Introduction
Neuroblastoma (NB) is one of the most common
extracranial, solid, pediatric malignancies. NB originates from
neural crest cells that can be destined for anywhere in the
sympathetic nervous system (1), and
accounts for 8–10% of pediatric malignancies and 15% of pediatric
cancer-associated mortalities worldwide (2). NB is an extremely heterogeneous
disease; for low-risk or intermediate-risk NB, the prognosis is
favorable after surgical resection alone or with minimal
chemotherapy (3). However, >60%
of high-risk patients with NB die following recurrence, despite
responding well to aggressive chemotherapy at the beginning of
treatment (4). This suggests there
is a lack of effective salvage regimens for patients with
disease-recurrence.
Although the majority of patients with NB achieve
complete remission under conventional treatments, including
surgery, chemotherapy and radiotherapy, a number of patients still
relapse in the late stages of chemotherapy, with acquired
multi-drug resistance (MDR) (5). MDR
contributes heavily to minimal residual disease (MRD) after
chemotherapy, which leads to the recurrence of high-risk NB
(6). Despite a large number of
innovative studies on MRD, the prognosis of high-risk NB has
remained poor over the past decade (7–9). Due to
the issues with traditional chemotherapy drugs in NB, including
increases in genetic mutations, dysregulated activity of tumor
suppressor genes and serious side effects on organs (10–12), the
aim of the present study was to identify effective and
well-tolerated methods for treating NB.
Ganglioside GD2 is a type of glycosphingolipid
molecule that is uniformly expressed on the membrane of neurogenic
tumor cells (13). The high
expression level of GD2 in NB cells and its restricted distribution
in normal tissues indicates that anti-GD2 monoclonal antibodies may
be suitable for immunotherapy (14).
Four types of anti-GD2 monoclonal antibody have been used in
clinical trials, including murine anti-GD2 monoclonal antibody 3F8
(15), chimeric human-murine
anti-GD2 monoclonal antibody ch14.18 (16), human anti-GD2 monoclonal antibody
hu14.18 and human anti-GD2 monoclonal antibody hu3F8 (17). Simon et al (18) identified in a phase IV clinical trial
that patients who receive ch14.18 maintenance treatment after
chemotherapy acquire a higher 3-year overall survival compared with
those who receive only small doses of maintenance chemotherapy or
no maintenance therapy.
Recently, numerous studies have focused on enhancing
the treatment effects of anti-GD2 monoclonal antibody (19–21). The
mechanisms by which anti-GD2 monoclonal antibody induces apoptosis
of NB include complement-dependent cytotoxicity (CDC) and
antibody-dependent cell-mediated cytotoxicity (ADCC) (22). However, numerous studies have
suggested that the effect of CDC is associated with side effects,
such as pain in anti-GD2 monoclonal antibody treatment (23,24).
Sorkin et al (25) identified
that a mutation in anti-GD2 monoclonal antibody can reduce pain so
that the tolerance to anti-GD2 monoclonal antibody is increased
without a reduction in the killing effect of GD2 antibody. Thus, it
may be possible to improve the curative effect of anti-GD2
monoclonal antibody through enhancing ADCC.
The ADCC effect of anti-GD2 monoclonal antibody on
NB cells is associated with the Fc receptor (FcR) on killer cells,
which combines with the Fc fragment of the anti-GD2 monoclonal
antibody, activating ADCC and inducing the apoptosis of NB
(26). A number of studies have used
anti-GD2 monoclonal antibody combined with granulocyte-macrophage
colony stimulating factor (GM-CSF) or interleukin-2 (IL-2), and
have demonstrated that combination therapy exerts stronger effects
compared with using anti-GD2 monoclonal antibody alone (27–29).
This indicates that an increase in the number or activity of killer
cells is a key factor in enhancing the efficacy of anti-GD2
monoclonal antibody.
With the development of tumor immunology in recent
years, it has been reported that cytokine-induced killer
(CIK)/natural killer (NK) cells transfusion, a kind of adoptive
cellular immunotherapy, has significant effect in neuroblastosma
MRD treatment without obvious side effects (30). It recognizes and kills target tumor
cells by binding specific cell surface markers (31). NK cells are one of the most important
immune effector cell types in the process of ADCC (32). However, it has been reported
(33) that NK function is limited in
some patients with neuroblastoma; therefore, the treatment effect
of anti-GD2 monoclonal antibody is reduced in these patients
(34). CIK cells are ex
vivo-expanded T lymphocytes (35), a subset of T lymphocytes with a
natural killer T-cell phenotype expressing both the CD56 and CD3
markers presents non-histocompatibility complex cytotoxicity
against target cells, and exhibits improved anti-tumor activity
compared with NK or lymphokine-activated killer cells (36).
In our previous study (37), mononuclear cells (MNCs) from cord
blood (CBMNCs) were incubated with IL-2 and IL-7 for 21 days, and
the percentage of CD3+CD56+ CIK cells and
CD3−CD56+ NK cells reached 14.26±1.15 and
29.52±0.89%, respectively, while percentage of total CIK/NK
(CD3+/−CD56+) cells reached 43.77±1.93%,
which increased significantly compare to 9.31±1.77% before culture.
Furthermore, the percentage of CD3+CD8+ cells
was not significantly increased, indicating a risk reduction of
having graft versus host disease (GVHD) in patients. It was also
identified that FcRγIII (CD16) and lymphocyte function-associated
antigen-1 (LFA-1) are highly expressed in these cells. In
conclusion, CIK/NK cells can enhance the killing effect of tumor
cells by providing the ligands needed. The effect of CIK/NK cells
combined with anti-GD2 monoclonal antibody in targeting human NB
cells is not yet known, and further studies are required.
To examine the effects of CIK/NK cells combined with
anti-GD2 monoclonal antibody in targeting human NB cells, flow
cytometry was performed to detect the expression of GD2 and
intercellular adhesion molecule-1 (ICAM-1) on the NB cell line
SK-N-SH, and CD16 expression on CIK/NK cells. The aim of this study
was to investigate the effect of anti-GD2 monoclonal antibody and
CIK/NK cells on SK-N-SH cells. The results provide experimental
evidence supporting the use of combined treatment with CIK/NK cells
and anti-GD2 monoclonal antibody for MDR-NB, in order to improve
the prognosis and overall survival of patients.
Materials and methods
Sample collection and cell line
culture
Human cord blood samples were obtained from
full-term deliveries between January and March 2016 in the
Department of Obstetrics, Sun-Yat Sen Memorial Hospital. This study
was approved by the Ethics Committee of Sun Yat-sen Memorial
Hospital at Sun Yat-sen University (Guangzhou, China). Patients
provided informed written consent. A total of 10 patients aged
between 24 and 30 years were recruited. Exclusion criteria included
premature delivery and high-risk pregnancies. A total of 30 ml
human cord blood was collected from each patent and processed
immediately or stored in 4°C for <4 h. MNCs, a group of cells
with a one lobed nucleus containing two groups of cells,
lymphocytes and monocytes, were isolated using a Ficoll-Paque
gradient method (38). A total of 35
ml blood were added slowly into a 50 ml centrifuge tube containing
15 ml Ficoll-Paque Premium (Sigma-Aldrich; Merck KGaA), then
centrifuge at 400 × g at room temperature for 20 min. The middle
layer cells were collected and washed by phosphate buffer saline
(HyClone; GE Healthcare Life Sciences) in triplicate, and cultured
in X–VIVO medium (HyClone; GE Healthcare Life Sciences)
supplemented with 10% fetal bovine serum (HyClone; GE Healthcare
Life Sciences), 1% penicillin-streptomycin (Sigma-Aldrich; Merck
KGaA), IL-2 (80 ng/ml; Abcam) and IL-7 (40 ng/ml) at 37°C with 5%
CO2. Half of the medium was replaced and cytokines were
re-applied every 3 days. The human NB SK-N-SH cell line was
purchased from the Cell Bank of Sun-Yat Sen Medical School, and
cultured in DMEM (HyClone; GE Healthcare Life Sciences)
supplemented with 12% fetal bovine serum (HyClone; GE Healthcare
Life Sciences) and 1% penicillin-streptomycin (Sigma-Aldrich; Merck
KGaA) at 37°C with 5% CO2.
