Gastric cancer (GC) is a malignant tumor type, with
wide-reaching impacts on human health. In 2016, there were ~834,000
GC-associated mortalities worldwide (1). GC is the sixth most common type of
cancer worldwide in terms of incidence, with the second highest
mortality rate among all types of cancer worldwide (1). In China, it has been estimated that
there were 67,910 new cases of GC and 49,800 GC-associated
mortalities in 2015 (2); therefore,
GC is one of the most common types of cancer ranking second
following lung cancer in terms of morbidity and mortality, and the
5-year survival rate of GC is only 28% (2). As the majority of patients with GC are
primarily diagnosed at the advanced stages of disease, the
potential for successful treatment is limited to a few patients
where early detection and comprehensive treatment were achieved
(3,4). Even with use of combination
chemotherapy, consisting of platinum and 5-fluorouracil (5-FU),
only a modest survival advantage is obtained for patients with
advanced GC (5–8). Therefore, the identification of novel
therapeutics for the treatment of advanced GC represents an
important area of investigation.
Immunotherapy is the treatment of disease by
inducing, enhancing or suppressing an immune response (9). Immunomodulatory regimens often have
fewer adverse side effects compared with the presently used drugs
and include less potential for creating resistance when treating
microbial diseases (10). Two types
of cancer immunotherapies exist: Active and passive (11). Active immunotherapies utilize
components of the patient's own immune system, in order to boost an
immune response against tumors (11). Examples of active immunotherapies
include chimeric antigen receptor (CAR)-T cell therapy and cancer
vaccines (11). Passive
immunotherapies utilize components of the immune system
manufactured outside of the body, including monoclonal antibodies
(11). Over the past 10 years,
cancer immunotherapy has demonstrated to be surprisingly effective
in the treatment of melanoma and has subsequently been applied to
breast, prostate, kidney and lung cancer (12). Therefore, immunotherapy was
designated as the breakthrough treatment of the year in 2013
(12).
The potential use of immunotherapy in GC has
received a considerable amount of interest. The molecular features
of GC have been analyzed by the Cancer Genome Atlas Research
Network and four classes of tumor subtypes have been identified,
including Epstein-Barr (EB) virus-positive tumors, microsatellite
instability tumors, genomically stable tumors and tumors with
chromosomal instability (13). In
the EB virus subgroup, which accounts for 15% of GC tumors, the
expression of programmed death-ligand-1 (PD-L1) is increased
(13), which is indicative of the
presence of stable immune cells and supports the use of an immune
checkpoint inhibitor for the treatment of this GC subtype (13).
In the present review, three principal types of
cancer immunotherapies for GC were evaluated, including immune
checkpoint inhibitors, adoptive cell therapy, including CAR-T
cells, and tumor vaccines.
In tumor immunity, the immune system recognizes and
eliminates tumor cells in order to inhibit tumor development
(14). However, tumors can escape
recognition and destruction by the immune system, thereby achieving
a malignant reproduction regime (15). As the primary participant in the
tumor immune response, the regulation of T lymphocyte activity can
exert coordinated effects upon stimulatory and inhibitory
molecules, with these inhibitory molecules serving as an immune
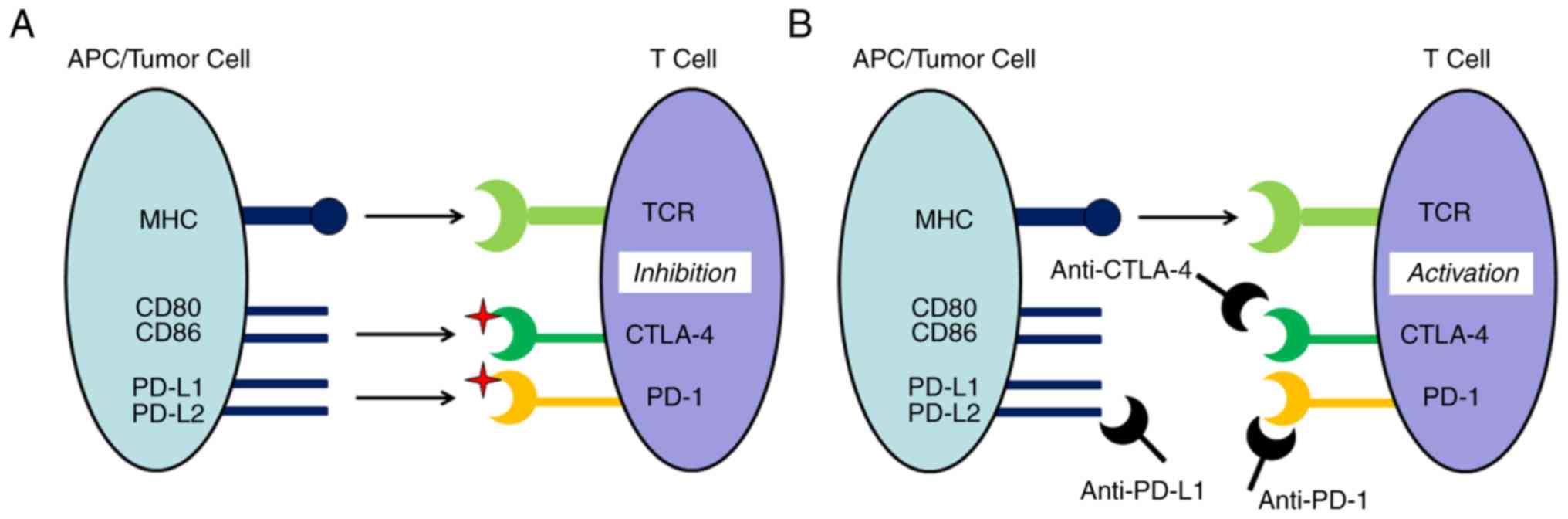
checkpoint (16). The capacity for
malignant tumors to escape immune surveillance involves the
suppression of T cell activity and can occur through immune
checkpoint pathways (Fig. 1A)
(17,18). As shown in Fig. 1A, the activity of T cells is
inhibited by cytotoxic T lymphocyte-associated antigen-4 (CTLA-4)
and programmed death 1 (PD-1)/PD-L1. Checkpoint inhibitor signaling
pathways contribute to the anti-tumor effects of T cells, which
achieve their goal of destroying tumor cells by inhibiting the
capacity for tumor immune escape. As shown in Fig. 1B, checkpoint inhibitors combine with
CTLA-4, PD-1 and PD-L1 to activate the immune response. Immune
checkpoint inhibitors have previously been demonstrated to be
effective in the treatment of a variety of malignant tumor types.
As a result, utilization of immune intervention checkpoint
signaling pathways has become a novel cancer treatment strategy
(19,20). In the past decade, three main types
of checkpoint inhibitor immunotherapy drugs have been developed for
use in preclinical and clinical studies. These drugs target CTLA-4,
PD-1 or PD-L1 (21).
