Introduction
Pancreaticoduodenectomy (PD) is performed for tumors
of the pancreatic head, bile duct and ampulla of Vater. PD has a
high risk of postoperative pancreatic fistula, intra-abdominal
abscess and bleeding due to the fistula and delayed gastric
emptying (1,2), which causes malnutrition and impairs
quality of life. Complications related to postoperative pancreatic
fistula can be fatal. Ever since the reports by Watson in 1944
(3) and Traverso and Longmire in
1978 (4), reduction surgeries such
as pylorus-preserving PD (PPPD), subtotal stomach-preserving PD
(SSPPD) and duodenum-preserving pancreatic head resection have been
performed actively for organ preservation. The standard PD (SPD)
tends to be selected only for patients with simultaneous gastric
cancer or history of gastrectomy and patients with tumors of the
pancreatic head region involving the stomach. To reduce
complications after PD, the usefulness of these reduction surgeries
and perioperative predictive factors have been investigated
(1,2,5,6).
In recent years, the involvement of plasma ghrelin
in postoperative outcomes has been reported. Ghrelin was discovered
as an intrinsic ligand for the growth hormone-secretagogue receptor
(GHSR) in 1999 by Kojima et al (7). Ghrelin is peptide hormone mainly
produced in the stomach and has an active form acylated by ghrelin
O-acyltransferase and a desacyl form, which is a degradation
product. In healthy humans, the blood concentration of desacyl
ghrelin (DG) is about 4–5 times that of acyl ghrelin (AG). AG has
unique functions such as growth hormone secretion, promotion of
food intake and gastrointestinal motility, gastric acid secretion,
weight gain action and strong anti-inflammatory action (7–12). In
contrast, DG is not involved in growth hormone secretion activity,
but there are reports of actions on the promotion or suppression of
food intake, an anti-arteriosclerotic effect, suppression of
inflammatory cell infiltration, protection against muscle atrophy,
neuroprotection and others (13,14).
Depending on the procedure, PD can involve resection
of the stomach. However, studies on plasma ghrelin in patients
undergoing PD are rare. This study aimed to clarify the
significance of the perioperative plasma ghrelin level in PD
patients.
Patients and methods
Patients
This study is retrospective study. It was approved
by the Human Ethics Review Board of the University of Miyazaki on
2018/11/21 (reference number O-0426), and it conforms to the
provisions of the Declaration of Helsinki. Informed consent for
data collection was obtained from the patients using the opt-out
procedure. Patient data were retrieved from the departmental
database. Between April 2003 and December 2011, 195 patients
underwent PD for hepatobiliary pancreatic disease at the Division
of Hepato-Biliary-Pancreatic Surgery, Department of Surgery,
University of Miyazaki Faculty of Medicine in Japan. Plasma ghrelin
was measured in 83 of these patients. Among them, 14 patients had
benign disease (tumors and chronic inflammatory disease), and 69
had malignant tumors. Short-term outcomes were evaluated in all 83
patients, and long-term outcomes were evaluated in 69 patients
after excluding those with benign disease. To assess patient
condition, we used the following indices to respectively score
combined immunonutrition and inflammation status: The prognostic
nutritional index (PNI) and the high-sensitivity modified Glasgow
Prognostic Score (HS-mGPS) (15–18). The
following factors were examined: Age, sex, body mass index (BMI),
diabetes mellitus, preoperative biliary drainage, nutritional score
(PNI), inflammation-based prognostic score (HS-mGPS), serum tumor
markers [carcinoembryonic antigen (CEA), carbohydrate antigen
19-9], tumor location, tumor type, tumor size, pathological status
based on the international Union Against Cancer (UICC)
tumor-node-metastasis (TNM) classification (8th edition) (19), surgical procedure (SPD, PPPD, SSPPD),
portal vein resection, operation time, blood loss, severe
complications, postoperative hospital stay, adjuvant chemotherapy,
plasma ghrelin level and DG-to-AG ratio (D/A). We used the median
for the basic values for the analysis and the cut-off values
derived from receiver operating characteristic (ROC) analysis for
the tumor markers, plasma ghrelin and D/A. The PNI was calculated
as 10 × albumin (g/dl) + 0.005 × lymphocyte count (/µl). The
HS-mGPS was determined based on C-reactive protein (CRP) and
albumin levels. The scoring system was as follows: (1) Patients with a normal CRP value (<0.3
mg/dl) were allocated a score of 0, regardless of the albumin
level; (2) patients with a CRP level
≥0.3 mg/dl combined with an albumin level ≥3.5 g/dl were allocated
a score of 1; and (3) patients with
a CRP ≥0.3 mg/dl and an albumin <3.5 g/dl were allocated a score
of 2. Postoperative complications were classified using the
Clavien-Dindo grading system (20),
where grade III or higher represents morbidity.
Measurement of plasma ghrelin
levels
Blood samples were collected in a tube containing
aprotinin and ethylenediaminetetraacetic acid (Wako, Osaka, Japan)
before breakfast after an overnight fast. Plasma total ghrelin (TG)
concentrations were calculated as the AG concentration plus the DG
concentration. Blood sampling points were preoperatively, 2 weeks,
and 1, 6 and 12 months after surgery.
Surgical procedure
The same surgical team performed all operations and
oversaw the perioperative management. The operative technique was
essentially similar to that described previously (21). The organs resected during PD included
the gallbladder, common hepatic duct, head of the pancreas,
duodenum except for a 3–4 cm portion nearby the bulb and
approximately 10 cm of the proximal jejunum. The pancreas was
divided with a scalpel. The duodenum was transected approximately
3–4 cm distal to the pyloric ring for PPPD, and the stomach was
transected approximately 2–3 cm proximal to the pyloric ring at the
antrum in SSPPD. We performed pancreatojejunostomy by the
duct-to-mucosa method with eight interrupted sutures of 5-0 PDS-II
(polydioxanone; Johnson & Johnson Co.) and the modified Kakita
method with 3-0 Prolene (polypropylene; Johnson & Johnson Co.)
(22). An end-to-side
hepaticojejunostomy was then performed 5–10 cm distal from the
pancreatojejunostomy. Finally, end-to-side duodeno- or
gastrojejunostomy was performed to place the stomach and duodenum
into a straight vertical line as described for the retrocolic route
or the antecolic route, which was decided by randomized controlled
trial (23). A Braun anastomosis was
then created. Closed drains were inserted behind the
hepaticojejunostomy and at the upper side of the
pancreatojejunostomy. All patients received prophylactic
antibiotics for 3 days and an H2 blocker or proton pump
inhibitor to prevent stress peptic ulcer. None of the patients
received octreotide.