Characterization of GD2, CD54 and CD16
expression and flow cytometry analysis
Cells were harvested for experiments after 21 days
in culture. After cell harvesting, the proportion of
CD3+CD56+ (CIK) cells,
CD3−CD56+ (NK) cells and
CD3+/−CD56+ (CIK/NK) cells was detected by
flow cytometry. The proportion of CIK cells are a group of immune
effector cells characterized by the cell surface marker
CD3−CD56+ and the proportion of NK cells are
a type of lymphocytes, which are distinguished by the cell surface
marker CD3-CD56+ (39). Both CIK and
NK cells play critical role in immune anti-tumor effect (40). The ratio of CD3+CD56+ CIK, CD3-CD56+
NK or total CD3+/-CD56+ CIK/NK cells accounts for of total
mononuclear cells, which was calculated by the following formula:
Ratio of CIK cells (%)=number of cells
(CD3+CD56+)/number of cells (all MNCs); ratio
of NK cells (%)=number of cells
(CD3−CD56+)/number of cells (all MNCs); ratio
of total CIK/NK cells (%)=number of cells
(CD3+/−CD56+)/number of cells (all MNCs). The
cell surface expression of GD2 and CD54 on SK-N-SH cells and CD16
expression on CIK/NK cells was assessed by staining with 5 µl
anti-GD2-phyroerythrin (PE; cat. no. 562100) or anti-CD54-PE-Cy5
(cat. no. 555512) together with anti-45-ECD (cat. no. A07784), or
anti-CD16- fluorescein isothiocyanate (cat. no. 555406) antibodies
for 20 min at 4°C. Anti-CD45-ECD were purchased from Beckman
Coulter, Inc., and all other antibodies were purchased from BD
Biosciences. Cells were then washed by phosphate buffer saline
(HyClone; GE Healthcare Life Sciences) and analyzed using a BD
FACSVerse (BD Biosciences). Data were analyzed using FlowJo
software (FlowJo 7.6.1).
Determination of saturated
concentration of anti-GD2 on SK-N-SH cells
To determine the effects of different anti-GD2
monoclonal antibody doses on SK-N-SH cells, the cell death rate of
NB cells that had been treated with anti-GD2 monoclonal antibody
was assessed by flow cytometry. As a preliminary experiment, the
optimum treatment concentration of anti-GD2 antibody was tested.
Cells (1×105) were seeded in a 24-well plate with C-DMEM
medium and cultured for 24 h to allow the cells to adhere to the
dish, then 0.5, 1, 2, 5, 10, 20 and 50 µg/ml of anti-GD2 antibody
was added to each well. IgG1 was added as a control group. After
culture for 1 h, cells were harvested using 0.25% trypsin and
washed with phosphate-buffered saline (HyClone; GE Healthcare Life
Sciences) in triplicate, then cells were stained with GD2-PE/Cy7
antibody for 20 min in the dark and washed. The expression of GD2
on the cell surface was detected using flow cytometry.
Flow cytometry for cell viability
assay
For the determination of optimal effector/target
(E/T) ratios of CIK/NK cells over SK-N-SH cells, SK-N-SH cells were
treated with 0.25% trypsin to detach them from dishes and washed
with PBS in triplicate. Cells were labeled with 3 µM
3,3′-dioctadecyloxacarbocyanine perchlorate (DIO; Beyotime
Institute of Biotechnology) at 37°C for 30 min, then
1×105 cells were seeded in a 24-well plate. Different
E/T ratios of CIK/NK cells were added and mixed with each well of
SK-N-SH cells. The numbers of cells added were 1×105
(E/T=1:1), 2×105 (E/T=2:1), 5×105 (E/T=5:1)
and 1×106 (E/T=10:1) (24). The mixed cells were co-cultured in
37°C and 5% CO2 for 4 h. The mixed cells were then
harvested and washed with PBS in triplicate, and stained with 5 µl
propidium iodide (PI; Sigma-Aldrich; Merck KGaA) for 10 min at 4°C.
A flow cytometry assay was performed to detect the percentage of
late apoptotic and dead SK-N-SH cells (labeled as
DIO+).
For the killing effect experiments, cells were
treated with IgG only, CIK/NK cells only, anti-GD2 only or CIK/NK
combined with anti-GD2. SK-N-SH cells (1×105) in IgG
control group, CIK/NK treated group and CIK/NK + anti-GD2 treated
group were labeled with 3 µM DIO for 30 min at 37°C, while cells in
the anti-GD2 treated group were not stained with DIO. SK-N-SH cells
were mono-cultured or co-cultured with CIK/NK cells (optimal-fold
relative cell number) in the absence or presence of saturated
concentration of anti-GD2 monoclonal antibody for 4 h at 37°C.
Cells were washed with PBS in triplicate and apoptotic cells,
defined as late apoptotic and necrotic cells, were labeled with 5
µl PI for 10 min at 4°C before performance of flow cytometry assay.
Cell viability was determined using flow cytometry on a BD
FACSVerse (BD Biosciences). Data were analyzed by FlowJo software.
Each of the experiments were conducted individually, and each of
them has a specific control group, therefore the graphs were
produced differently according to their own control group.
Cell apoptotic rate in IgG treated group, CIK/NK
treated group and CIK/NK+anti-GD2 treated group were calculated
using the following equation: Apoptotic rate
(%)=DIO+PI+ (%)/DIO+ (%) ×100,
where DIO+PI+ cells were the dead SK-N-SH
cells that were previously labeled with DIO and then labeled with
PI, and DIO+ cells were all the SK-N-SH cells, including
living and late apoptotic/dead cells.
Statistical analysis
Data were processed using SPSS 20.0 software (IBM
Corp.). A Student's t-test or one-way ANOVA with Tukey's post-hoc
test was used to compare groups. P<0.05 was considered to
indicate a statistically significant difference. Data are presented
as the mean ± standard deviation. All experiments were conducted in
triplicate and repeated three times.
Results
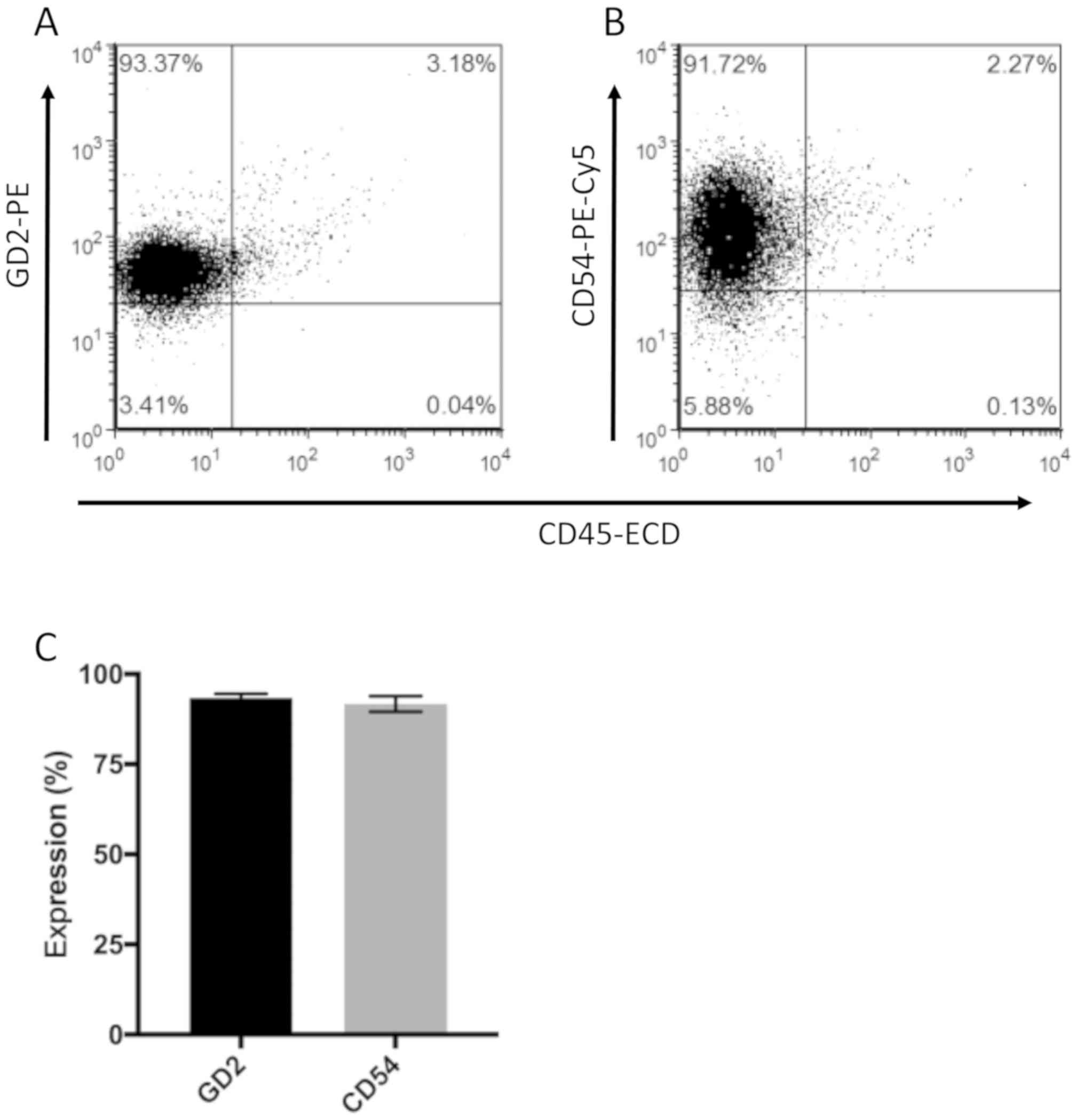
GD2 and CD54 (ICAM-1) are highly
expressed in human neuroblastoma SK-N-SH cells
To characterize the molecular basis of the effect of
anti-GD2 monoclonal antibody or CIK/NK cells on human NB SK-N-SH
cells, the cell surface expression of GD2 and CD54 (ICAM-1) was
assessed using flow cytometry analyses. The results showed that GD2
and CD54 (ICAM-1) were highly expressed in 93.37±1.2% (Fig. 1A and C) and 91.72±2.15% (Fig. 1B and C) on human neuroblastoma
SK-N-SH cells.