Ipilimumab is a monoclonal antibody that targets
CTLA-4, which was approved by the USA Food and Drug Administration
(FDA) for the treatment of advanced melanoma in 2011 (22). However, Ipilimumab has also been used
in the treatment of numerous other types of cancer, including
small-cell lung cancer (23). In a
stage II clinical trial (NCT01585987) comparing Ipilimumab with
that of standard care as administered immediately following first
line chemotherapy in 114 patients with locally advanced
(unresectable) or metastatic gastric and gastroesophageal junction
cancer, no beneficial effects of Ipilimumab were observed (Table I) (24).
Tremelimumab is a monoclonal antibody that targets
CTLA-4, which was approved as an orphan drug treatment for
malignant mesothelioma on April 15, 2015 (25). The remission rate was 5% for 18
patients with gastric/gastroesophageal junction adenocarcinoma
included in a phase II clinical trial (26); a rate that was below the second-line
chemotherapy curative effect of cytotoxic drugs. Although the test
of tremelimumab failed to achieve a pre-set remission rate in the
final analysis, 4 patients achieved a stable condition and there
was one case of partial relief, thereby demonstrating a continuing
curative effect in remission, and such findings are promising with
regard to the treatment of advanced GC.
Pembrolizumab, an IgG4 antibody, was the first
monoclonal antibody to be developed that targets PD-1 (27). Pembrolizumab was approved by the USA
FDA for the treatment of advanced non-small cell lung cancer in
2017 (28). The safety, tolerability
and anti-tumor activity of pembrolizumab (also referred to as
MK-3475) were assessed in patients with advanced triple negative
breast cancer (TNBC), advanced head and neck cancer, advanced
urothelial cancer and advanced GC in a phase I clinical trial
(KEYNOTE-012/NCT01848834) (29). Of
the 162 patients with advanced GC screened, 39 PD-L1+
patients were enrolled in order to evaluate pembrolizumab. The
results revealed that the overall response rate (ORR) was 33% (95%
CI, 19–50) (29), the 6-month
progression-free survival (PFS) and OS rates were 24 and 69%,
respectively. These results indicate that pembrolizumab exhibits a
manageable degree of toxicity and promising antitumor activity in
patients with advanced GC, with PD-L1 expression levels associated
with the ORR.
Due to the encouraging results of the KEYNOTE-012
trial, numerous clinical trials involving inhibitory treatment of
PD-1 for GC were initiated. The first study (30) was a phase II clinical trial of
pembrolizumab as monotherapy and in combination with cisplatin +
5-FU in subjects with recurrent or metastatic gastric or
gastroesophageal junction (G/GEJ) adenocarcinoma
(KEYNOTE-059/NCT02335411) (31).
Based on this research, pembrolizumab was approved as a third-line
therapy for recurrent or metastatic G/GEJ cancer by the FDA in
September 2017. In addition, there has been a phase III,
randomized, open-label clinical trial (32) of pembrolizumab compared with
paclitaxel in subjects with advanced gastric or gastroesophageal
junction adenocarcinoma that progressed following first-line
therapy with platinum and fluoropyrimidine (KEYNOTE-061) (33). Finally, a randomized,
active-controlled, partially blinded, biomarker select, phase III
clinical trial of pembrolizumab + cisplatin + 5-FU as a first-line
treatment in subjects with advanced G/GEJ adenocarcinoma is ongoing
(KEYNOTE-062) (34).
Currently in progress is a study involving a phase I
dose escalation trial (NCT02268825) to assess the mean tolerated
dose (MTD) of MK-3475 (pembrolizumab) in combination with mFOLFOX6,
followed by a phase II expansion open label, nonrandomized trial
with MK-3475 at the MTD in combination with mFOLFOX6 and
supplemental celecoxib in patients with advanced gastrointestinal
cancer. In this study, 128 cases of late-stage colorectal, stomach,
esophagus, pancreas and biliary tract cancer are being assessed,
which will be completed in 2020.
In 2014, the FDA approved nivolumab, sold under the
name Opdivo, which is a monoclonal antibody that targets PD-1 and
is used for the treatment of advanced melanoma and lung squamous
carcinoma (35). In 59 patients with
advanced GC, nivolumab monotherapy was tested in the clinical trial
Checkmate-032 (NCT02267343); the ORR was 17%, and the 6-month PFS
and OS rates were 18 and 49%, respectively (36).
A study with 480 patients is in progress for a phase
III trial (NCT02267343) to evaluate the efficacy and safety of
ONO-4538 (nivolumab) in the standard treatment failure of
unresectable advanced or recurrent GC, including esophagogastric
junction cancer, which are refractory to or intolerant of standard
therapy. Preliminary results revealed an improvement in survival
with nivolumab treatment in advanced G/GEJ adenocarcinoma compared
with placebo treatment (37).
In September 2017, based on a phase III study
(ATTRACTION-02) of nivolumab in treating advanced gastric or
gastroesophageal junction cancer in the Asian population in Japan,
nivolumab was approved as a third-line treatment for unresectable
or advanced G/GEJ (Table I)
(38). This is the first time that a
PD-1 monoclonal antibody has been approved for third-line treatment
of advanced GC.
In addition, a phase I/II clinical trial
(NCT01928394) is currently in progress to investigate the safety
and efficacy of nivolumab as a single agent and in combination with
ipilimumab in advanced solid tumors (39). The original project was designed to
include six tumor types, including TNBC, GC, pancreatic
adenocarcinoma, small cell lung cancer, bladder cancer and ovarian
cancer; however, as of January 2017 only patients with bladder and
pancreatic cancer have been recruited (Table I).
To the best of our knowledge, three checkpoint
inhibitor immunotherapy drugs against PD-L1 have been developed,
including MDX-11-5, MEDI4736 and Avelumab. MDX-1105 (also known as
BMS-936559) is a human monoclonal IgG4 antibody (40), and in a multicenter phase I trial
(NCT00729664) (41), a total of 207
patients, including seven with GC, were treated with this
anti-PD-L1 antibody. MDX-11-5 mediated the blockade of PD-L1,
induced a durable tumor regression and prolonged stabilization of
the disease; however, this was only observed in patients with
non-small-cell lung cancer, melanoma or renal cell cancer. MDX-1105
was demonstrated to be relatively safe with regard to its use in
the treatment of advanced GC (19).
As an engineered human monoclonal antibody targeting
PD-L1, the safety and efficacy of avelumab were evaluated in a
phase I, open-label, dose-escalation clinical trial (NCT01772004),
which started in 2013 and was conducted in 1,758 cases with solid
tumors, including 150 cases of stomach/stomach esophagus carcinoma
(45). An additional phase I,
open-label, dose-escalation clinical trial (NCT01943461) of
avelumab is currently underway in Japanese patients with metastatic
or locally advanced solid tumors, with plans to expand the study
with the inclusion of Asian patients with GC, and the trial is
expected to be completed by the end of June 2019 (46).