Adjuvant chemotherapy
In 2016, the Japan Adjuvant Study Group of
Pancreatic Cancer (JASPAC) reported the results of a phase III
study of S-1 vs. gemcitabine (GEM) for resected pancreatic cancer.
S-1 significantly prolonged overall survival (OS) and relapse-free
survival, and S-1 therapy is currently recommended (24). At the time of the present study,
there was no evidence on adjuvant therapy for pancreatic cancer,
and various methods such as S-1, GEM or S-1+GEM were selected.
Evidence for adjuvant chemotherapy for biliary carcinoma and
ampullary carcinoma was still lacking at the time GEM or
GEM+cisplatin were chosen.
Statistical analysis
Clinical parameters are expressed as the number (%)
or median value and range. Comparisons between groups were made
using the χ2 test for categorical variables and the
Mann-Whitney U test for continuous variables. The difference
between plasma ghrelin concentrations at different time-points was
tested for significance using a Friedman test followed by a post
hoc Bonferroni correction. Survival was analyzed using the
Kaplan-Meier method, and the log-rank test was used to determine
the differences between the two groups. The cutoff for definition
of a subgroup was determined by a ROC analysis. A univariate
analysis was performed to assess significant differences in
clinicopathological characteristics. The independent risk factors
affecting severe complications and prognostic factors were
determined by multivariate analysis using a Cox proportional
hazards model for variables that were significant following
univariate analysis. The associated 95% confidence interval (CI)
was subsequently determined. P<0.05 was considered statistically
significant. Statistical analyses were performed using JMP
11® (SAS Institute Inc., Cary, NC, USA).
Results
Clinicopathological
characteristics
PD was performed in 83 patients (49 men, 34 women)
with a median age of 70 (range 36–85) years: 63 underwent PPPD, 11
SSPPD and 9 SPD for diagnoses that included pancreatic disease
(n=47), bile duct disease (n=24) and ampullary tumor (n=12). The
clinicopathological characteristics of the SPD group (n=9) and
Non-SPD group (n=74) are summarized in Table I. Of the 83 patients, 69 had a
malignant tumor (pancreatic carcinoma: 36, bile duct carcinoma: 22,
ampullary carcinoma: 11 patients). Thirty-three patients (47.8%)
had diabetes mellitus, and 44 (63.8%) required biliary drainage for
preoperative jaundice and cholangitis. The progression of cancer by
TNM classification tended toward advanced cases (Stage I: 9, II:
25, III: 35 patients). The clinicopathological characteristics of
the pancreatic carcinoma group (PCG, n=36) and the non-pancreatic
carcinoma group (Non-PCG, n=33) are summarized in Table II. The PCG included many patients
with deeper invasive lesions (P=0.0156) and portal vein resection
(38.9% vs. 0.0%, P<0.0001) and adjuvant chemotherapy (86.1% vs.
63.6%, P=0.0304). In the Non-PCG, more patients required
preoperative biliary drainage than in the PCG (78.8% vs. 50.0%,
P=0.0130).
 | Table I.Clinicopathological characteristics
of patients undergoing SPD and non-SPD. |
Table I.
Clinicopathological characteristics
of patients undergoing SPD and non-SPD.
| Variables | SPD (n=9) | Non-SPD (n=74) | P-value |
|---|
| Age, years [median
(range)] | 76 (61–79) | 69 (36–85) | 0.1220 |
| Sex
(male/female) | 7/2 | 42/32 | 0.2260 |
| BMI,
kg/m2 [median, (range)] | 19.5
(16.3–24.4) | 20.8
(13.8–29.0) | 0.3448 |
| Diabetes
mellitus | 3 (33.3%) | 32 (43.2%) | 0.5697 |
| Preoperative
biliary drainage | 3 (33.3%) | 47 (63.5%) | 0.0807 |
| PNI [median,
(range)] | 44.1
(42.3–49.2) | 43.7
(29.4–51.4) | 0.6102 |
| HS-mGPS
(0/1/2) | 7/2/0 | 48/10/16 | 0.2768 |
| Tumor location
(pancreas/bile duct/ampulla) | 5/3/1 | 42/21/11 | 0.9285 |
| Tumor type
(malignant/benign) | 9/0 | 60/14 | 0.1524 |
| Portal vein
resection n(%) | 3 (33.3%) | 11 (14.9%) | 0.1624 |
| Operation time, min
[median, (range)] | 675 (552–726) | 579 (427–967) | 0.0514 |
| Blood loss, ml
[median (range)] | 1800
(1150–3040) | 1455
(440–6870) | 0.2472 |
| CD score ≥III
n(%) | 5 (55.6%) | 21 (28.4%) | 0.0970 |
| Postoperative
hospital stay, days [median (range)] | 37 (29–49) | 36 (24–116) | 0.9649 |
| Preoperative
ghrelin, fmol/ml [median (range)] |
| AG | 2.19
(1.21–12.41) | 7.28
(0.15–59.36) | 0.0250 |
| DG | 20.31
(4.49–66.60) | 44.26
(3.08–306.39) | 0.0994 |
| Total
ghrelin | 22.47
(6.70–79.01) | 54.70
(4.36–313.65) | 0.0489 |
|
DG-to-AG ratio | 6.00
(2.03–34.34) | 4.36
(1.05–142.11) | 0.3087 |
| Table II.Clinicopathological characteristics
of the PCG and non-PCG patients. |
Table II.
Clinicopathological characteristics
of the PCG and non-PCG patients.
