110. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gu FF, Zhang Y, Liu YY, Hong XH, Liang JY,
Tong F, Yang JS and Liu L: Lung adenocarcinoma harboring
concomitant SPTBN1-ALK fusion, c-Met overexpression, and HER-2
amplification with inherent resistance to crizotinib, chemotherapy,
and radiotherapy. J Hematol Oncol. 9:662016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Pu W, Geng X, Chen S, Tan L, Tan Y, Wang
A, Lu Z, Guo S, Chen X and Wang J: Aberrant methylation of CDH13
can be a diagnostic biomarker for lung adenocarcinoma. J Cancer.
7:2280–2289. 2016. View Article : Google Scholar : PubMed/NCBI
|