Tumor cells exert an inhibitory effect upon the
immune system, which restricts the induction and activation of the
patient's autoimmune response (47).
As an approach to mitigate this eventuality, immune lymphocytes are
usually removed from the patient and trained to activate specific
immune cells capable of recognizing cancer cells in vitro
(48). Following amplification,
these engineered cells can be re-infused into the patient to
produce a rapid enhancement of the patient's immune function and
destroy the tumor cells (49).
Immune cells used in such training are primarily derived from
lymphokine-activate killer cells, natural killer cells, cytotoxic T
cells and tumor infiltrating lymphocytes (TILs), and this
immunotherapy is referred to as adoptive cell therapy. Adoptive
cell therapy is considered an active immunotherapy (11). CAR-T cell therapy is one of the most
effective means for the treatment of malignant tumors (49,50).
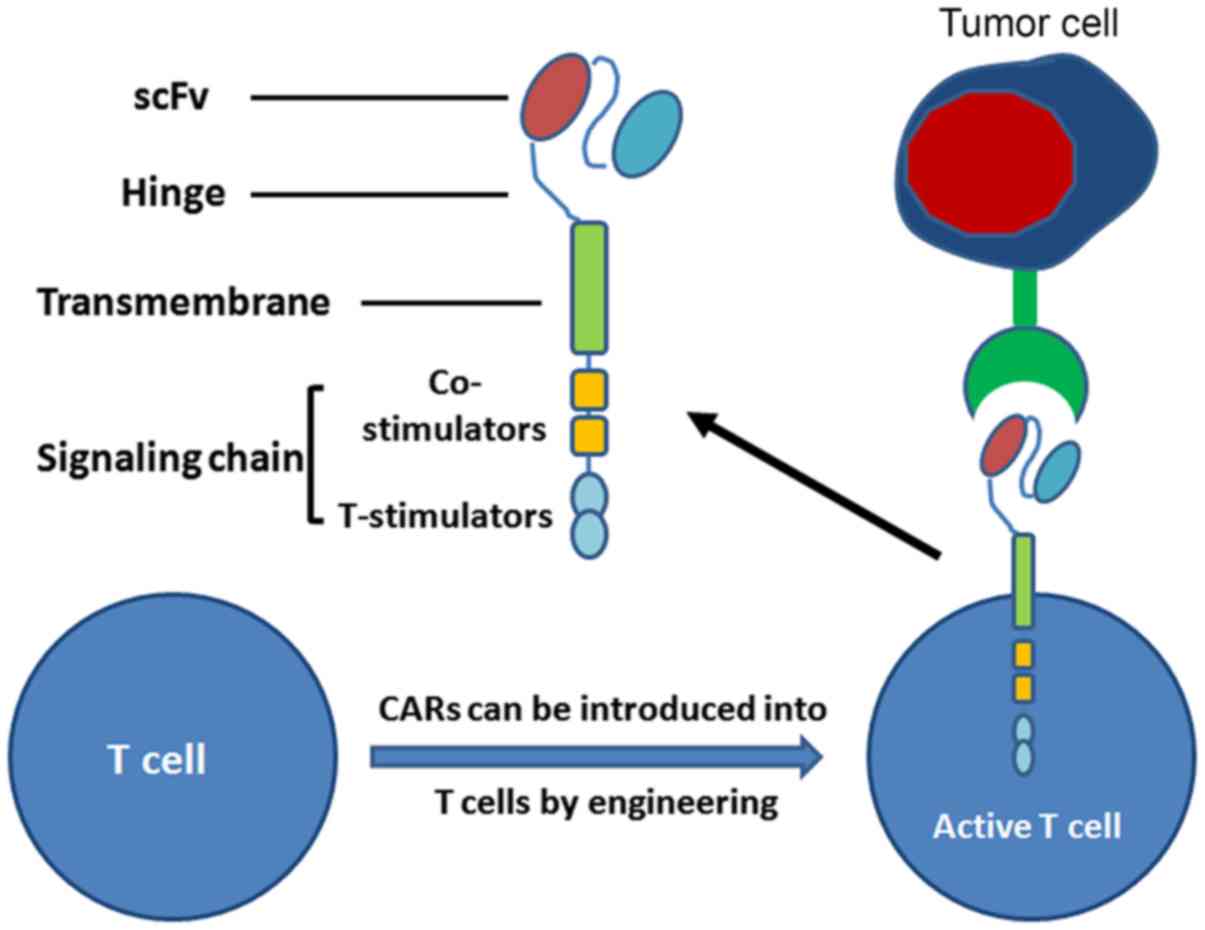
The core of CAR-T cells is the CAR, which includes
three domains: i) The single chain fragment variable (scFv, binding
tumor-associated antigen); iii) the extracellular hinge and
transmembrane domain; and iii) the intracellular signaling domain
(51). CARs can be introduced into T
cells with high efficiency using viral vectors, and provide a means
for recognition of cell surface components not restricted to major
histocompatibility complexes (48).
Therefore, T cells with CARs have the capacity to identify a
broader range of cell surface components compared with the TCRs of
natural T cells (Fig. 2). CAR-T
technology represents a promising novel approach for the treatment
of cancer. In July 2017, the CAR-T therapy CTL019, for use against
relapsed/refractory acute lymphoblastic leukemia, was granted
breakthrough therapy designation by the USA FDA (52). Currently, numerous biopharmaceutical
companies are developing CAR-T technology for cancer therapy
(53,54).
CAR-T cell therapies have demonstrated efficacy
against hematological malignancies, as demonstrated in a number of
clinical trials (Table I). Recent
studies have extended the application of CAR-T cell therapies for
the treatment of solid tumors (55–59).
Over the past decade, research has been directed at examining the
efficacy of CAR-T therapy for use in gastrointestinal tumors, and
antigens, including human epidermal growth factor receptor 2
(HER2), carcinoembryonic antigen (CEA), mucin 1 (MUC1) and
epithelial cell adhesion molecule (EpCAM), have been used as
targets in CAR-T therapy for GC (Table
I).
HER2 is a proto-oncogene, which serves an important
role in the pathogenesis and clinical development of gastric and
gastroesophageal cancer (60–63).
Investigators have developed anti-HER2 CAR-modified T cells and
validated their efficiency in targeting HER2-positive cancers in
preclinical studies (64). In order
to establish the efficacy and adverse effects, and evaluate CAR-T
cells persistence, tumor elimination and disease status following
treatment, clinical studies (65–67) have
been conducted with GC (Table
I).