| Variables | PCG (n=36) | Non-PCG (n=33) | P-value |
|---|
| Age, years [median
(range)] | 68.5 (43–85) | 69.0 (51–82) | 0.9091 |
| Sex
(male/female) | 15/21 | 24/9 | 0.0093 |
| BMI,
kg/m2 [median (range)] | 20.7
(13.8–28.4) | 22.3
(16.3–29.0) | 0.4208 |
| Diabetes mellitus
n(%) | 21 (58.3%) | 12 (36.4%) | 0.0680 |
| Preoperative
biliary drainage n(%) | 18 (50.0%) | 26 (78.8%) | 0.0130 |
| PNI [median
(range)] | 43.7
(29.4–51.4) | 43.6
(33.9–50.6) | 0.9605 |
| HS-mGPS
(0/1/2) | 26/4/6 | 19/6/8 | 0.4388 |
| Tumor marker |
|
|
|
| CEA,
ng/ml [median (range)] | 2.8 (0.6–17.6) | 2.4 (0.8–10.5) | 0.4276 |
| CA19-9,
U/ml [median, (range)] | 100.4
(1.0–8132.8) | 32.0
(2.0–31462) | 0.1598 |
| Tumor size, mm
[median, (range)] | 30 (3–85) | 26 (15–63) | 0.2604 |
| Pathological depth
of invasion (T1/T2/T3/T4) | 5/1/13/17 | 4/10/10/9 | 0.0156 |
| Pathological nodal
stage (N0/N1/N2) | 15/12/9 | 17/12/4 | 0.3826 |
| Metastatic lymph
nodes, n [median, (range)] | 1 (0–25) | 0 (0–6) | 0.1208 |
| Stage
(I/II/III) | 4/10/22 | 5/15/13 | 0.0904 |
| Performed operation
(SPD/PPPD/SSPPD) | 5/22/9 | 4/27/2 | 0.0840 |
| Portal vein
resection n(%) | 14 (38.9%) | 0 (0%) | <0.0001 |
| Operation time, min
[median, (range)] | 654 (450–967) | 580 (432–934) | 0.6096 |
| Blood loss, ml
[median, (range)] | 1520
(460–6870) | 1800
(700–5930) | 0.3158 |
| CD score ≥III
n(%) | 2 (5.6%) | 18 (54.6%) | <0.0001 |
| Postoperative
hospital stay, days [median, (range)] | 33 (25–49) | 43 (25–116) | 0.0012 |
| Adjuvant
chemotherapy n(%) | 31 (86.1%) | 21 (63.6%) | 0.0304 |
| Preoperative
ghrelin, fmol/ml, [median, (range)] |
|
|
|
| AG | 7.09
(0.86–21.78) | 6.30
(0.55–59.36) | 0.8288 |
| DG | 45.88
(3.27–120.85) | 40.75
(4.49–306.39) | 0.7502 |
| Total
ghrelin | 54.70
(4.89–128.15) | 46.57
(6.70–313.65) | 0.8806 |
|
DG-to-AG ratio | 4.94
(1.19–40.90) | 4.92
(1.05–142.11) | 0.9665 |
Plasma ghrelin and immunonutritional
status
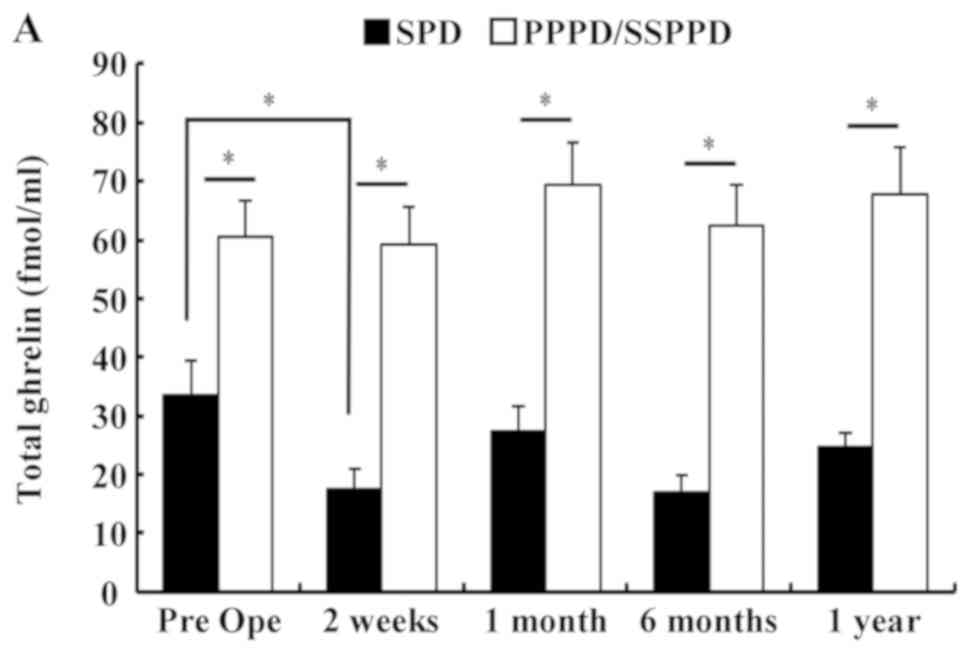
Fig. 1 shows the
chronological change of plasma TG and D/A after PD. The TG in
patients who underwent SPD was significantly lower than that in
those who underwent PPPD or SSPPD (Fig.
1A). In SPD patients, TG had declined significantly at 2 weeks
after surgery (mean, preoperative 32.8 vs. 2 weeks postoperatively
15.9 fmol/ml, P=0.0388). There were no significant differences at
other times points. Table I shows
the significant difference between the SPD group and the Non-SPD
group in AG and TG, but shows no difference in the D/A. The
perioperative D/A declined significantly at 6 months after surgery
in patients with SPD (mean; preoperative, 10.6 vs. 6 months
postoperatively, 4.5; P=0.0234), but there were no significant
differences at other time points (Fig.
1B). In all 83 patients, the median preoperative values of AG,
DG, TG and D/A were 6.49, 40.86, 47.33 fmol/ml and 4.92. The cutoff
values for morbidity of AG, DG, TG and D/A calculated by ROC
analysis were 10.6, 41.6, 47.3 fmol/ml and 3.1. The median PNI was
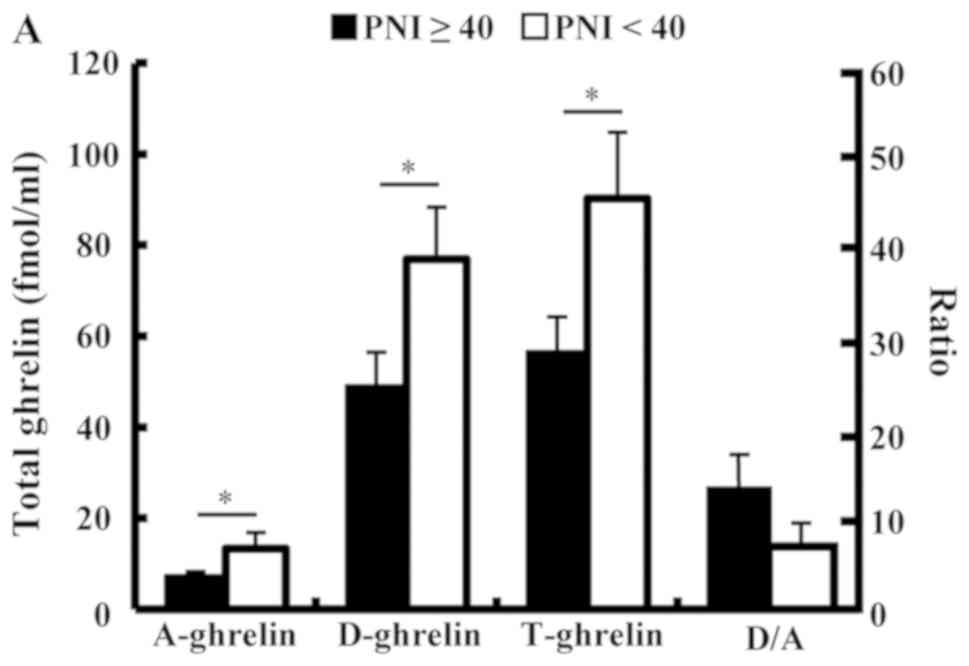
43.7, and 55 patients (66.3%) had a HS-mGPS score of 0. The plasma
ghrelin levels of the high PNI group (PNI ≥40) were significantly
lower than those of the low PNI group (PNI <40) and showed a
negative association. The D/A of the high PNI group (PNI ≥40)
tended to be higher than low PNI group, but there was no
significant difference (Fig. 2A).