Anti-GD2 monoclonal antibody induces
cell death at a saturated concentration
The results indicate that following treatment with
low dose anti-GD2 antibody, (<5 µg/ml), the detection of GD2 on
the cell surface decreased from >95% (in the control group) to
~75% (5 µg/ml treatment group; P<0.001; Fig. 2A). This indicates that anti-GD2
antibody effectively combines with GD2 on the cell surface even at
concentrations of <5 µg/ml. However, at doses >5 µg/ml, there
was no statistically significant difference in GD2 detection
between groups (Fig. 2B), suggesting
that increasing the anti-GD2 antibody concentration had no effect
on SK-N-SH cells. Therefore, the concentration of 5 µg/ml was
selected for subsequent experiments. After 4 h of incubation with 5
µg/ml anti-GD2 antibody 3F8 at 37°C and 5% CO2, cells
were observed to be larger and rounded in shape compared with cells
prior to treatment (Fig. 2C). The
results indicate that anti-GD2 antibody treatment led to 8.43±1.06%
cell death compared with 0.92±0.05% in the control group
(P<0.001; Fig. 2D). This
demonstrates that treatment with anti-GD2 antibody significantly
increased apoptosis compared with the control group.
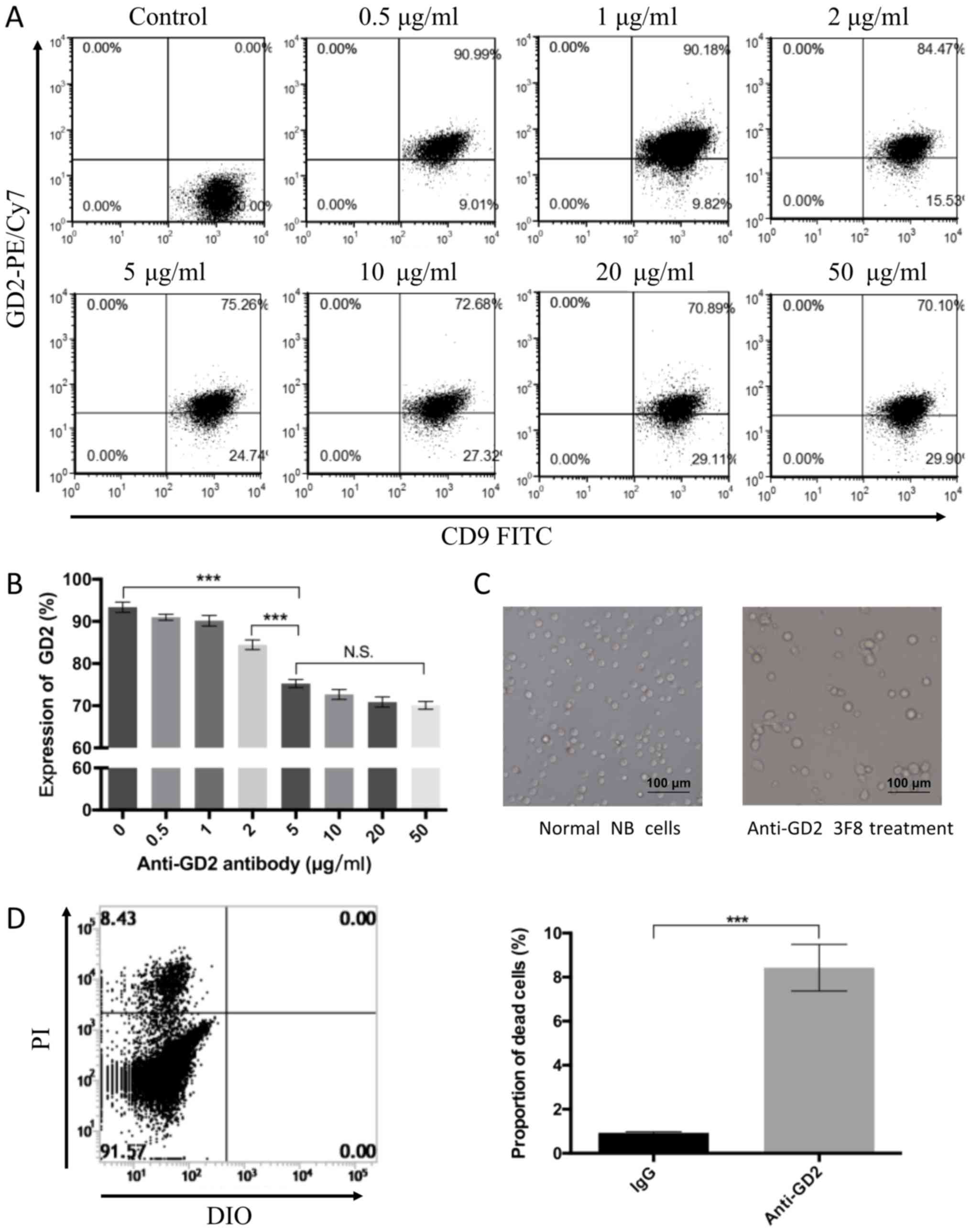 | Figure 2.Anti-GD2 monoclonal antibody induces
cell death at a saturated concentration. (A) Anti-GD2 antibody at
0.5, 1, 2, 5, 10, 20 or 50 µg/ml was added to each well after
culture for 1 h. After treatment with low dose anti-GD2 antibody,
(<5 µg/ml), the expression of GD2 on the cell surface decreased
from >95% (control group) to ~75% (5 µg/ml treatment group). (B)
There was no statistically significant difference in GD2 expression
between 5 µg/ml and >5 µg/ml treatment groups. (C) SK-N-SH cells
marked by DIO were observed to be larger and more rounded when 5
µg/ml anti-GD2 antibody 3F8 was added. (D) SK-N-SH cells were
stained with PI and analyzed by flow cytometry. Anti-GD2 antibody
led to 8.43±1.06% cell death compared with 0.92±0.05% in the
control group. ***P<0.001. Scale bar, 100 µm. PE, phyroerythrin;
N.S., not significant; DIO, 3,3′-dioctadecyloxacarbocyanine
perchlorate; PI, propidium iodide; NB, neuroblastoma; FITC,
fluorescein isothiocyanate. |
IL-2 and IL-7-cultured CIK/NK cells
partially express CD16
CBMNCs were isolated using a density gradient
centrifugation method and cultured in complete X–VIVO medium
supplemented with IL-2 and IL-7. The proportion of
CD3+CD56+ CIK cells and
CD3−CD56+ NK cells was evaluated prior to
culture, and identified to be 2.20±0.92 and 9.85±1.28%,
respectively. In total, CD3+/−CD56+ CIK/NK
cells accounted for 12.05±2.09%. After 21 days of culture, the
proportion of CD3+CD56+ CIK cells increased
to 43.60±1.98% and CD3−CD56+ NK cells
increased to 10.80±1.73%. In total,
CD3+/−CD56+ CIK/NK cells accounted for
54.40±1.56% (Fig. 3A and B). These
percentages were increased by 19.8-, 1.1- and 4.5-fold compared
with before culture, respectively. As shown in Fig. 3C, CBMNCs were single cells when
freshly isolated, and cell colonies gradually formed during 21 days
of culture. Expression of CD16 on CIK/NK cells was detected after
culture, and the results indicated that CD16 was expressed on the
cell surface of 19.01±1.27% of CIK/NK cells (Fig. 3D).