CEA is generally expressed in GC, and CEA-specific
CAR-T cells can contribute to the delay of tumor growth and an
extension in the survival of mice with GC (68). The primary purpose of the clinical
trial NCT02349724 was to verify the safety of CEA-targeted CAR-T
cells and to identify the proper dosage of CAR-T cells that should
be infused (69).
MUC1 and EpCAM are transmembrane glycoproteins that
are highly expressed in various types of cancer, including advanced
prostate cancer, lung cancer and nasopharyngeal carcinoma (70–74).
MUC1-specific CAR-T cells have previously been demonstrated to be
effective in attacking MUC1-positive tumor cells (75); however, the altered expressions of
EpCAM are associated with an aggressive biological response in GC
(76). EpCAM-targeted CAR-T cells
for stomach cancer will be evaluated in the phase I/II trials
NCT02617134 and NCT02725125 starting in 2015 and estimated to be
completed in November 2019, to assess the safety and efficacy of
anti-MUC1 CAR-T cells for MUC1-positive relapsed or refractory
solid tumors (77,78).
A tumor antigen vaccine is a vaccine generated from
cancer cells, portions of cancer cells or pure tumor antigens,
which are isolated from tumor cells. A tumor antigen vaccine may
stimulate the body's immune system to locate and destroy cancer
cells (79). Sipuleucel-T (developed
by Dendreon Corporation) was the first FDA-approved tumor vaccine,
approved in April 2010 for the treatment of asymptomatic or mild
metastatic castration treatment of prostate cancer (80). Tumor vaccines mainly include
whole-cell tumor vaccines, gene-modified tumor vaccines, dendritic
cell vaccines, peptide vaccines and DNA vaccines (81). At present, thousands of tumor
antigens that have been examined to evaluate their efficacy as
antitumor agents and the antitumor activity of tumor peptide
vaccines, such as G17DT, vascular endothelial growth factor
receptor (VEGFR) and OTSGC-A24, have also been utilized in previous
studies investigating GC (82–84).
G17DT is a vaccine that neutralizes gastrin-17,
which is a hormone required for the growth of a number of cancer
types of the gastrointestinal tract. G17DT has previously been
demonstrated to be well tolerated and effective in the treatment of
patients with advanced cancer (85–87).
Previous studies (88,89) and a clinical trial (90) have been designed to investigate
antibody responses to G17DT, dose-ranges, tolerability and safety
in the treatment of patients with GC (Table I). In addition, results from a
clinical phase II/III study (NCT00042510) revealed that following
successful inoculation, G17DT induced specific and affinity
antgastrin antibody (AGA), and AGA could inhibit proliferation and
metastasis of tumors (89);
therefore, G17DT combined with cisplatin and 5-FU could contribute
to prolonging the median time-to-progression and median survival
time for patients with unresectable adenocarcinoma of the stomach
or gastroesophageal junction, compared with those without an
anti-G17DT immune response (89). A
report from the FDA, which designated G17DT as a fast track product
on February 21, 2003, suggested that this agent may provide a way
to improve the overall survival of stage IV GC when used in
combination with cisplatin and 5-FU (91).
To improve the survival of patients with advanced
GC, the safety and optimal dosing schedule of a cancer vaccine
cocktail was evaluated in a phase I/II study (NCT01227772) with
OTSGC-A24 targeting novel specific tumor antigens, including
forkhead box M1, DEP domain containing 1, kinesin family member
20A, URLC10 and VEGFR1 (97).
Due to the notable success of immunotherapy in the
treatment of different tumor types, including melanoma and lung
squamous carcinoma (98,99), the investigation of the therapeutic
value of immunotherapy has expanded rapidly for application to
other cancer types, including GS. However, the overall
immunogenicity of gastric carcinoma is relatively weak and the
immune treatment efficiency is quite limited in GC (13). Therefore, treatment with an immune
checkpoint inhibitor is applicable for only a restrictive group of
these patients, such as those with a gastric tumor subtype positive
for the EB virus (100,101).
After having established the effectiveness and
safety of GC immunotherapy, the next critical issue to address
involves selection of the best mode of treatment (102,103).
The investigation of targeted immune checkpoints has changed from
that of single drug treatment to that involving a combination
therapy, and this approach of applying immunotherapy in combination
with chemotherapy has been adopted in numerous clinical settings
(104). The majority of findings
from studies on GC have demonstrated that, compared with
chemotherapy alone, the combination of immunotherapy and
chemotherapy improves the efficacy of treatment with varying
degrees of success (105,106). Nonetheless, due to the side effects
associated with chemotherapy, the optimal protocol for combining
chemotherapy with immunotherapy requires further investigation.
Immunotherapy was once considered to have little
effect in common epithelial cancers with lower mutation rates
(107,108); however, a recent study demonstrated
that adoptive transfer of autologous lymphocytes can produce
widespread lytic activity against cancer cells (109). Zacharakis et al (110) reported a patient with breast cancer
with adoptive transfer of four mutant-protein-specific TILs in
conjunction with interleukin-2 and checkpoint blockade, which
mediated the complete durable regression of metastatic breast
cancer. The new immunotherapy approach is also expected to be used
for the treatment of GC.
Not applicable.
This work was supported by the Key Discipline
Construction of Shanxi Normal University (grant no. 0505/02100030)
and the Shanxi Provincial University of Science and Technology
Innovation Project (grant no. 20161107).
All data generated or analyzed during this study are
included in this published article.