The TG level in the patients with a HS-mGPS score of 1 was
significantly lower than that of those with a score of 2 (score 1:
26.9 vs. score 2: 78.8 fmol/ml, P=0.0451). The D/A in the patients
with a HS-mGPS score of 0 tended to be higher than other score
group, but there was no significant difference (Fig. 2B).
Surgical outcomes
In the 83 patients, the median operation time and
blood loss were 607 min and 1520 ml, respectively. The morbidity
rate was 31.3%, and the severe complications were pancreatic
fistula (14.5%), intra-abdominal abscess (15.7%), intra-abdominal
bleeding (6.0%) and liver abscess (1.2%). As shown in Table I, the Non-PCG had more severe
complications than the PCG (54.6% vs. 5.6%, P<0.0001).
Univariate and multivariate analyses
of clinical factors associated with morbidity
Clinical factors affecting severe complications were
evaluated by univariate and multivariate analyses (Table III). A univariate analysis showed
that sex [male, hazard ratio (HR): 3.22, P=0.0291], location of the
disease (not pancreas, HR: 8.54, P<0.0001) and D/A (<3.1, HR:
6.23, P=0.0018) were significant variables influencing unfavorable
morbidity. Among them, location of the disease (not pancreas, HR:
9.64, P=0.0005) and D/A (<3.1, HR: 5.34, P=0.0292) remained as
independent risk factors for severe complications in a subsequent
multivariate analysis.
| Table III.Univariate and multivariate analyses
of clinical factors affecting severe complications (n=83). |
Table III.
Univariate and multivariate analyses
of clinical factors affecting severe complications (n=83).
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variables | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age (≥70
years) | 2.42 | 0.92–6.33 | 0.0722 |
|
|
|
| Sex (male) | 3.22 | 1.13–9.19 | 0.0291 | 1.99 | 0.56–7.06 | 0.2857 |
| BMI (<20.8
kg/m2) | 1.04 | 0.41–2.62 | 0.9409 |
|
|
|
| Diabetes mellitus
(yes) | 2.62 | 0.95–7.20 | 0.0616 |
|
|
|
| Preoperative
biliary drainage (yes) | 1.76 | 0.66–4.70 | 0.2610 |
|
|
|
| PNI (<40.0) | 0.75 | 0.18–3.05 | 0.6876 |
|
|
|
| HS-mGPS (1+2) | 1.72 | 0.66–4.52 | 0.2669 |
|
|
|
| Disease location
(not pancreas) | 8.54 | 2.90–25.15 | <0.0001 | 9.64 | 2.71–34.35 | 0.0005 |
| Tumor type
(benign) | 1.27 | 0.38–4.25 | 0.6982 |
|
|
|
| Performed operation
(PPPD) | 1.09 | 0.36–3.24 | 0.8834 |
|
|
|
| Portal vein
resection (yes) | 0.55 | 0.14–2.15 | 0.3863 |
|
|
|
| Operation time
(≥607 min) | 0.77 | 0.30–1.96 | 0.5844 |
|
|
|
| Blood loss (≥1520
ml) | 1.52 | 0.59–3.86 | 0.3841 |
|
|
|
| Preoperative plasma
ghrelin (fmol/ml) |
|
|
|
|
|
|
| AG
(<10.6) | 1.79 | 0.58–5.52 | 0.3142 |
|
|
|
| DG
(<41.6) | 3.09 | 1.16–8.28 | 0.0246 | 2.21 | 0.61–8.08 | 0.2289 |
| Total
ghrelin (<47.3) | 2.60 | 0.99–6.81 | 0.0523 |
|
|
|
|
DG-to-AG ratio (<3.1) | 6.23 | 1.98–19.67 | 0.0018 | 5.34 | 1.19–24.03 | 0.0292 |
Survival analyses
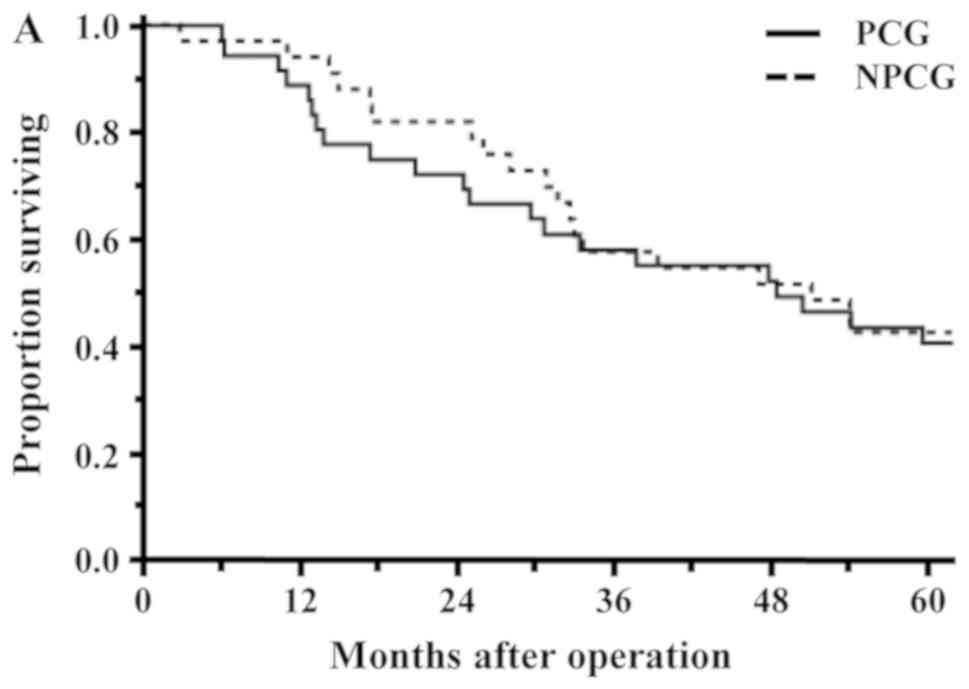
Long-term results were examined in the 69 patients
with malignant tumor. The rate of 5-year OS in all patients was
41.5%. The OS rates of the PCG and Non-PCG were 40.7 and 42.4%,
respectively, and the survival rate between the two groups was not
significantly different (P=0.8773; Fig.