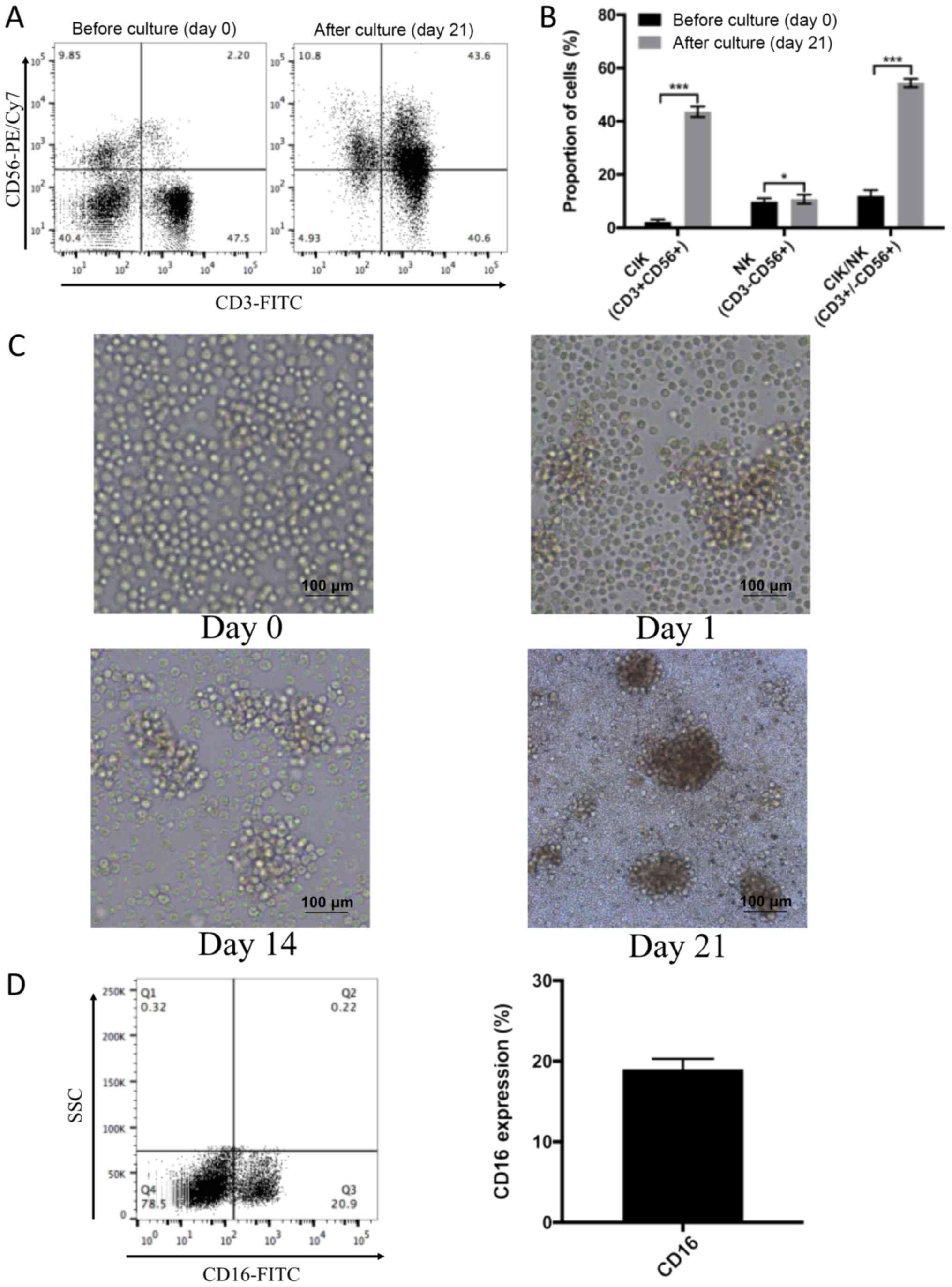 | Figure 3.IL-2 and IL-7-cultured CIK/NK cells
partially express CD16. (A) The proportion of
CD3+CD56+ CIK cells and CD3-CD56+ NK cells
was evaluated prior to culture, and (B) found to be 2.20±0.92 and
9.85±1.28%, respectively, while mixed
CD3+/−CD56+ CIK/NK cells was 12.05±2.09%.
After 21 days of culture, the proportion of
CD3+CD56+ CIK cells increased to 43.60±1.98,
CD3−CD56+ NK cells to 10.80±1.73 and mixed
CD3+/−CD56+ CIK/NK cells to 54.40±1.56%. (C)
CBMNCs were all single cells when freshly isolated, and cell
colonies gradually formed during 21 days of culture. (D) y-axis
showed SSC view, x-axis showed the CD16 was partially expressed on
CIK/NK cell surfaces, at a rate of 19.01±1.27%. Scale bar, 100 µm.
*P<0.05 and ***P<0.001 IL, interleukin; PE, phyroerythrin;
CIK, cytokine-induced killer; NK, natural killer; CBMNCs,
mononuclear cells from cord blood; SSC, side scatter. |
CIK/NK cells lead to cell death at
various E/T ratios
To determine whether CIK/NK cells could induce cell
death in human NB SK-N-SH cell line and to assess the optimal E/T
ratio, a specific killing experiment was performed and a flow
cytometry assay was used to analyze apoptotic cells. The results
showed that after 4 h of culture, CIK/NK cells had gathered around
and adhered to targeted NB SK-N-SH cells. The targeted cells had
become larger than normal and some of the cell membranes had burst
after adherence by CIK/NK cells (Fig.
4A). According to the aforementioned equation, when E/T ratio
was 1:1, the proportion of apoptotic cells was 5.94±0.25%. When E/T
ratio was increased to 2:1, 5:1 and 10:1, the proportion of
apoptotic cells was 8.33±1.46, 8.56±0.71 and 9.00±0.40%,
respectively (Fig. 4B and C).
One-way ANOVA indicated that when E/T ratio increased from 1:1 to
2:1, the apoptotic rate increased significantly. However, when the
E/T ratio was increased further, there were no significant
differences between groups (Fig.
4C). This suggested that an E/T ratio of 2:1 was optimal for
cell death, and therefore it was selected for subsequent
experiments.