LY collected and analysed the data, and was a major
contributor in writing the original draft of the manuscript. YW
collected and analysed data. HW reviewed and edited the
manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Global Burden of Disease Cancer
Collaboration, ; Fitzmaurice C, Akinyemiju TF, Al Lami FH, Alam T,
Alizadeh-Navaei R, Allen C, Alsharif U, Alvis-Guzman N, Amini E, et
al: Global, regional, and national cancer incidence, mortality,
years of life lost, years lived with disability, and
disability-adjusted life-years for 29 cancer groups, 1990 to 2016:
A systematic analysis for the global burden of disease study. JAMA
Oncol. 4:1553–1568. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Takeuchi C, Yamamichi N, Shimamoto T,
Takahashi Y, Mitsushima T and Koike K: Gastric polyps diagnosed by
double-contrast upper gastrointestinal barium X-ray radiography
mostly arise from the Helicobacter pylori-negative stomach with low
risk of gastric cancer in Japan. Gastric Cancer. 20:314–321. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yu G, Torres J, Hu N, Medrano-Guzman R,
Herrera-Goepfert R, Humphrys MS, Wang L, Wang C, Ding T, Ravel J,
et al: Molecular characterization of the human stomach microbiota
in gastric cancer patients. Front Cell Infect Microbiol. 7:3022017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fuchs CS, Tomasek J, Yong CJ, Dumitru F,
Passalacqua R, Goswami C, Safran H, Dos Santos LV, Aprile G, Ferry
DR, et al: Ramucirumab monotherapy for previously treated advanced
gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An
international, randomised, multicentre, placebo-controlled, phase 3
trial. Lancet. 383:31–39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shen L, Xu JM, Feng FY, Jiao SC, Wang LW,
Li J, Guan ZZ, Qin SK, Wang JJ, Yu SY, et al: Trastuzumab in
combination with chemotherapy versus chemotherapy alone for
first-line treatment of HER2-positive advanced gastric or
gastroesophageal junction cancer: A Phase III, multi-center,
randomized controlled trial, Chinese subreport. Zhonghua Zhong Liu
Za Zhi. 35:295–300. 2013.(In Chinese). PubMed/NCBI
|
|
7
|
Galdy S, Cella CA, Spada F, Murgioni S,
Frezza AM, Ravenda SP, Zampino MG and Fazio N: Systemic therapy
beyond first-line in advanced gastric cancer: An overview of the
main randomized clinical trials. Crit Rev Oncol Hematol. 99:1–12.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bang YJ, Van CE, Feyereislova A, Chung HC,
Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T, et al:
Trastuzumab in combination with chemotherapy versus chemotherapy
alone for treatment of HER2-positive advanced gastric or
gastro-oesophageal junction cancer (ToGA): A phase 3, open-label,
randomised controlled trial. Lancet. 376:687–697. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mellman I: Immunotherapies definition.
Dictionary.com. Retrieved 2009-06-02. Nature. 480:480–489. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Masihi KN: Fighting infection using
immunomodulatory agents. Expert Opin Biol Ther. 1:641–653. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Copp J, Xie WD, Zhang C and Berglin J:
Immunotherapy and cell therapy for cancer. CJPT. 30:87–94.
2016.
|
|
12
|
Couzin-Frankel J: Breakthrough of the year
2013. Cancer immunotherapy. Science. 342:1432–1433. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular characterization of gastric adenocarcinoma.
Nature. 513:202–209. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Keir ME, Butte MJ, Freeman GJ and Sharpe
AH: PD-1 and its ligands in tolerance and immunity. Annu Rev
Immunol. 26:677–704. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Douglas H and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Walker LS: Treg and CTLA-4: Two
intertwining pathways to immune tolerance. J Autoimmun. 45:49–57.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dolan DE and Gupta S: PD-1 pathway
inhibitors: Changing the landscape of cancer immunotherapy. Cancer
Control. 21:231–237. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity, and immune
correlates of anti-PD-1 antibody in cancer. N Engl J Med.
366:2443–2454. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hodi FS, O'Day SJ, McDermott DF, Weber RW,
Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel
JC, et al: Improved survival with ipilimumab in patients with
metastatic melanoma. N Engl J Med. 363:711–723. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jacob JA: Cancer immunotherapy researchers
focus on refining checkpoint blockade therapies. JAMA.
314:2117–2119. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ipilimumab, . https://www.accessdata.fda.gov/scripts/opdlisting/oopd/listResult.cfm
|
|
23
|
Hellmann MD, Ott PA, Zugazagoitia J, Ready
NE, Hann CL, De Braud FG, Antonia SJ, Ascierto PA, Moreno V, Atmaca
A, et al: Nivolumab (nivo) ± ipilimumab (ipi) in advanced
small-cell lung cancer (SCLC): First report of a randomized
expansion cohort from CheckMate 032. J Clin Oncol. 35:85032017.
View Article : Google Scholar
|
|
24
|
ClinicalTrials.gov, . An efficacy study in
gastric and gastroesophageal junction cancer comparing ipilimumab
versus standard of care immediately following first line
chemotherapy. https://clinicaltrials.gov/ct2/show/NCT01585987
|
|
25
|
Tremelimumab, . https://www.accessdata.fda.gov/scripts/opdlisting/oopd/listResult.cfm
|
|
26
|
Ralph C, Elkord E, Burt DJ, O'Dwyer JF,
Austin EB, Stern PL, Hawkins RE and Thistlethwaite FC: Modulation
of lymphocyte regulation for cancer therapy: A phase II trial of
tremelimumab in advanced gastric and esophageal adenocarcinoma.
Clin Cancer Res. 16:1662–1672. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Scapin G, Yang X, Prosise WW, McCoy M,
Reichert P, Johnston JM, Kashi RS and Strickland C: Structure of
full-length human anti-PD1 therapeutic IgG4 antibody pembrolizumab.
Nat Struct Mol Biol. 22:953–958. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Garon EB, Rizvi NA, Hui R, Leighl N,
Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L,
et al: Pembrolizumab for the treatment of non-small-cell lung
cancer. N Engl J Med. 372:2018–2028. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Muro K, Chung HC, Shankaran V, Geva R,
Catenacci D, Gupta S, Eder JP, Golan T, Le DT, Burtness B, et al:
Pembrolizumab for patients with PD-L1-positive advanced gastric
cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial.
Lancet Oncol. 17:717–726. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bang YJ, Kang YK, Catenacci DV, Muro K,
Fuchs CS, Geva R, Hara H, Golan T, Garrido M, Jalal SI, et al:
Pembrolizumab alone or in combination with chemotherapy as
first-line therapy for patients with advanced gastric or
gastroesophageal junction adenocarcinoma: Results from the phase II
nonrandomized KEYNOTE-059 study. Gastric Cancer. 22:828–837. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
ClinicalTrials.gov, . A study of
pembrolizumab (MK-3475) in participants with recurrent or
metastatic gastric or gastroesophageal junction adenocarcinoma
(MK-3475-059/KEYNOTE-059). https://clinicaltrials.gov/ct2/show/NCT02335411
|
|
32
|
Shitara K, Özgüroğlu M, Bang YJ, Di
Bartolomeo M, Mandalà M, Ryu MH, Fornaro L, Olesiński T, Caglevic
C, Chung HC, et al: Pembrolizumab versus paclitaxel for previously
treated, advanced gastric or gastro-oesophageal junction cancer
(KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial.
Lancet. 392:123–133. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
ClinicalTrials.gov, . A study of
pembrolizumab (MK-3475) versus paclitaxel for participants with
advanced gastric/gastroesophageal junction adenocarcinoma that
progressed after therapy with platinum and fluoropyrimidine
(MK-3475-061/KEYNOTE-061). https://clinicaltrials.gov/ct2/show/NCT02370498
|
|
34
|
ClinicalTrials.gov, . Study of
pembrolizumab (MK-3475) as first-line monotherapy and combination
therapy for treatment of advanced gastric or gastroesophageal
junction adenocarcinoma (MK-3475-062/KEYNOTE-062). https://clinicaltrials.gov/ct2/show/NCT02494583
|
|
35
|
Nivolumab, . https://www.accessdata.fda.gov/scripts/opdlisting/oopd/listResult.cfm
|
|
36
|
Le TD, Bendell JC, Calvo E, Kim JW,
Ascierto PA, Sharma P, Ott PA, Bono P, Jeffry D, Evans TRJ, et al:
Safety and activity of nivolumab monotherapy in advanced and
metastatic (A/M) gastric or gastroesophageal junction cancer
(GC/GEC): Results from the CheckMate-032 study. J Clin Oncol.