3A). The survival rate between the SPD group and PPPD/SSPPD
group was also not significantly different (44.4% vs. 41.0%,
P=0.8199; Fig. 3B).
Univariate and multivariate analyses
of prognostic factors
Factors associated with OS were evaluated by
univariate and multivariate analyses (Table IV). A univariate analysis showed
that diabetes mellitus (Yes, P=0.0001), CEA (≥4.6 ng/ml, P=0.0301),
pathological depth of invasion (T4, P=0.0043), performed operation
(PPPD, P=0.0313), blood loss (≥1565 g, P=0.0103), postoperative
hospital stay (≥36 days, P=0.0144) and D/A (<3.1, P=0.0012) were
significant variables influencing unfavorable OS. Among them,
diabetes mellitus (Yes, HR: 3.47, P=0.0014), postoperative hospital
stay (≥36 days, HR: 2.28, P=0.0371) and D/A (<3.1, HR: 4.73,
P=0.0010) remained as independent risk factors for OS in a
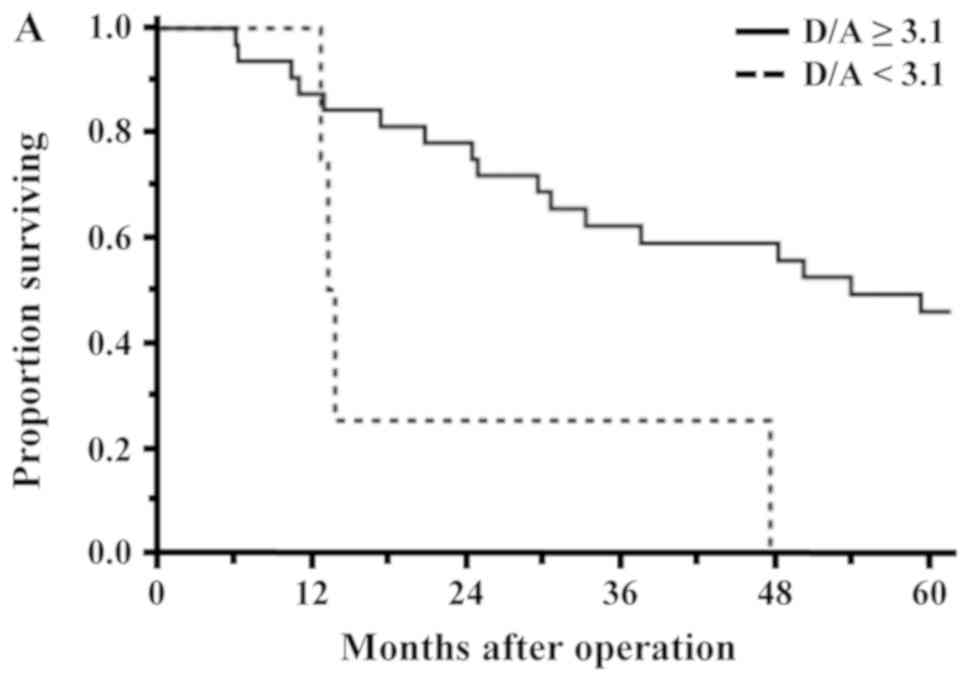
subsequent multivariate analysis. The rates of OS of the low D/A
group (D/A <3.1) and high D/A group (D/A ≥3.1) were 15.4 and
47.6%, respectively (P=0.0134). In the patients of the PCG and
Non-PCG, the rates of OS between the low D/A group and high D/A
group were 0.0% vs. 50.8% (P=0.0040) and 11.1% vs. 50.0%
(P=0.0247), respectively, and were significantly different
(Fig. 4A and B).
| Table IV.Univariate and multivariate analyses
of prognostic factors (n=69). |
Table IV.
Univariate and multivariate analyses
of prognostic factors (n=69).
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variables | P-value | HR | 95% CI | P-value |
|---|
| Age (≥69
years) | 0.1924 |
|
|
|
| Sex (male) | 0.5077 |
|
|
|
| BMI (≥21.2
kg/m2) | 0.0349 | 1.23 | 0.62–2.48 | 0.5568 |
| Diabetes mellitus
(yes) | 0.0002 | 2.79 | 1.37–5.75 | 0.0046 |
| Preoperative
biliary drainage (yes) | 0.3491 |
|
|
|
| PNI (<40.0) | 0.4849 |
|
|
|
| HS-mGPS (1+2) | 0.5406 |
|
|
|
| Tumor marker |
|
|
|
|
| CEA
(≥4.9 ng/ml) | 0.0464 | 2.07 | 0.89–4.56 | 0.0898 |
| CA19-9
(≥500.0 U/ml) | 0.0094 | 1.42 | 0.66–2.90 | 0.3589 |
| Tumor location (not
pancreas) | 0.8773 |
|
|
|
| Tumor size (≥30
mm) | 0.0101 | 2.20 | 1.02–4.75 | 0.0452 |
| Pathological depth
of invasion (T4) | 0.0095 | 1.35 | 0.67–2.67 | 0.3987 |
| Lymph node
metastasis (yes) | 0.1049 |
|
|
|
| Stage (III) | 0.0816 |
|
|
|
| Performed operation
(PPPD) | 0.1921 |
|
|
|
| Portal vein
resection (yes) | 0.2831 |
|
|
|
| Operation time
(≥631 min) | 0.0478 | 1.01 | 0.47–2.23 | 0.9771 |
| Blood loss (≥1580
ml) | 0.0224 | 1.34 | 0.57–3.10 | 0.5006 |
| CD score
(≥III) | 0.3294 |
|
|
|
| Postoperative
hospital stay (≥36 days) | 0.0336 | 2.09 | 1.13–3.96 | 0.0181 |
| Adjuvant
chemotherapy (yes) | 0.5544 |
|
|
|
| Preoperative plasma
ghrelin (fmol/ml) |
|
|
|
|
| AG (<10.6) | 0.1529 |
|
|
|
| DG (<41.6) | 0.0950 |
|
|
|
| Total ghrelin
(<47.3) | 0.2743 |
|
|
|
| DG-to-AG ratio
(<3.1) | 0.0134 | 3.06 | 1.34–6.76 | 0.0089 |
Discussion
There are many reports on plasma ghrelin after
gastrectomy and esophagectomy (10,12), but
there are very few reports after PD. Until now, perioperative
change of the plasma ghrelin level, such as transient suppression
during the day following pancreatectomy and its significance as a
predictive marker of postoperative complications have been reported
(25,26). The present study is the first report,
to our knowledge, to evaluate plasma ghrelin in relation to
long-term outcomes.