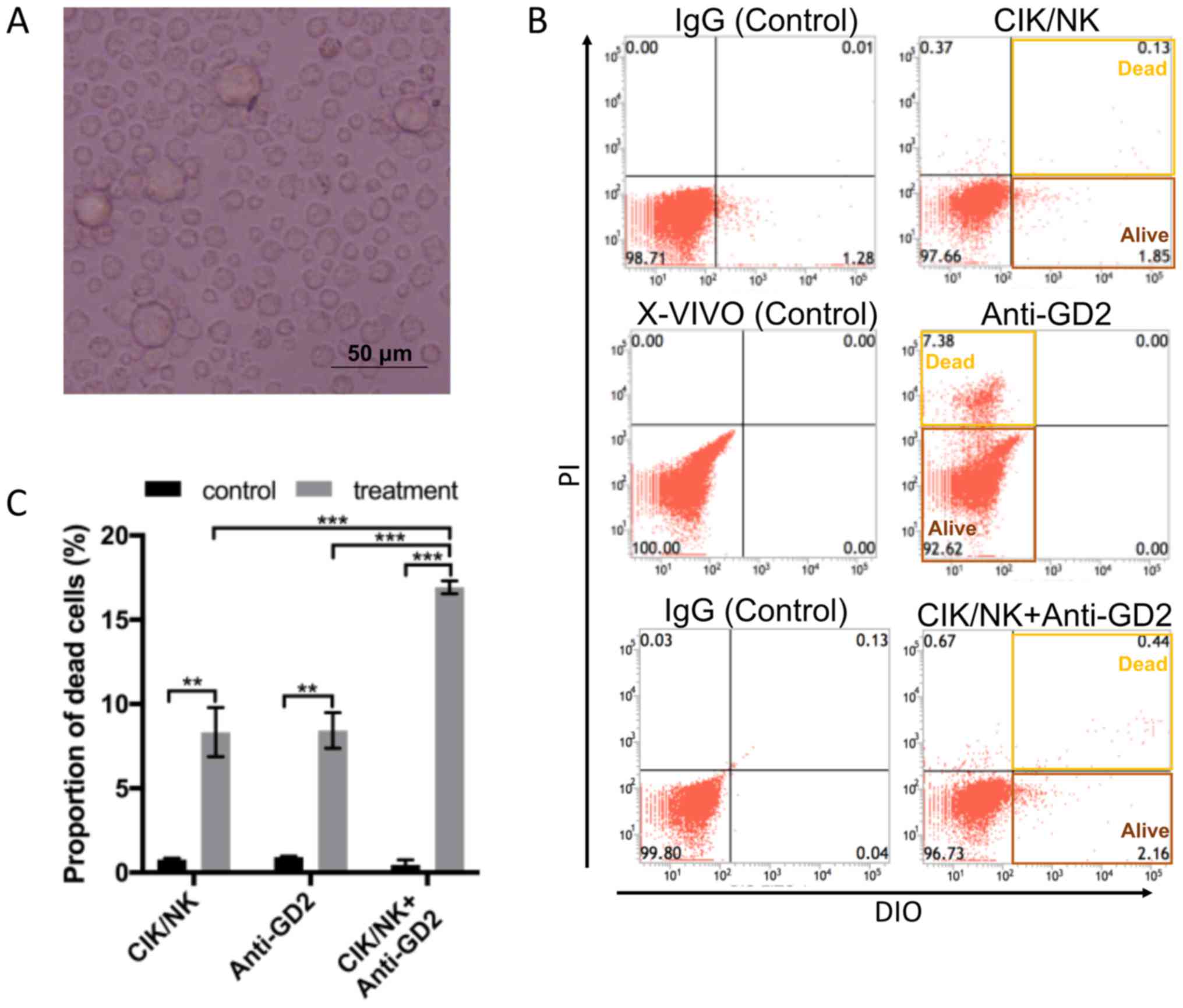
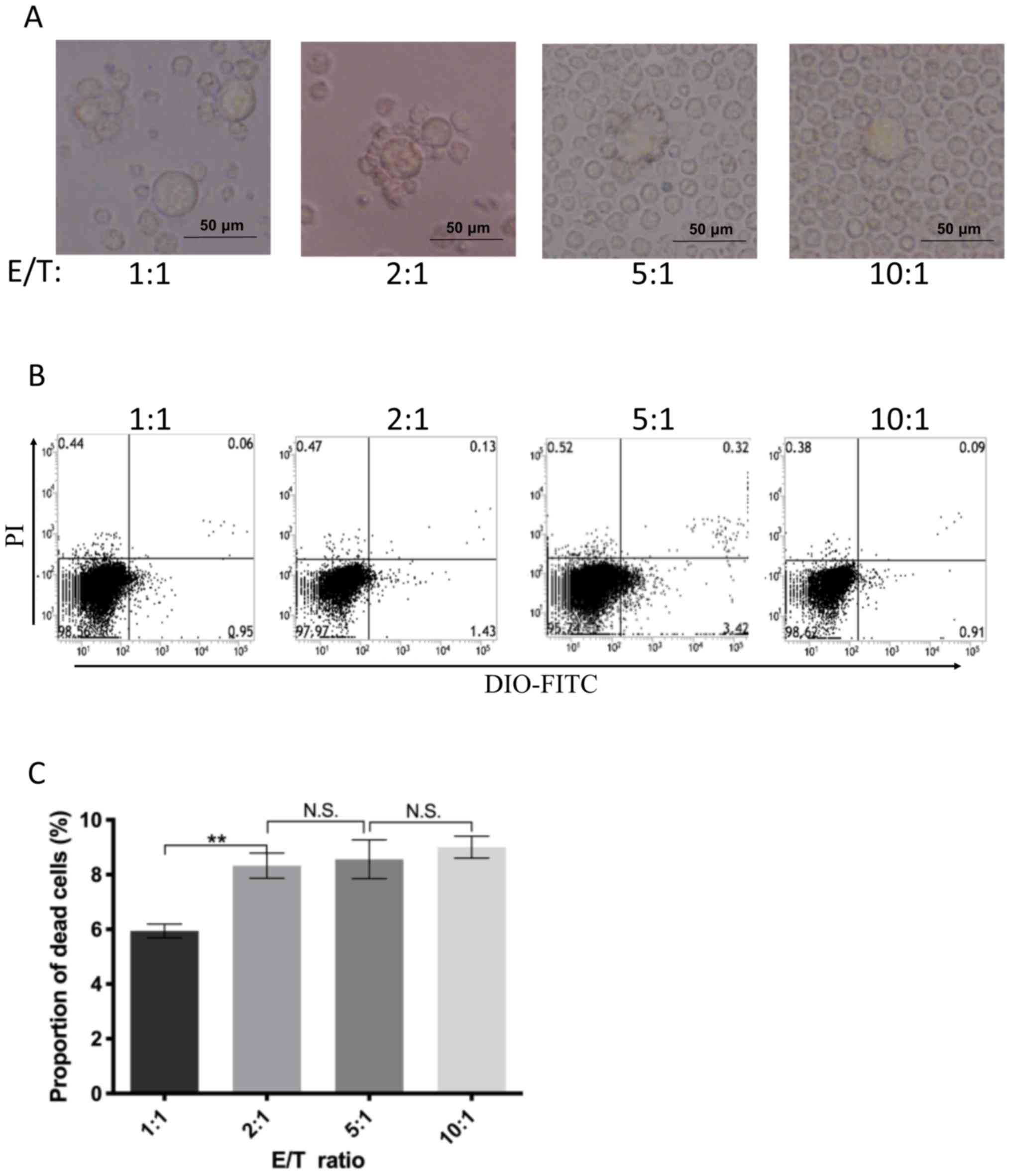 | Figure 4.CIK/NK cells lead to cell death at
various E/T ratios. (A) Various E/T ratios of CIK/NK cells were
added and mixed with each well of SK-N-SH cells and images were
obtained after 4 h of co-culture. CIK/NK cells surrounded and
adhered to targeted neuroblastoma SK-N-SH cells. Targeted cells
became larger than normal. A number of the cell membranes burst
after adherence by CIK/NK cells. (B) When the E/T ratio was 1:1,
the apoptotic rate was 5.94±0.25%, and when the E/T ratio increased
to 2:1, 5:1 and 10:1, the apoptotic cell percentages were
8.33±1.46, 8.56±0.71 and 9.00±0.40%, respectively. (C) When the E/T
ratio increased from 1:1 to 2:1, the apoptotic rate significantly
increased. However, when the E/T ratio was increased further, there
were no significant differences between groups. Scale bar, 50 µm.
**P<0.01. CIK, cytokine-induced killer; NK, natural killer; E/T,
effector/target; PI, propidium iodide; DIO,
3,3′-dioctadecyloxacarbocyanine perchlorate; N.S., not
significant. |
Anti-GD2 monoclonal antibody combined
with CIK/NK cells significantly increases apoptotic rate
To further investigate whether combining CIK/NK
cells with anti-GD2 monoclonal antibody could enhance the induction
of cell death, a combination killing experiment was performed.
After incubation with an E/T ratio 2:1 of CIK/NK cells and 5 µg/ml
anti-GD2 antibody 3F8 at 37°C and 5% CO2 for 4 h,
SK-N-SH cells were observed to be surrounded and adhered by CIK/NK
cells (Fig. 5A). All cells were
subsequently harvested and analyzed by flow cytometry. The results
showed that the combined treatment induced an apoptotic rate of
16.92±0.38%, which was significantly higher than the IgG control
group and the CIK/NK cell or anti-GD2 antibody mono-treatment
groups (P<0.001; Fig. 5B and
C).
Discussion
NB is one of the most common pediatric extracranial
solid tumors, and its occurrence and development has marked
heterogeneity (41). NB can either
differentiate from mature nerve cells or low-stage ganglion tumors
spontaneously, or metastasize early with highly malignant
characteristics (8). Among high-risk
stage IV patients with NB, >60% eventually die of relapse even
after comprehensive treatment including surgery, radiotherapy or
chemotherapy (42). The reason for
relapse in patients with stage IV NB is the presence of
chemotherapy-resistant NB cells, which induces MRD (5). Chemotherapy is the most effective
treatment for NB; however, its effectiveness is constrained by the
presence of MDR in tumor cells. Furthermore, increasing the dose of
chemotherapeutic drugs may lead to severe toxic effects in multiple
organs, including the heart, liver, kidney and ear (43). This suggests that it is necessary to
identify a more effective and tolerable treatment strategy for MDR
NB.