34:2016. View Article : Google Scholar
|
|
37
|
Kang YK, Boku N, Satoh T, Ryu MH, Chao Y,
Kato K, Chung HC, Chen JS, Muro K, Kang WK, et al: Nivolumab in
patients with advanced gastric or gastro-oesophageal junction
cancer refractory to, or intolerant of, at least two previous
chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised,
double-blind, placebo-controlled, phase 3 trial. Lancet.
390:2461–2471. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Boku N, Kang YK, Satoh T, Chao Y, Kato K,
Chung HC, Chen JS, Muro K, Kang WK, Yoshikawa T, et al: 617OA Phase
3 Study of nivolumab (Nivo) in previously treated advanced gastric
or gastroesophageal junction (G/GEJ) cancer: Updated results and
subset analysis by PD-L1 expression (ATTRACTION-02). Ann Oncol.
28:2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
ClinicalTrials.gov, . A study of nivolumab
by itself or nivolumab combined with ipilimumab in patients with
advanced or metastatic solid tumors. https://clinicaltrials.gov/ct2/show/NCT01928394
|
|
40
|
Lee JY, Lee HT, Shin W, Chae J, Choi J,
Kim SH, Lim H, Won Heo T, Park KY, Lee YJ, et al: Structural basis
of checkpoint blockade by monoclonal antibodies in cancer
immunotherapy. Nat Commun. 7:133542016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ,
Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, et al:
Safety and activity of anti-PD-L1 antibody in patients with
advanced cancer. N Engl J Med. 366:2455–2465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Segal NH, Antonia SJ, Brahmer JR, Maio M,
Blake-Haskins A, Vasselli XL, Ibrahim RA, Lutzky J and Khleif S:
Preliminary data from a multi-arm expansion study of MEDI4736, an
anti-PD-L1 antibody. J Clin Oncol. 32:30022014. View Article : Google Scholar
|
|
43
|
Levy A, Massard C, Soria JC and Deutsch E:
Concurrent irradiation with the anti-programmed cell death ligand-1
immune checkpoint blocker durvalumab: Single centre subset analysis
from a phase 1/2 trial. Eur J Cancer. 68:156–162. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
A phase 1b/2 study of MEDI4736 with
tremelimumab, MEDI4736 or tremelimumab monotherapy in gastric or
GEJ adenocarcinoma. https://clinicaltrials.gov/ct2/show/NCT02340975
|
|
45
|
Chung HC, Arkenau HT, Lee J, Rha SY, Oh
DY, Wyrwicz L, Kang YK, Lee KW, Infante JR, Lee SS, et al: Avelumab
(anti-PD-L1) as first-line switch-maintenance or second-line
therapy in patients with advanced gastric or gastroesophageal
junction cancer: Phase 1b results from the JAVELIN solid tumor
trial. J Immunother Cancer. 7:302019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
ClinicalTrials.gov, . Avelumab in
metastatic or locally advanced solid tumors (JAVELIN Solid Tumor
JPN). https://clinicaltrials.gov/ct2/show/NCT01943461
|
|
47
|
Mohme M, Riethdorf S and Pantel K:
Circulating and disseminated tumour cells-mechanisms of immune
surveillance and escape. Nat Rev Clin Oncol. 14:155–167. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Stauss HJ, Morris EC and Abken H: Cancer
gene therapy with T cell receptors and chimeric antigen receptors.
Curr Opin Pharmacol. 24:113–118. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Patel JM, Dale GA, Vartabedian VF, Dey P
and Selvaraj P: Cancer CARtography: Charting out a new approach to
cancer immunotherapy. Immunotherapy. 6:675–678. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Gill S, Maus MV and Porter DL: Chimeric
antigen receptor T cell therapy: 25 years in the making. Blood Rev.
30:157–167. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Zhang Q, Zhang Z, Peng M, Fu S, Xue Z and
Zhang R: CAR-T cell therapy in gastrointestinal tumors and hepatic
carcinoma: From bench to bedside. Oncoimmunology. 5:e12515392016.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Novartis CAR-T cell therapy CTL019
receives FDA breakthrough therapy designation for treatment of
adult patients with r/r DLBCL. https://www.novartis.com/news/media-releases/novartis-car-t-cell-therapy-ctl019-receives-fda-breakthrough-therapy-designation
|
|
53
|
Lee YH and Kim CH: Evolution of chimeric
antigen receptor (CAR) T cell therapy: Current status and future
perspectives. Arch Pharm Res. Mar 4–2019.(Epub ahead of print).
View Article : Google Scholar
|
|
54
|
Brudno JN and Kochenderfer JN: Recent
advances in CAR T-cell toxicity: Mechanisms, manifestations and
management. Blood Rev. 34:45–55. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Hege KM, Bergsland EK, Fisher GA,
Nemunaitis JJ, Warren RS, McArthur JG, Lin AA, Schlom J, June CH
and Sherwin SA: Safety, tumor trafficking and immunogenicity of
chimeric antigen receptor (CAR)-T cells specific for TAG-72 in
colorectal cancer. J Immunother Cancer. 5:222017. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Lonez C, Verma B, Hendlisz A, Aftimos P,
Awada A, Van Den Neste E, Catala G, Machiels JH, Piette F, Brayer
JB, et al: Study protocol for THINK: A multinational open-label
phase I study to assess the safety and clinical activity of
multiple administrations of NKR-2 in patients with different
metastatic tumour types. BMJ Open. 7:e0170752017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Tchou J, Zhao Y, Levine BL, Zhang PJ,
Davis MM, Melenhorst JJ, Kulikovskaya I, Brennan AL, Liu X, Lacey
SF, et al: Safety and efficacy of intratumoral injections of
chimeric antigen receptor (CAR) T cells in metastatic breast
cancer. Cancer Immunol Res. 5:1152–1161. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Zhang C, Wang Z, Yang Z, Wang M, Li S, Li
Y, Zhang R, Xiong Z, Wei Z, Shen J, et al: Phase I escalating-dose
trial of CAR-T therapy targeting CEA+ metastatic colorectal
cancers. Mol Ther. 25:1248–1258. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Li J, Li W, Huang K, Zhang Y, Kupfer G and
Zhao Q: Chimeric antigen receptor T cell (CAR-T) immunotherapy for
solid tumors: Lessons learned and strategies for moving forward. J
Hematol Oncol. 11:222018. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Abrahao-Machado LF and Scapulatempo-Neto
C: HER2 testing in gastric cancer: An update. World J
Gastroenterol. 22:4619–4625. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Kurokawa Y, Matsuura N, Kimura Y, Adachi
S, Fujita J, Imamura H, Kobayashi K, Yokoyama Y, Shaker MN,
Takiguchi S, et al: Multicenter large-scale study of prognostic
impact of HER2 expression in patients with resectable gastric
cancer. Gastric Cancer. 18:691–697. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Sheffield BS, Garratt J, Kalloger SE,
Li-Chang HH, Torlakovic EE, Gilks CB and Schaeffer DF: HER2/neu
testing in gastric cancer by immunohistochemistry: Assessment of
interlaboratory variation. Arch Pathol Lab Med. 138:1495–1502.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zulfiqar M, Bhalla A, Weindel M and
Shidham VB: Molecular diagnostics in esophageal and gastric
neoplasms. Clin Lab Med. 33:867–873. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Whilding LM and Maher J: ErbB-targeted CAR
T-cell immunotherapy of cancer. Immunotherapy. 7:229–241. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
A clinical research of CAR T cells
targeting HER2 positive cancer. https://clinicaltrials.gov/ct2/show/NCT02713984
|
|
66
|
ClinicalTrials.gov, . Treatment of
chemotherapy refractory human epidermalgrowth factor
receptor-2(HER-2) positive advanced solid tumors (CART-HER-2).