In the present study, the plasma ghrelin levels did
not change significantly over a one-year period, but the ghrelin
level in the SPD patients was significantly lower than that in the
PPPD/SSPPD patients. Seven of the SPD patients had undergone distal
gastrectomy for gastric cancer in the past, and their ghrelin
levels were already low prior to the SPD. Postoperatively, plasma
ghrelin tends to recover to a normal level with time in patients
who have undergone distal gastrectomy (27). Nine patients in this study underwent
PD a median 6 (range 2–47) years after gastrectomy. Although
Helicobacter pylori infection was not investigated in this
study, H. pylori infection and the brevity of the period
from gastrectomy to PD may have affected the delayed recovery of
plasma ghrelin. Suppression of plasma ghrelin has been reported in
patients with H. pylori (28). Takachi et al (10) indicated the possibility of
compensatory ghrelin production in the remnant stomach and
duodenum. As ghrelin does not recover in patients with total
gastrectomy (10,27), the influence of the residual stomach
is significant, and a significant decline in ghrelin after SPD also
suggests an association with duodenal compensation. The decrease in
D/A 6 months after surgery may be the effect of decompensation due
to residual stomach and duodenum, and recovery 1 year after surgery
may be related to the restoration of compensation by other
organs.
The PNI and HS-mGPS used in the present study are
known as prognostic factors for patients with cancer (15–18).
Plasma ghrelin and PNI in this study showed an inverse association.
In the HS-mGPS, ghrelin is inversely associated with serum albumin,
a nutritional indicator, irrespective of the inflammatory state.
Ghrelin promotes food intake, and an inverse association between
plasma ghrelin concentration and BMI has been shown (29,30). Our
results can be explained that fasting due to preoperative jaundice
and cholangitis develops into malnutrition, and as a result,
ghrelin increased as positive feedback in the low PNI group and
HS-mGPS score 2 group. In the present study, PNI and HS-GPS were
not independent factors in the analyses of risk factors of
morbidity and mortality. Depending on the control of obstructive
jaundice and cholangitis, the high inflammatory state can last and
progress to malnutrition and weight loss (31). It is speculated that the relatively
good control of jaundice and cholangitis in the present study
patients affected the analyses between the PNI and HS-GPS and
outcomes. The D/A tended to be higher in the good group of
conditions, whether PNI or HS-mGPS, as opposed to the inversely
associated plasma ghrelin concentrations. It may be that DG which
is still insufficiently researched is involved.
As mentioned above, plasma ghrelin, especially AG
and TG, has been reported to be associated with surgery outcomes.
The present study focused specifically on D/A because it included
SPD patients with significantly lower plasma ghrelin levels. There
was no significant difference between morbidity and mortality
between the SPD group and Non-SPD group. Therefore, we suggest that
relative evaluation by D/A is important rather than evaluation
based on the absolute value of plasma ghrelin. In the multivariate
analyses of morbidity and mortality, a lower D/A was an independent
risk factor. A high preoperative AG level is the result of feedback
on malnutrition and inflammatory response and may cause
postoperative complications and a poor prognosis. Previous studies
reported that ghrelin associated with cancer cell proliferation,
invasion and migration in cell lines of pancreatic, breast, renal
and colorectal cancer (32–35). The correlation of the ghrelin gene
and GHSR expression in cancer patients with prognosis was also
reviewed (36). However, AG alone
cannot be a risk factor, and the involvement of DG is
indispensable. Some reports indicated that DG protects
cardiomyocytes from ischemic injury and promotes muscle
regeneration and inhibit apoptosis in myoblasts cocultured with
colon carcinoma cells (37,38). Specific receptors of DG that promote
these activities have not been identified, and a feedback mechanism
such as that with AG is unknown. Further research on the
relationship with AG is also necessary.
One limitation of the present study is that the
background of the subjects is unbalanced. The disease indication
for PD is not unified, the tumor factors are irregular, and only a
very few patients underwent SPD or SSPPD with resection of the
stomach. Although not presented in this report, the tumor size,
diabetes mellitus and postoperative hospital stay listed as poor
prognosis factors other than D/A ratio were particularly involved
in the PCG. Another limitation is the insufficient extraction of
factors that affect ghrelin production and feedback. In addition to
nutrition and inflammation, H. pylori infection and cachexia
status affect ghrelin production (28,39,40).
These factors cannot be ignored because the rate of H.
pylori infection is higher in Japanese people, and the
progression of pancreatic and biliary carcinoma is strongly related
to cachexia (41,42).
This study showed the D/A to be a potentially useful
predictive factor for postoperative complications and prognosis
after PD. Based on the outcomes of SPD cases with decreased
preoperative plasma ghrelin, the absolute value of plasma ghrelin
alone cannot explain complications or prognosis. Because of the
limitations of a small sample size and the single-institution
nature of this study, it will be necessary to conduct a
prospective, large, multicenter trial in patients to fully take
into consideration patient, tumor and surgical factors. The
mechanism of the physiological activity of DG must be elucidated in
the next step.
Acknowledgements
The authors would like to thank Professor Kazuo
Chijiiwa (Department of Surgery, University of Miyazaki Faculty of
Medicine, deceased November 26, 2013) for designing the present
study and performing surgery. The authors would like to acknowledge
Dr Jiro Ohuchida (Department of Surgery, Miyazaki Prefectural
Miyazaki Hospital), Dr Motoaki Nagano (Department of Surgery,
Miyazaki Medical Center Hospital) and Dr Yoshiro Fujii (Department
of Surgery, Yokohama City University Medical Center) who assisted
with performed the surgery, blood sampling and follow-up care.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
TN performed the surgery, analyzed the data and
wrote the manuscript. HT measured plasma ghrelin levels and
analyzed the data. TH performed the surgery and analyzed the data.