In recent years, immunotargeting treatment of MDR NB
has been demonstrated to significantly prolong patient survival
(44). Following treatment with
anti-GD2 monoclonal antibody combined with IL-2, GM-CSF or
cis-retinoic acid, the 5-year overall survival time of
relapsed/refractory patients with NB has improved by 20–30%
(45,46). This finding suggests that anti-GD2
monoclonal antibody has enormous potential for the treatment of
relapsed/refractory NB. Anti-GD2 monoclonal antibody has been found
to stimulate a CDC killing effect by specifically binding to tumor
cell surface GD2 or activating the ADCC effect by binding to Fc
receptors on killer cells (17–23).
However, the dosage of anti-GD2 antibody is restricted by severe
side effects, such as intolerable pain and allergy (47). This suggests that a novel strategy
based on anti-GD2 antibody is required.
CIK cells are mononuclear cells that can be isolated
from peripheral blood or cord blood. The cells are cultured with
various cytokines and are CD3+CD56+ (48). Due to the expression of CD3 and CD56
on the cell surface, CIK cells not only demonstrate anti-tumor
activity, but also have non-major histocompatibility
complex-restricted killing activity (49). The killing effect of CIK cells on
tumor cells is mainly via expression of LFA-1, which specifically
binds to ICAM-1 (CD54) on the surface of tumor cells, resulting in
the secretion of benzyloxycarbonyl-L-lysine thiobenzyl ester
esterase (granzyme A) that can penetrate the cell membrane and lead
to tumor cell death (50). However,
previous experiments have demonstrated that the efficacy of CIK/NK
cells alone for the treatment of patients with high-risk stage IV
NB is limited (51). This is due to
the large amount of complement fragments produced by anti-GD2
antibodies during the killing of NB tumor cells, which can cause
severe pain (52). Since anti-GD2 is
already in late phase of clinical trials (25), numerous evidence has reported that it
is effective for the treatment of neuroblastoma, despite of the
tolerable side effects, and it shows no harm to normal cells.
CIK/NK cell transfusion is a type of adoptive cellular
immunotherapy (35), which is
commonly used in clinical treatment. It recognizes and kills target
tumor cells by binding to specific cell surface markers based on
the immune system (17). To the best
of our knowledge, there is no evidence showing that CIK/NK cells
identify and kill normal cells. Therefore, maximizing the anti-GD2
antibody-mediated ADCC effect is a feasible research direction for
improving anti-GD2 antibody treatment for relapsed/refractory
NB.
In the present study, the cytokine combination of
IL-2 and IL-7 was used for culturing CBMNCs to obtain CIK/NK cells,
based on our previous study (37).
After 21 days, the proportion of CD3+CD56+CIK
and CD3−CD56+ NK cells was 43.60±1.98 and
10.80±1.73%, respectively, and the proportion of CIK/NK mixed cells
was 54.40±1.56%, which indicated increases of 19.8-, 1.1- and
4.5-fold, respectively. CD16 expression on the surface of CIK/NK
cells was 19.01±1.27% after culture, which was similar to the
results reported by Bonanno et al (53). Compared with the ‘classical’ CIK
amplification system (54) (IL-2,
IL-1a, IFN-γ and anti-CD3 monoclonal antibodies), not only were NK
cells effectively expanded, but also the proportion of
CD8+ cells had not been significantly increased, which
could lead to a decreased rate of GVHD (55). This suggests that the two-cytokine
culture system provides effective targeting of anti-GD2 antibodies
to NB cells and involves a simple preparation process with fewer
side effects.
The findings of the present study showed that when
various E/T ratios of CIK/NK cells were implemented, the higher the
E/T ratio, the more CIK/NK cells adhered around NB tumor cells.
After 4 h of treatment, some NB cells exhibited cell membrane
rupture and died, indicating that CIK/NK cells had anti-tumor
activity against NB cells in vitro. The killing rate
gradually increased as E/T ratio was increased, from 5.94±0.26% at
the 1:1 ratio to 9.00±0.40% at the 10:1 ratio, suggesting that an
increase in effector cells could enhance the anti-tumor effect to a
certain extent. It was also found that at E/T >2:1, the cell
apoptotic rate curve began to stabilize, suggesting that when
CIK/NK cells reached a certain threshold, they could not further
increase the apoptotic rate of NB tumor cells. Therefore, clinical
application of CIK/NK cell immunotherapy for NB tumors should use
an infusion of an appropriate number of cells, in order to achieve
maximum efficacy, while minimizing side effects, including GVHD
caused by infusion of immune cells.
For the anti-GD2 antibody experiment, it was
identified that GD2 was highly expressed on SK-N-SH cells, which
was also highly expressed on other malignancies, including bladder
cancer (56), breast cancer
(57) and some other solid tumors in
children (58). The effects of
different concentrations of anti-GD2 antibody on NB cells was
examined. The experimental results showed that when the antibody
concentration reached 5 µg/ml, there were no significant changes in
the expression rate of anti-GD2 antibody on the cell surface with
increases in concentration. This finding was similar to the results
of Esser et al (59).
Anti-GD2 antibody mediates the ADCC effect of immune cells on tumor
cells in vivo; the Fc segment of anti-GD2 antibody binds to
the FcR on the immune cell surface and stimulates the immune cell
to release perforin and granzyme that can cleave the NB cell
membrane (20). In addition, the
anti-GD2 antibody itself can also form antigen-antibody complexes
by binding to GD2 antigen on the surface of NB cells, activating
the classical complement pathway (CDC pathway) for cell death
(60). This study's results showed
that the apoptotic rate under anti-GD2 monoclonal antibody alone
was 8.43±1.06% at 5 µg/ml. However, activation of the classical
complement pathway requires the binding of two or more antibodies
to the Fc segment (61), therefore
anti-GD2 antibody killing of target cells through the CDC pathway
is not a highly effective therapeutic method, which is consistent
with our in vitro results.
However, CIK/NK cells combined with anti-GD2
antibody only increased the cell death rate to 16.92±0.38%, which
was <20% in the present study. This may be explained by the low
expression of FcRγIII (CD16) on the surface of CIK/NK cells, which
was only 19.01±1.27%. FcRγIII (CD16) activates the ADCC pathway by
combining with Fc region of the anti-GD2 antibody (62). However, this study's bi-factor (IL-2
and IL-7) culture system has no effect on increasing the expression
of CD16 on these cells, therefore no comparison is necessary for
the expression of CD16 before and after culture. The expression of
CD16 on CIK/NK cells was tested after culture, in order to
determine the possible proportion of CIK/NK cells involved in
anti-GD2-mediated ADCC effect, which may provide an explanation to
the low killing effect of combined therapy. Seidel et al
(63) showed long treatment time may
be beneficial for increasing killing efficacy. Furthermore, in this
experiment we defined late apoptosis and cell death induced by
CIK/NK cells only, anti-GD2 only or CIK/NK cells combined with
anti-GD2 as effective killing, which does not include early
apoptosis, therefore PI single staining was performed instead of
Annexin-V/PI double staining, which may give another explanation to
the low killing effect.
In conclusion, this study provided supporting
evidence for treating relapsed/refractory NB with CIK/NK cells
combined with anti-GD2 antibodies. Immunotherapy combined with
monoclonal antibodies is a potential novel strategy for treating
relapsed and refractory NB; however, further studies are required
in order to validate this method.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the
Guangdong Natural Science Foundation (grant nos. 2014A030313024 and
2017A030313806) and the Guangdong Science and Technology Department
(grant no. 2015B050501004).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CZ and XX performed the experiments and wrote the
manuscript. KH designed the experiments and collected the samples.
XP analyzed the experimental data. YL, LL and WW performed data
analysis and revised the manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Sun Yat-sen Memorial Hospital at Sun Yat-sen University (Guangzhou,
China). This study was performed in compliance with the Helsinki
Declaration. All patients gave written informed consent to
participate in the present study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Keshelava N, Davicioni E, Wan Z, Ji L,
Sposto R, Triche TJ and Reynolds CP: Histone deacetylase 1 gene
expression and sensitization of multidrug-resistant neuroblastoma
cell lines to cytotoxic agents by depsipeptide. J Natl Cancer Inst.