https://clinicaltrials.gov/ct2/show/NCT01935843
|
|
67
|
ClinicalTrials.gov, . Her2 and TGFBeta
cytotoxic T cells in treatment of Her2 positive malignancy
(HERCREEM). https://clinicaltrials.gov/ct2/show/NCT00889954
|
|
68
|
Wang L, Ma N, Okamoto S, Amaishi Y, Sato
E, Seo N, Mineno J, Takesako K, Kato T and Shiku H: Efficient tumor
regression by adoptively transferred CEA-specific CAR-T cells
associated with symptoms of mild cytokine release syndrome.
Oncoimmunology. 5:e12112182016. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Guest RD, Kirillova N, Mowbray S, Gornall
H, Rothwell DG, Cheadle EJ, Austin E, Smith K, Watt SM, Kühlcke K,
et al: Definition and application of good manufacturing
process-compliant production of CEA-specific chimeric antigen
receptor expressing T-cells for phase I/II clinical trial. Cancer
Immunol Immunother. 63:133–145. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Chalick M, Jacobi O, Pichinuk E, Garbar C,
Bensussan A, Meeker A, Ziv R, Zehavi T, Smorodinsky NI, Hilkens J,
et al: MUC1-ARF-A novel MUC1 protein that resides in the nucleus
and is expressed by alternate reading frame translation of MUC1
mRNA. PLoS One. 11:e01650312016. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Rajabi H, Hiraki M, Tagde A, Alam M,
Bouillez A, Christensen CL, Samur M, Wong KK and Kufe D: MUC1-C
activates EZH2 expression and function in human cancer cells. Sci
Rep. 7:74812017. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Genitsch V, Zlobec I, Thalmann GN and
Fleischmann A: MUC1 is upregulated in advanced prostate cancer and
is an independent prognostic factor. Prostate Cancer Prostatic Dis.
19:242–247. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Lee HK, Kwon MJ, Seo J, Kim JW, Hong M,
Park HR, Min SK, Choe JY, Ra YJ, Jang SH, et al: Expression of
mucins (MUC1, MUC2, MUC5AC and MUC6) in ALK-positive lung cancer:
Comparison with EGFR-mutated lung cancer. Pathol Res Pract.
215:459–465. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Wang MH, Sun R, Zhou XM, Zhang MY, Lu JB,
Yang Y, Zeng LS, Yang XZ, Shi L, Xiao RW, et al: Epithelial cell
adhesion molecule overexpression regulates epithelial-mesenchymal
transition, stemness and metastasis of nasopharyngeal carcinoma
cells via the PTEN/AKT/mTOR pathway. Cell Death Dis. 9:22018.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Maher J and Wilkie S: CAR mechanics:
Driving T cells into the MUC of cancer. Cancer Res. 69:4559–4562.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Warneke VS, Behrens HM, Haag J, Krüger S,
Simon E, Mathiak M, Ebert MP and Röcken C: Members of the EpCAM
signalling pathway are expressed in gastric cancer tissue and are
correlated with patient prognosis. Br J Cancer. 109:2217–2227.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
ClinicalTrials.gov, . CAR-T cell
immunotherapy in MUC1 positive solid tumor. https://clinicaltrials.gov/ct2/show/NCT02617134
|
|
78
|
ClinicalTrials.gov, . Study evaluating the
efficacy and safety with CAR-T for stomach cancer (EECSC).
https://clinicaltrials.gov/ct2/show/NCT02725125
|
|
79
|
Ott PA, Hu Z, Keskin DB, Shukla SA, Sun J,
Bozym DJ, Zhang W, Luoma A, Giobbie-Hurder A, Peter L, et al: An
immunogenic personal neoantigen vaccine for patients with melanoma.
Nature. 547:217–221. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Cheever MA and Higano CS: PROVENGE
(Sipuleucel-T) in prostate cancer: The first FDA-approved
therapeutic cancer vaccine. Clin Cancer Res. 17:3520–3526. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Ribas A, Butterfield LH, Glaspy JA and
Economou JS: Current developments in cancer vaccines and cellular
immunotherapy. J Clin Oncol. 21:2415–2432. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Gilliam AD and Watson SA: G17DT: An
antigastrin immunogen for the treatment of gastrointestinal
malignancy. Expert Opin Biol Ther. 7:397–404. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Park DJ, Thomas NJ, Yoon C and Yoon SS:
Vascular endothelial growth factor a inhibition in gastric cancer.
Gastric Cancer. 18:33–42. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Sundar R, Rha SY, Yamaue H, Katsuda M,
Kono K, Kim HS, Kim C, Mimura K, Kua LF and Yong WP: A phase I/Ib
study of OTSGC-A24 combined peptide vaccine in advanced gastric
cancer. BMC Cancer. 18:3322018. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Watson SA, Michaeli D, Grimes S, Morris
TM, Robinson G, Varro A, Justin TA and Hardcastle JD: Gastrimmune
raises antibodies that neutralize amidated and glycine-extended
gastrin-17 and inhibit the growth of colon cancer. Cancer Res.
56:880–885. 1996.PubMed/NCBI
|
|
86
|
Smith AM, Justin T, Michaeli D and Watson
SA: Phase I/II study of G17-DT, an anti-gastrin immunogen, in
advanced colorectal cancer. Clin Cancer Res. 6:4719–4724.