NI, MH and KY performed the surgery, blood sampling and follow-up
care. AN contributed to surgical and survival analyses,
univariate/multivariate analyses and reviewed the manuscript. KK
and MN conceived and designed the current study, measured plasma
ghrelin levels, analyzed plasma ghrelin and immunonutritional
status and critically revised the manuscript. All authors read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Human Ethics
Review Board of the University of Miyazaki (approval no. O-0426)
and conformed to the provisions of the Declaration of Helsinki.
Informed consent for data collection was obtained from all patients
using an opt-out procedure. Patient data were retrieved from the
departmental database.
Patient consent for publication
Patient consent for publication was obtained from
the patients using the opt-out procedure.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AG
|
acyl ghrelin
|
|
BMI
|
body mass index
|
|
CD
|
Clavien-Dindo score
|
|
CEA
|
carcinoembryonic antigen
|
|
CRP
|
C-reactive protein
|
|
D/A
|
DG-to-AG ratio
|
|
DG
|
desacyl ghrelin
|
|
GEM
|
gemcitabine
|
|
GHSR
|
growth hormone-secretagogue
receptor
|
|
HS-mGPS
|
high-sensitivity modified Glasgow
Prognostic Score
|
|
OS
|
overall survival
|
|
PD
|
pancreaticoduodenectomy
|
|
PNI
|
prognostic nutritional index
|
|
PPPD
|
pylorus-preserving
pancreaticoduodenectomy
|
|
ROC
|
receiver operating characteristic
|
|
SPD
|
standard pancreaticoduodenectomy
|
|
SSPPD
|
subtotal stomach-preserving
pancreaticoduodenectomy
|
|
TG
|
total ghrelin
|
References
|
1
|
Diener MK, Knaebel HP, Heukaufer C, Antes
G, Büchler MW and Seiler CM: A systematic review and meta-analysis
of pylorus-preserving versus classical pancreaticoduodenectomy for
surgical treatment of periampullary and pancreatic carcinoma. Ann
Surg. 245:187–200. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang W, Xiong JJ, Wan MH, Szatmary P,
Bharucha S, Gomatos I, Nunes QM, Xia Q, Sutton R and Liu XB:
Meta-analysis of subtotal stomach-preserving
pancreaticoduodenectomy vs. pylorus preserving
pancreaticoduodenectomy. World J Gastroenterol. 21:6361–6373. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Watson K: Carcinoma of ampulla of vater
successful radical resection. Br J Surg. 31:368–373. 1944.
View Article : Google Scholar
|
|
4
|
Traverso LW and Longmire WJ: Preservation
of the pylorus in pancreaticoduodenectomy. Surg Gynecol Obstet.
146:959–962. 1978.PubMed/NCBI
|
|
5
|
Hiyoshi M, Chijiiwa K, Ohuchida J, Imamura
N and Nagano M: Comparative study of gastric emptying and
nutritional status after pylorus-preserving vs. subtotal
stomach-preserving pancreaticoduodenectomy. Hepatogastroenterology.
59:1018–1022. 2012.PubMed/NCBI
|
|
6
|
Zhao R, Chang Y, Wang X, Zhang P, Zhang C
and Lian P: Pylorus-preserving pancreaticoduodenectomy versus
standard pancreaticoduodenectomy in the treatment of duodenal
papilla carcinoma. Oncol Lett. 15:6368–6376. 2018.PubMed/NCBI
|
|
7
|
Kojima M, Hosoda H, Date Y, Nakazato M,
Matsuo H and Kangawa K: Ghrelin is a growth-hormone-releasing
acylated peptide from stomach. Nature. 402:656–660. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Asakawa A, Inui A, Kaga T, Yuzuriha H,
Nagata T, Ueno N, Makino S, Fujimiya M, Niijima A, Fujino MA and
Kasuga M: Ghrelin is an appetite-stimulatory signal from stomach
with structural resemblance to motilin. Gastroenterology.
120:337–345. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Muccioli G, Tschöp M, Papotti M, Deghenghi
R, Heiman M and Ghigo E: Neuroendocrine and peripheral activities
of ghrelin: Implications in metabolism and obesity. Eur J
Pharmacol. 440:235–254. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Takachi K, Doki Y, Ishikawa O, Miyashiro
I, Sasaki Y, Ohigashi H, Murata K, Nakajima H, Hosoda H, Kangawa K,
et al: Postoperative ghrelin levels and delayed recovery from body
weight loss after distal or total gastrectomy. J Surg Res. 130:1–7.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Doki Y, Takachi K, Ishikawa O, Miyashiro
I, Sasaki Y, Ohigashi H, Nakajima H, Hosoda H, Kangawa K, Sasakuma
F, et al: Ghrelin reduction after esophageal substitution and its
correlation to postoperative body weight loss in esophageal cancer
patients. Surgery. 139:797–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takiguchi S, Murakami K, Yanagimoto Y,
Takata A, Miyazaki Y, Mori M and Doki Y: Clinical application of
ghrelin in the field of surgery. Surg Today. 45:801–807. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsuchimochi W, Kyoraku I, Yamaguchi H,
Toshinai K, Shiomi K, Kangawa K and Nakazato M: Ghrelin prevents
the development of experimental diabetic neuropathy in rodents. Eur
J Pharmacol. 702:187–193. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yano Y, Nakazato M, Toshinai K, Inokuchi
T, Matsuda S, Hidaka T, Hayakawa M, Kangawa K, Shimada K and Kario
K: Circulating des-acyl ghrelin improves cardiovascular risk
prediction in older hypertensive patients. Am J Hypertens.
27:727–733. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kanda M, Fujii T, Kodera Y, Nagai S,
Takeda S and Nakao A: Nutritional predictors of postoperative
outcome in pancreatic cancer. Br J Surg. 98:268–274. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang P, Xi M, Li QQ, He LR, Liu SL, Zhao
L, Shen JX and Liu MZ: The modified glasgow prognostic score is an
independent prognostic factor in patients with inoperable thoracic
esophageal squamous cell carcinoma undergoing chemoradiotherapy. J
Cancer. 5:689–695. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chen P, Fang M, Wan Q, Zhang X, Song T and
Wu S: High-sensitivity modified Glasgow prognostic score (HS-mGPS)
is superior to the mGPS in esophageal cancer patients treated with
chemoradiotherapy. Oncotarget. 8:99861–99870. 2017.PubMed/NCBI
|
|
18
|
Cui Y, Li J, Cao YH, Liu MY, Shi ZX and
Gao TH: Predictive and prognostic significance of high-sensitivity
modified glasgow prognostic score (HS-mGPS) in advanced gastric
cancer patients treated with neoadjuvant chemotherapy. Zhonghua
Zhong Liu Za Zhi. 39:195–200. 2017.(In Chinese). PubMed/NCBI
|
|
19
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM classification of malignant tumors8th.