99:1107–1119. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chowdhury F, Lode HN, Cragg MS, Glennie MJ
and Gray JC: Development of immunomonitoring of antibody-dependent
cellular cytotoxicity against neuroblastoma cells using whole
blood. Cancer Immunol Immunother. 63:559–569. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cotterill SJ, Pearson AD, Pritchard J,
Foot AB, Roald B, Kohler JA and Imeson J: Clinical prognostic
factors in 1277 patients with neuroblastoma: Results of the
European neuroblastoma study group ‘survey’ 1982–1992. Eur J
Cancer. 36:901–908. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Maris JM: Recent advances in
neuroblastoma. N Engl J Med. 362:2202–2211. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yamamoto N, Kozaki A, Hartomo TB, Yanai T,
Hasegawa D, Kawasaki K, Kosaka Y, Matsuo M, Hirase S, Mori T, et
al: Differential expression of minimal residual disease markers in
peripheral blood and bone marrow samples from high-risk
neuroblastoma patients. Oncol Lett. 10:3228–3232. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Carr-Wilkinson J, O'Toole K, Wood KM,
Challen CC, Baker AG, Board JR, Evans L, Cole M, Cheung NK, Boos J,
et al: High frequency of p53/mdm2/p14arf pathway abnormalities in
relapsed neuroblastoma. Clin Cancer Res. 16:1108–1118. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gillet JP, Efferth T and Remacle J:
Chemotherapy-induced resistance by atp-binding cassette transporter
genes. Biochim Biophys Acta. 1775:237–262. 2007.PubMed/NCBI
|
|
8
|
Jackson JR, Kim Y, Seeger RC and Kim ES: A
novel minimal residual disease model of neuroblastoma in mice. J
Pediatr Surg. 51:991–994. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tchirkov A, Greze V, Plantaz D, Rouel N,
Vago P and Kanold J: Very long-term molecular follow-up of minimal
residual disease in patients with neuroblastoma. Pediatr Blood
Cancer. 65:e274042018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Haber M, Smith J, Bordow SB, Flemming C,
Cohn SL, London WB, Marshall GM and Norris MD: Association of
high-level mrp1 expression with poor clinical outcome in a large
prospective study of primary neuroblastoma. J Clin Oncol.
24:1546–1553. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
D'Aguanno S, D'Alessandro A, Pieroni L,
Roveri A, Zaccarin M, Marzano V, De Canio M, Bernardini S, Federici
G and Urbani A: New insights into neuroblastoma cisplatin
resistance: A comparative proteomic and meta-mining investigation.
J Proteome Res. 10:416–428. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Iwasaki I, Sugiyama H, Kanazawa S and
Hemmi H: Establishment of cisplatin-resistant variants of human
neuroblastoma cell lines, tgw and goto, and their drug
cross-resistance profiles. Cancer Chemother Pharmacol. 49:438–444.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hakomori S: Tumor-associated carbohydrate
antigens defining tumor malignancy: Basis for development of
anti-cancer vaccines. Adv Exp Med Biol. 491:369–402. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Allende ML and Proia RL: Lubricating cell
signaling pathways with gangliosides. Curr Opin Struct Biol.
12:587–592. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Regina Todeschini A and Hakomori SI:
Functional role of glycosphingolipids and gan-gliosides in control
of cell adhesion, motility, and growth, through glycosy-naptic
microdomains. Biochim Biophys Acta. 1780:421–433. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wu ZL, Schwartz E, Seeger R and Ladisch S:
Expression of GD2 ganglioside by untreated primary human
neuroblastomas. Cancer Res. 46:440–443. 1986.PubMed/NCBI
|
|
17
|
Ahmed M and Cheung NK: Engineering
anti-GD2 monoclonal antibodies for cancer immunotherapy. FEBS Lett.
588:288–297. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Simon T, Hero B, Faldum A, Handgretinger
R, Schrappe M, Niethammer D and Berthold F: Consolidation treatment
with chimeric anti-GD2-antibody ch14.18 in children older than 1
year with metastatic neuroblastoma. J Clin Oncol. 22:3549–3557.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sait S and Modak S: Anti-GD2 immunotherapy
for neuroblastoma. Expert Rev Anticancer Ther. 17:889–904. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tran HC, Wan Z, Sheard MA, Sun J, Jackson
JR, Malvar J, Xu Y, Wang L, Sposto R, Kim ES, et al: TGFβR1
blockade with galunisertib (LY2157299) enhances anti-neuroblastoma
activity of the anti-GD2 antibody dinutuximab (ch14.18) with
natural killer cells. Clin Cancer Res. 23:804–813. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ladenstein R, Pötschger U, Valteau-Couanet
D, Luksch R, Castel V, Yaniv I, Laureys G, Brock P, Michon JM,
Owens C, et al: Interleukin 2 with anti-GD2 antibody ch14.18/CHO
(dinutuximab beta) in patients with high-risk neuroblastoma
(HR-NBL1/SIOPEN): A multicentre, randomised, phase 3 trial. Lancet
Oncol. 19:1617–1629. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Modak S and Cheung NK: Disialoganglioside
directed immunotherapy of neuroblastoma. Cancer Invest. 25:67–77.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cheung NK, Cheung IY, Kushner BH,
Ostrovnaya I, Chamberlain E, Kramer K and Modak S: Murine anti-GD2
monoclonal antibody 3F8 combined with granulocyte-macrophage
colony-stimulating factor and 13-cis-retinoic acid in high-risk
patients with stage 4 neuroblastoma in first remission. J Clin
Oncol. 30:3264–3270. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Federico SM, McCarville MB, Shulkin BL,
Sondel PM, Hank JA, Hutson P, Meagher M, Shafer A, Ng CY, Leung W,
et al: A pilot trial of humanized anti-GD2 monoclonal antibody
(hu14.18K322A) with chemotherapy and natural killer cells in
children with recurrent/refractory neuroblastoma. Clin Cancer Res.
23:6441–6449. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sorkin LS, Otto M, Baldwin WM III, Vail E,
Gillies SD, Handgretinger R, Barfield RC, Ming Yu H and Yu AL:
Anti-GD(2) with an FC point mutation reduces complement fixation
and decreases antibody-induced allodynia. Pain. 149:135–142. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Xu H, Guo H, Cheung IY and Cheung NK:
Antitumor efficacy of anti-GD2 IgG1 is enhanced by fc
glyco-engineering. Cancer Immunol Res. 4:631–638. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheung IY, Kushner BH, Modak S, Basu EM,
Roberts SS and Cheung NV: Phase I trial of anti-GD2 monoclonal
antibody hu3F8 plus GM-CSF: Impact of body weight, immunogenicity
and anti-GD2 response on pharmacokinetics and survival.
Oncoimmunology. 6:e13583312017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kushner BH, Cheung IY, Modak S, Basu EM,
Roberts SS and Cheung NK: Humanized 3F8 anti-GD2 monoclonal
antibody dosing with granulocyte-macrophage colony-stimulating
factor in patients with resistant neuroblastoma: A phase 1 clinical
trial. JAMA Oncol. 4:1729–1735. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ozkaynak MF, Gilman AL, London WB, Naranjo
A, Diccianni MB, Tenney SC, Smith M, Messer KS, Seeger R, Reynolds
CP, et al: Corrigendum: A comprehensive safety trial of chimeric
antibody 14.18 with GM-CSF, IL-2, and isotretinoin in high-risk
neuroblastoma patients following myeloablative therapy: Children's
oncology group study ANBL0931. Front Immunol. 9:16412018.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shoae-Hassani A, Hamidieh AA, Behfar M,
Mohseni R, Mortazavi-Tabatabaei SA and Asgharzadeh S: NK
cell-derived exosomes from NK cells previously exposed to
neuroblastoma cells augment the antitumor activity of
cytokine-activated NK cells. J Immunother. 40:265–276. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zenarruzabeitia O, Vitallé J, Astigarraga
I and Borrego F: Natural killer cells to the attack: Combination
therapy against neuroblastoma. Clin Cancer Res. 23:615–617. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Muntasell A, Ochoa MC, Cordeiro L,
Berraondo P, López-Díaz de Cerio A, Cabo M, López-Botet M and
Melero I: Targeting NK-cell checkpoints for cancer immunotherapy.