2000.PubMed/NCBI
|
|
87
|
Brett BT, Smith SC, Bouvier CV, Michaeli
D, Hochhauser D, Davidson BR, Kurzawinski TR, Watkinson AF, Van
Someren N, Pounder RE and Caplin ME: Phase II study of
anti-gastrin-17 antibodies, raised to G17DT, in advanced pancreatic
cancer. J Clin Oncol. 20:4225–4231. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Gilliam AD, Watson SA, Henwood M, McKenzie
AJ, Humphreys JE, Elder J, Iftikhar SY, Welch N, Fielding J, Broome
P and Michaeli D: A phase II study of G17DT in gastric carcinoma.
Eur J Surg Oncol. 30:536–543. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Ajani JA, Hecht JR, Ho L, Baker J,
Oortgiesen M, Eduljee A and Michaeli D: An open-label,
multinational, multicenter study of G17DT vaccination combined with
cisplatin and 5-fluorouracil in patients with untreated, advanced
gastric or gastroesophageal cancer: The GC4 study. Cancer.
106:1908–1916. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Rocha-Lima CM, de Queiroz Marques Junior
E, Bayraktar S, Broome P, Weissman C, Nowacki M, Leslie M and
Susnerwala S: A multicenter phase II study of G17DT immunogen plus
irinotecan in pretreated metastatic colorectal cancer progressing
on irinotecan. Cancer Chemother Pharmacol. 74:479–486. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Gastrin 17 vaccine-Aphton, . Anti-gastrin
17 immunogen, G17DT. BioDrugs. 17:223–225. 2003.PubMed/NCBI
|
|
92
|
Zhao T, Zhao W, Chen Y, Liu L, Ahokas RA
and Sun Y: Differential expression of vascular endothelial growth
factor isoforms and receptor subtypes in the infarcted heart. Int J
Cardiol. 167:2638–2645. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Wada S, Tsunoda T, Baba T, Primus FJ,
Kuwano H, Shibuya M and Tahara H: Rationale for antiangiogenic
cancer therapy with vaccination using epitope peptides derived from
human vascular endothelial growth factor receptor 2. Cancer Res.
65:4939–4946. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Ishizaki H, Tsunoda T, Wada S, Yamauchi M,
Shibuya M and Tahara H: Inhibition of tumor growth with
antiangiogenic cancer vaccine using epitope peptides derived from
human vascular endothelial growth factor receptor 1. Clin Cancer
Res. 12:5841–5849. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Masuzawa T, Fujiwara Y, Okada K, Nakamura
A, Takiguchi S, Nakajima K, Miyata H, Yamasaki M, Kurokawa Y, Osawa
R, et al: Phase I/II study of S-1 plus cisplatin combined with
peptide vaccines for human vascular endothelial growth factor
receptor 1 and 2 in patients with advanced gastric cancer. Int J
Oncol. 41:1297–1304. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Ishikawa H, Imano M, Shiraishi O, Yasuda
A, Peng YF, Shinkai M, Yasuda T, Imamoto H and Shiozaki H: Phase I
clinical trial of vaccination with LY6K-derived peptide in patients
with advanced gastric cancer. Gastric Cancer. 17:173–180. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
ClinicalTrials.gov, . Study of OTSGC-A24
vaccine in advanced gastric cancer. https://clinicaltrials.gov/ct2/show/NCT01227772
|
|
98
|
Valpione S and Campana LG: Immunotherapy
for advanced melanoma: Future directions. Immunotherapy. 8:199–209.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Stinchcombe TE: Unmet needs in squamous
cell carcinoma of the lung: Potential role for immunotherapy. Med
Oncol. 31:9602014. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Dong M, Wang HY, Zhao XX, Chen JN, Zhang
YW, Huang Y, Xue L, Li HG, Du H, Wu XY and Shao CK: Expression and
prognostic roles of PIK3CA, JAK2, PD-L1, and PD-L2 in Epstein-Barr
virus-associated gastric carcinoma. Hum Pathol. 53:25–34. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Shinozaki-Ushiku A, Kunita A and Fukayama
M: Update on Epstein-Barr virus and gastric cancer (review). Int J
Oncol. 46:1421–1434. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Bolm L, Käsmann L, Paysen A, Karapetis C,
Rades D, Wellner UF, Keck T, Watson DI, Hummel R and Hussey DJ:
Multimodal anti-tumor approaches combined with immunotherapy to
overcome tumor resistance in esophageal and gastric cancer.
Anticancer Res. 38:3231–3242. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Lazăr DC, Avram MF, Romosan I, Cornianu M,
Tăban S and Goldis A: Prognostic significance of tumor immune
microenvironment and immunotherapy: Novel insights and future
perspectives in gastric cancer. World J Gastroenterol.
24:3583–3616. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Cui J, Li L, Wang C, Jin H, Yao C, Wang Y,
Li D, Tian H, Niu C, Wang G, et al: Combined cellular immunotherapy
and chemotherapy improves clinical outcome in patients with gastric
carcinoma. Cytotherapy. 17:979–988. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Wang Y, Wang C, Xiao H, Niu C, Wu H, Jin
H, Yao C, He H, Tian H, Han F, et al: Adjuvant treatment combining
cellular immunotherapy with chemotherapy improves the clinical
outcome of patients with stage II/III gastric cancer. Cancer Med.
6:45–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Zhandossov O, Kaussova G and Koten A:
Combined treatment for gastric cancer: Immunological approach. Turk
J Gastroenterol. 29:151–156. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Hamanishi J, Mandai M, Ikeda T, Minami M,
Kawaguchi A, Murayama T, Kanai M, Mori Y, Matsumoto S, Chikuma S,
et al: Safety and antitumor activity of anti-PD-1 antibody,
nivolumab, in patients with platinum-resistant ovarian cancer. J
Clin Oncol. 33:4015–4022. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Le DT, Durham JN, Smith KN, Wang H,
Bartlett BR, Aulakh LK, Lu S, Kemberling H, Wilt C, Luber BS, et
al: Mismatch repair deficiency predicts response of solid tumors to
PD-1 blockade. Science. 357:409–413. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Stevanović S, Pasetto A, Helman SR,
Gartner JJ, Prickett TD, Howie B, Robins HS, Robbins PF, Klebanoff
CA, Rosenberg SA and Hinrichs CS: Landscape of immunogenic tumor
antigens in successful immunotherapy of virally induced epithelial
cancer. Science. 356:200–205. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Zacharakis N, Chinnasamy H, Black M, Xu H,
Lu YC, Zheng Z, Pasetto A, Langhan M, Shelton T, Prickett T, et al:
Immune recognition of somatic mutations leading to complete durable
regression in metastatic breast cancer. Nat Med. 24:724–730. 2018.
View Article : Google Scholar : PubMed/NCBI
|