Wiley-Blackwell; 2017
|
|
20
|
Dindo D, Demartines N and Clavien PA:
Classification of surgical complications: A new proposal with
evaluation in a cohort of 6336 patients and results of a survey.
Ann Surg. 240:205–213. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hiyoshi M, Chijiiwa K, Fujii Y, Imamura N,
Nagano M and Ohuchida J: Usefulness of drain amylase, serum
C-reactive protein levels and body temperature to predict
postoperative pancreatic fistula after pancreaticoduodenectomy.
World J Surg. 37:2436–2442. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kakita A, Yoshida M and Takahashi T:
History of pancreaticojejunostomy in pancreaticoduodenectomy:
Development of a more reliable anastomosis technique. J
Hepatobiliary Pancreat Surg. 8:230–237. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chijiiwa K, Imamura N, Ohuchida J, Hiyoshi
M, Nagano M, Otani K, Kai M and Kondo K: Prospective randomized
controlled study of gastric emptying assessed by (13)C-acetate
breath test after pylorus-preserving pancreaticoduodenectomy:
Comparison between antecolic and vertical retrocolic
duodenojejunostomy. J Hepatobiliary Pancreat Surg. 16:49–55. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Uesaka K, Boku N, Fukutomi A, Okamura Y,
Konishi M, Matsumoto I, Kaneoka Y, Shimizu Y, Nakamori S, Sakamoto
H, et al: Adjuvant chemotherapy of S-1 versus gemcitabine for
resected pancreatic cancer: A phase 3, open-label, randomised,
non-inferiority trial (JASPAC 01). Lancet. 388:248–257. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nanashima A, Murakami G, Takagi K, Arai J,
Sumida Y, Kodama T and Nagayasu T: Relationship between serum
ghrelin level and physiology in patients who underwent hepatectomy
and pancreatectomy. Acta Med Nagasaki. 61:55–60. 2017.
|
|
26
|
Sasaki K, Asaoka T, Eguchi H, Fukuda Y,
Iwagami Y, Yamada D, Miyazaki Y, Noda T, Takahashi T, Gotoh K, et
al: Plasma ghrelin suppression as an early predictor for
postoperative complications after pancreatoduodenectomy.
Pancreatology. 18:73–78. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Takiguchi S, Takata A, Murakami K,
Miyazaki Y, Yanagimoto Y, Kurokawa Y, Takahashi T, Mori M and Doki
Y: Clinical application of ghrelin administration for gastric
cancer patients undergoing gastrectomy. Gastric Cancer. 17:200–205.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kasai C, Sugimoto K, Moritani I, Tanaka J,
Oya Y, Inoue H, Tameda M, Shiraki K, Ito M, Takei Y and Takase K:
Changes in plasma ghrelin and leptin levels in patients with peptic
ulcer and gastritis following eradication of Helicobacter
pylori infection. BMC Gastroenterol. 16:1192016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shiiya T, Nakazato M, Mizuta M, Date Y,
Mondal MS, Tanaka M, Nozoe S, Hosoda H, Kangawa K and Matsukura S:
Plasma ghrelin levels in lean and obese humans and the effect of
glucose on ghrelin secretion. J Clin Endocrinol Metab. 87:240–244.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Date Y, Murakami N, Toshinai K, Matsukura
S, Niijima A, Matsuo H, Kangawa K and Nakazato M: The role of the
gastric afferent vagal nerve in ghrelin-induced feeding and growth
hormone secretion in rats. Gastroenterology. 123:1120–1128. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kumamoto Y, Kaizu T, Tajima H, Nishizawa
N, Ei S, Igarashi K and Watanabe M: Neutrophil-to-lymphocyte ratio
as a predictor of postoperative morbidity in patients with distal
cholangiocarcinoma. Mol Clin Oncol. 9:362–368. 2018.PubMed/NCBI
|
|
32
|
Duxbury MS, Waseem T, Ito H, Robinson MK,
Zinner MJ, Ashley SW and Whang EE: Ghrelin promotes pancreatic
adenocarcinoma cellular proliferation and invasiveness. Biochem
Biophys Res Commun. 309:464–468. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Jeffery PL, Murray RE, Yeh AH, McNamara
JF, Duncan RP, Francis GD, Herington AC and Chopin LK: Expression
and function of the ghrelin axis, including a novel preproghrelin
isoform, in human breast cancer tissues and cell lines. Endocr
Relat Cancer. 12:839–850. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lin TC, Liu YP, Chan YC, Su CY, Lin YF,
Hsu SL, Yang CS and Hsiao M: Ghrelin promotes renal cell carcinoma
metastasis via Snail activation and is associated with poor
prognosis. J Pathol. 237:50–61. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Waseem T, Javaid-Ur-Rehman, Ahmad F, Azam
M and Qureshi MA: Role of ghrelin axis in colorectal cancer: A
novel association. Peptides. 29:1369–1376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lin TC and Hsiao M: Ghrelin and cancer
progression. Biochim Biophys Acta Rev Cancer. 1868:51–57. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yanagi S, Sato T, Kangawa K and Nakazato
M: The homeostatic force of ghrelin. Cell Metab. 27:786–804. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zeng X, Chen S, Lin Y and Ke Z: Acylated
and unacylated ghrelin inhibit apoptosis in myoblasts cocultured
with colon carcinoma cells. Oncol Rep. 39:1387–1395.
2018.PubMed/NCBI
|
|
39
|
Garcia JM, Garcia-Touza M, Hijazi RA,
Taffet G, Epner D, Mann D, Smith RG, Cunningham GR and Marcelli M:
Active ghrelin levels and active to total ghrelin ratio in
cancer-induced cachexia. J Clin Endocrinol Metab. 90:2920–2926.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kerem M, Ferahkose Z, Yilmaz UT, Pasaoglu
H, Ofluoglu E, Bedirli A, Salman B, Sahin TT and Akin M: Adipokines
and ghrelin in gastric cancer cachexia. World J Gastroenterol.
14:3633–3641. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ozola Zalite I, Zykus R, Francisco
Gonzalez M, Saygili F, Pukitis A, Gaujoux S, Charnley RM and Lyadov
V: Influence of cachexia and sarcopenia on survival in pancreatic
ductal adenocarcinoma: A systematic review. Pancreatology.
15:19–24. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Abe K, Uwagawa T, Haruki K, Takano Y, Onda
S, Sakamoto T, Gocho T and Yanaga K: Effects of ω-3 fatty acid
supplementation in patients with bile duct or pancreatic cancer
undergoing chemotherapy. Anticancer Res. 38:2369–2375.
2018.PubMed/NCBI
|