Curr Opin Immunol. 45:73–81. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Burga RA, Yvon E, Chorvinsky E, Fernandes
R, Cruz CRY and Bollard CM: Engineering the TGFβ receptor to
enhance the therapeutic potential of natural killer cells as an
immunotherapy for neuroblastoma. Clin Cancer Res. 25:4400–4412.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Thommesen JE, Michaelsen TE, Loset GA,
Sandlie I and Brekke OH: Lysine 322 in the human IgG3 C (H)2 domain
is crucial for antibody dependent complement activation. Mol
Immunol. 37:995–1004. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Schmeel LC, Schmeel FC, Coch C and
Schmidt-Wolf IG: Cytokine-induced killer (CIK) cells in cancer
immunotherapy: Report of the international registry on CIK cells
(IRCC). J Cancer Res Clin Oncol. 141:839–849. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Schmidt-Wolf IG, Negrin RS, Kiem HP, Blume
KG and Weissman IL: Use of a SCID mouse/human lymphoma model to
evaluate cytokine-induced killer cells with potent antitumor cell
activity. J Exp Med. 174:139–149. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wu YF, Lin YC, LI Y, Wang XP and Wei J:
Exploratory research of setting an optimal minor-factor culture
system of cytokine-induced killer cells/natural cells. J Sun
Yat-Sen University (Medical Sciences),. 30:361–366. 2009.
|
|
38
|
Akhter N, Madhoun A, Arefanian H, Wilson
A, Kochumon S, Thomas R, Shenouda S, Al-Mulla F, Ahmad R and Sindhu
S: Oxidative stress induces expression of the toll-like receptors
(TLRs) 2 and 4 in the human peripheral blood mononuclear cells:
Implications for metabolic inflammation. Cell Physiol Biochem.
53:1–18. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Biederbick KD and Schmidt-Wolf IGH:
Efficacy of cytokine-induced killer cells targeting CD40 and GITR.
Oncol Lett. 17:2425–2430. 2019.PubMed/NCBI
|
|
40
|
Gao D, Cai Y, Chen Y, Li W, Wei CC, Luo X
and Wang Y: Novel TLR7 agonist stimulates activity of CIK/NK
immunological effector cells to enhance antitumor cytotoxicity.
Oncol Lett. 15:5105–5110. 2018.PubMed/NCBI
|
|
41
|
Pinto NR, Applebaum MA, Volchenboum SL,
Matthay KK, London WB, Ambros PF, Nakagawara A, Berthold F,
Schleiermacher G, Park JR, et al: Advances in risk classification
and treatment strategies for neuroblastoma. J Clin Oncol.
33:3008–3017. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Weinstein JL, Katzenstein HM and Cohn SL:
Advances in the diagnosis and treatment of neuroblastoma.
Oncologist. 8:278–292. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ning BT, Yu B, Chan S, Chan JL, Huang JD
and Chan GC: Treatment of neuroblastoma with an engineered
‘Obligate’ anaerobic salmonella typhimurium strain YB1. J Cancer.
8:1609–1618. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kholodenko IV, Kalinovsky DV, Doronin II,
Deyev SM and Kholodenko RV: Neuroblastoma origin and therapeutic
targets for immunotherapy. J Immunol Res. 2018:73942682018.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yu AL, Gilman AL, Ozkaynak MF, London WB,
Kreissman SG, Chen HX, Smith M, Anderson B, Villablanca JG, Matthay
KK, et al: Anti-GD2 antibody with GM-CSF, interleukin-2, and
isotretinoin for neuroblastoma. N Engl J Med. 363:1324–1334. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Dobrenkov K and Cheung NK: GD2-targeted
immunotherapy and radioimmunotherapy. Semin Oncol. 41:589–612.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Anghelescu DL, Goldberg JL, Faughnan LG,
Wu J, Mao S, Furman WL, Santana VM and Navid F: Comparison of pain
outcomes between two anti-GD2 antibodies in patients with
neuroblastoma. Pediatr Blood Cancer. 62:224–228. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Pan Y, Wu Y, Ji J, Cai H, Wang H, Jiang Y,
Sang L, Yang J, Gao Y, Liu Y, et al: Effect of cytokine-induced
killer cells on immune function in patients with lung cancer. Oncol
Lett. 11:2827–2834. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sangiolo D, Martinuzzi E, Todorovic M,
Vitaggio K, Vallario A, Jordaney N, Carnevale-Schianca F, Capaldi
A, Geuna M, Casorzo L, et al: Alloreactivity and anti-tumor
activity segregate within two distinct subsets of cytokine-induced
killer (CIK) cells: Implications for their infusion across major
HLA barriers. Int Immunol. 20:841–848. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Kim HM, Lim J, Kang JS, Park SK, Lee K,
Kim JY, Kim YJ, Hong JT, Kim Y and Han SB: Inhibition of human
cervical carcinoma growth by cytokine-induced killer cells in nude
mouse xenograft model. Int Immunopharmacol. 9:375–380. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Xu YC, Xu Q, Li JJ, Gu XF, Lin XL, Sun L,
Lu HM, Tang L, Ma Y, Lu Z and Wang HX: Chemotherapy with or without
autologous cytokine-induced killer cell transfusion as the
frst-line treatment for stage IV gastrointestinal cancer: A phase
II clinical trial. J Cancer Res Clin Oncol. 142:1315–1323. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Mueller I, Ehlert K, Endres S, Pill L,
Siebert N, Kietz S, Brock P, Garaventa A, Valteau-Couanet D, Janzek
E, et al: Tolerability, response and outcome of high-risk
neuroblastoma patients treated with long-term infusion of anti-GD2
antibody ch14.18/CHO. MAbs. 10:55–61. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Bonanno G, Iudicone P, Mariotti A, et al:
Thymoglobulin, interferon-g and interleukin-2 efficiently expand
cytokine-induced killer (CIK) cells in clinical-grade cultures. J
Transl Med. 8:1292010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Leemhuis T, Wells S, Scheffold C, Edinger
M and Negrin RS: A phase I trial of autologous cytokine-induced
killer cells for the treatment of relapsed Hodgkin disease and
non-Hodgkin lymphoma. Biol Blood Marrow Transplant. 11:181–187.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Rettinger E, Kreyenberg H, Merker M, Kuçi
S, Willasch A, Bug G, Ullrich E, Wels WS, Bonig H, Klingebiel T and
Bader P: Immunomagnetic selection or irradiation eliminates
alloreactive cells but also reduces anti-tumor potential of
cytokine-induced killer cells: Implications for unmanipulated
cytokine-induced killer cell infusion. Cytotherapy. 16:835–844.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Vantaku V, Donepudi SR, Ambati CR, Jin F,
Putluri V, Nguyen K, Rajapakshe K, Coarfa C, Battula VL, Lotan Y
and Putluri N: Expression of ganglioside GD2, reprogram the lipid
metabolism and EMT phenotype in bladder cancer. Oncotarget.
8:95620–95631. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Orsi G, Barbolini M, Ficarra G, Tazzioli
G, Manni P, Petrachi T, Mastrolia I, Orvieto E, Spano C, Prapa M,
et al: GD2 expression in breast cancer. Oncotarget. 8:31592–31600.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Tesfaye M and Savoldo B: Adoptive cell
therapy in treating pediatric solid tumors. Curr Oncol Rep.
20:732018. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Esser R, Müller T, Stefes D, Kloess S,
Seidel D, Gillies SD, Aperlo-Iffland C, Huston JS, Uherek C,
Schönfeld K, et al: NK cells engineered to express a GD2-specific
antigen receptor display built-in ADCC-like activity against tumor
cells of neuroectodermal origin. J Cell Mol Med. 16:569–581. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Wold ED, Smider VV and Felding BH:
Antibody therapeutics in oncology. Immunotherapy (Los Angel).
2:1082016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Stasiłojć G, Österborg A, Blom AM and
Okrój M: New perspectives on complement mediated immunotherapy.
Cancer Treat Rev. 45:68–75. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Kudo K, Imai C, Lorenzini P, Kamiya T,
Kono K, Davidoff AM, Chng WJ and Campana D: T lymphocytes
expressing a CD16 signaling receptor exert antibody-dependent
cancer cell killing. Cancer Res. 74:93–103. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Seidel D, Shibina A, Siebert N, Wels WS,
Reynolds CP, Huebener N and Lode HN: Disialoganglioside-specific
human natural killer cells are effective against drug-resistant
neuroblastoma. Cancer Immunol Immunother. 64:621–634. 2015.
View Article : Google Scholar : PubMed/NCBI
|